Embed Size (px)
Citation preview

Journal of Neurology, Neurosurgery, and Psychiatry 1992;55:943-948
Cerebral symptoms after whiplash injury of theneck: a prospective clinical andneuropsychological study of whiplash injury
Thierry M Ettlin, Udo Kischka, Sandra Reichmann, ErnstW Radii, Sabine Heim,Daniel a Wengen, D Frank Benson
AbstractTwenty one unselected patients with anacute whiplash injury of the neck hadneurological and neuropsychologicalassessment, cervical x rays, EEG, BAEP,MRI, and an otoneurological examinationwithin two weeks of the injury. Sub-jectively, 13 patients reported con-centration deficits, 18 reported sleepdisturbances, 9 had symptoms of depres-sion, and 7 female patients told of men-strual irregularities. Neuropsychologicalexamination revealed significantly lowerperformance in tests related to attentionand concentration compared to sex, ageand educational matched control subjects.Otoneurological examination showedabnormalities in 9 of 17 whiplash subjects.EEG showed questionable changes in 8 of18 recordings. MRI and BAEP were nor-mal in all patients. Repeat neuropsycho-logical testing in 15 patients at threemonths showed that attention deficits hadimproved but were still shown in 12 of 14and the concentration deficits in 8 of 13patients. At one year all patients hadreturned to work, 16 to full and 5 to parttime employment. In 4, cognitive dysfunc-tion remained the only significant prob-lem. These findings are discussed as beingcompatible with possible damage to basalfrontal and upper brain stem structuresafter whiplash injury of the neck.
( Neurol Neurosurg Psychiatry 1992;55:943-948)
University Clinics,Basel CH-4031,SwitzerlandNeurology ClinicT M EttlinU KischkaS ReichmannEW RadiiS HeimOtorhinolaryngologyClinicD a WengenDepartment ofNeurology, UCLASchool of Medicine,Los Angeles, USAF BensonCorrespondence to:Dr Ettlin
Received 9 October 1990and in revised form26 January 1992.
Accepted 15 February 1992
The major symptoms reported after whiplashinjuries are neck pain, upper back pain, head-ache and muscle spasms.' 2 A subgroup ofwhiplash victims develop a chronic debilitywith somatic complaints, affective alterationsand depressed cognitive performance withparticular problems in concentration andmemory.3-7Whether whiplash injury can cause cerebral
dysfunction remains controversial. Only a fewstudies based on neuropsychological evalu-ation have attempted to describe the cerebralsymptoms; these studies show evidence oforganic brain dysfunction.8 12 6These reports,however, concern subjects who are in thechronic postinjury stage; evaluation in theacute, early stages following whiplash injury islacking.
This study was designed to test patientsduring the acute stages following whiplashinjury and continue prospective follow up
evaluations. Twenty one consecutive patientswho sustained an acute whiplash injury andwere seen in the Emergency Department,University Hospital, Basel, had a full neuro-logical and comprehensive neuropsychologicalassessment, cervical x rays, EEG, BAEP, MRI,and an otoneurological examination. Neuro-psychological testing was repeated at threemonths postinjury in 15 patients and again attwo years postinjury in 4 patients.
Patients and methodsSelectionTwenty six consecutive patients presentedbetween November 1988 and June 1989,within one hour to one day following a typicalwhiplash injury. Five patients (two females andthree males) dropped out of the study. Thus 21patients were referred for the additional exam-inations described below. None had a historyof previous cervical injury. There were 18females, ranging in age from 18 to 46 years,and three males, from 24 to 35 years of age.The average patient age was 28-8 years, 28-4years for the females and 29-3 years for themales. All had been involved in traffic acci-dents. The mechanism was a rear end impactin 15 patients, head-on collision in threepatients and lateral impact in three patients.None experienced direct head trauma. All wereactively employed before injury.
