Embed Size (px)
Citation preview

CONGENITAL HEART DISEASE
456
Embryologic development of the heart beginswith the fusion of angiogenetic cell clusters with-in the splanchnic mesoderm layer of the primi-tive embryo to form the heart tube at 18 to 21days of gestation. The cardiac tube surrounds acore of cardiac jelly, which serves as an extra-cellular matrix, and plays a key role in the com-plex intracellular signaling and feedback mecha-nisms that regulate cardiac morphogenesis. Thecardiac tube consists of a myocardial mantlethree to five layers thick and an inner single layerof endocardial cells. The endocardial cells play arole in the formation of endocardial cushions, aswell as in cellular signaling. The heart begins torhythmically contract as early as day 17, oncethe functional units of the myocytes begin toform. Myocardial growth proceeds with seg-mentation and looping of the heart tube and cel-lular differentiation and migration along theembryologic axes, with the establishment of lat-erality and the organization of the primitive cellsinto a sophisticated organ.
The fetal circulation adapts to placental gasexchange and nutritional support. The right sideof the heart is responsible for about two thirds ofthe fetal cardiac output, which is shuntedthrough the ductus arteriosus into the descend-ing aorta. During development, pulmonary vas-cular resistance is high and pulmonary bloodflow is low. Closer to term, pulmonary bloodflow slowly increases and, as new arteriolesdevelop and increased pulmonary arterial cross-
sectional area increases, pulmonary vascularresistance decreases. At birth, with the entranceof air into the lungs and alveolar expansion, pul-monary vascular resistance falls and pulmonaryblood flow rapidly increases 8- to 10-fold. Theductus arteriosus changes from a right-to-leftconduit to a left-to-right shunt after birth, until itcloses within the first hours to days of life. Pul-monary arterial blood pressure is thought toreach adult levels by 2 to 6 weeks after birth.Increased pulmonary venous return to the leftatrium elevates left-sided intracardiac pressuresrelative to the right-sided pressures, and thevalve of the foramen ovale closes.
Deviations from this complex process of car-diac development lead to congenital cardiacanomalies, with presentations that vary from theimmediate postnatal period to adulthood. Con-genital cardiac lesions can be broadly dividedinto cyanotic and acyanotic lesions. The clinicalmanifestations of congenital heart disease in theneonatal period usually result in cyanosis, respi-ratory distress, and/or hypoperfusion with evi-dence of cardiogenic shock. Congenital heartdisease is suspected when a history and physicalexamination, a chest radiograph, and an ECGshow one or more of these clinical findings. Fur-ther evaluation by Doppler echocardiography isroutine and an integral part of the noninvasiveevaluation of congenital heart disease (see alsochapter 44). Echocardiography can determinethe basic anatomic configuration of the heart,
Our understanding of the complexities of congenital heart disease, a deviation from normal cardiacanatomic development that affects 8 in 1000 births, has progressed immensely since the establish-ment of the Board of Pediatric Cardiology (and hence the subspecialty) in 1961. Advances have par-alleled improvements in diagnostic imaging, such as echocardiography and cardiac angiography, andinnovations in surgical repair techniques. Basic scientific investigation has led to greater comprehen-sion of the patterns of embryologic development and of the aberrancies that cause the common con-genital anomalies. This chapter gives a broad overview of the genesis of congenital heart disease witha focus on the role of corrective surgical interventions.
Alden M. Parsons, G. William Henry, and Michael R. Mill
Chapter 46
Surgical Interventions forCongenital Heart Disease

CONGENITAL HEART DISEASE
SURGICAL INTERVENTIONS FOR CONGENITAL HEART DISEASE
457
and Doppler studies provide information aboutpatterns and disturbances in blood flow. Angiog-raphy can further elucidate the cardiopulmonarydefects. Indications for angiography may includeinconsistencies in the noninvasive findings, theneed for images of the branch pulmonary arter-ies, or suspected complex ventricular septaldefects (VSDs). Abnormalities of the aortic arch,such as coarctation or vascular rings, are bestevaluated by magnetic resonance imaging.
