Embed Size (px)
Citation preview
65The Permanente Journal/ Spring 2007/ Volume 11 No. 2
Presentation of Osteitis and OsteomyelitisPubis as Acute Abdominal Pain
By Diane V Pham, MDKendall G Scott, MD
AbstractOsteitis pubis is the most common inflammatory condi-
tion of the pubic symphysis and may present as acute ab-dominal, pelvic, or groin pain. Osteomyelitis pubis canoccur concurrently and spontaneously with osteitis pu-bis. Primary care physicians should consider these con-ditions in patients presenting with abdominal and pelvicpain. A thorough history, including type of physical ac-tivity, and a focused physical examination will be useful,and imaging modalities may be helpful. A biopsy andculture of the pubic symphysis will usually confirm thediagnosis. Treatment for osteitis pubis generally involvesrest and anti-inflammatory medications. Failure with thisconservative treatment should alert the physician to thepossibility of osteomyelitis, which needs treatment withantibiotics. Prognosis for recovery is excellent with de-finitive diagnosis and treatment.
IntroductionAbdominal pain may be the presenting symptom in
a wide range of diseases. This proposes a difficult chal-lenge for the primary care physician. Acute pain oftenrequires emergency surgical intervention, but unnec-essary invasive procedures can be avoided when a goodhistory is taken and thorough physical examination isconducted. Osteitis pubis is a common but often undi-agnosed condition causing pain in the pubic area, groin,and lower rectus abdominal muscle. Osteomyelitis pubisis an infectious disease with clinical manifestations simi-lar to those of osteitis pubis. These conditions are of-ten overlooked as or masked by abdominal pain, whichmay lead to unnecessary tests and procedures. Thiscase report discusses the onset of acute abdominal painin an athlete with both osteomyelitis and osteitis pu-bis. It is important to recognize that both conditionsmay occur simultaneously in one patient. Failure toidentify both disease processes could lead to inaccu-rate treatment and lifelong complications.
Case PresentationA previously healthy male, age 17 years, presented
with a three-day history of severe right lower quadrantabdominal pain. Initial workup findings, including thosefor a computed tomography scan of the abdomen andpelvis, were normal, and he was treated with nonste-roidal anti-inflammatory drugs (NSAIDs). He returnedtwo days later with a fever of 38.3°C and worseningsharp, constant abdominal pain, radiating to the supra-pubic area and exacerbated by movement. He was nau-seated and anorectic and vomited nonbilious,nonbloody material once. His past medical history anda review of systems provided no new insights.
His abdomen was soft and nondistended, but he ex-hibited right lower quadrant tenderness with involun-tary guarding and rebound tenderness. The psoas, ob-turator, and Rovsing’s signs were positive; rectalexamination findings were normal. The leukocyte countwas 12,400 cells/mL, with a polymorphonuclear leu-kocytosis. Diagnostic laparoscopy showed no defini-tive intra-abdominal pathology, although a long, mildlyengorged retroperitoneal appendix was removed; thepathologist found no inflammation.
Fever and worsening abdominal and suprapubic painpersisted, with pain radiating to both groins and pre-venting ambulation. Additional detailed history uncov-ered the information that the patient was an avid col-lege soccer and tennis player and had participated in asoccer tournament the previous week. Examination nowshowed tenderness in the right lower quadrant andsuprapubic and bilateral groin areas, tenderness of thepubic symphysis, and worsening pain with abductionof either hip. He developed bilateral inguinal lymphad-enopathy, with no evident skin lesion. He had nega-tive findings on blood tests including total protein, al-bumin, liver tests, complement components 3 and 4,creatine kinase, aldolase, beta
2-microglobulin, anti-DNA,
and antinuclear antibody panel. His erythrocyte sedi-
CASE STUDY
Diane V Pham, MD, (left) is a third-year family medicine resident at the Fontana MedicalCenter, CA. E-mail: [email protected].