MethodsAll patients had an immediate neurologicalcheck up and had a full neurological examina-tion within three days. Each patient was askedfor a description of the accident and thepresent complaints. They were then ledthrough a structured interview with questionsconcerning their previous medical history andthe exact time schedule the current symptomshad developed (see table 1 for the interviewquestions and results).A full cervical radiographic series was per-
formed shortly after admission to the Emer-gency Room.EEG was performed within 3 to 8 days after
the injury using a 16 channel system with 30minutes of recording including photostimula-tion and EEG mapping.BAEPs were recorded within 7 to 14 days
with a click of 85 dB SL. The interpeak laten-cies I-III, III-V and I-V were measured out.
Otoneurological examination was per-formed within 14 days and included clinicaltesting of the vestibular system and a complete
943
Ettlin, Kischka, Reichmann, Radii, Seim, a Wengen, Benson
Table 1 Structured interview. Questions and results
Previous Immediate 3 days 3 months I yearInterview history post injury post injury post inury post injuryQuestions N = 21 N 21 N = 21 N = 19 N 17
Headache 3 14 18 11 7Neck pain 2 16 20 12 6Brachialgia 0 9 15 6 2Vertigo 1 8 16 8 4Nausea 0 10 3 4 0Visual symptoms 0 3 9 7 0Irregular menstruation 0 0 5 3 0Impaired concentration 0 5 13 10 5Impaired memory 0 1 10 9 4Depression 2 3 9 8 2Sleep disturbances 0 3 18 10 1Anxiety 3 0 10 7 1Irritability 0 2 7 11 3Employment disability N = 21none 21 5 8 12 16partial 0 0 0 2 5full 0 16 13 7 0
Figures indicate number of patients.
electronystagmography test battery (eye track-ing test, optokinetic nystagmus test, rotatingchair test, caloric test) and BAEPs.'8 Periph-eral vestibular deficit was suggested by eitherhorizontal spontaneous nystagmus, canal pare-sis of more than 30% following caloric irriga-tion, or asymmetry in the rotating chair test.Central vestibular deficit was suggested byvertical, rotatory or dissociated spontaneousnystagmus, low gain or saccades in the eyetracking test, low gain in optokinetic nys-tagmus testing, deficient fixation suppressionor pathological but symmetrical brain stemauditory responses. Nystagmus with decres-
- -- -.,...
..NI ,...
UUM
U1Z2UU
m
U
KU
__%;.
',l1
_r
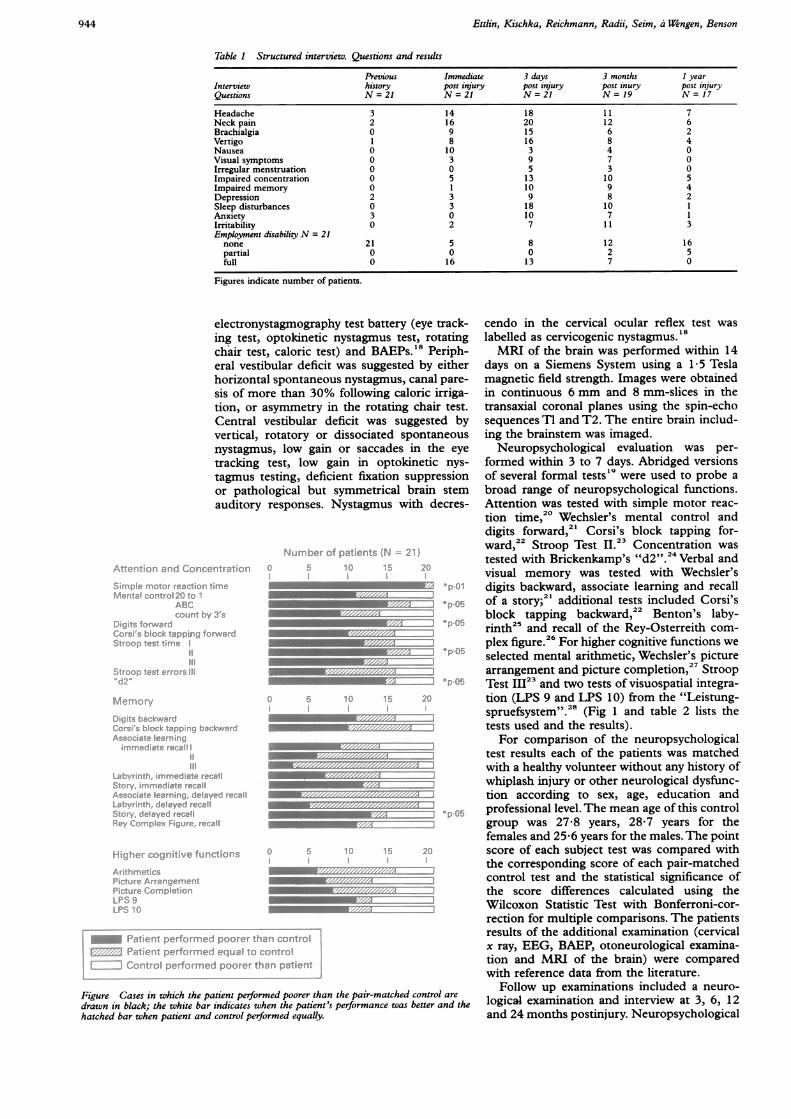
Figure Cases in which the patient performed poorer than the pair-matched control are
drawn in black; the white bar indicates when the patient's performance was better and the
hatched bar when patient and control performed equally.