Therapy for congenital heart disease hasevolved with surgical and nonsurgical innova-tions. The development of transcatheter proce-dures has made therapeutic cardiac catheteriza-tion a viable alternative to surgery for specificcongenital cardiac lesions (see chapter 45). Inaddition, advances in imaging and prenatal diag-nosis have spurred the development of antenatalsurgical intervention for congenital heart disease.
INTERVENTIONAL CARDIOLOGYEarly management of congenital heart lesions
was largely surgical. With the development ofangiography, initially a diagnostic modality,interventional catheter-based techniques formanagement of congenital heart diseasebecame possible. Definitive treatment withdevice closure now exists for amenable lesionssuch as fossa ovalis (secundum type) atrial sep-tal defect (ASD), muscular VSD, and patent duc-tus arteriosus. Balloon valvuloplasty for pul-monic or aortic stenosis and balloon angioplastywith stenting for branch pulmonary artery steno-sis and coarctation of the aorta are other com-mon catheter-based interventions that havebeen used with some success. Studies on tran-scatheter perforation and pulmonic valvuloplas-ty in pulmonary atresia with intact ventricularseptum have reported an 81% initial successrate; however, more than 50% of patients mayneed a systemic-to-pulmonary shunt to augmentpulmonary blood flow or are better suited fordefinitive surgical repair.
SURGICAL TREATMENTThe development of pediatric cardiac surgery
has led to the survival of many children withcomplex congenital heart disease. These suc-cesses have depended on improved diagnoses,advances in surgical technique, and the devel-
opment of a means for extracorporeal circula-tion—cardiopulmonary bypass (CPB). Complexrepairs for previously fatal lesions such as trans-position of the great arteries and hypoplasticleft-sided heart syndrome (HLHS) have becomeroutine, with declining mortality rates andimproved long-term outcomes.
Surgically Correctable Lesions: Common Congenital AnomaliesVentricular Septal Defects
Ventricular septal defect is the most commoncongenital cardiac anomaly, occurring in 20% ofpatients with congenital heart disease (Fig. 46-1).Interventricular communication occurs with thefailure of the ridges of tissue to fuse to form theseptum. VSDs are traditionally classified as peri-membranous, muscular, and doubly committedsubarterial, with the perimembranous and mus-cular types further classified on the basis ofanatomic location as inlet, outlet, or trabecular.Of surgically repaired defects, 80% are peri-membranous. Of patients with VSDs, 50% haveother associated cardiac anomalies. The flowacross a VSD is related to the size of the VSD.“Restrictive” VSDs are small to medium-sized,with a pressure gradient across the defect.“Nonrestrictive” VSDs are large, with equal leftventricular and right ventricular (RV) pressures.Congestive heart failure can develop with signif-icant left-to-right shunting and increased volumeload to the pulmonary vasculature, the left atri-um, and the left ventricle. Persistent elevation inpulmonary vascular resistance (PVR) can lead toequalization of PVR and systemic vascular resist-ance (SVR) and irreversible changes to the pul-monary vasculature. Eisenmenger’s complex(reversal of the shunt to right to left and subse-quent cyanosis) can result if the VSD is leftuntreated. Surgical repair is performed bymeans of a median sternotomy and exposurevia the right atrium, right ventricle, or pulmonaryartery, depending on the location of the lesion.
Atrial Septal Defect An interatrial communication accounts for 10
to 15% of congenital cardiac anomalies. The termASD refers to a spectrum of anomalies that arebroadly classified into four categories: oval fossaor “secundum” defect, ASD of the atrioventricular

CONGENITAL HEART DISEASE
SURGICAL INTERVENTIONS FOR CONGENITAL HEART DISEASE
458
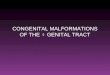
Figure 46-1 Transatrial Repair of Ventricular Septal Defect (VSD)
Cannula in superiorvena cava
Aorta
Pulmonarytrunk
Retractedseptal leaflet
Right ventricle
Perimembranous VSD
Cannula in inferiorvena cava
Oxygenatedblood
Deoxygenatedblood
VSD with leftto right shunt
Right atriotomy and retraction of the tricuspid valve leaflets provide excellent exposure of the perimembranous VSD.
