Embed Size (px)
Citation preview

Catherine Bull M.S.N, P.N.P-CClinical Coordinator, Pediatric and Adult Congenital Cardiac Surgical ServicesDepartment of Cardiothoracic SurgeryNYU Medical Center

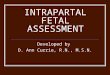
Qp Pulmonary blood flow~ 1 cup
Qp:Qs ratio is the amount of blood going to the lungs compared to the amount of blood going to the body.
Qp : Qs (LUNGS : BODY)
Qp : Qs 1 : 1
Qs Systemic blood flow~ 1 cup

Blood flow to the body or the lungs is not 100% ductal dependent

Transposition of the Great Arteries
Truncus ArteriosusTotal Anomalous Venous return

TGA : Aorta arises
from the anatomic RV
PA arises from the anatomical LV
NORMAL


• Parallel circulations• Mixing can occur at
PFO, PDA or VSD• Most mixing occurs at
the PFO• Without a mixing:
– cyanosis, hypercarbia, tachypnea, tachycardia and acidosis may occur
nn

To increase SaO2 you must increase mixing: PGE to
open duct BAS Volume Oxygen
PDAPDA PFOPFO
NORMAL


Arterial Switch The aorta and the PA
are transected and the coronary arteries are removed.
The aorta and the coronary arteries and attached to the neoaortic root
PA is attached to the neopulmonary root


Decreased LV function Coronary ischemia Nitroglycerine/Heparin
▪ Usually a surgical problem In older patients with IVS whose LV only
exposed to pulmonary pressures pre-operatively
Decreased cardiac outputArrhythmias

Failure of pulmonary veins to connect to the to the LA
Blood from both the systemic and pulmonary venous systems return to the RA the RA, RV & pulmonary
arteries enlarge to compensate for the increased volume
An ASD is essential for CO and always present
NORMAL

Supracardiac: pulmonary veins attach to SVC.
NORMAL

Cardiac: pulmonary veins attach directly to the heart via RA or coronary sinus
NORMAL

Infracardiac: pulmonary veins attach below the diaphragm. Prone to obstruction.
NORMAL

• Unobstructed:Unobstructed:– May be asymptomatic at first– CHF, FTT & frequent upper
respiratory infections will occur
SupracardiacSupracardiac
InfracardiacInfracardiac
• Obstructed:Obstructed:― Profound cyanosis within
the first few hours of life ― Typical “ground glass”
CXR― No PGE― Surgical Emergency

CXR: Typical “ground
glass” appearance of lung fields
Small heart

Attach pulmonary vein confluence to posterior LA and close the ASDLigate the vertical vein

•Create a large ASD and baffle veins from the RA to LA

Unroof coronary sinus and baffle pulmonary venous return to the LA

•Attach pulmonary vein confluence to posterior LA•Ligate the vertical vein•Close the ASD

Low cardiac output: Noncompliant LV. Treated w/ inotropes. Avoid aggressive volume overload-unresolved
LA hypertension & PHTN. PHTN:
r/o pulmonary venous obstruction. Ventilation, O2, NO & sedation to decrease PVR.
Respiratory failure: Due to obstructed veins preop and resultant
pulmonary vascular congestion. Treated with mechanical ventilation, paralysis,
sedation, PEEP & possibly ECMO. Re obstruction
occurs in 10% of patients-usually obstructed infracardiac type

CHF, mild cyanosis & FFT within the first month of life.
Can develop pulmonary hypertension by 3 months.
NORMAL

The pulmonary arteries are excised from the truncus
RV to PA conduit placed
VSD is closed in a manner in which the truncal valve recieves blood from the left ventricle

PHTN: preop overcirculation results in PA
pressures=>Paralyze, sedate, O2 and NO. Low CO:
RV dysfunction=> volume (need a high CVP), inotropes & vasodilators.
Cyanosis: RL PFO =>will resolve with RV function.

Pulmonary blood flow is ductal dependant

Tetralogy of Fallot
Pulmonary Atresia
w/ Intact Ventricular
Septum
Tricuspid Atresia
Regular Pulmonary Atresia Real Pulmonary Atresia Pulmonary Atresia w/ MAPCA’s

TOF is characterized by 4 cardiac anomalies: Ventricular septal defect Pulmonary stenosis or
pulmonary atresia/right ventricular outflow tract obstruction (RVOTO)
Overriding aorta Right ventricular
hypertrophy

Hemodynamics depends on the amount of PS and the size of the VSD Severe PS: Cyanotic
▪ RL shunt▪ Qp<Qs
Mild PS: Pink Tet▪ LR shunt▪ Qp>Qs▪ CHF
NORMAL

Patch closure of VSD Relieve RVOTO
Resect muscle below the valve
Enlarge the pulmonary artery above the valve
OR transannular patch
with removal of valve


• RV dysfunction– Inotropes – May have pleural effusions (esp. right) and ascites
• Junctional Eptopic Tachycardia– PREVENTIONPREVENTION– keep HR low with cooling, no chronotropic drugs,
sedation– Amiodarone
• CyanosisCyanosis– due to right to left shunt across PFO if present
• Pulmonary insufficiency– all patients with transannular patch
• Residual VSD– not well tolerated
• Residual RVOTO– well tolerated