cendo in the cervical ocular reflex test waslabelled as cervicogenic nystagmus.'8MRI of the brain was performed within 14
days on a Siemens System using a 1*5 Teslamagnetic field strength. Images were obtainedin continuous 6 mm and 8 mm-slices in thetransaxial coronal planes using the spin-echosequences TI and T2. The entire brain includ-ing the brainstem was imaged.
Neuropsychological evaluation was per-formed within 3 to 7 days. Abridged versionsof several formal tests'9 were used to probe abroad range of neuropsychological functions.Attention was tested with simple motor reac-tion time,20 Wechsler's mental control anddigits forward,2' Corsi's block tapping for-ward,22 Stroop Test 11.23 Concentration wastested with Brickenkamp's "d2".24 Verbal andvisual memory was tested with Wechsler'sdigits backward, associate learning and recallof a story;2' additional tests included Corsi'sblock tapping backward,22 Benton's laby-rinth25 and recall of the Rey-Osterreith com-plex figure.26 For higher cognitive functions weselected mental arithmetic, Wechsler's picturearrangement and picture completion,27 StroopTest 123 and two tests of visuospatial integra-tion (LPS 9 and LPS 10) from the "Leistung-spruefsystem".28 (Fig 1 and table 2 lists thetests used and the results).For comparison of the neuropsychological
test results each of the patients was matchedwith a healthy volunteer without any history ofwhiplash injury or other neurological dysfunc-tion according to sex, age, education andprofessional level. The mean age of this controlgroup was 27-8 years, 28&7 years for thefemales and 25 6 years for the males. The pointscore of each subject test was compared withthe corresponding score of each pair-matchedcontrol test and the statistical significance ofthe score differences calculated using theWilcoxon Statistic Test with Bonferroni-cor-rection for multiple comparisons. The patientsresults of the additional examination (cervicalx ray, EEG, BAEP, otoneurological examina-tion and MRI of the brain) were comparedwith reference data from the literature.
Follow up examinations included a neuro-logical examination and interview at 3, 6, 12and 24 months postinjury. Neuropsychological
..M-44.
