Embed Size (px)
Citation preview

© 2007 International Society of Travel Medicine, 1195-1982Journal of Travel Medicine, Volume 14, Issue 5, 2007, 320–325
320
Chikungunya — pronounced chik-n-gunya, with the accent on the fi rst syllable — is an alphavi-
rus that causes disease in Africa and Asia. The name chikungunya is derived from the Makonde word meaning “ that which bends up. ” This is in reference to the stooped posture that develops from the ar-thritic symptoms of the disease. However, some au-thors overlooked this reference and assumed that the term was derived from Swahili (a native lan-guage of East Africa and now the offi cial language of Tanzania).
Chikungunya viral disease was fi rst described in Tanzania in 1952 to 1953. 1 – 3 Since then, the out-breaks have been reported from Africa and many parts of Asia. 4 – 6 In 1958, the virus was fi rst isolated in Asia from Bangkok, Thailand. 7 Asian countries that have reported chikungunya activity include Thailand, Cambodia, Vietnam, Laos, Indonesia, Malaysia, Myanmar, India, Sri Lanka, and the Philippines. 8 – 19
In recent months, large outbreaks of chikungu-nya viral infections have been reported from India and from some smaller islands in the Indian Ocean. Aedes aegypti and Aedes albopictus mosqui-toes, which act as vectors for chikungunya viral infections, are widely distributed in several South and Southeast Asian countries. These same vec-tors transmit the dengue virus. 20,21 Large numbers of people travel between India, the Indian Ocean islands, and the neighboring countries, and it is to
REVIEW
Chikungunya Viral Infections: An Emerging Problem
Suranjith L. Seneviratne , MRCP , * Padmalal Gurugama , MBBS , † and Jennifer Perera , MD ‡ * Department of Clinical Immunology, John Radcliffe Hospital, Oxford, UK ; † Professorial Medical Unit, Teaching Hospital Peradeniya, Kandy, Sri Lanka ; ‡ Department of Microbiology, University of Colombo, Colombo, Sri Lanka
DOI: 10.1111/j.1708-8305.2007.00135.x
S. L. S. and J. P. contributed equally to this review.
Corresponding Author: Dr Suranjith L. Seneviratne, MRCP, Department of Clinical Immunology, John Radcliffe Hospital, Headington, Oxford OX3 9DU, UK. E-mail: suran200@ yahoo.co.uk
be expected that cases of chikungunya infection would spread to other countries in the region. These countries are also popular tourist destina-tions, and patients may present on their return with a “ dengue-like illness ” due to a chikungunya viral infection. In fact, it is possible that clinicians are already seeing such patients but incorrectly assuming their symptoms as due to the dengue vi-rus. Several imported cases of chikungunya infec-tion have already been reported from different European countries. 22,23
In this short review, we describe aspects relating to the recent outbreaks of chikungunya infection in some South Asian countries, the detection of im-ported cases in several European countries, the chi-kungunya virus and its mosquito vector, and the clinical manifestations, diagnosis, and treatment of these infections.
Recent Outbreaks of Chikungunya Viral Infections
Recently, India and several islands in the Indian Ocean such as the French Reunion Islands, Mauri-tius, and Seychelles have been reporting large num-bers of patients with chikungunya viral infection. 24 – 26 Estimates suggest that since December 2005, more than 200,000 cases have occurred in India. Andhra Pradesh was the fi rst state to report a reemergence of this infection. 26 Of 362 serum samples collected in this state and tested at the National Institute of Virol-ogy, Pune, 139 had been positive for chikungunya an-tibodies, six for dengue antibodies, and 15 for both. 15
The Reunion Island epidemic began in March 2005, and by January 2006, an estimated 1,200 new cases were seen each week. 25 Some reports suggest that by May 2006, nearly 255,000 people (of 777,000

321
J Travel Med 2007; 14: 320–325
Chikungunya Infections in Travelers
residents) in Reunion had been affected and that 77 deaths were associated with chikungunya infec-tion. 27 – 29 In neighboring Mauritius, 3,500 cases were reported in 2005. 25 Initially, most of the patients had a history of travel to Reunion, but later cases oc-curred without a specifi c travel history. Since No-vember 2005, an increasing number of cases have also been reported from Seychelles, Mayotte, Comoros, Madagascar, and Malaysia. Furthermore, since March 2005, 123 cases with a confi rmed chi-kungunya infection have developed severe clinical signs (neurological signs or fulminant hepatitis) and needed treatment in an intensive care setting.