Kendall G Scott, MD, (right) is the Program Director for the Southern California KaiserPermanente Residency Program in Fontana and an Adjunct Assistant Professor in the Department
of Physician Assistant Education at Loma Linda University, CA. E-mail: [email protected].
CME
Osteitis pubis isa commonbut often
undiagnosedcondition causingpain in the pubicarea, groin, and
lower rectusabdominal
muscle.Osteomyelitis
pubis is aninfectious disease
with clinicalmanifestationssimilar to thoseof osteitis pubis.

66 The Permanente Journal/ Spring 2007/ Volume 11 No. 2
CASE STUDY
mentation rate (ESR) was 109 mm/h and C-reactiveprotein (CRP) level was 11.6 mg/dL; his leukocyte countremained elevated.
A pelvic radiograph showed slight deformity of theright suprapubic ramus at the level of the pubic sym-physis, with irregularity of the iliac wing at the anterioriliac spine region. A 99mtechnetium methyl diphosphonate
bone scan showed increased radiotracer ac-tivity in the left superior pubic ramus, leftanterior iliac crest, and right posterior iliaccrest. A pelvic magnetic resonance imaging(MRI) scan revealed multiple enlarged rightinguinal lymph nodes and an increased sig-nal in the right inferior pubic ramus and rightilium bone marrow, with muscular changes.These findings were consistent with osteo-myelitis and osteitis pubis. It was decided thata confirmatory pubic biopsy was not needed.
The patient was treated with intravenouscefazolin, ibuprofen, and bed rest. Over aweek his condition improved markedly; hebecame afebrile and he was able to ambulatewith assistance. His white blood cell count
normalized; his ESR and CRP level were descending.He was discharged to complete a six-week antibioticregimen via a peripherally inserted central catheter, plusibuprofen and physical therapy. His ESR and CRP levelnormalized, but he was not completely asymptom-atic until three months later, at which time he returnedto his normal soccer and tennis training.
DiscussionBackground
Edwin Beer first described osteitis pubis in 1924 inpatients undergoing suprapubic surgery.1 It is the mostcommon inflammatory disease of the pubic symphysis.It can be seen in any patient population but is moreprevalent in men ages 30 to 49 years.2 Although theprecise etiology of osteitis pubis remains unknown,trauma during surgery or childbirth is responsible formost cases. Infection seems to be a predisposing fac-tor.3,4 Biopsies of the pubic symphysis and adjacent bonyareas show signs of subacute and chronic inflammationinvolving the periosteum, bone, and cartilage.4
Osteomyelitis pubis is often misdiagnosed as osteitispubis, until conservative treatment for osteitis pubisfails.5 Risk factors for osteomyelitis pubis include fe-male incontinence surgery, sports injury, pelvic malig-nancy, and intravenous drug use.6 Often there is in-oculation during gynecologic or urologic surgery.However, other cases of osteomyelitis pubis inexplica-
bly follow seemingly normal spontaneous vaginal de-livery or, as in the patient described here, athletic ac-tivity.7–9 Causative organisms differ according to riskfactors. Patients with recent pelvic surgery usually havepolymicrobial infection, involving fecal flora. Staphy-lococcus aureus is the major cause among athletes,whereas pseudomonas aeruginosa infection is the pre-dominant pathogen in intravenous drug users.6
The remainder of this discussion focuses on occur-rence of osteitis and osteomyelitis pubis in the athlete.