M.:M-
m
944
Cerebral symptoms after whiplash injury of the neck: a prospective clinical and neuropsychological study of whiplash injury
Table 2 Neuropsychological test results. Initial evaluation. Raw point scores. N = 21
Controlsmean (SD)
Attention and Concentration1 Simple motor reaction time2 Mental control 20 to 13 ABC4 count by 35 Digits forward6 Corsi's block tapping forward7 Stroop test time I8 II9 III10 Stroop test errors III11 d2
Memory12 Digits backward13 Corsi's block tapping backward14 Associate learning I15 immediate recall II16 III17 Labyrinth immediate recall18 Story immediate recall19 Associate learning delayed recall20 Labyrinth delayed recall21 Story delayed recall22 Rey complex figure delayed recall
Higher Cognitive Functions23 Arithmetics24 Picture arrangement25 Picture completion26 LPS 927 LPS 10
0.19 (0.02)2.95 (0.21)2.57 (0.81)2.17 (1.0)7.85 (0.91)5.95 (0.74)11.62 (1.59)13.95 (1.39)22.0 (6.07)0.52 (0.51)
457.2 (71.6)
6.71 (1.3)5.48 (0.6)8.09 (1.09)9.52 (0.68)9.95 (0.22)2.83 (1.2)12.91 (2.4)9.81 (0.51)1.19 (0.51)
11.69 (3.09)12.31 (2.81)
14.86 (1.35)13.09 (1.51)9.91 (0.3)
25.52 (6.55)32.33 (5.49)
Patientsmean (SD)
0.27 (0.1)2.8 (0.41)2.3 (0.86)2.15 (0.98)6.42 (1.26)5.84 (0.83)13.2 (3.25)15.7 (4.67)25.6 (7.39)0.4 (0.6)
389.2 (72.0)
5.33 (1.19)4.89 (0.9)7.95 (1.57)9.3 (1.13)9.84 (0.5)2.81 (2.04)11.26 (3.4)9.14 (1.35)1.32 (0.95)8.93 (2.78)11.18 (1.9)
15.0 (1.58)13.76 (1.26)9.48 (0.6)
23.1 (6.54)25.2 (7.48)
The numbers in tests 5, 6, 11-16, 18, 19, 21, 22, 24-27 signify correct answers. The numbers in tests 10 and 17 denote errors. Thenumbers for tests 1, 7, 8, 9 stand for seconds. For tests 2-4 a score was calculated from times and errors (a higher score means abetter result).
assessment (a parallel version), was repeated at3 months in 15 patients and at two years in 4patients.As both neuropsychological performance
and response to electrophysiological testingmay be vulnerable to centrally acting analge-sics and muscle relaxants, medication duringthe period of testing was avoided when poss-ible. Fourteen patients received no medicationat all during the testing. The medication of theremaining seven is presented in detail below.
ResultsTable 1 summarises the complaints and symp-toms the patients reported in the structuredinterview on the pre-traumatic, immediate,three days, three months and one year post-whiplash injury and the frequency of employ-ment disability. Though none of the patientsapparently had direct head trauma, 12 couldnot give a precise description of the movementof their body and head at the moment ofcollision. Intensity and frequency of most ofthe reported symptoms were highest at 3 dayspost-injury. Immediately after the injury fivepatients were aware of decreased concentra-tion. Within three days, 13 patients had notedconcentration or memory problems. Sleepdisturbance was reported by 18 patients withinthree days and 9 patients reported symptomsof depression including depressed mood, lossof energy and decreased motivation; only 2 ofthe 9 had a previous history of depression.Interestingly, 7 of the 18 female patientsreported menstrual irregularities; one hadirregular menstrual bleeding the day followingthe injury and 4 more within three days; onereported an interruption of menstrual bleedingand one a delay in the menstrual cycle.On neurological examination all patients
showed tenderness over the cervical regionwith some limitation of motion of the cervicalspine. Sensory loss was present and includedmore than one dermatomal segment of theupper extremities in most patients, but armweakness was more diffuse than radicular. Inthree patients the deep tendon reflexes weredecreased on the painful arm. All other resultson routine neurological examination were neg-ative.
Cervical spine x rays were obtained in 19 ofthe 21 patients. Thirteen showed a loss ofcervical lordosis; two a sharp reversal oflordosis at C4-5 or C5-6.EEGs were obtained in 18 patients and were
focally slow in 8. Occipital focus was present in4, temporo-occipital in 2, parieto-occipital inone, and temporoparietal in one. One patienthad mild overall slowing and one showedparoxysmal bifrontal theta waves. Eight hadnormal EEGs.BAEPs were obtained in 14 patients. No
abnormalities were noted.Otoneurological examinations were ob-
tained in 18 patients. Ten had abnormalities:three showed findings consistent with centralvestibular dysfunction, one had findings con-sistent with a peripheral vestibular dysfunc-tion, four showed a cervicogenic nystagmus. Inone there was a combination of central vestibu-lar dysfunction and a cervicogenic nystagmusand one had peripheral vestibular dysfunctionplus cervicogenic nystagmus.MRI obtained in 15 patients were without
abnormalities except for one small, nonspecificwhite matter lesion in a 36 year old female.