Retractedseptal leaflet
Leftventricle
Region of conductionnerve bundle onwall of left ventricle
The septal leaflet of the tricuspid valve may need to be bisected to permit placement of pledgetted sutures at its junction with the VSD. Superficial sutures are placed along the inferior border of the VSD to prevent injury to the conduction system.
Septal leafletAnterior leaflet
Syntheticpatch
Posterior leaflet
The VSD is closed with a synthetic patch and pledgetted sutures. The septal leaflet, if detached, is then repaired with a running suture.

CONGENITAL HEART DISEASE
SURGICAL INTERVENTIONS FOR CONGENITAL HEART DISEASE
459
septal defect (AVSD) type or partial AVSD or“ostium primum” defect, superior or inferior sinusvenosus defects, and coronary sinus defects.ASDs often coexist with other anomalies, such aspartial anomalous venous drainage. The degreeof hemodynamic disturbance is related to the sizeof the defect and the amount of blood flow shunt-ing. Indications for closure are a significant left-to-right shunt, leading to a ratio of pulmonary bloodflow to systemic blood flow (also known as shuntfraction, Qp:Qs) of greater than 1.5:1, or knownvenous thrombosis (because of the risk of para-doxical embolization and cerebrovascular acci-dent). Device closure can be performed for sim-ple oval fossa ASDs. Surgical repair is most oftenperformed via a median sternotomy with CPBand bicaval cannulation via a right atriotomy.
Patent Ductus Arteriosus Patent ductus arteriosus is a vascular connec-
tion postnatally between the main pulmonarytrunk or proximal left pulmonary artery and thedescending thoracic aorta. This anomaly occursin about 1 in 2000 to 2500 births and accountsfor 10% of congenital heart lesions. In full-terminfants, the ductus arteriosus is usually function-ally closed by 10 to 15 hours after birth. Persis-tent blood flow through this vessel is often asso-ciated with other congenital anomalies, anddepending on the vascular connections, pul-monary blood flow may be dependent on paten-cy of the ductus, as in lesions of RV outflowobstruction. In this case, the vessel may be keptopen with prostaglandin E1 therapy until an aor-topulmonary connection is surgically created.When no other associated anomalies exist, andductus closure has not occurred after medicaltherapy with indomethacin for 48 to 72 hours,direct surgical ligation or division via a left pos-terolateral thoracotomy or, alternatively,catheter-based device closure is indicated. Surgi-cal closure before 10 days of age reduces theduration of ventilatory support, the length of hos-pital stay, and the overall morbidity rate.
Atrioventricular Septal Defects Atrioventricular septal defects are defects
involving deficiencies in the AV septum andabnormalities of the AV valves (mitral and tricus-pid), commonly referred to as “endocardial
cushion defects.” AVSDs account for 4 to 5% ofcongenital heart disease, and 7 to 25% of AVseptal defects are associated with other cardiacdefects. There is a wide spectrum of lesions,with a partial AVSD being limited to a deficiencyin the atrial portion of the atrioventricular sep-tum and a common atrioventricular valve(ostium primum ASD) and a complete AVSDreferring to a deficiency of the entire atrioven-tricular septum with a common atrioventricularvalve. Complete AVSDs are commonly seen inpatients with Down’s syndrome and can occurin combination with tetralogy of Fallot (TOF) inthis patient population. The mortality rate forunrepaired complete AVSDs at 2 years of age isas high as 80% because of progressive conges-tive heart failure and pulmonary vascular dis-ease. Surgical repair is performed via a mediansternotomy with CPB and with the use of a rightatriotomy. The interatrial and/or interventricularcommunication is closed, and valvular compe-tency is restored.
