-
5/26/2018 Cardiotocogram(Ctg)
1/36
CARDIOTOCOGRAM
DR IMRAN KHANSUPERVISER
DR.AFIFUDDIN
-
5/26/2018 Cardiotocogram(Ctg)
2/36
Definition
Cardiotocography (CTG)
CTG is technical means of recording (-grahpy) the fetal heart
beat(cardio-) and the uterine contraction (-toco-). The machine
used toperform this monitoring is called a cardiotocograph. CTG
monitoring
is essentially the used of cardiotocograph for evaluation of
fetalwellbeing in labour
-
5/26/2018 Cardiotocogram(Ctg)
3/36
Basic features and fetal heart rate pattern
Fetal heart rate pattern has 4 recognizable
features : Baseline heart rate 110 160
Baseline variability 5 25
Acceleration
Deceleration
-
5/26/2018 Cardiotocogram(Ctg)
4/36
-
5/26/2018 Cardiotocogram(Ctg)
5/36
-
5/26/2018 Cardiotocogram(Ctg)
6/36
Baseline FHR : the mean level of FHR when this is stable,
excluding acceleration and deceleration. It is determined
overperiod of 5 10 minutes and expressed in beats per
minute(BPM).
Baseline variability : the minor fluctuation in baseline
FHRoccurring at 3 5 cycle per minute. It is measured byestimating
the difference in beat per minutes betweenhighest peak and the
lowest trough of fluctuation in oneminute segment of trace. It is
consider to reduce if less 5
-
5/26/2018 Cardiotocogram(Ctg)
7/36
Acceleration: transient increase in FHR of 15 bpm or moreand
lasting 15 second or more.
Deceleration: Transient episodes of slowing FHR below
thebaseline level of more than 15bpm and lasting 15 second or
more
-
5/26/2018 Cardiotocogram(Ctg)
8/36
Classification of CTG and Intrapartum trace ( RCOG 2001)
Classification Definition
Normal All four features fall into the category
Suspicious A CTG whose features fall into one ofthe non
reassuring categories and theremainder of the features
arereassuring
Pathological A CTG whose features fall into two ormore non
reassuring categories or
one or more abnormal categories
-
5/26/2018 Cardiotocogram(Ctg)
9/36
Baseline Variability Deceleration Acceleration
Reassuring 110 - 160 > 5 None Present
Non reassuring 100 109161 - 180
< 5 for >40min but 180
< 5 for > 90min
Atypical variabledeceleration, latedeceleration,single
prolongeddeceleration >3min
-
5/26/2018 Cardiotocogram(Ctg)
10/36
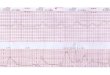
Types of deceleration
Early deceleration
Late deceleration
Variable deceleration
Atypical deceleration
Prolonged deceleration
-
5/26/2018 Cardiotocogram(Ctg)
11/36
Early deceleration : Uniform, repetitive, periodic slowing of
FHR
with onset early in the contraction and return to baseline at
the endof contraction
Late deceleration : Uniform repetitive periodic slowing of
FHRwith onset mid to end of contraction and nadir more than 20
secondafter the peak of contraction and ending after the
contraction
Variable deceleration : variable, intermittent periodic slowing
ofFHR with rapid onset and recovery. Time relationships
withcontraction cycle are variable and they may occur in
isolation
Prolonged deceleration : An abrupt decrease in FHR to levelbelow
baseline last atleast 60 90 seconds. These decelerationbecome
pathological if they cross to contraction,i.e. greater than
3minutes
-
5/26/2018 Cardiotocogram(Ctg)
12/36
Atypical variable : variable deceleration with any of
following
additional deceleration component : loss of primary or secondary
rise in baseline rate
Slow return to baseline FHR after the end of contraction
Prolonged secondary rise in baseline rate
Biphasic deceleration
Continuation of baseline rate at lower level
Sinusoidal pattern : A regular oscillation of baseline long
termvariability resembling a sine wave. This smooth, undulating
patternlasting at least 10 minutes, has a relatively fixed period
of 3 5cycle per minute and amplitude of 5 -15
-
5/26/2018 Cardiotocogram(Ctg)
13/36
-
5/26/2018 Cardiotocogram(Ctg)
14/36
-
5/26/2018 Cardiotocogram(Ctg)
15/36
-
5/26/2018 Cardiotocogram(Ctg)
16/36
-
5/26/2018 Cardiotocogram(Ctg)
17/36
-
5/26/2018 Cardiotocogram(Ctg)
18/36
-
5/26/2018 Cardiotocogram(Ctg)
19/36
-
5/26/2018 Cardiotocogram(Ctg)
20/36
-
5/26/2018 Cardiotocogram(Ctg)
21/36
-
5/26/2018 Cardiotocogram(Ctg)
22/36
-
5/26/2018 Cardiotocogram(Ctg)
23/36
-
5/26/2018 Cardiotocogram(Ctg)
24/36
-
5/26/2018 Cardiotocogram(Ctg)
25/36
Modes of fetal heart monitoring
Continuous CTG
Intermittent CTG
Internal / direct monitoring ( fetal scalp electrode )
Intermittent auscultation
-
5/26/2018 Cardiotocogram(Ctg)
26/36
INDICATION FOR CONTINUOUS CTG MONITORING
Maternal condition
Antenatal Hypertension Diabetes mellitus Antepartum hemorrhage
Cardiac disease Severe anemia
Hyperthyroidism Renal disease
Intrapartum Vaginal bleeding Maternal pyrexia Chorioamnionitis
Epidural / reginonal anesthesia
Labour Previous ceaseran section Prolonged ROM Induced /
augmented labour Uterine hyperstimulation
Fetal condition
Growth restricted fetus Oligohydramion Prematurity Rhesus
isoimmunization Multiple pregnancy Breech
Meconium stained liquor Post term pregnancy
-
5/26/2018 Cardiotocogram(Ctg)
27/36
Intermittent CTG monitoring ( 2Hourly )
For all other patient not listed above
Internal or direct monitoring / Fetal scalp electrode
Indication
External tracing inadequate / poor quality for
interpretation
Monitoring 1sttwin in twin pregnancy in labour
Contraindication Face presentation
Unknown presentation
HIV seropositive / Hep B,C
Suspected thrombocytopenia
Intermittent auscultation
Auscultation of FHR at regular intervals for at least 60
second
-
5/26/2018 Cardiotocogram(Ctg)
28/36
It is equally as effective as continuous CTGmonitoring for low
risk women in labour.