Table 2 shows the raw point scores of eachneuropsychological subtest for the patient andcontrol group. Figure 1 shows the perfor-mances of each patient compared with theperformance of the corresponding pair-
945

Ettlin, Kischka, Reichmann, Radii, Seim, a Wengen, Benson
matched control subject for each test. In thesubtests related to attention and concentrationthe score differences were statistically sig-nificant. From 21 patients, 20 showed a highersimple motor reaction time (p = 0-01) and 15performed poorer inWechsler's mental controlsubtest "ABC" (p = 0 05), digit span (p =0 05), sustained attention test Stroop II (p =0 05) and concentration test "d2" (p = 0 05).Although 10 patients complained aboutimpaired memory, the only significant differ-ence demonstrated in formal memory tests wasthe poorer performance of the patients in thedelayed recall of a story (p = 0.05). As thelearning ability of both verbal and visuospatialmaterial was similar in both patients andcontrols, the decreased ability to recall suggestsa retrieval dysfunction. No differences wereshown on subtests probing higher cognitivefunctions.
Seven patients were on medication duringthe period of different testings. They weretaking either a combination drug of the musclerelaxant orphenadrine citrate and the analgesicparacetamol, dihydroergotamine mesylate orthe non-steroidal antiinflammatory agents ibu-profen or diclofenac sodium. All four patientstaking medication at the time of EEG record-ing showed focal slowing. From the threepatients taking medication during otoneuro-logical examination one showed a combinationof central vestibular dysfunction and cervico-genic nystagmus, one cervicogenic nystagmusand one normal results. From four patients onmedication during neuropsychological testingthree showed lower results than their controlsin the subtests related to attention and concen-tration. The fourth patient, taking ibuprofen,did not show a lower performance.
Nineteen patients returned for follow upneurological examination and interview threemonths and 17 one and two years after theinjury. Structured interviews (table 1) sug-gested that although cerebral symptoms, poorconcentration and subjective memory dysfunc-tion, depression, anxiety and irritability hadimproved in most, only 5 patients reportedcomplete recovery three months after theinjury. In addition, four reported late onsetsymptoms including depression, anxiety, irrita-bility and sleep disturbances.
Follow up examination two years postinjuryshowed that the course of symptoms had beenstable since one year after the injury in allpatients. Thus from 17 patients re-examinedone year after the injury 10 reported completerecovery. Seven patients had chronic or inter-mittent headache, 6 together with neck pain, 4together with vertigo and 2 together withdepression. Additionally, five of these patientshad still poor concentration and subjectivememory dysfunction. One other had isolatedword finding problems and memory dysfunc-tion.
Follow up neuropsychological assessment (aparallel version) could be obtained from 15patients at three months postinjury and asecond follow up testing from four patientswith persistent employment disability one ortwo years postinjury. The test results showed
that of the 14 retested patients with initialattentional deficits, two now had results equalto their controls, 10 others had improved buttwo actually had lower test results than before.Of 13 retested patients with initial deficits inconcentration, 8 were improved, 4 unchangedand one had poorer results.Three patients were on medication at the
time of retesting. Two were taking diclofenacsodium and ibuprofen, one showing poorer,one improved and one unchanged scores com-pared to the initial evaluation.At three months, 12 patients had returned to
full employment; three had been off work fortwo days only and five had no employmentdisability at all (table 1).Nine had not returned to regular employ-
ment after three months; seven were stilldisabled and 2 had returned to partial employ-ment. The reason was chronic or intermittentheadache or/and neck pain or/and vertigo pluscognitive dysfunction. Five of these patientswere adamant that cognitive disturbancesinterfered with their performance at workindependently from intermittent or insignifi-icant head and neck pain. At one and two yearpost injury 16 patients had returned to fullemployment. Five patients were still partiallydisabled: Four of these belonged to the 5patients with persisting cognitive dysfunction;the fifth had isolated headache and neck pain.Repeated neuropsychological testing at oneyear in two and two year postinjury in the othertwo patients with chronic cognitive dysfunc-tion demonstrated that the test results wereunchanged compared to previous testings.