Estimates from 2004 suggest that nearly 1.5 million people travel from Mauritius, Reunion, Seychelles, Mayotte, and Madagascar to main-land Europe each year. Thus, it is likely that large numbers of infected people may be importing the virus into Europe. Furthermore, A albopictus , the main mosquito vector in the Reunion epidemic, is already found in several European countries. 30 However, at present, the exact vectorial compe-tence and effi cacy of virus transmission of these vec-tors in Europe are not known.
From April 1, 2005, to February 28, 2006, 307 imported cases of chikungunya have been identifi ed in France. 22 Most imported cases were seen in pa-tients living in the Provence-Alpes-Cote d ’ Azur re-gion in Southeast France, which is home to a large Comorian community. None of the imported cases in France developed serious manifestations. In ad-dition, imported cases have also been reported in Germany, UK, Belgium, Switzerland, Norway, China, and the Czech Republic. 23 In March 2006, a nurse in France, who had never traveled to the Indian Ocean, developed a laboratory-confi rmed chikungunya infection 3 days after caring for a patient with an imported infection. Laboratory transmission of chikungunya infection has been previously reported. 31,32
Reasons for the reemergence of chikungunya in-fections in India and islands in the Indian Ocean are unclear. Studies on virus isolates from the current outbreak suggest that specifi c viral gene mutations may in some way facilitate its large-scale spread in the region. Alternatively, the lack of herd immunity in these regions may have contributed to its rapid spread across states and countries.
The Chikungunya Virus and its Mosquito Vector
The chikungunya virus, a positive strand, enveloped RNA virus, is a member of the Alphavirus genus and
belongs to the Togaviridae family. 33 It is endemic in large parts of Africa, the Middle East, India, and South-East Asia and is closely related to O ’ nyong-nyong viruses. 34
Khan and colleagues have studied the complete nucleotide sequence of the S27 African prototype chikungunya virus. 35 They found its genome to be similar in structure to that of other alphaviruses, and the presence of an internal polyadenylation site within the 3 ′ nontranslated region. Genetic analysis of chikungunya viruses based on partial E1 enve-lope glycoprotein gene sequences from African and Asian isolates showed the presence of three distinct phylogroups. 36 The fi rst contained all isolates from West Africa; the second comprised all Southern, Eastern, and Central African strains; and the third contained isolates from Asia. Historical evidence that the virus originated in Africa and was subse-quently introduced into Asia was confi rmed by phy-logenetic tree analysis. 36
Schuffenecker and colleagues 37 investigated changes in the viral genome of chikungunya viruses isolated from the present outbreak, with a view to understanding its unusual virulence that has re-sulted in unexpected morbidity and mortality pat-terns. They suggest that the outbreak began with a strain related to the East African strains of the virus. All the recent Indian Ocean sequences examined were found to share certain areas, which were dif-ferent from the previously determined sequences.
Numerous mosquito species are involved in the maintenance of chikungunya viral infections in Africa. 38 – 40 For example, in Senegal, Aedes furcifer , Aedes taylori , Aedes luteocephalus , Aedes africanus , and Aedes neoafricanus were determined to be of major importance in maintaining chikungunya vi-rus transmission cycles. In Asia, chikungunya virus is transmitted from human to human mainly by A aegypti and to a lesser extent by A albopictus through an urban transmission cycle. Aedes albopictus has been the species implicated in the recent major epidemic in Reunion. Outbreaks typically occur dur-ing the rainy season when vector densities tend to rise.
Clinical Manifestations
Chikungunya infection is characterized by abrupt onset fever, severe arthralgia, rash, and other con-stitutional symptoms. 41 Headache, conjunctival injection, and slight photophobia may occur. Generalized myalgia with back and shoulder pain is common, and lymphadenopathy occurs fre-quently. 16 The incubation period is between 2 and

J Travel Med 2007; 14: 320–325
322 Seneviratne et al.
10 days (usually 2 – 3 d), and the illness lasts for be-tween 1 and 7 days.