Anatomy and PathomechanicsThe pubic symphysis is a rigid, fibrocartilaginous joint
between the pubic rami. The abdominal muscles, con-sisting of the rectus abdominus and external and inter-nal oblique muscles, attach distally to the inguinal liga-ment, conjoined tendon, and pubic symphysis. Theadductor muscles, consisting of the pectineus, adduc-tor longus, adductor brevis, adductor magnus, and gra-cilis, arise from the superior and inferior rami of thepubis.10 These two muscle groups act antagonisticallyto stabilize the symphysis. Any muscle imbalances be-tween the abdominal and hip adductor muscles maycause osteitis pubis.11
Sprinting, cutting, and kicking activities involvingjumping, twisting, or turning motions cause microtraumaand shear stress across the pubic symphysis, resultingin inflammation. These repetitive movements occur inrunning, soccer, tennis, ice hockey, and football, butany active person may present with osteitis pubis. Thusit must be considered in any patient with groin, hip, orabdominal pain.12 Osteomyelitis pubis, a bacterial in-fection of the pubic symphysis or adjacent bone alsohas been reported to occur spontaneously in athletes.13
Clinical Findings and DiagnosisA detailed medical history, including the actual mo-
tions the patient repeats during sports activity and a fa-miliarity with the possible mechanisms of injury, canlead the physician to a more accurate diagnosis. Thor-ough examination of the groin, abdomen, hips, spine,and lower extremities is crucial.14 Patients with osteitispubis can present with vague unilateral or bilateral com-plaints of abdominal, pelvic, or groin pain. Usually in-sidious in nature, it can occasionally be acute, sharp,burning pain in athletes after prolonged activity. Use ofthe abdominal or adductor muscles (eg, running, pivot-ing, and kicking) exacerbates the pain. The patient mayalso report weakness or difficulty ambulating.