DiscussionThe patient population in this prospectivestudy of whiplash injury patients is differentfrom most published studies that are attainedretrospectively with selected patients sufferinga chronic course. Only two studies of whiplashpatients in the acute stage are known: onereport focussed on EEG findings only;29 theother, a recent follow up study on 78 patients,demonstrated that initial neck pain intensity,cognitive impairment as indicated on a self-rating questionnaire and age predicted theoutcome afterwhiplash injury but psychosocialfactors, negative affect and personality traitsdid not.17
In our group dysfunction of attention andconcentration was more frequent than expec-ted. When compared with pair-matched con-trols the patients showed a significant increasein simple motor reaction time and significantlydecreased sustained attention, digit span andconcentration. In addition, the frequency foremotional problems was high; 9 patients repor-ted depression early in the course; 7 of theseindividuals had never previously experiencedsignificant depressive reactions.On cervical spine x ray loss of cervical
lordosis and sharp reversal of cervical lordosisat C4-5 or C5-6 found in our patients can bothalso occur in asymptomatic poeple and havepoor prognostic value.30The EEG was abnormal in 10 of 18 acute
946
Cerebral symptoms after whiplash injury of the neck: a prospective clinical and neuropsychological study of whiplash injury
subjects. Several EEG studies have reportedabnormalities in 30-50% of whiplashpatients' 13 31-33 but a recent study29 reportedminimal abnormalities in only three of 68patients. Considering that mild overall slowingis found in 10-15% of normal subjects,34 thesignificance of mild overall slowing with focalemphasis in our 10 patients remains unclear.The normal results with MRI and BAEP
studies confirm the negative results of Yarnellet al 12 who studied chronic whiplash patientsand show that MRI and BEAP were alsonormal when obtained in the acute stage.The otoneurological examination is reported
as a sensitive method for detecting vestibulardysfunction following whiplash trauma.35-37Our results (10 abnormal out of 18 tested)demonstrate that the number with vestibulardysfunctions early in the course is high.At one year postinjury 10 patients reported
complete recovery and 16 were back to fullemployment. In one patient, however, wordfinding problems and memory dysfunctionpersisted and 4 patients remained partiallydisabled mainly because of cognitive dysfunc-tion.The aetiology of cerebral symptoms follow-
ing whiplash injury has been controversial.Brain lesions have been produced in experi-mental animals,38-40 and cases of proven cere-
bral contusion and subdural haematoma havebeen reported following whiplash injuries,4'but many studies5 69 15 42 have interpretedcerebral symptoms as indication of a neuroticpersonality.What causes, other than brain damage,
could explain the early findings?Medication such as analgesics and muscle
relaxants often prescribed to treat the pain ofwhiplash injury are known to influence neuro-
psychological and electrophysiological data. Atmost, medication played only a minor role inour patients as 14 had no medication at allduring the period of testing and those usingmedication had no more positive findings inany of the tests than those without medica-tion.
Pain and distress can also cause inattentionand decreased concentration. In fact, theseconditions are difficult to measure independ-ently and pain was probably a factor forcognitive dysfunctioning in some of thepatients. Other patients, particularly the fourwith persistent employment disability, showedchronic attention and concentration problemsindependent of pain intensity and one patientreported word finding problems as the onlysymptom.
Depression could impair attention and con-
centration and as 9 patients had symptoms ofdepression the differentiation from other cau-
ses remains difficult. Only two of the patientshad previous episodes of depression; mostwere psychiatrically healthy subjects and theirpost injury depression deserves considerationas an organic depression.