Pulmonary valve & main pulmonary artery are atretic
Pulmonary blood flow is supplied by PDA (most
common) multiple
aortopulmonary collateral arteries (MAPCAs)
TOF/PATOF/PA
TOF/PA w/ MAPAC’sTOF/PA w/ MAPAC’s

Blalock-Taussig Shunt followed by full repair later in infancy

Pulmonary valve atresia with no VSD
Hypoplastic RV (Variable) Size of the RV is determined
by the size of the TV High RV pressure RV sinusoids (Variable)
May form due to high RV pressure.
Steal coronary blood flow from CA
NORMAL

RV SinusoidsRV Sinusoids

Need to do 2 things: establish pulmonary blood flow and get the RV to grow Pulmonary valve balloon angioplasty
▪ Works best when the leaflets of valve are only fused
BTS Transannular patch

2 Ventricle Repair (Adequate RV without sinusoids) Balloon angioplasty +/- BTS
1 ½ Ventricle Repair (Borderline RV +/-sinusoids) +/- Balloon angioplasty BTS +/- Transannular patch
Single Ventricle Repair (Inadequate RV +/- sinusoids) BTS

Borderline RV +/-sinusoids: BTS & transannular patch
to allow pulmonary insufficiency and subsequent RV growth.▪ Adequate RV growth:
complete repair▪ Inadequate RV growth:
Bidirectional Glenn procedure (1 ½ ventricle repair)

The tricuspid valve is absent w/ no communication between the RA and RV
Results in RV and PA hypoplasia and a single left ventricle
NORMAL

No VSD, PA, hypoplastic RV Pulmonary blood flow is ductal dependant
Small VSD, hypoplastic PV, hypoplastic RV (most common) Pulmonary blood flow is ductal dependant
Large VSD, small to adequate PV & RV Qp:Qs is variable

Cyanosis, hypoxemia and metabolic acidosis usually occur within the first few days of life if pulmonary blood flow is not adequate and the PDA closes. Qp<Qs
Management strategies should be aimed at balancing pulmonary and systemic blood flow to maintain Qp=Qs.

Blalock Taussig Shunt Pallative shunt
between the right innominate artery and the RPA that provides pulmonary blood flow.
Variable Qp:Qs

Blood flow to the body is ductal dependant

Coarctation of the Aorta Interrupted Aortic Arch Hypoplastic Left Heart Syndrome

Systemic blood flow is ductal dependant
Blood to the upper body comes from the LV & aorta: pre-ductal sats are higher
Blood to the lower part of the body comes from the PA and PDA: post-ductal sats are lower
Decreased peripheral perfusion & metabolic acidosis if duct closes
NORMAL

Type A= awayType BType C= close

End-to-end anastomosis w/ PDA ligation

Pulmonary hypertension
Issues related to DiGeorge Syndrome
Recurrent laryngeal nerve palsy
Pherenic nerve damage
Recurrent stenosis at site of repair


Underdevelopment of the left side of the heart due to:1. Mitral stenosis/atresia2. Aortic stenosis/atresia 3. Hypoplastic left
ventricle4. Hypoplastic aortic arch
100% of systemic blood flow is ductal dependent
NORMAL

The amount of blood flow to the pulmonary and systemic circulations depends on the relationship between SVR & PVR
As PVR falls blood will naturally go to the lungs & away from the body
NORMAL

• 1st few days of life: well appearing baby (Qp=Qs) Sat 80% Pink and warm
• As the ductus closes blood flows into the lungs resulting in CHF and decreased cardiac output. (Qp>Qs 3:1) Sat >90%– Ashen, tachypeanic, cool, difficulty feeding
• There is progressive deterioration resulting in pulmonary edema and cardiogenic shock. (Qp>>Qs 5:1)– Metabolic acidosis, cold & gray

Prevent the natural progression Lower the systemic vascular resistance Give extra circulating blood volume
The sick neonate requires aggressive intervention Goal is to re-establish systemic perfusion
(Qp:Qs=1) and provide blood flow to the systemic organs▪ Lower the systemic vascular resistance▪ Give extra circulating blood volume

BT ShuntBT Shunt Sano ShuntSano Shunt
1. Creation of Neoaorta
2. Oversew MPA
3. Atrial septectomy
4. BTS/Sano

Patient Management

Systemic blood flow is grossly indicated by Lactate and BE/BD on ABG. BD < -2 or Lactate > 2 indicates
metabolic acidosis and too little systemic blood flow.
BE > 0 or Lactate < 2 indicates adequate systemic blood flow.
Pulmonary blood flow is indicated by PaO2 on ABG. PaO2 > 50 indicates too much PBF PaO2 < 30 indicates too little PBF

O2 Sats = pulmonary blood flow (gross measurement)
O2 Sat 80%= Qp:Qs of 1:1 Sats > 90%: too much pulmonary blood
flow Sats < 75%: too little pulmonary blood
flow
O2 Sats in patients with single ventricle physiology tell you how much blood is going to the lungs-not necessarily how well the lungs are working.

