Embed Size (px)
Citation preview
CHAPTER-I ANTI-
COAGULANTS
Year III Pharm.DDr. V. Chitra
COAGULATION
Platelets and clotting factors are responsible for initiating coagulation. When an injury occurs, platelets (thrombocytes) immediately migrate to the damaged area. Because platelets stick to each other (aggregation) and to the vessel walls (adhesion), they form a plug around the injured tissue. Plasma clotting factors reach the platelet plug and interact with each other to form a stable blood clot. Hemostasis is the balance between clot formation and clot breakdown that occurs throughout the day.
1-2
ANTICOAGULANT MECHANISM OF ACTION
Interfere with plasma clotting factorsAnticoagulants
Inhibit platelet aggregationAntiplatelets
Dissolve clotsThrombolytics
27-3
ANTICOAGULANTS
The clinically useful anticoagulants produce their pharmacological response by interfering with plasma clotting factors, inhibiting platelet aggregation, or dissolving clots.
1-4
ANTICOAGULANTSThe mechanism of anticoagulation determines the onset and duration of drug action. Heparin has a quick onset and duration of action because the anticoagulant effect occurs as soon as the thromboplastin-drug complex is formed. Warfarin has a long onset and duration of action because it takes days to clear the normal clotting factors before an effect can be observed.
1-5
ANTIPLATELETS
Antiplatelet drugs inhibit platelet aggregation so the platelet plug does not form, or they block platelet adhesion so the plug does not attach to the wall of the blood vessel and block blood flow. These drugs make the platelets less sticky by directly inhibiting adenosine diphosphate (ADP)–mediated platelet aggregation.
1-6
THROMBOLYTICS
Thrombolytics either complex with the plasminogen activator proteins (streptokinase) or the activator protein, tPA, tissue plasminogen activator Interfering with stage four of clot formation
1-7
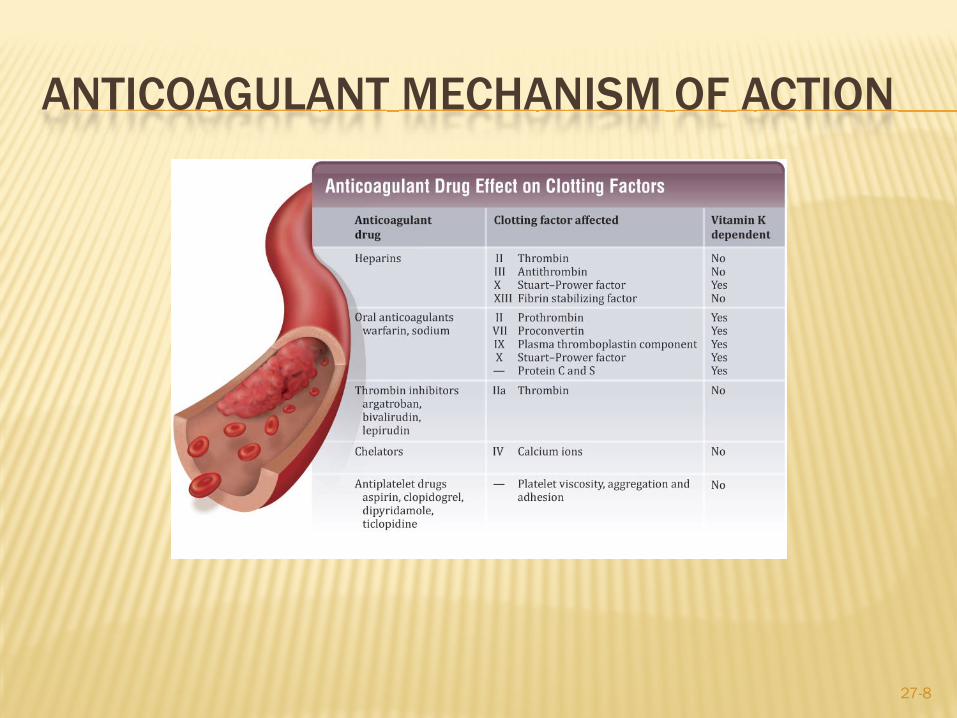
ANTICOAGULANT MECHANISM OF ACTION
27-8
HEPARINS
Standard heparins and LMW heparins:Bind antithrombinIncrease inactivation of factor X
LMW heparins are more effective at binding active factor X.