Tricuspid Atresia Tricuspid atresia, a congenital lesion with an
absent right-sided AV connection, occurs in up to3.7% of patients with congenital heart disease.Left ventricular preload is dependent on interatrialblood flow via an ASD. Often, there is an associ-ated VSD with left-to-right shunting, the degree ofwhich depends on the size of the VSD and theright ventricle or infundibular chamber, and theright- and left-sided pressures. The physiology ofthe lesion varies by the amount of pulmonaryblood flow. The original surgical repair, the classicFontan procedure, involved a direct connectionbetween the right atrium and the main pulmonaryartery. Present-day conversion to the Fontan circu-lation usually requires a two-stage surgicalapproach after early palliation. A cavopulmonaryanastomosis can be performed as early as 3months of age but is usually created between 4and 9 months, followed by the Fontan procedure,which is performed between 18 months and 3years. The modern Fontan procedure includes atotal cavopulmonary connection using a bidirec-tional Glenn shunt and an extracardiac conduitconnection between the inferior vena cava andthe pulmonary artery. The bidirectional Glennshunt is a connection between the divided end of

CONGENITAL HEART DISEASE
SURGICAL INTERVENTIONS FOR CONGENITAL HEART DISEASE
460
the superior vena cava and the right pulmonaryartery that shunts venous return from the superiorvena cava directly to both lungs. This modificationreduces associated morbidity and mortality rates,including a lowered incidence of early failure anda reduction in early and late arrhythmias.
Surgically Correctable Lesions: Complex Congenital AnomaliesDouble-Outlet Right Ventricle
Double-outlet right ventricle is a conotruncalmalformation with both great arteries arisingfrom the right ventricle and an associated VSD.This anomaly has a wide spectrum of presenta-tions depending on the location of the VSD, itsrelation to the great vessels, and the degree ofarterial overriding of the interventricular septum.Classifications are based on the relationship ofthe VSD to the great vessels: subaortic VSD withor without pulmonary stenosis, subpulmonaryVSD with or without subaortic stenosis, doublycommitted VSD, and noncommitted or remoteVSD. The degree of hemodynamic compromiseof this lesion depends on the variable degree ofsubvalvar stenosis and the size and precise posi-tion of the VSD. The surgical approach alsodepends on the nature of the lesion.
Hypoplastic Left Heart SyndromeHypoplastic left heart syndrome (HLHS), a
congenital lesion with univentricular physiology,involves an atretic left ventricle, an underdevel-oped mitral or aortic valvular apparatus, or both,and hypoplasia of the ascending aorta. Systemicblood flow is usually ductal-dependent, and theappearance of symptoms in the neonatal periodusually correlates with spontaneous ductal clo-sure. Thus, early management with prostaglandinE1 to maintain ductal patency is life-sustaining.The appropriate balance between pulmonaryand systemic blood flow (Qp:Qs) is critical.HLHS accounts for 25% of cardiac mortalityduring the first week of life. The major neonatalpalliative approach is the Norwood procedure,in which an aortopulmonary connection is cre-ated (Figs. 46-2 and 46-3). This procedureinvolves the enlargement of the aortic arch witha homograft patch, and a shunt to provide pul-monary blood flow. The surgery is usually per-formed during the neonatal period and carries a
20 to 40% risk of mortality. The Norwood pro-cedure is followed by a bidirectional Glennshunt at 3 to 6 months of age and a Fontan pro-cedure at 2 to 3 years of age. Alternatively, car-diac transplantation is favored for HLHS at somecenters. The operative risk of cardiac transplan-tation in the neonatal period is 10%, but there isa high mortality rate (25%) for patients on thewaiting list.