The fever (39 – 40°C) is often accompanied by in-termittent shaking chills. A “ saddle-back ” fever pat-tern may occur (an acute phase lasting 2 – 3 d, remitting for 1 – 2 d, before developing fever again). Joint involvement is usually symmetrical, polyar-ticular, and migratory and predominantly affects small joints of the hands, wrists, ankles, and feet. 42 Larger joints are less frequently involved. Periar-ticular swelling, pain, redness, and limitation of movement may be seen. The pain on movement is worse in the morning, improved by mild exercise and exacerbated by strenuous exercise. Fluid accu-mulation in the joints is uncommon. Patients with milder articular manifestations are usually symp-tom free within a few weeks, but more severe cases may take months to resolve. 43
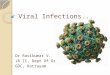
Skin manifestations are typical. Many present with fl ushing, affecting their face and trunk. A mac-ulopapular or petechial rash primarily involving the trunk and limbs can occur with defervescence. The rash may also affect the face, palms, and soles and be accompanied by pruritus. Most patients will have a headache during the acute disease, although it is usually not very severe. Photophobia and retroor-bital pain may also occur. Some have conjunctival injection, and others complain of a sore throat due to pharyngeal infl ammation. During the recent outbreak in Reunion and in the fi rst outbreak in India, neurological complications such as meningo-encephalitis were seen in a small proportion. 27,44 Mother to child transmission of chikungunya virus has been seen in the recent Reunion Island out-break. 45 Chikungunya infection tends to present differently in younger patients. The arthralgia and arthritis appear to be less prominent and last for a shorter time. The rash is also seen less frequently.
Previous reports on chikungunya infection sug-gest that it is often a self-limiting illness. Most pa-tients recover completely over a period of a few weeks. However, 5% to 10% of patients experience chronic joint pain, stiffness, and swelling lasting a year or more. The present outbreak appears to be more severe than previous ones, as several patients have developed complications and some deaths have also been reported.
Clinical manifestations of chikungunya infec -tion may be clinically indistinguishable from those due to dengue. 46 In Asia, the chikungunya virus has been isolated from children having an illness very similar to Dengue Haemorrhagic Fever (DHF). Dual infections may also occur, where both dengue and chikungunya have been simultaneously iso lated
from the same patient. 47 Hemorrhagic manifesta-tions in chikungunya have been described parti-cularly among cases in South-East Asia and the Indian subcontinent. 48 – 51 These are milder and less common when compared with dengue. Classically, shock does not occur.
Diagnosis
Chikungunya infection should be suspected clini-cally when the characteristic triad of fever, rash, and rheumatic manifestations is present. Leucopenia is typical, and there may be a relative monocytosis. Thrombocytopenia occurs frequently. The main differential is between dengue and O ’ nyong-nyong fevers. It has been suggested that dengue is charac-terized by more myalgia than arthralgia. Labora-tory tests are needed for defi nitive diagnosis.
Virus isolation by inoculation of mosquitoes, mosquito or mammalian cell cultures, or suckling mice is possible. Most patients have viremia during the fi rst 48 hours of illness, but this may persist for up to 4 days in some patients. In patients recovering from chikungunya infection, virus-specifi c immu-noglobulin M antibodies are readily detected by cap-ture enzyme-linked immunosorbent assay. These may persist for more than 6 months. Hemagglutina-tion inhibition (HI) antibodies appear when viremia ceases and are generally positive by day 5 to day 7 of illness. Neutralization and HI antibodies tend to parallel each other. Polymerase chain reaction - based techniques are also available for diagnosis. 52 – 55
Treatment
No specifi c treatment is available for chikungunya viral infections. The illness is usually self-limiting. However, the recent epidemic in several South Asian countries appears to be resulting in greater morbidity and even some deaths. It is important to exclude other dangerous diseases such as dengue. Rest helps the acute joint symptoms. Movement and mild exercise tend to improve morning stiffness and arthralgia, but severe exercise may worsen the arthralgia. Analgesics and anti-infl ammatory drugs are useful. However, care is needed when using these drugs as the chikungunya virus is capable of causing thrombocytopenia. More than 12% of patients develop chronic joint symptoms, which respond only partially to the nonsteroidal anti- infl ammatory drugs (NSAIDs).
