Embed Size (px)
DESCRIPTION
ldskgfdsk;jg
Citation preview

CASE STUDY
I. DEMOGRAPHICAL DATA
Name: E.V.E
Age: 11 years old
Gender: Male
Address: Sitio Ibabaw Dulumbayan, Teresa, Rizal
Civil Status: Single
Date of Birth: Septemr 14, 2001
Place of Birth: Taytay, Rizal
Nationality: Filipino
Ethnic Group: None
Primary Language Spoken: Tagalog
Highest Educational Attainment: Grade 4
Occupation: N/A
Religious Orientation: Roman Catholic
Health Care Financing: Family
A. PRESENT HEALTH HISTORY
The patient was admitted last April 16 at around 8:00 pm due to chief complains of vomiting and episodes of loose stools, specifically 5 times. His admitting diagnosis is Acute Gastroenteritis with mild dehydration due to Amoebiasis. According to the patient’s mother, they went on swimming last April 7 which she thought her son got the infectious agent. Moreover, the patient had been hospitalized for 4 days from now and so he is already in possible discharge.
B. PAST HEALTH HISTORY
According to the patient’s mother, E.V.E have had Amoebiasis before when he was still 6 years old and he was also been hospitalized for 3 days due to it. “Hindi ko na kasi matandaan kung pano siya nagka-Amoebiasis noon, per siguro dahil sa pagkain,” the patient’s mother verbalized. Also, the patient had pneumonia when he was still on his neonatal period but according to his mother, he was no longer manifesting the condition today. The patient has complete vaccinations. He usually got colds and fever at approximately 2-3 times a year and

over the counter medications is their way of treating it. He had also childhood diseases such as chicken pox and mumps. His chicken pox just happened last May 2012 at lasted for more than a week. He had mumps when he was still on Grade 2. He was breastfed up to 2 years of age as his mother stated. Also, he is not taking any vitamins or supplements.
C. FAMILY HEALTH HISTORY
GENOGRAM
D.V G.V (-) old age arthritis D.B W.E (-) DM (-) HPN
E.R.EL.V L.J.V L.R.E (A/W)(A/W) (A/W) (A/W) E.L.E E.M.E (A/W) (DM)
J.E E.E (Patient) E.J.E (A/W) asthma E.V.E (A/W)
The patient’s father is Edmundo 48 years old and his mother, Leah rose is 39 years old. They are both alive and well with no present illnesses according to the patient’s mother. He has 4 siblings. The eldest is Junro, 16 years old male, the 2nd is Edrolyn, 15 years old female, who has asthma, the patient is the 3rd child and the youngest is Edmund Jun, 4 years old. All are alive and well aside from her sister who has asthma. The patient’s grandmother from his mother’s side was already deceased and her gradmother has arthritis. E.V.E’s mother has 3 siblings, she is the youngest and all of them are alive and well. However, his grandparents from his father’s side were already both deceased. Her grandmother died due to Diabetes Mellitus and his grandfather passed away due to Hypertension. His father has also 3 siblings; he is the eldest and the only male in the family and all of them are all alive and well.