Tetralogy of FallotClassically, TOF refers to four major congenital
defects: VSD, infundibular pulmonary stenosis,dextroposition of the aorta, and RV hypertrophy(Fig. 46-4). The common anatomic abnormalityresponsible for all features is posterior malalign-ment of the outlet septum. TOF can present witha range of clinical findings: from cyanosis at birthto oxygen desaturation without cyanosis (“thepink tetralogy”). The degree of compromise isdetermined by the severity of the RV outflowobstruction and the size and location of theVSD. The reported mortality rate for unrepairedTOF is 30% by 6 months of age, 50% by 2 years,and up to 84% by 5 years. Infants with severeforms of TOF are often maintained onprostaglandin E1 to support pulmonary bloodflow until repair. Studies reviewing early pallia-tive procedures versus complete repair showlower overall mortality rates for early completerepair of uncomplicated TOF relative to a two-stage approach to TOF repair. Total correction isaccomplished on CPB. Closure of the VSD andprovision of unobstructed flow from the rightventricle are the main goals of surgery.
Total Anomalous Pulmonary Venous ReturnThere are three types of total anomalous pul-
monary venous return: supracardiac (most com-mon, 50%), with pulmonary venous drainageinto the innominate vein through a vertical vein;intracardiac, with drainage into the coronarysinus or the right atrium (least common); andinfracardiac, with drainage into the inferior venacava. Total anomalous pulmonary venous returnmay present with total pulmonary venousobstruction and pulmonary edema, requiringurgent surgical intervention. Without surgery,the mortality rate is 100% in the first year of life.Surgical repair with direct anastomosis of the

CONGENITAL HEART DISEASE
SURGICAL INTERVENTIONS FOR CONGENITAL HEART DISEASE
461
Stage IIAt about 6 months of age, after pulmonary vascular resistance falls, a bidirectional Glenn shunt is necessary to reduce volume load on the right ventricle. The previous Blalock-Taussig shunt is divided.
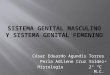
The main pulmonary artery and a cryopreserved aortic homograft create a neoaorta. Pulmonary blood flow is established through a systemic-to-pulmonary artery shunt.
Atretic aortaPatent ductus arteriosus
Atrial septal defect
Hypoplastic left ventricle
Right atriotomy
Ligated ductus arteriosus
Oversewn distal pulmonary artery
Innominate artery
Modified Blalock- Taussig shunt
Superior vena cava
of “neoaorta”
Right pulmonary artery
Atretic aorta
Main pulmonary artery
Divided Blalock- Taussig shunt
Ligated azygos vein
Neoaorta
Superior vena cava
Right pulmonary artery
Oversewn proximal superior vena cava
Stage IHypothermic cardiopulmonary bypass and right atriotomy are utilized to excise the interatrial septum. The main pulmonary artery is transected and a “neoaorta” is created.
Norwood Correction of HLHSFigure 46-2

common pulmonary venous channel to the rightatrium is accomplished under circulatory arrestor low-flow continuous CPB and carries a mor-tality rate of approximately 16%.
Transposition of the Great Arteries The neonate with discordant ventriculoarterial
connections is dependent on intracardiac mix-ing for survival and typically presents withcyanosis at birth. Initial management of transpo-sition of the great arteries with prostaglandin E1and balloon septostomy to increase atrial mixingis life-sustaining, but the mortality rate withoutsurgical repair is very high. Initial complete repairis optimal if it can be done within the first 30 daysof life. Correction involves the redirection of sys-temic venous blood to the pulmonary circulationand pulmonary venous blood to the systemicarterial circulation. Over the years, numerous
surgical approaches have been proposed for cor-rection of transposition of the great arteries.Based on the outcomes obtained at numerouscenters, the surgical approach of choice today isthe arterial switch procedure (Fig. 46-5). Mortali-ty rates have steadily declined since the arterialswitch procedure has become widely accepted.
Truncus Arteriosus Truncus arteriosus, a relatively uncommon
defect (0.21–0.34% of those with congenitalheart disease), consists of a single semilunarvalve (the truncal valve) that regulates outflowfrom the single arterial trunk (rather than normallyseparate LV and RV outflow tracts) to the aorta,pulmonary arteries, and coronary circulation.The single arterial trunk overrides the interven-tricular septum. Left-to-right shunting occurs via aVSD and the aortopulmonary connection.