(ABG sat) (VBG sat)
Ao Sat SVO2 Qp/Qs= 80% - 60% =20=1
100% - 80% 20 1PV sat PA sat(Assumed) (ABG sat)

Not enough cardiac output Sats>90% Poor peripheral perfusion Cool extremities Tachypnea Diaphoresis Poor weight gain “Norwood gray”

Too little pulmonary blood flow Sats < 75% Bounding pulses Cyanotic with good perfusion “Blue is better than gray!”

What affects Qp:Qs? Systemic vascular
resistance (SVR) Pulmonary vascular
resistance (PVR)

Always Remember BLOOD FLOWS THE PATH OF LEAST RESISTANCE
• Too little cardiac output Lactate > 2.5, Sats>90%, PaO2 > 50
decrease the SVR or increase PVR
• Too little pulmonary blood flow Sats<75%, PaO2 < 30
decrease the PVR or fill the tank*be very careful of increasing SVR in patients with
single ventricle physiology— DON’T DO IT!

The easiest way to increase CO is to vasodilate the patient
Other ways to manipulate PVR & SVR Temperature FiO2 Ventilator changes Sedation

Factors that PVR Factors that PVRHypoxia PaO2 (NITROGEN) Hyperoxia PaO2 (OXYGEN)Hypoventilation PaCO2 Hyperventilation PaCO2 Hypothermia Normothermia
Agitation Analgesics
Factors that SVR **Factor that SVR**Hypothermia NormothermiaAgitation Analgesics/sedationCatecholamines (high dose dopa, epi) Vasodilators (Milrinone)
NO

In all post-op patients w/ single ventricle physiology you MUST do two things ….
1. Ask yourself “is the patient warm, well perfused and non-acidotic?” If so then STOP and revaluate whatever you where going to do next.
2. Relearn how to read an ABG– 7.31/35/58/-4; lactate :5 like this?– lactate :5; -4/58/35/7.31 or like
this?

• Sat 75-90%, PaO2 35-50, BE > 0, Lactate < 2.5
• Investigate, correct and reinvestigate any metabolic acidosis
• Afterload reduction: • Milrinone 0.25-0.75 mcg/kg/min
• Volume: • Based on perfusion and acid base
status• Anticipate volume requirement
• Hgb= 13-15…..always above 11
• Normal sinus rhythm• Normothermia to slightly
cool but not hot

Avoid unnecessary noxious stimuli No baths or weights on night shift Cluster cares No excessive crying or IV sticks
Normothermia Avoid dehydration Weight gain- calories, calories, calories….
3KG baby needs 60 cc q 3h of 24 cal/oz formula to achieve 130 cal/kg/day- we do not always get here prior to DC
NG/PO feedings to achieve 10g/day wt gain

AcidosisArrhythmiasAnemiaSats > 93%Sats < 70%Dehydration

A ventricle that is working double time
Variable cardiac output Increased caloric
requirement/difficulty feedingTachypneaA need for close supervision/follow-
upA risk for sudden death

• Stressful hospitalization– Fetal dx: long time to think and web surf
– Antenatal dx: no time to prepare
– Long hospitalization: 14-36 days
• Transition home– Most fragile between the 1st and 2nd stage
• Must have scale and pulse ox prior to DC
– 20% risk of death prior to the second stage– Close follow-up by NP’s in clinic in addition to
Nutritionist• Anticipation of future surgeries

High Risk Patient population: Single Ventricle requiring staged
repairs Hybrid procedures and palliations MBT shunts PA, VSD, MAPCAs Other complex lesions including
heterotaxy syndrome

Approximately 7 to 15% of these infants will die unexpectedly at home before Stage 2.
Possible Causes Coronary artery obstruction or spasm Aortic arch obstruction Low cardiac output Arrhythmia Shunt thrombosis Sepsis or infection

Predictors Intact atrial septum Older age at the time of surgery Post op arrhythmias Airway complications Decreased ventricular fx pre and post op Anatomic subtypes
▪ Aortic atresia▪ Small ascending aorta diameter

Infants with Complex Single Ventricle have significant growth failure after Stage I palliation.
Only 3.6% at or above 50th percentile in weight at the time of Stage II palliation (Atz et al, 2004)
Feeding difficulties and inadequate nutrition can strongly influence outcomes!

All Single Ventricle patients go home with a scale and pulse ox
Family keeps daily log of feeding, weight and O2 saturations
Monitored by NPs either by phone or in high risk clinic

Family has “red flags” to call for: Weight loss: 30
grams of weight in one day
Lack of weight gain: 20 grams of over 3 days
O2 sats drop below 70%

Weekly visits after discharge x 4 weeks Every other week visits until Pre-Glenn
Cath (~3-4 months of age). Special attention to Sats, weight,
vomiting, diarrhea, feeding difficulties, URI
Monitor Pulse oximetry Weight BP Echocardiogram as necessary
Monthly Monitor EKG, Chest X-ray

Reduce interstage mortality to 0% Improved nutritional status and
weight gain will positively influence timing of Stage II palliation and outcome of surgical treatment.