continuous EFM should be offered andrecommended if;A)there is
evidence on auscultation of abaseline 160bpm.
B)there is evidence on auscultation of anydecelerations.C)If any
intrapartum risk facrors develop.Intermittent auscultation should
be done;A)every 15-30min(throughout and aftercontraction) in active
first stage of labour.B)every 5 min in active
secondstage(throughout and after contraction)
-
5/26/2018 Cardiotocogram(Ctg)
29/36
RESPONSIBILITIES ASSOCIATED WITH EFM(electronic fetal
monitoring)
a)Reason, benefits and limitation should be explained to
patient
b)The date, time on the machine should be correctly set.
C)paper speed should be set at 1cm/min
d)Traces should be labeled with mothers name, date,time,RN.
E)Any intrapartum events that affect FHR should be recorded
on the tracing, signed, date and time.
F)Any member of staff who reviewed the CTG tracing should
note their findings on tracing together with time ,date,
signature and chop.
-
5/26/2018 Cardiotocogram(Ctg)
30/36
G)If CTG is suspicious/pathological, staff and house
officer should ;.inform medical officer OR specialist.
.change maternal position left lateral
.Withhold oxytocin infusion if required
.Vaginal examination
-
5/26/2018 Cardiotocogram(Ctg)
31/36
Causes of fetal heart rate bradycardia
.fetal bradycardia is define as a decrease in the baseline
FHR to less than 100beats per minute1.FETAL HYPOXIA; bradycardia
is a late sign of fetal
hypoxia(a continual lack of oxygen)
.The heart rate slow in response to a depression of
heart muscle(myocardial)activity caused by this
continued decrease in needed oxygen.
2.MEDICATION; Medication such as narcotics cause
bradycardia by preventing receptors sites in the fetal
heart muscle from accepting epinephrine, which works
to increase heart rate.
-
5/26/2018 Cardiotocogram(Ctg)
32/36
3.EPIDURAL;Causes vasodilation, which leads toan increase in the
incidence of maternal hypotension
during labour which causes bradycardia indirectly due
to reflex mechanism, a potential complication forregional
anesthesia.
4.SYNTHETIC OXYTICIN(PITOCIN)may produced
bradycardia by causing hyperstimulation of the
uterine muscle(myometrium),resulting in hypoxia.
.
-
5/26/2018 Cardiotocogram(Ctg)
33/36
5.MATERNAL HYPOTENSION;
supine hypotension syndrome caused
by pressure of the uterus and its
content on the inferior vena cava ,
when you lay on your back, results in
decrease in maternal blood pressure
-
5/26/2018 Cardiotocogram(Ctg)
34/36
Causes of fetal heart rate
tachycardia.Tachycardia; suspicious tachycardia is defined as
beingbetween 161-180 whereas a pathological pattern is above
180.
1.FETAL HYPOXIA; Tachycardia may be early sign of
hypoxia(fetal lack of adequate oxygen).
2.MEDICATION; Medication used to prevent/stop premature
labor such as terbutaline(sympathomimetic),have a
stimulating effect on the fetal heart, which increase the
heart
rate.
-
5/26/2018 Cardiotocogram(Ctg)
35/36
THANKS
-
5/26/2018 Cardiotocogram(Ctg)
36/36
3.PREMATURITY;Apremature baby hasan immature nervous system
resulting
in increased heart rate.4.MATERNAL FEVER; Both themothers and
the babys metabolism isincrease, which result in increaseheart
rate.5.FETAL INFECTION;This may be anearly sign of an
intrauterine
infection(a stress reaction tosepsis)prolonged ruptured
ofmembrane may lead to maternal and
f t l i f ti