CONGENITAL HEART DISEASE
SURGICAL INTERVENTIONS FOR CONGENITAL HEART DISEASE
462
Stage IIIA modified Fontan procedure is completed 6–12 months after stage II utilizing an extracardiac GORE-TEX� conduit to connect inferior vena cava blood flow to the pulmonary artery
Superior vena cava
Right pulmonary artery
GORE-TEX� conduit
Neoaorta
Pulmonary artery
Extracardiac conduit
Closure of right atrium
Closed purse string for bypass cannula in IVC
Systemic venous blood bypasses the right heart directly to the pulmonary arteries and lungs. Oxygenated blood is pumped from the left to right atrium through a septotomy. The “neoaorta” directs oxygenated systemic blood flow from the right ventricle.
Initial steps
Norwood Correction of HLHS: Fontan CirculationFigure 46-3

CONGENITAL HEART DISEASE
SURGICAL INTERVENTIONS FOR CONGENITAL HEART DISEASE
463
Deoxygenated blood
Patent ductus arteriosus
Stenotic pulmonary artery
Oxygenated blood
VSD with right to left shunt
Right ventricular hypertrophy
Ligated ductus arteriosus
Stenotic pulmonary trunk
Stenotic pulmonary valve
Aortic and mitral valve seen through VSD
Hypertrophied right ventricle
GORE-TEX� graft with pledgets
Retracted tricuspid valve
Pulmonary valvotomy followed by pericardial patch to reduce stenosis
Pericardial patch to reduce subpulmonic stenosis
Tetralogy of FallotFigure 46-4

CONGENITAL HEART DISEASE
SURGICAL INTERVENTIONS FOR CONGENITAL HEART DISEASE
464
Patients are occasionally cyanotic at birth butmost often develop symptoms of CHF within thefirst weeks of life. Surgical repair can be accom-plished safely in the neonatal period (Fig. 46-6).The mortality rate for untreated truncus arterio-sus is as high as 65% at 6 months of age and 75%at 1 year.
Pediatric Heart TransplantationThe success of pediatric cardiac transplanta-
tion is highest in the neonatal period. For HLHSor primary cardiomyopathies, the 5-year survivalrate after transplantation is greater than 80%.Pediatric heart transplantation has been per-formed in more than 3500 children since the late1960s. Congenital heart disease indications fortransplantation are HLHS, severe Ebstein’sanomaly, pulmonary atresia with intact ventricu-lar septum, unbalanced AV canal, single ventriclewith subaortic stenosis, complex truncus arterio-sus, and double-inlet left ventricle. Of the trans-plantation rates for the two broad categories ofindications for heart transplantation in children,
the rates of transplantation for congenital heartdisease have recently reached and surpassed therates for cardiomyopathy, the previously morecommon indication for transplantation.
The major drawback to cardiac transplantationas an answer to end-stage disease is the availabil-ity of donors, with a potential recipient to donorratio of approximately 15:1. Two risk factors havebeen identified for death while waiting on the car-diac transplantation list: status 1 at listing (ICUpatients on inotropic agents) and ventilatordependence. An obstacle to long-term survivalafter cardiac transplantation, besides rejection, isthe development of graft coronary disease, whichoccurs in 2 to 30% of patients at 1 year after trans-plantation and in up to 50% of patients at 5 years.Rejection accounts for approximately 30% ofdeaths in children who have undergone hearttransplantation. Developments in the field ofimmunosuppression and improvements in graftpreservation and operative techniques haveresulted in much improved outcomes, and fur-ther advances in these areas are on the horizon.
Systemic venous blood bypasses the right heart directly to the pulmonary arteries and lungs. Oxygenated blood is pumped from the left to right atrium through a septotomy. The “neoaorta” directs oxygenated systemic blood flow from the right ventricle.