Finally, secondary gain is often thought tocontribute to post whiplash symptoms but can
most probably be excluded in our patients. Theneuropsychological impairments were limited
to psychomotor functions and it would beexpected that psychogenic causation wouldproduce inhomogeneous test results and alsoaffect higher cognitive functions.The "post-concussion syndrome" lists sim-
ilar cognitive, emotional and somatic symp-toms and has been plagued by the sameorganic/psychogenic controversy. The neuro-psychological dysfunctions seen in our patientswith whiplash injury correspond to problemsnoted in the early stage of recovery fromconcussion." 4
Attention and concentration deficits, emo-tional changes, sleep disturbances and men-strual irregularities suggest possible damage tobasal frontal and upper brain stem structures,sites of limbic and hypothalamic connections.The reticular formation and its projections alsooccupy this area and are known to play a majorrole in the regulation of attention and concen-tration." " Electrophysiological studies35 37 38also suggest that the functional abnormalitiesfollowing whiplash injury evolve from dis-turbances in the midbrain, reticular formation,vestibular nuclei and the hypothalamus as wellas the basal orbital and septal frontal regions.These areas are particularly prone to traumaticbrain injury.4Although a wide range of other aetiologies
could be responsible for the cerebral symptomsour findings may be due to organic braindysfunction after whiplash injury.
1 Zenner P. Die Schleuderverletzun der HWS und ihre Begut-achtung. Berlin: SpringerVerlag 1987.
2 Hirsch SA, Hirsch PJ, Hiramoto H, Weiss A. Whiplashsyndrome. Orthop Clin of North Am 1988;19:791-5.
3 GayJR, Abbott KH. Common whiplash injuries of the neck.J3AMA 1953;152:1698-704.
4 Janes JM, Hooshmand H. Severe extension, flexion injuriesof the cervical spine. Mayo Chir Proc 1965;40:353-9.
5 Hodge JR. The whiplash neurosis. Psychosomatics 1971;12:245-9.
6 Erdmann H. Die Schleuderverletzung der Halswirbelsaeule.Die Wirbelsaeule in Forschung und Praxis. Stuttgart: Hip-pokrates Verlag 1973.
7 Wiesner H, Mumenthaler M. Schleuderverletzung derHalswirbelsaeule. Ther Umsch 1974;31:640-9.
8 Berstad JR, Bacrum B, Loecher EA, Mogstad RE, Spastad0. Whiplash: Chronic organic brain syndrome withouthydrocephalus ex vacuo. Acta Neurol Scand 1975;51:268-84.
9 Kraemer G. HWS-Schleudertraumen. Zur Pathogenese derzerebralen Beteiligung und persistierenden Stoerungen.Med Welt 1983;34:1134-40.
10 Berry H. Psychological aspects of whiplash injury. InWilkins RH, Rengachary SS, eds. Neurosurgery. NewYork:McGraw-Hall, 1985.
11 Foletti GB, Regli F. Le traumatisme cervical indirect:facteurs de mauvais prognostic a long terme. SchweizRundsch Med Prax 1987;76:1304-9.
12 Yarnell PR, Rossie GV. Minor whiplash head injury withmajor debilitation. Brain Inj 1988;2:255-8.
13 Laubichler W Zur Aetiologie des neurastheniformen "Psy-chosyndroms" nach Verletzungen der Halswirbelsaeule,einschliesslich cervicocephalem Beschleunigungstrauma.Beitr Gerichd Med 1988;46:439-49.
14 Radanov BP, Dvorak J, Valach L. Psychische Veraender-ungen nach Schleuderverletzungen der Halswirbelsaeule.Schweiz Med Wochenschr 1989;119:536-43.
15 Ettlin TM, Kischka U, Kaeser HE. Kognitive und psy-chische Stoerungen nach HWS-Schleudertrauma.Schweiz Rundsch Med Prax 1989;78(36):967-9.
16 Kischka U, Ettlin TM, Heim S, Schmid G. Cerebralsymptoms following whiplash injury. Eur Neurol 1991;31:136-40.
17 Radanov BP, Di Stefano G, Schnidrig A, Ballinari P. Role ofpsychosocial stress in recovery from common whiplash.Lancet 1991;338:712-15.
18 Allum JHR, Ura M, Honegger F, Pfaltz CR. Classificationof peripheral and central (pontine infarction) vestibulardeficits: Selection of a neurootological test battery usingdiscriminant analysis. Acta Otolaryngol (Stockh) 1991;111:16-26.