II. GORDON’S FUNCTIONAL HEALTH PATTERNS
A. Nutrition
Before Hospitalization:
The patient eats 3 times daily. He loves to eat sweets and salty foods. Usually for breakfast, he eats bread and drink milo. For lunch and dinner they often have vegetable dish and sometimes with meat and fish according to the patient’s mother. “Hindi naman sila namimili ng ulam. Kahit anong ihain kinakain naman nila,” the patient’s mother verbalized. In every meal, the patient drinks 2 glasses of water. They seldom eat out on fast foods or restaurants. His sister often cooks food for them as a family. Sometimes he eats junkfoods and soda for snacks. Also, the patient does not have any food allergies noted. In the past 2 days prior to hospital admission, the patient had difficulty eating. He lost appetite and had vomited several times. He only had lugaw each meal time.
During the hospitalization:
The patient’s appetite is becoming better compared to 2 days prior his hospitalization according to her mother. He eats a lot more compared to the past 2 days before he was admitted. He usually drinks up to 700ml of water daily. He is not nauseated and doesn’t suffer from any gastric upset. However, episodes of vomiting were still noted during the first 2 days of hospitalization. He had several medications; these are as follows, ceftriaxone 500mg TIV q8, Buscupan ½ ampoule TIV, Erceflora 1 tube daily, Paracetamol 7.5ml q4 if with fever, Metronidazole 500mg tablet TID and Zithromax 500mg tablet daily.
Norms:Various daily food guides have been developed to help healthy people meet the daily
requirements of essential nutrients and to facilitate meal planning. Food group plans emphasize
the general types or groups of foods rather than the specific foods, because related foods are
similar in composition and often have similar nutrient values. For example, all grains, whether
wheat or oats, are significant source of carbohydrate, iron, and the B vitamin thiamine. Daily
food guides that are currently used includes Dietary Guidelines for Americans and the Food
Guide Pyramids
(Source: Fundamentals of Nursing. Kozier and Erb. 2008. Pp 1246.)
Interpretation: The patient usually eats vegetables and is not picky. He also drinks water every
time he eats. They do not eat on fast food chains often. So, they prepare their own food; which
is better compared to commercially prepared ones. However, as like other kids of his age he
loves eating junk foods and sweets for snacks. In the morning he consumes mainly
carbohydrates which is good in order to keep him active during the day considering his age
where in he is at playful stage.

B. Rest and Sleep
Before Hospitalization:
The patient has average hours of sleep. He often sleeps at 9:00 pm and wakes up at 8:00am
making it up to 11 hours of sleep in total. However, when he has school, the patient’s mother
said that by 8:00 pm he was already asleep and wakes up at 5:00am. At present, because it’s
summer break, there are no classes the patient also takes a nap at noontime. Usually around
1:00 to 3:00pm. E.V.E also mentioned that he is satisfied with his sleeps and does not have any
disturbances during his resting period. He does not have any difficulty sleeping. He is refreshed
during the day and does not sleepy.
During Hospitalization:
According to the patient, he does not have any difficulty sleeping in the hospital. He still sleeps
at 9:00pm and wakes up at 7 or 8:00am. However, he has slight sleep disturbances as he said,
sometimes when the doctors or nurses checks them in the ward he wakes up; also whenever he
has to take medications, he has to wake up.
Norms: Most healthy children need 10 to 12 hours of sleep a night to function optimally.
(Source: Fundamentals of Nursing 8th edition by Kozier and Erb pp. 1168)
Interpretation:
The patient has adequate sleep and rest because he has a total of 11 hours of sleep at night
and also he mentioned that he also sleeps during noontime. During his hospital admission, he
has minimal disturbances which is appropriate because due medications have to be taken
within the time prescribed and nurses’ checking them at the ward from time to time is inevitable
and it is on purpose of their stay in the hospital.
Elimination
Before Hospitalization:
2 days prior to hospital admission the patient had several episodes of loose bowel movement, 5
times during the day of April 16 to be exact. He described his stools as black and tarry
according to his mother. Usually he urinates 3 times a day and the color of the urine is often
slightly turbid with no foul odor. Also, he does not have any difficulty urinating.

During Hospitalization:
In the first 2 days of hospital admission the patient still have episodes of loose stools though the
frequency is decreasing day by day. During the day assessed, he is already for discharge and
he had his bowel movement once. He does not have any difficulty moving his bowel and the
consistency is not loose anymore. He urinates 4 to 5 times daily and describes the color of his
urine as yellowish with no foul smell. Also, he does not have any problems urinating.
Norms: Voiding or urination all refer to the process of emptying the urinary bladder. This occurs
when the adult bladder contains between 250 and 450 mL of urine. Each person must take 8-10
glasses of water every day. The frequency of defecation is highly individual, varying from
several times per day to two or three times per week. Many people believe that “regularity”
means a bowel movement every day.
(Source: Fundamentals of Nursing 8th edition by Kozier and Erb pp. 1326 and 1325.)
Interpretation: The patient was able to void without any discomfort as reported by him. From
having loose stools, he said that his stools become better than before and that he only moves
his bowel once a day already. So, he no longer has problems regarding his bowel movement
and urination pattern.
C. Health and Illness
The patient describes a healthy individual as a person who is active, playful, happy and does
not have any sickness. He stated, “Syempre kapag wala kang sakit, nakakapaglaro ka at
masaya ka.” He said that he likes all vegetables. He is not picky when it comes to food. “Para
po maging malusog, kelangan kumain ng maraming gulay,” the patient verbalized.
Norms: Health is a highly individual perception. Many people define and describe health as the
following:
• Being free from symptoms of disease and pain as much as possible
• Being able to be active and to do what they want or must
• Being in good spirits most of the time
These characteristics indicate that health is not something that a person achieves suddenly.
(Source: Fundamentals of Nursing. Kozier and Erb. 2008. Pp 295).