A waddling gait may be observed. On examination,hip motion will exacerbate pain, and its range can be
Presentation of Osteitis and Osteomyelitis Pubis as Acute Abdominal Pain
Although theprecise
etiology ofosteitis pubis
remainsunknown,
trauma duringsurgery or
childbirth isresponsible
for mostcases.
67The Permanente Journal/ Spring 2007/ Volume 11 No. 2
CASE STUDY
restricted. The most obvious and specific finding is ten-derness of the pubic bone, superior pubic rami, or in-ferior pubic rami.14
When osteitis pubis is associated with fever, lymphad-enopathy, nausea, vomiting, and anorexia, one mustconsider the concurrent diagnosis of osteomyelitis pu-bis. These symptoms can be easily mistaken for thoseof acute appendicitis.
Laboratory data are not required for the diagnosis ofeither osteitis or osteomyelitis pubis. In the latter theremay be an increased leukocyte cell count and an el-evated sedimentation rate, similar to data found withacute abdominal pain.
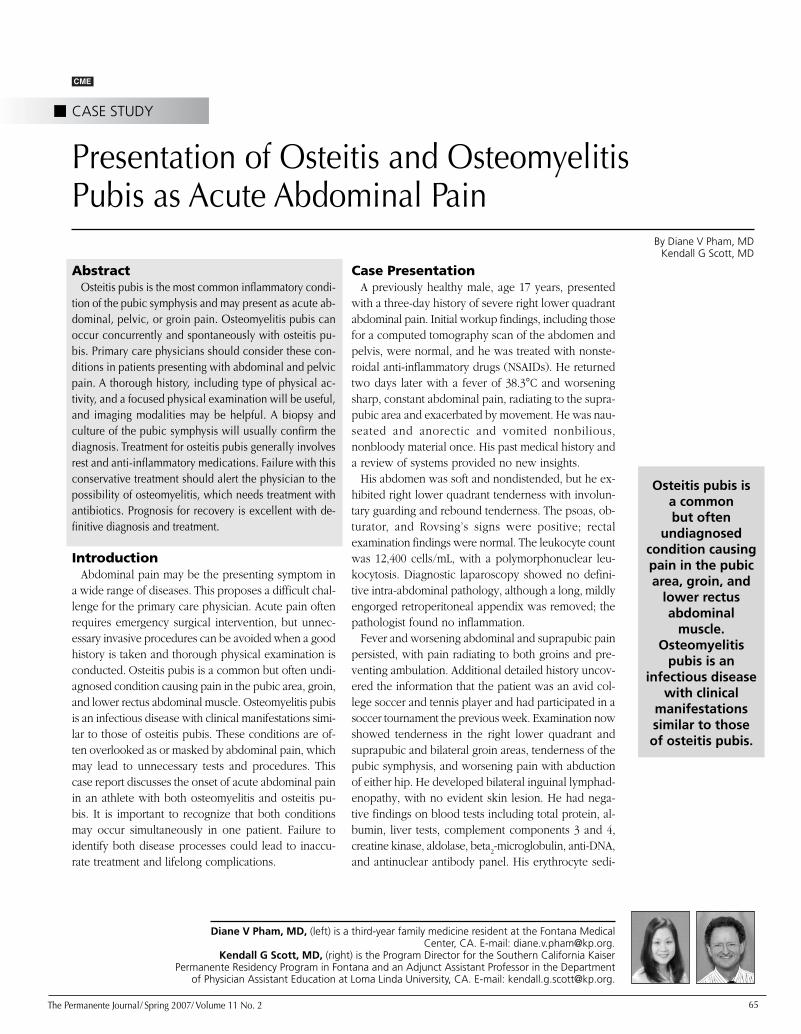
ImagingPelvic radiographs may show irregular borders over
the pubic symphysis and rami. Varying degrees of ar-ticular surface irregularity, erosion, sclerosis, and os-teophyte formation may be present. These findings arenot specific to osteitis pubis and may not be detectableearly. Symphysography, injection of the symphysealcleft with noniodine contrast, is used to view morphol-ogy and potentially provoke symptoms. This proce-dure can confirm osteitis pubis15 (Figure 1).
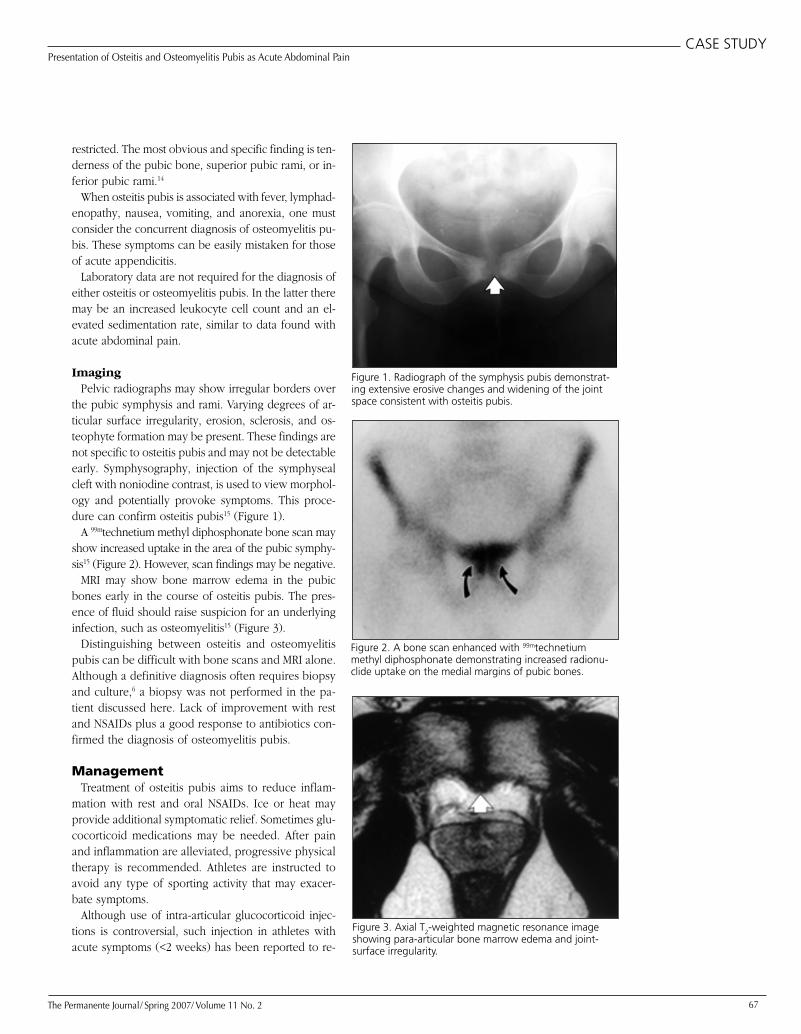
A 99mtechnetium methyl diphosphonate bone scan mayshow increased uptake in the area of the pubic symphy-sis15 (Figure 2). However, scan findings may be negative.