947
Ettlin, Mschka, Reichmann, Radii, Seim, a Wengen, Benson
19 Perret E. Gehirn und Verhalten. Bern: Verlag Hans Huber,1973.
20 Brickenkamp R. Handbuch apparativer Verfahren in derPsychologie. Goettingen: Hogrefe, 1986.
21 Wechsler D. A standardized memory scale for clinical use. JPsychol 1945;19:87-95.
22 Milner B. Interhemispheric differences in the localization ofpsychological processes in man. Brit Med Bull 1971;27:272-7.
23 Stroop JR. Studies of interference in serial verbal reactions.J Exp Psychol 1935;18:643-62
24 Brickenkamp R. Test d2-Aufmerksamkeits-Belastungstest.Goettingen: Hogrefe, 1962.
25 Benton AL, Hamsher K.de S. Multilingual aphasia examina-tion. Iowa City: University of Iowa 1976. (Manual, rev,1978).
26 Rey A. L'examen psychologique dans les cas d'encephalo-pathie traumatique. Arch de Psychol 1941;28(112):286-340.
27 Wechsler C. Wechsler Adult InteUligence Scale-Revised. NewYork: Psychological Corporation, 1981.
28 HornW Leistungspruefsystem (L-P-S). Goettingen: Hogrefe,1983.
29 Jacome DE. EEG in whiplash: a reappraisal. Clin Electro-encephalogr 1987;18:41-5.
30 Gore DR, Sepic SB, Gardner GM. Roentgenographicfindings of the cervical spine in asymptomatic people.Spine 1986;11:521-4.
31 Fischer D, Palleske H. Das EEG nach der sogenanntenSchleuderverletzung der Halswirbelsaeule. ZentralblNeurochir 1976;37:25-35.
32 Pavlincova E, Mumenthaler M, Karbowski K. Elektroenze-phalographische Befunde bei reinen Schleuderverletzun-gen der Halswirbelsaeule. Nervenarzt 1977;48:505-8.
33 Torres F, Shapiro SR. Electroencephalograms in whiplashinjury. Arch Neurol 1961;5:28-35.
34 Christian W. Klinische Elektroencephalographie. Stuttgart:GeorgThieme Verlag, 1975:43.
35 Hinoki M. Vertigo due to whiplash injury: a neurootologicalapproach. Acta Otolaryngol 1984;Supp4l9:9-29.
36 Toglia JU. Acute flexion-extension injury of the neck.Electronystagmographic study of 309 patients. Neurology1976;26:808-14.
37 Ushio N, Ishida I, Koike S et al. Studies on invertedoptokinetic nystagmus in cases with whiplash injury. PractOtol (Kyoo) 1971;64:493-509.
38 Kawakami M. EEG findings in experimental whiplashinjury. In: Hami K, ed. Whiplash injury. Tokyo: Kanokara-Shuppan, 1972:136-49.
39 Miura Y, Tanaka M. Disturbances of the venous system inthe head and neck regions in rabbits with whiplash injury.Brain Nerve (Tokyo) 1970;2:217-23.
40 Ommaya AK, Faas F, Yarnell P. Whiplash injury and braindamage. JAMA 1968;204:285-9.
41 Ommaya AK, Yarnell P. Subdural hematoma after whiplashinjury. Lancet 1969;II:237-9.
42 Buehring M. Reflex dystrophy following so-called whiplashinjury of the cervical spine. Z Orthop 1984;122:281-6.
43 Gronwall D, Wrightson P. Delayed recovery of intellectualfunction after minor head injury. Lancet 1974;2:605-9.
44 Dikmen S, Reitan RM. Emotional sequelae of head injury.Ann Neurol 1977;2:492-4.
45 Heilman KM,Watson RT,Valenstein E. Neglect and relateddisorders. In: Heilman KM, Valenstein E, eds. Clinicalneuropsychology. New York: Oxford University Press1985:252-84.
46 Mesulam MM. Attention, confusional states and neglect.In: Mesulam MM, ed. Principles of behavioral neurology.Philadelphia: FA Davis, 1985:135-40.
47 Alexander MP. Traumatic brain injury. In: Benson DF,Blumer D, eds. Psychiatric aspects of neurologic diseaseVol 2. NewYork: Grune and Stratton, 1982:219-48.
948





