Interpretation: Observing the patient’s response, he is right that he should eat a lot because
considering his age. He is active and quite playful. Thus, eating a lot will give him energy to
sustain in his activities during the day. Parents with school aged children do have a hard time
having their child eat vegetables because they prefer processed foods such as hotdogs and
sausages but the patient said that he eats vegetables and that he is not picky which is again
appropriate in having a proper balanced diet.
Activity/ Exercise
The patient’s daily activities are mainly outside playing with his playmates. He said he plays
basketball and other outdoor games. He often goes biking with his playmates around the vicinity
of their place during the afternoon. He also plays computer games but not usually because he
said his mother does not give him money sometimes to pay in the computer shop.
Norms: Make an activity or exercise for at least 30 minutes.
(Fundamentals of Nursing 8th edition by Kozier and Erb pp. 1105)
Interpretation: The patient is active, he is outside all day often and so his lifestyle is not
sedentary.
III. PHYSICAL ASSESSMENT
A. Initial Vital Signs
Time: 8:00am
Date: April 20, 2013
Temp: 36.0°C / Axillary
PR: 92 beats/minute= regular; strong
RR: 21 cycles/minute= regular;shallow
BP: 90/60 mmHg
Norms: For the body to function on a cellular level, a core body temperature between 36.5°C and 37.7°C must be maintained.
(Source: Health Assessment in Nursing. Weber and Kelley. Third Edition.)

Pulse rate of adults ranges from 60- 100 beats/minute. A normal adult inspiration lasts 1 to 1.5 seconds and an expiration lasts 2 to 3 seconds. A typical blood pressure for a healthy adult is 120/80.
(Source: Fundamentals of Nursing. Kozier and Erb. 2008. )
Interpretation: The patient’s vital signs are within the normal range and are stable.
B. General Appearance
Actual Findings: The patient has a dark even complexion with no presence of
hyperpigmentation and lesions on skin. He wears appropriate clothing to situation and weather.
His nails on toes are a bit long. Since his hospital admission, he never took a bath just sponge
bath. However, he does not have any foul odor. He is conscious, cooperative and coherent. He
responds to my questions promptly during the interview. He is also aware of person, place and
time.
Norms: Color is even without obvious lesions: light to dark beige-pink in lighted skinned client;
light tan to dark brown or olive in dark-skinned clients. Dress is appropriate for the occasion and
weather. The client is clean and groomed appropriately for occasion. Stains on hands and dirty
nails may reflect certain occupations such as mechanic or gardener. Client is cooperative and
purposeful in his or her interactions with other. Affect is appropriate for the client’s situation.
(Source: Health Assessment in Nursing. Weber and Kelley. Third Edition.pp.)
Interpretation: In general appearance, the patient looks not properly groomed because he
didn’t take a bath for days. Nevertheless, he is very cooperative in participating during the
interview. His thoughts are appropriate to the situation and he is in a good mood because he
knew he is on possible discharge. Thus, the patient is somewhat aware and oriented to person,
place and time
C.HEENT
Actual Findings:
S: The patient stated, “Hindi naman po sumasakit ang ulo ko. Malinaw ang mga mata ko. Hindi
din po ako bingi, naririnig naman kita ng maayos.”
O: The patient’s head is normocephalic, round and symmetrical. His hair is evenly distributed,
dyed in brown color. The scalp is lighter in color than the skin color. His face is uniform in color