MRI may show bone marrow edema in the pubicbones early in the course of osteitis pubis. The pres-ence of fluid should raise suspicion for an underlyinginfection, such as osteomyelitis15 (Figure 3).
Distinguishing between osteitis and osteomyelitispubis can be difficult with bone scans and MRI alone.Although a definitive diagnosis often requires biopsyand culture,6 a biopsy was not performed in the pa-tient discussed here. Lack of improvement with restand NSAIDs plus a good response to antibiotics con-firmed the diagnosis of osteomyelitis pubis.
ManagementTreatment of osteitis pubis aims to reduce inflam-
mation with rest and oral NSAIDs. Ice or heat mayprovide additional symptomatic relief. Sometimes glu-cocorticoid medications may be needed. After painand inflammation are alleviated, progressive physicaltherapy is recommended. Athletes are instructed toavoid any type of sporting activity that may exacer-bate symptoms.
Although use of intra-articular glucocorticoid injec-tions is controversial, such injection in athletes withacute symptoms (<2 weeks) has been reported to re-
Presentation of Osteitis and Osteomyelitis Pubis as Acute Abdominal Pain
Figure 2. A bone scan enhanced with 99mtechnetiummethyl diphosphonate demonstrating increased radionu-clide uptake on the medial margins of pubic bones.
Figure 1. Radiograph of the symphysis pubis demonstrat-ing extensive erosive changes and widening of the jointspace consistent with osteitis pubis.
Figure 3. Axial T2-weighted magnetic resonance imageshowing para-articular bone marrow edema and joint-surface irregularity.

68 The Permanente Journal/ Spring 2007/ Volume 11 No. 2
CASE STUDY
sult in a more rapid recovery.16 Thus, these injectionsmay help athletes who need to return to competitionwithin one to two weeks.
Surgery is rarely indicated and should be re-served for patients with severe pain or pubic in-stability nonresponsive to conservative therapy.Wedge resection of the symphysis can improveearly symptoms but may lead to later posteriorpelvic instability, requiring another surgical pro-cedure.17 Video-assisted placement of anextraperitoneal retropubic synthetic mesh maysupport the damaged area and accelerate the re-habilitation process for osteitis pubis.18
Osteomyelitis pubis requires identification ofthe organism and treatment with the appropriateantibiotic. Initially antibiotics are given intrave-
nously for two weeks, followed by oral antibiotics forat least six weeks or until the ESR is normalized. Surgi-cal debridement may be required if there is no responseto medical therapy.6 Rest, NSAIDs, and physical therapyare prescribed just as they are for osteitis pubis.
PrognosisOsteitis pubis is a self-limiting condition, but time until
full recovery in athletes ranges from three weeks to 32months (average, nine months). There has been a re-ported 25% recurrence rate and a complete end to sportsactivities in 25% of those affected with osteitis pubis.13
Osteomyelitis pubis is not self-limiting, but when it istreated adequately with antibiotics, the prognosis forrecovery is excellent. Data about the disease’s recur-rence rate in athletes are not available.
ConclusionAbdominal pain can be a challenging problem with
an extensive differential diagnosis. Acute pain canbe misleading and can result in unnecessary inva-sive procedures. Osteitis pubis should be consideredin the differential diagnosis when any patient com-plains of abdominal, pelvic, or groin pain. When painoccurs with fever, osteomyelitis should be suspected.To correctly diagnose these conditions, the primarycare physician must maintain a high index of suspi-cion. When the conditions are recognized, specificconservative treatment can produce quick relief andgood results. ❖
AcknowledgmentKatharine O’Moore-Klopf of KOK Edit provided editorial
assistance.
Presentation of Osteitis and Osteomyelitis Pubis as Acute Abdominal Pain
References1. Beer E. Periostitis of the symphysis and descending rami of
the pubes following suprapubic operations. Int J Med Surg1924 May;37(5):224–5.
2. Andrews SK, Carek PJ. Osteitis pubis: a diagnosis for thefamily physician. J Am Board Fam Pract 1998 Jul–Aug;11(4):291–5.
3. Adams RJ, Chandler FA. Osteitis pubis of traumaticetiology. J Bone Joint Surg 1953 Jul;35-A(3):685–96.
4. Lavelle JL, Hamm F. Osteitis pubis: its etiology andpathology. J Urol 1951;66:418.
5. Sexton DJ, Heskestad L, Lambeth WR, McCallum R, LevinLS, Corey GR. Postoperative pubic osteomyelitismisdiagnosed as osteitis pubis: report of four cases andreviews. Clin Infect Dis 1993 Oct;17(4):695–700.
6. Ross JJ, Hu LT. Septic arthritis of the pubic symphysis:review of 100 cases. Medicine (Baltimore) 2003Sep;82(5):340–5.
7. Burns JR, Gregory JG. Osteomyelitis of the pubic symphysisafter urologic surgery. J Urol 1977 Nov;118(5):803–5.
8. Eskridge C, Longo S, Kwark J, Robichaux A, Begneaud W.Osteomyelitis pubis occurring after spontaneous vaginaldelivery: a case presentation. J Perinatol 1997 Jul–Aug;17(4):321–4.
9. Combs JA. Bacterial osteitis pubis in a weight lifter withoutinvasive trauma. Med Sci Sports Exerc 1998Nov;30(11):1561–3.
10. Netter, FH. Atlas of human anatomy, 2nd ed. EastHanover(NJ): Novartis Medical Education; 1997. p 234–5,456–9.
11. Hannan C, Hall T, Pyne L. Groin pain from a manipulativetherapy perspective. Aust Physiother Assoc Sport PhysiotherGroup 1994;3:10–6.
12. Rodriguez C, Miguel A, Lima H, Heinrichs K. Osteitis pubissyndrome in the professional soccer athlete: a case report. JAthl Train. 2001 Dec;36(4):437–40.
13. Fricker PA, Taunton JE, Ammann W. Osteitis pubis inathletes: infection, inflammation, or injury? Sports Med1991 Oct;12(4):266–79.
14. Morelli V, Espinoza L. Groin injuries and groin painin athletes: part 2. Prim Care Clin Office Pract2005;32:185–200.
15. O’Connell MJ, Powell T, McCaffrey NM, O’Connell D,Eustace SJ. Symphyseal cleft injection in the diagnosis andtreatment of osteitis pubis in athletes. AJR Am J Roentgenol2002 Oct;179(4):955–9.
16. Holt MA, Keene JS, Graf BK, Helwig DC. Treatment ofosteitis pubis in athletes: results of corticosteroid injections.Am J Sports Med 1995 Sep–Oct;23(5):601–7.
17. Grace JN, Sim FH, Shives TC, Coventry MB. Wedgeresection of symphysis pubis for the treatment of osteitispubis. J Bone Joint Surg Am 1989 Mar;71(3):358–64.
18. Paajanen H, Heikkinen J, Hermunen H, Airo I. Successfultreatment of osteitis pubis by using totally extraperitonealendoscopic technique. Int J Sports Med 2005May;26(4):303–6.
Osteitis pubis isa self-limitingcondition, buttime until full
recovery inathletes ranges
from threeweeks to 32months …



![RENTGENOLÓGIA KONÍ [2], [3], [5], [24], [25], [31], [33 ... · 6 Základy zobrazovacej diagostiky psa, ačky a koňa, IVA VFU 2018 REETGEEOLÓGIA KOEÍ Osteitis a osteomyelitis](https://img.pdfslide.net/doc/110x75/5dd09270d6be591ccb61a3f5/rentgenolgia-kon-2-3-5-24-25-31-33-6-zklady-zobrazovacej.jpg)

