Standard heparin is more effective at inactivating factor XIII and binding thrombin.NOT interchangeable
27-9
HEPARINSMajor toxicity is hemorrhage. (black box warning, epidural or spinal hematomas with anesthesia)
At high doses:PetechiaeBleeding from open wounds
Other side effects:Fever, alopecia, osteoporosis, and thrombocytopenia
Heparin antidote:Protamine sulfate (binds to heparin)
27-10
ORAL ANTICOAGULANTS—COUMARIN
Coumarin:
Discovered from spoiled sweet clover
Action on clotting factors II, VII, IX, & X
Onset of activity slow—12 to 72 hours
Duration of action long—2 to 10 days
27-11
ORAL ANTICOAGULANTS—COUMARINSide effects:
Nausea and diarrheaHypotensionFatigueAlopecia
Major toxicity is hemorrhage.Mephyton is the antidote (vitamin K) with plasma
Crosses placenta:May cause hemorrhage in fetus
27-12
ANTIPLATELET DRUGS
The oral antiplatelets include:Thromboxane is a potent platelet aggregator and vasoconstrictor
AspirinAlters cyclooxygenase needed to generate thromboxaneIrreversible, need new platelets to form (can happen in a few hours)
27-13
ANTIPLATELET DRUGS
Clopidogrel (Plavix) and Ticlopidine (Ticlid)Block adenosine diphosphate (receptor on platelet cell membranes important for platelet aggregation), binding and preventing activation of glycoproteins IIa/IIIB (receptor for fibrinogen and fibronectin) important in the crosslinking of platelets to fibrin.
1-14
ANTIPLATELET DRUGS
Dipyridamole (Persantine)Increases extracellular adenosine (inhibitor of platelet reactivity) by decreasing reuptake of adenosine in platelets, RBC’s, and endothelial cells Inhibits phosphodiesterase enzyme, increasing cAMP in the cell and blocking platelet response to ADP
1-15
ANTIPLATELET DRUGS
Side effects include:HeadacheVomitingRashDizzinessDiarrhea
Ticlopidine and clopidogrel can cause:Thrombocytopenia
27-16
SPECIAL CONSIDERATIONS
Anticoagulant therapy should be administered at the same time each day.
Patients should be carefully observed for signs of increased bleeding or hemorrhage.
All heparin vials should be examined carefully to determine correct strength.
Any patient with active bleeding should not receive anticoagulants.
27-17
MONITORING COAGULATION
Therapeutic dosage is maintained and evaluated based on clotting time:
Partial thromboplastin time (PTT)Prothrombin time (PT)International normalized ratio (INR)Activated partial thromboplastin time (APTT)
Drugs that affect platelet aggregation can cause increased bleeding.
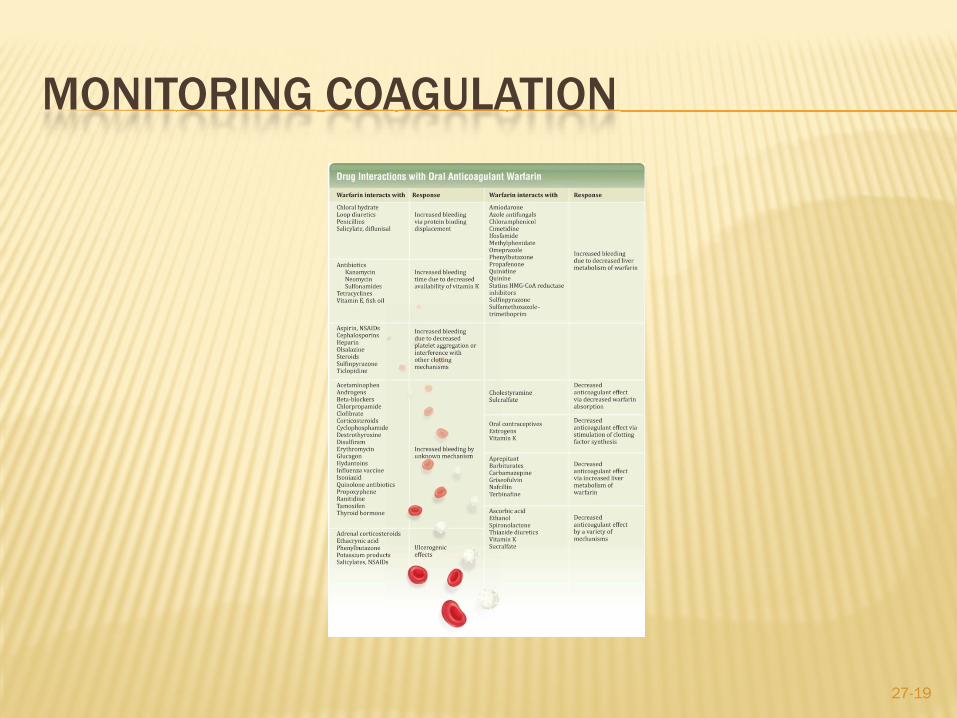
Warfarin has the greatest potential for drug interactions.
27-18
MONITORING COAGULATION
27-19
FIBRINOLYTIC/THROMBOLYTIC DRUGS
Clot busters:Dissolve preformed blood clots
Include the following drugs:Urokinase, streptokinase, alteplase, tenecteplase, reteplase
They are used to lyse pulmonary and coronary artery thrombosis.Major adverse effect is hemorrhage.
27-20
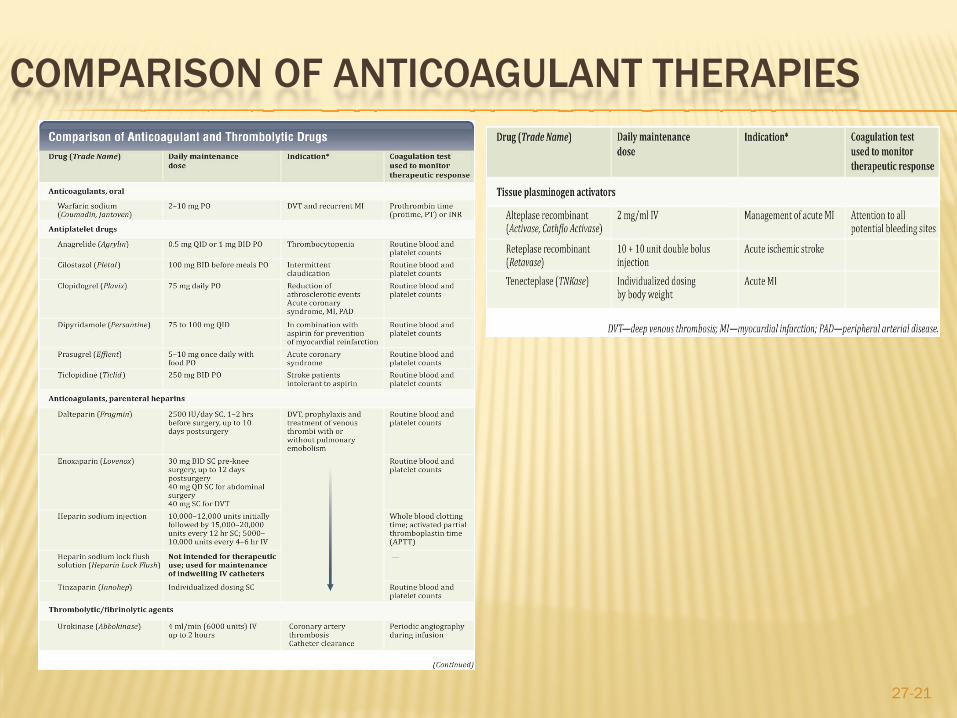
COMPARISON OF ANTICOAGULANT THERAPIES
27-21
PREFERRED THERAPY
Heparin: Venous thrombosis and pulmonary embolism
Warfarin:Prophylaxis of venous thrombosis and pulmonary emboli
Antiplatelets:Coronary artery disease
Thrombolytics:Dissolution of preformed clots


![[Product Monograph Template - Standard] · PDF fileCAMBIA® (diclofenac potassium) Product Monograph Page 8 of 33 ... • Anti-coagulants (e.g. warfarin) • Anti-platelet agents (e.g](https://img.pdfslide.net/doc/110x75/5aa1a3e67f8b9a436d8bddd4/product-monograph-template-standard-diclofenac-potassium-product-monograph.jpg)