and temperature with a scar on the forehead. His eyebrows are black in color and aligned; eye
lashes are curled outward; the eyelids blink bilateral; pink conjunctiva; the cornea is shiny,
transparent and equal in size; pupils are black in color; he can move his eyes without any
discomfort. Both ears have the same color with the patient’s face and aligned to the outer
canthus of the eye; pinna moves back when palpated; there is a presence of cerumen on both
ears, and it is yellowish in color. He can hear well because he responds to my questions
attentively during the interview. His nose is at the center and is symmetrical; uniform in color,
and has patent airways. The patient can breathe freely on both nares. The lips is pinkish in
color; the teeth are white; no missing teeth and tooth decays noted; the tongue is also pinkish in
color as well as the gums, uvula, soft and hard palate.
Norms: The skull is round, normocephalic and symmetrical with frontal, parietal, and occipital
prominences. Smooth skull contour. Hair is evenly distributed, thick hair, silky, resilient hair, no
infection and no infestations. Eyebrows are evenly distributed; skin intact, eyebrows
symmetrically aligned, equal movements. Eyelashes are equally distributed and curled slightly
outward. Bulbar conjunctiva is transparent, capillaries sometimes evident, sclera appears white.
Ears are mobile, Firm, and not tender, Pinna recoils after it is folded. Color same as facial skin,
symmetrical, auricle aligned with outer canthus of eye, about 10 degrees from vertical. Nose is
symmetric and straight, no discharge or flaring, uniform color. Lips is uniform pink in color. 32
adult teeth; smooth shiny white teeth; pink gums; moist, firm gum texture. Light pink, smooth
palate. Lighter pink hard palate and more irregular in texture. Tongue in central position, pink
color, no lesions, raised papillae, moves freely with no tenderness.
(Source: Health Assessment in Nursing. Weber and Kelley. Third Edition.)
Interpretation: In the HEENT assessment, most of the results are considered to be normal
based on the norms. However, the patient’s hair for instance is not, for the patient admitted he
dyed his hair making it brown in color. Though he doesn’t have missing tooth or tooth decays,
his teeth are not all permanent some are temporary.
C. Chest and Back
Actual Findings:
S: E.V.E verbalized, “Hindi naman po sumasakit ang dibdib ko, pati na din ang likod ko hindi
naman nangangalay o sumasakit. Hindi rin ako nahihirapang huminga.”

O: The chest is symmetric and expands as he breathes. His respiration is quiet rhythmic,
effortless and has 21 cycles in one full minute. The skin is intact and the temperature is even.
Norms and Standards: Chest is symmetric. Breasts are not tender when palapated, slightly
unequal with no presence of mass and/or lesions. Skin intact and uniform temperature. Full and
symmetric chest. Fremitus is heard most clearly at the apex of the lungs. Percussion notes
resonate, except over scapula lowest point of resonance is at the diaphragm and vesicular and
bronchovesicualr breath sounds.
(Source: Fundamentals of Nursing. Kozier and Erb. 2008.)
Interpretation: There are no deviations from normal noted.
D. Abdomen
Actual Findings:
S: “Hindi na po sumasakit ang aking tyan. Nakakakain ako ng marami at hindi na ko nagsusuka
buhat nung isang araw pa.”
O: The patient’s abdomen is round, uniform in color with no lesions noted.
Norms: Unblemished skin, uniform color, no lesions, silver-white striae or surgical scars. Flat,
rounded or scaphoid. No evidence of liver/spleen enlargement. Symmetric contour. Symmetric
movements caused by respiration. Visible peristalsis in very lean client.
(Source: Health Assessment in Nursing. Weber and Kelley. Third Edition.)
Interpretation: The patient’s abdomen has no deviation from normal findings noted.
E. Extremities
Actual Findings:
S: “Hindi naman po masakit at nangangalay ang mga binti at braso ko.”
O: The patient has smooth coordinated movements; he can move his extremities without any
discomfort. His muscle tone is equal in both upper and lower extremities. The skin’s
temperature and color are uniform.