Chloroquine phosphate (250 mg/d) has been found to be useful in arthritis refractory to aspirin or NSAIDs. An open pilot study to assess its effi cacy

323
J Travel Med 2007; 14: 320–325
Chikungunya Infections in Travelers
was done in 10 patients, with treatment given for 20 weeks. 56 Both joint symptoms and morning stiffness improved signifi cantly. Seven of the ten patients considered their symptoms as improved. It is possi-ble that hydroxychloroquine would be useful as treatment in this setting. Hydroxychloroquine has been extensively used in rheumatological practice and is less toxic to the eyes than chloroquine.
No vaccine is currently available. A phase II, ran-domized, double-blind, placebo-controlled safety and immunogenicity study of live chikungunya vi-rus vaccine SI-GSD-218 was conducted in 73 healthy adult volunteers and found to be safe and highly immunogenic. 57 However, funding for this project appears to have been discontinued. Travel-ers to affected areas should be advised to take anti-mosquito measures. Aedes aegypti female mosquitoes have two periods of peak biting activity, which are a few hours after dawn and in the late afternoon around dusk. 58 It would be advisable for pregnant women, the elderly, and those with signifi cant med-ical conditions not to travel to countries affected by the present chikungunya epidemic as meningoen-cephalitis has been described in neonates of women infected a few days before giving birth and in the el-derly among the recent cases in the Indian Ocean.
Conclusions
Health personnel in South Asia and South-East Asia are likely to come across patients with chikun-gunya viral infections, especially following the re-cent large outbreaks in some countries of the region. It is an important differential in patients presenting with a dengue-like illness, where dengue testing has proved negative. These countries are also popular tourist destinations, and patients may present on their return with a dengue-like illness due to a chi-kungunya viral infection. Several imported cases of chikungunya have already been reported from countries in Europe. Knowledge of aspects of this disease should allow the condition to be suspected and treated appropriately.
Declaration of Interests
The authors state that they have no confl icts of interest.
References
1. Robinson MC . An epidemic of virus disease in South-ern Province, Tanganyika Territory in 1952 – 53. 1.
Clinical features . Trans R Soc Trop Med Hyg 1955 ; 49 : 28 – 32 .
2. Lumsden WHR . An epidemic disease in Southern Province, Tanganyika Territory, in 1952 – 53. 11. General description and epidemiology . Trans R Soc Trop Med Hyg 1955 ; 49 : 33 – 57 .
3. Ross RW . The Newala epidemic. III. The virus: iso-lation, pathogenic properties and relationship to the epidemic . J Hyg 1956 ; 54 : 177 – 191 .
4. Pastorino B , Muyembe-Tamfum JJ , Bessaud M , et al . Epidemic resurgence of Chikungunya virus in Democratic Republic of the Congo: identifi cation of a new Central African strain . J Med Virol 2004 ; 74 : 277 – 282 .
5. Muyembe-Tamfum JJ , Peyrefi tte CN , Yogolelo R , et al . Epidemic of chikungunya virus in 1999 and 2000 in the Democratic Republic of the Congo . Med Trop (Mars) 2003 ; 63 : 637 – 638 .
6. Mackenzie JS , Chua KB , Daniels PW , et al . Emerg-ing viral diseases of Southeast Asia and the Western Pacifi c . Emerging Infect Dis 2001 ; 7 : 497 – 504 .
7. Hammon WM , Rudnick A , Sather GE . Viruses associated with hemorrhagic fevers of the Philip-pines and Thailand . Science 1960 ; 131 : 1102 – 1103 .
8. Thaikruea L , Charearnsook O , Reanphumkarnkit S , et al . Chikungunya in Thailand: a re-emerging dis-ease? Southeast Asian J Trop Med Public Health 1997 ; 28 : 359 – 364 .
9. