Embed Size (px)
Citation preview
Case Presentation
Thamer Abdullah Bin Traiki
Case Presentation
• A 44-year-old woman with a history of multiple complicated urinary tract infections requiring intermittent hospitalization over the previous year was referred with anasarca and bloody diarrhea.
• Type 2 diabetes mellitus, morbid obesity, congestive heart failure, and severe pulmonary hypertension.
Cont…
• Two months earlier, the patient had been treated sequentially with levofloxacin, ceftriaxone, and augmentin for an Escherichia coli urinary tract infection.
• Eight weeks after this antibiotic treatment, while at a rehabilitation center, frequent watery diarrhea developed, with approximately 15 watery bowel movements per day mixed with blood.
Cont…
• There was NO fever .• But there was cramping lower abdominal
pain.• Stool culture results and microscopy for ova
and parasites were negative. • Stool enzyme immunoassay (EIA) for C difficile
was positive.
Cont…
• Treatment with oral metronidazole was initiated .
• However, her diarrhea persisted after 6 days of treatment.
• The pt then readmitted.
Cont…
Investigation upon admission :• WBCs 16• Hb 10• MCV 83• Nucleated RBCs 83%• Plat 361• Bands 7%• U&E were N except urea & creat
Cont…
• Treatment with oral vancomycin was initiated and oral metronidazole was continued.
• The patient's diarrhea persisted, now 3 weeks after initiation of treatment.
• She began to develop worsening pulmonary edema and anasarca.
• Oral vancomycin was continued and treatment with intravenous metronidazole was initiated.
Cont…
• WBCs repeated 23
• CT showed thickening of the wall of the colon but NO megacolon or abscess .
• The pt underwent Flex Sig .
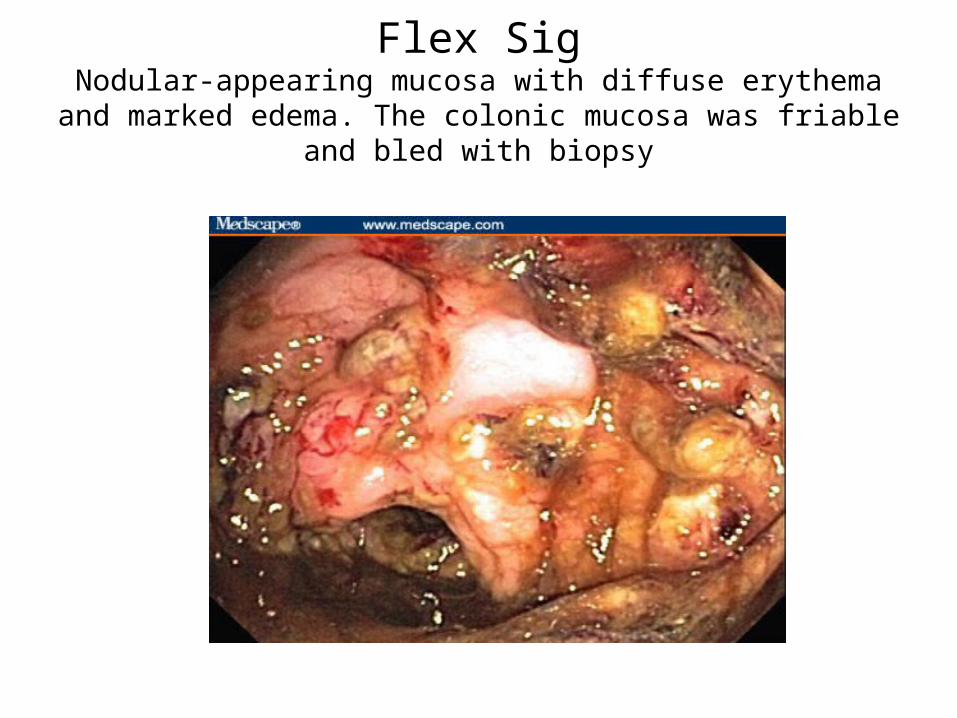
Flex SigNodular-appearing mucosa with diffuse erythema and marked edema.
The colonic mucosa was friable and bled with biopsy
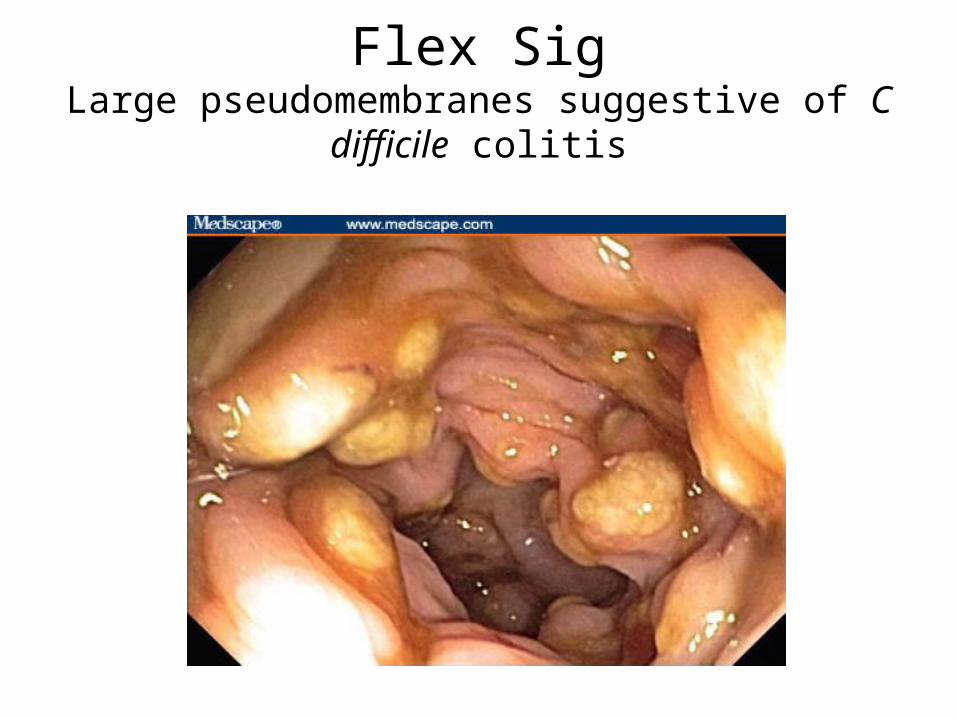
Flex SigLarge pseudomembranes suggestive of C difficile colitis

Cont…Pathology
• Biopsies of the descending colon showed microulcerations in the epithelium with overlying pseudomembrane (Figure 3). There was no evidence of cytomegalovirus infection on biopsy or by viral cultures.
Cont…• Vancomycin enemas were started and treatment with oral
vancomycin and intravenous metronidazole were continued without improvement.
• The patient continued to have abdominal pain and now also had intermittent low-grade fevers.
• One dose of intravenous immune globulin (IVIG) was administered, with an improvement in diarrhea symptoms within 36 hours of administration.
• Six weeks after the onset of symptoms, the patient's diarrhea has resolved, with normalization of her white blood cell count and renal function.
• She has been discharged on a prolonged taper of oral vancomycin and a 1-month course of oral metronidazole.
Clostridium difficile-associated Diarrhea
(CDAD)
Clostridium Difficile
• motile Gram positive rod. • quite commonly in the faeces of neonates.• Considered to be normal till the age of 2 years because the cells of a newborn's colon are too
immature to bind the toxins produced by the bacteria. Gastroenterol Clin North Am, 2001 30(3), 753.
• not generally regarded as a normal commensal in adults .
Cont…
• produces an enterotoxin (toxin A) and a cytotoxin (toxin B)
• Clostridium difficile is the leading infectious cause of nosocomial diarrhea.
Arch Intern Med. 1996;156:1449-1454.
• can cause life-threatening diarrhea and colitis
Cont…
• occurs in about 20% of hospitalized patients taking antibiotics .
Arch Intern Med 1986;146(1):95-100
• Most patients treated for this infection improve, but about 20% relapse. Clin Infect Dis 1997;24(3):324-33
Relapse is defined as recurrence of symptoms and documentation of infection within 2 months of successful
standard therapy. Patients with relapsing C difficile colitis are prone to further
relapses, each one making eradication more difficult.
Risk factors for CDAD
C. difficile-associated disease occurs when the normal intestinal flora is altered, allowing C. difficile to flourish in the intestinal tract and produce a toxin that causes a watery diarrhea .
Cont…risk factor
Antimicrobial use,• C difficile infection has been reported with use of virtually all
antibiotics and some antiviral and antifungal agents. It most commonly occurs with use of the penicillins , ampicillin and amoxicillin, the cephalosporins, and clindamycin.
• The prevalence of complicating pseudomembranous colitis is variable but can be as great as 10% in patients taking clindamycin or lincomycin .
Mayo Clin Proc 2001;76(7):725-30
Cont…risk factor
• gastrointestinal surgery or manipulation,• severe underlying disease increases the risk
of nonoscomial CDAD in hospitalized patients Infect Control Hosp Epidemiol. 2002;23:653-659
• elderly and patients with colonic disease are predisposed for the c. diff
• Repeated enemas, prolonged nasogastric tube insertion .
CDAD
• Symptoms typically occur 7-10 days following antibiotic therapy, but have been reported to occur as early as on the first day of therapy or as long as 10 weeks after the completion of therapy.
Med Clin North Am. 1982;66:655-664.
• Frequent bowel movements, abdominal pain, and fever.
• Systemic manifestations may include dehydration, prerenal azotemia, sepsis syndrome, toxic colitis, and even death in seriously ill patients.
Cont…
The clinical presentation
• range from an asymptomatic carrier state, to unexplained leukocytosis in the absence of diarrhea or to fulminant colitis.
• In subacute cases of infection, hypoalbuminemia results from pancolitis, leading to the loss of albumin, which is only partially compensated for by hepatic synthesis.
• Host immune factors and the virulence of the C difficile strain account for differences in clinical presentation.
Infect Immun. 1991;59:2456-462.
Cont…
• Laboratory tests may demonstrate a marked elevation in the white blood cell count with a left shift to immature forms.
Cont…
• Diagnosis C difficile produces 2 protein exotoxins, toxin A and toxin B, that induce fluid secretion,
inflammation, and apoptosis of intestinal epithelial cells.
Most C difficile strains that cause disease produce both toxin A and toxin B. However, 2% of the isolates of C difficile associated with outbreaks are A-B+ (ie, toxin A negative, toxin B positive).
J Clin Micribiol. 2004;42:1035-1041.
Cont…
• Enzyme immunoassay (EIA) for C difficile toxins has a sensitivity that ranges from 88%-93%.
Eur J Clin Microbiol Infect Dis. 2007;26:115-11
ELISA usually detect toxin A
• Stool cytotoxic assay has a significantly higher sensitivity for the detection of both toxins, but requires 48 hours to perform.
Cont…
If the clinical suspicion for C difficile infection is high and stool EIA is negative,
initiation of treatment should be considered while awaiting the results of
the stool cytotoxic assay.
You have to keep in your mind
• Osmotic diarrhea frequently occurs with the use of antibiotics.
This is secondary to the inhibition of colonic microflora that normally ferment unabsorbed carbohydrate to short-chain fatty acids that are subsequently absorbed by colonic mucosa.
• antibiotic-associated diarrhea not caused by C.Diff. e.g.Klebsiella oxytoca infection
In contrast to CDAD, characterized by 3 or 4 loose bowel movements a day, usually without any other systemic complaints. It can be treated conservatively by stopping the inciting antibiotic .
Treatment • Discontinuation of the offending antibiotic .• Avoidance of antimotility agents • Start oral metronidazole or vancomycin 10-14 days.• Earlier studies which demonstrated a 96%
response rate to metronidzole therapy,Gastroenterol Clin North Am, 2001 30(3), 753.
• BUT prospective observational study performed in 2005 by Musher et al involving 207 patients with C difficile diarrhea found that 22% continued to have symptoms after 10 days of treatment.
Cont…
Standard therapy for Clostridium difficile infection
• Metronidazole (Flagyl) 250-500 mg PO tid or qid X 10-14 days
• Vancomycin HCl (Vancocin, Vancoled) 125 mg PO qid X 10-14 days
Cont…
Metronidazole is first-line therapy. WHY ?
• Cost as well as concern about antibiotic resistance. • Can be given orally & parenterally while Vanco can’t
reach high concentration if given IV• Development of vancomycin-resistant Enterococcus
faecium infection . Am J Infect Control 1995;23(2):87-94
Cont…The indications for oral vancomycin :• WBCs of (> 20,000 cells/mm3), • new elevation in serum creatinine,• toxic megacolon, • septic shock, or• if there is failure to respond to metronidazole
within 48-72 hours.Curr Opin Gastroenterol. 2007; 23:4-9.
Cont…indication of Vanco
• Patients who are documented to be allergic to or intolerant of metronidazole
• Patients receiving warfarin• Woman who are pregnant or lactating • Patient with at least 2 recurrent episodes &
treated with oral metronidazole .
Causes for Recurrence
• The exact mechanism of recurrent C difficile colitis is unclear.
• Not related to bacterial resistance to standard antimicrobial therapies but “Hypothesis”
• breakdown of the normal flora barrier of the colon after antibiotic treatment.
• Vancomycin and metronidazole kill the vegetative form of C difficile but do not kill the spores, which can germinate and eventually produce toxins
• repeated use of antibiotics
Who Will Have Recurrence?
Fekety and colleagues 1997 studied the characteristics of patients with recurrent C difficile infection.
• previous C difficile diarrhea, • onset of disease in spring,• exposure to additional antibiotics for treatment of other
infections, • infection with immunoblot type 1 or type 2 strains of C
difficile, and• female sex.
Patients who have one recurrence are 65% more likely to have further
recurrences.
Treatment of Recurrences
Tapering oral antibiotic dose• The goal of initial treatment is to eliminate the
bacteria and vegetative spores.• Tapering the dose of vancomycin or
metronidazole over 4 to 6 weeks has been shown to be effective.
• Tapering the dose works to kill viable C difficile bacteria while allowing restoration of normal colonic flora .
Cont…
What about vanco enemas ?• A small retrospective case series suggested
that intracolonic vancomycin (ICV) may be effective as adjuvant treatment in patients with severe disease.
Clin Infect Dis. 2002;35:690-696.
PROBIOTIC THERAPY
• to repopulate or restore colonic bacteria as an adjunct to antibiotic therapy
Am J Gastroenterol 2000;95(1 Suppl):S11-13
• Saccharomyces boulardii is a nonpathogenic yeast that releases a protein that interferes with the binding of toxin A to its receptor .
Gastroenterology 1993;104:1108-15
Cont…
• In a recent meta analysis, only the probiotic Saccharomyces boluardi was effective for C difficile disease.
Am J Gastroenterol. 2006;101:812-822.
• The administration of S boulardii has been shown to be effective both on its own and in combination with metronidazole or vancomycin in patients with recurrent C difficile infection.
In a randomized placebo-controlled trial , S boulardii in combination with vancomycin or
metronidazole reduced the relapse rate by 50% and was well tolerated.
Cont…
Is there any role for IV immunoglobulin ?• Because C difficile colitis is a toxin-mediated disease,
it has been assumed that immune globulin acts by binding and neutralizing toxin but the exact mechanism by which IVIG antitoxin binds to toxins A and B in the colonic lamina propria or intestinal lumen is unclear.
Cont…
• In a retrospective review of 14 patients with severe, refractory or recurrent C difficile diarrhea who received adjunctive treatment with IVIG, 9 (64%) responded to treatment .
Dis Colon Rectum. 2006;49:1-6.
Surgery
• Subtotal colectomy• patients with severe CDAD who fail to respond to
medical therapy or have signs of systemic toxicity, organ failure, or peritonitis.
J Surg. 1998;85:229-231
THANK YOU