Norms and Standards: Equal size on both sides. No fasciculation/tremors. Joint moves
smoothly. Normally firm. Smooth coordinated movement. Equal strength on both sides. No
swelling, no tenderness, no nodules.
(Source: Health Assessment in Nursing. Weber and Kelley. Third Edition.)
Interpretation: The client can move his extremities without any discomfort. Thus, there are no
deviations from normal noted.
IV. LABORATORY RESULTS
Hematology
Examination: Ref. Values
Hemoglobin 133gll 125-160
Hematocrit 0.40 0.38-0.50
RBC 4.79x10/L 4.5-6.2(M)
4.5-5.5(F)
Leukocyte 21.3 x10/L 5-10
Stab 0-0.1
Neutrophil 0.84 0.40-0.60
Eosinophil 0.01-0.06
Basophil 0-0.01
Lymphocyte 0.06 0.20-0.40
Monocyte 0.20-0.40
ESR
Platelet count x10/L 150-350
Reticulocyte x10/L 5-15
Bleeding Time 2-4 minutes

Clotting Time 2-6 minutes
Clot ret. Time
Protime
Patient secs
Control secs 12-14 secs
% Activity % 70-100%
INR
APTT Secs
Control Secs
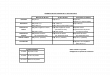
Norms Interpretation
Hematology Result04.13.07
Result04.20.07
NormalValues
Increased Decreased
WBC 14.43 x109/L
16.03 x109/L
5–10 x109/L
◊ Infection◊ Inflammation◊ Trauma
◊ Autoimmunedisease◊ Drug toxicity◊ Bone marrowfailure
Neutrophil 0.01 0.62 0.55-0.65
◊ stress◊ acuteinfection
◊ aplastic anemia◊ dietary deficiency
Lymphocytes 0.83 0.31 0.25-0.35
◊Chronicinfection◊ Viral Infection◊Mononucleosis
◊ Leukemia◊ Sepsis◊Immunodeficiency\diseases
Eosinophils 0.01 0.03 0.02-0.07
◊ Parasiticinfections◊ Allergicreactions
◊ IncreasedAdrenosteroidproduction

◊ Leukemia
Hemoglobin 101.1 g/L 110.7 g/L 116-140g/L
◊ Polycythemia◊ Dehydration◊ COPD
◊ Hemorrhage◊ Anemia◊ Cancer◊ Kidney disease◊ Sickle Cell
Anemia
Hematocrit 0.32 0.34 0.35-0.41
◊ Polycythemia◊ Dehydration◊ COPD
◊ Hemorrhage◊ Anemia◊ Hyperthyroidism◊ Dietary deficiency
Platelet 365 x109/L
615 x109/L
150-350x 109/L
◊ Malignantdisorder◊ Polycythemia◊ RheumatoidArthritis◊ IronDeficiencyAnemia
◊ Hemorrhage◊ Leukemia◊ Pernicious anemia◊ Hemolytic anemia◊ Chemotherapy
RBC 4.76 x1012/L
5.28 3.0 -5.0x1012/L
◊ Dehydration◊ Pulmonaryfibrosis
◊ Hemorrhage◊ Anemia◊ Dietary deficiency
(Source:http://cdn.nursingcrib.com/wpcontent/uploads/case%20study/
labhypertension.pdf )
FECALYSIS
COLOR: Greenish yellow
CONSISTENCY: mucoid
PARASITES:
AMOEBA: positive for E. Histolytica cyst.

CYST:
TROPHOZOITE:
PUS CELLS: 35-40/rpf
RBC: 3-6/rpf
OTHERS: bacteria: many
Norms:
Normal Findings Interpretation
Color brown normal
Consistency soft and bulky, small
and dry, depending
on the diet
normal
Parasite none (+)infection(-)normal
Pus Cells none (+)infection(-)normal
Bacteria none (+)infection (-)normal
Red Cells 0-3 normal
(Source: http://healcon.com/health-book/health-condition/fecalysis-norms-
_AQZ5AGquLGLjKmVjAwRmAmL=.htm)
ELECTROLYTES
RESULTS UNIT REF. VALUE
SODIUM 136.5 mmol/L 135-140
POTASSIUM 3.6 mmol/L 3.5-5.5
CHLORIDE 98-107