Ligamentum arteriosum divided
Aorta divided
LCA with button resected from the aorta
The aorta and the pulmonary artery are transected. The cut of the aorta is slanted and above the Valsalva’s sinuses. The pulmonary artery is divided above its valve at the same level of the transection of the aorta. Sinuses of the pulmonary artery and aorta are excised to translocate the coronary ostia from the pulmonary artery to the neo-aorta. Pericardium is utilized to reconstruct the neo-pulmonary artery sinuses.
Coronary arteries anastomosed to pulmonary artery
Distal pulmonary artery
Aorta repaired with pericardial patches
Initial steps
Final steps
Arterial Repair of Transposition of the Great ArteriesFigure 46-5

CONGENITAL HEART DISEASE
SURGICAL INTERVENTIONS FOR CONGENITAL HEART DISEASE
465
Ligated ductus arteriosus
Bisected pulmonary trunk
Right ventriculotomy exposes aortopulmonary valve through VSD
Common aortopulmonary trunk with single large valve
Oxygenated blood
Deoxygenated blood
VSD
Running closure of aortic wall
Care is taken not to damage the cardiac conduction system when sewing GORE-TEX� graft over the inferior rim of the VSD
Homograft with semilunar valve connects right ventricle with pulmonary artery bifurcation
Pericardial patch over closure of right ventriculotomy
Truncus ArteriosusFigure 46-6
FUTURE DIRECTIONSResearch in the field of perinatology and the
development of prenatal diagnostic modalitieshave led to advances in fetal heart surgery.Improvements in fetal Doppler ultrasound nowpermit diagnosis of fetal heart disease as early as
10 to 14 weeks of life. Antenatal intervention infetal heart disease is an emerging, but yetunproven field. To date, published informationabout antenatal interventions has been limitedto isolated case reports of balloon valvuloplastyfor severe semilunar valvular obstruction, per-

CONGENITAL HEART DISEASE
SURGICAL INTERVENTIONS FOR CONGENITAL HEART DISEASE
466
formed with minimal success. There are reportsof attempted pulmonic valvular dilatation ante-natally in pulmonary atresia with intact ventricu-lar septum and of attempted transuterine percu-taneous pacemaker lead placement forcongenital complete heart block. Future direc-tions involve further development of transuter-ine as well as transumbilical approaches to fetalheart disease.
REFERENCESAllen HD, Gutgesell HP, Clark EB, Driscoll DJ, eds. Moss and
Adams’ Heart Disease in Infants, Children, and Adoles-cents. Vol 1. 5th ed. Baltimore: Williams & Wilkins; 1995.
Ebert PA, Turley K, Stanger P, Hoffman JI, Heymann MA,Rudolph AM. Surgical treatment of truncus arteriosus inthe first 6 months of life. Ann Surg 1984;200:451–456.
Kohl T, Sharland G, Allan LD, et al. World experience of per-cutaneous ultrasound-guided balloon valvuloplasty inhuman fetuses with severe aortic valve obstruction. Am JCardiol 2000;85:1230-1233.
LeBlanc JG, Russell JL. Pediatric cardiac surgery in the 1990s.Surg Clin North Am 1998;78:729–747.
Nichols DG, Cameron DE, Greeley WJ, Lappe DG, Unger-leider RM, Wetzel RC, eds. Critical Heart Disease in Infantsand Children. St. Louis, MO: Mosby; 1995.
Saiki Y, Rebeyka IM. Fetal cardiac intervention and surgery.Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu2001;4:256–270.
Soto B, Becker AE, Moulaert AJ, Lie JT, Anderson RH. Classi-fication of ventricular septal defects. Br Heart J1980;43:332–343.
Townsend CM, Beauchamp DR, Evers MB, et al, eds. SabistonTextbook of Surgery: The Biological Basis of Modern Surgi-cal Practice. 16th ed. Philadelphia: WB Saunders; 2001.
Wilcox BR, Anderson RH. Surgical Anatomy of the Heart.2nd ed. New York: Gower Medical Publishing; 1992.