Norms:
Normal Findings Interpretation
Sodium 135-145 <145 mmol/L: Hypernatremia
An excess in sodium levels in
the blood in relation to water
is called 'hypernatremia'.
Causes of hypernatremia may
include kidney disease, lack
or little water intake or loss of
water due to diarrhea and/or
vomiting.
>135 mmol/L: Hyponatremia
A decrease in sodium levels in
the blood in relation to water
is called 'hyponatremia'. This
occurs when there is an
increase in the amount of
body water in relation to
sodium. This occurs with
diseases of the liver, kidney,
burn victims and those who
suffer from congestive heart
failure and other conditions.
Potassium 3.5-5 <3.5mmol/L: hypokalemia
>5 mmol/L: hyperkalemia
An abnormal increase in
potassium (hyperkalemia) or a
decrease in potassium
(hypokalemia) can seriously
affect the nervous system and
increases the chance of
arrhythmias.
Chloride 98-107 <107 mmol/L: hyperchloremia

Increased chloride levels is
'hyperchloremia'. Elevated
levels are seen in diarrhea,
some kidney disease and
sometimes in overactive
parathyroid glands.
>98 mmol/L: hypochloremia
Decreased chloride levels is
'hypochloremia'. Chloride is
normally lost in the urine,
sweat and stomach secretions
but an excessive loss can
happen from heavy sweating,
vomiting and adrenal gland or
kidney disease.
Calcium(ionized) 4.5-5.5 <5.5: hypercalcemia
LOW:
muscle twitching and
cramping
seizures
varying degrees of depression
hair loss
cataracts
conjunctivitus (inflammation of
the mucuos membrane of
inner eyelid)
>4.5: hypocalcemia
HIGH:
muscle weakness
fatigue
abdominal cramps
loss of appetite
nausea and /or vomiting
constipation

possible coma if left untreated
Magnesium 1.5-2.5 <2.5: hypermagnesemia
>1.5: hypomagnesemia
Signs and symptoms
associated with abnormal
levels:
decreased mental function
ranging from drowsiness to
coma in severe states
decreased tendon reflex
leading to paralysis
Nausea / vomiting
hypotension due to dilated
blood vessels
Phosphate 1.7-2.6 <2.6mmol/L:
hyperphosphatemia
Causes of increased
phosphate leves are due to
excess vitamin D, impaired
colon motility,
hypoparathyroidism, addisons
disease and increased intake
of phosphate foods
>1.7 mmol/L:
hypophosphatemia
Causes of decreased
phosphate are due to
malnutrition, excess use of
antacids, cushing syndrome,
and hyperparathyroidism
Signs and Symptoms:
Decrease cardiac respiratory
function
Muscle weakness

Fatigue
Confusion
Seizures
Bone pain
(Source: http://www.mdhealthnetwork.org/Blood-Tests-Electrolytes.htm)
V. DRUG STUDY
Home Medications
Name Dosage Action Indication Contraindication
Side Effects Nursing Responsibilities
Generic:AzithromycinBrand name:ZithromaxDrug Class:Macrolide antibiotic
500 mg/1 tab OD for 3 days
Azithromycin is an antibiotic (macrolide-type) used to treat a wide variety of bacterial infections. It works by stopping the growth of bacteria.This antibiotic treats only bacterial infections. It will not work for viral infections (e.g., common cold, flu).
Indicated for the treatment of patients with mild to moderate infections caused by susceptible strains of the designated microorganisms.
Ketolide or related allergy.
GI upset, abdominal pain, rash, chest pain; hepatotoxicity, allergy (eg, angioedema, cholestatic jaundice), C. difficile associated diarrhea.
Inform patient not to share medicationsDo not take drug with food or antacidsTake antacids 2h before or after taking the drugDirect sunlight (UV) exposure should be minimized during therapy with drug or patient might use sunblockReport immediately if onset of diarrhea occurs
Generic: 500 mg 1 Metronidaz Acute History of GI Take full

MetronidazoleBrand name:FlagylDrug Class:Anti-infectives,Anti-protozoals
tab for 7 days
ole is converted to reduction products that interact with DNA to cause destruction of helical DNA structure and strand leading to a protein synthesis inhibition and cell death in susceptible organisms. It is effective against a wide range of organisms including E. histolytica, T. vaginalis, Giardia, anaerobes e.g. Bacterioides sp, Fusobacterium sp, Clostridium sp, Peptococcus sp and Peptostreptococcus sp, and moderately active against Gardnerell
infection with susceptible anaerobic bacteriaAcute intestinal amebiasisAmebic liver abscessTrichomoniasis (acute and partners of patients with acute infection)Preoperative, intraoperative, postoperative prophylaxis for patients undergoing colorectal surgeryTopical application: Treatment of inflammatory papules, pustules, and erythema of rosacea
hypersensitivity to metronidazole or other nitroimidazole derivatives. Pregnancy (1st trimester) and lactation.
disturbances Furred tongue, glossitis, and stomatitis due to overgrowth of Candida. Weakness, dizziness, ataxia, headache, drowsiness, insomnia, changes in mood or mental state. Numbness or tingling in the extremities, epileptic form seizures (high doses or prolonged treatment). Transient leucopenia and thrombocytopenia. Hypersensitivity reactions. Urethral discomfort and darkening of urine. Raised liver enzyme values, cholestatic hepatitis, jaundice. Thrombophlebitis (IV).
course of drug therapy; take the drug with food if GI upset occurs.Do not drink alcohol (beverages or preparations containing alcohol, cough syrups); severe reactions may occur.Your urine may be a darker color than usual; this is expected.Refrain from sexual intercourse during treatment for trichomoniasis, unless partner wears a condom.Apply the topical preparation by cleansing the area and then rubbing a thin film into the affected area. Avoid contact with the eyes. Cosmetics may be applied to the area after application.You may experience these side effects: Dry mouth with strange

a sp and Campylobacter sp.
metallic taste (frequent mouth care, sucking sugarless candies may help); nausea, vomiting, diarrhea (eat frequent small meals).Report severe GI upset, dizziness, unusual fatigue or weakness, fever, chills.
Generic:Bacillus ClausiiBrand name:ErcefloraDrug class:Antidiarrheals
1 vial of 2 billion/ 5 ml suspension
Contributes to the recovery of the intestinal microbial flora altered during the course of microbialdisorders of diverse origin. It produces various vitamins, particularly group B vitamins thus contributingto correction of vitamin disorders caused by antibiotics & chemotherapeutic agents.
Acute diarrhea with duration of ≤14 days due to infection, drugs or poisons. Chronic or persistent diarrhea with duration of >14 days.
Not for use in immunocompromised patients (cancer patients on chemotherapy, patients takingimmunosuppressant meds)
No known side effects
Shake drug well before administrationAdminister drug within 30 minutes after openingDilute drug with sweetened milk or fruit juiceAdminister per oremMonitor patient for any unusual effects from drug

Promotesnormalization of intestinal flora.
VI. PATHOPHYSIOLOGY
Infective cysts are ingested through water or food contaminated with infected feces. The cysts travel through the digestive track until the small intestine. There, excystation occurs, forming a motile trophozoite. It then travels to the large intestine and colon. Here the infection can follow either of two phases: pathogenic and non-pathogenic.
In the pathogenic phase, the virulent trophozoite invades the gut, intestinal lumen, and sometimes the mucosa. Here they kill epithelial cells, neutrophils, and lymphocytes. In the process, they destroy tissues and cells, and produce colitis. Occasionally they manage to enter the capillaries, where they can be transported to the liver, lungs, or the brain. Once in those organs, the parasite can cause abscesses. The abscesses may subsequently burst, releasing many trophozoites which can re-enter the lumen. After feeding, the trophozoites extrude all

ingested material and binary fission occurs. They “round up” and form cysts, where they areresistant to the environment. The cysts pass through the digestive system and are contained in the feces. In feces, they can live anywhere from2-5 weeks, waiting for a new host.
In the non-pathogenic phase, the trophozoites feed on bacteria and detritus from the outer lining of the gut. They do not invade the membrane, and do not form ulcers or abscesses. After feeding, they round up and form cysts, as in the pathogenic phase.
(Source: http://nursingcrib.com/case-study/amoebiasis-amebiasis-amoebic-dysentery-case-study/)
VII. PRIORITIZED LIST OF PROBLEMS
Nursing Diagnoses Cues Rationale
Readiness for enhanced
self-care
S: “Gusto ko na pong maligo pero sabi ng nanay ko sa bahay na lang daw namin kase uuwi na naman daw kami.”
-to assist client in maintaining
responsibility for planning and
achieving self-care goals/general well
being
-to support client in making healh-
related decisions and pursuit of self-
care practices that promote helth to
foster self-esteem and support positive
self-concept.
-to encourage communication among
those who are involved in client’s
health promotion.
-to provide accurate and relevant
information regarding current and
future needs.
-to maintain general health and
physical well being
-to remain free of preventable
complications
-to control feelings of anxiety and help
patient manage the situation

Risk for Infection
Risk for deficient fluid
volume
Risk factors:
Immunosuppression
Antibiotic Therapy
Increased environmental exposure to pathogens
Insufficient knowledge to avoid exposure to pathogens
Risk factors:
Excessive losses through normal routes (e.g Diarrhea)
Oral fluid intake of 6 glasses per day
-to identify etiology/precipitating factors
-to note signs and symptoms of sepsis
-to demonstrate behaviors or lifestyle
changes to prevent development of
infection
-to avoid reoccurrences of the condition
-to identify risk factors and appropriate
interventions
-to demonstrate behaviors or lifestyle
changes to prevent development of
fluid volume deficit
(Source: NANDA 11th edition)

REFERENCES:
Weber and Kelly: Health Assessment in Nursing 3rd Edition
Kozier and Erb (2008): Fundamentals of Nursing 8th Edition)
Doenges, Moorhouse and Murr: Nurse’s Pocket Guide 11th edition
Source:http://cdn.nursingcrib.com/wpcontent/uploads/case%20study/labhypertension.pdf
Source:http://healcon.com/health-book/health-condition/fecalysis-norms_
AQZ5AGquLGLjKmVjAwRmAmL.htm
Source: http://www.mdhealthnetwork.org/Blood-Tests-Electrolytes.htm
Source: http://nursingcrib.com/case-study/amoebiasis-amebiasis-amoebic-dysentery-case-study/

VIII. NURSING CARE PLAN
Nursing Diagnosis
Analysis Goal and Objectives
Nursing Intervention
Rationale Evaluation
Readiness for enhanced self-care
Subjective:The patient verbalized, “Gusto ko na pong maligo pero sabi ng nanay ko sa bahay na lang daw namin kase uuwi na naman daw kami.”
Goal:After 8 hours of nursing interventions, the client will be able to maintain responsibility in achieving proper self-care
Objectives:
After 30 minutes of nursing intervention, the client’s condition will be monitored
After 5 minutes of nursing intervention, the client will be able to identify the importance of
Administer medications as ordered
Vital signs taken and recorded
Performed initial thorough assessment
Discuss to the client the importance of maintaining
To promote faster healing
To note any changes in the vital signs
To obtain baseline data
To promote maintenance of good proper
Goal was met as evidenced by healing of the skin rashes as evidenced by visual disappearance of the rashes and a rate of 0 in itchiness from a scale of 1-10.

maintaining good proper hygiene
After 10 minutes of nursing interventions, the client will be able to demonstrate ways in achieving proper hygiene
After 15 minutes of nursing
good proper hygiene
Provide ways to the client on how to achieve good proper hygiene
Initiate daily bathing and good grooming
Promote handwashing before and after eating and voiding
Encourage client to keep nails clean and short
Assist patient in developing
hygiene
To help the client learn ways on how to achieve good proper hygiene
To promote comfort
To remove dirt and prevent contamination and transmission of microorganisms
To prevent transmission of microorganisms into the body
To prevent re-

intervention, the client will be able to participate in prevention measures and treatment program
programs for preventive care
Encourage client to avoid consumption of such food and water if in doubt of its preparation
Instruct the client’s guardian to report in cases of vomiting and diarrhea
Inform the medications to be taken at home and its specific considerations
Promote the importance of compliance to home
occurence of the condition and further complications
To avoid ingestion of infectious agents
To monitor signs and symptoms of Amoebiasis
To promote timely healing
To enhance effect of treatment program

In another 10 minutes of nursing interventions, the client will be able to show willingness to participate in health promotion
medications
Inform the client’s guardian the importance of follow up visits
Encourage client that maintaining good proper hygiene is a key role in health promotion
Offer support
To promote commitment, optimizing better outcomes
To enhance understanding and cooperation
To reduce anxiety and boost self-esteem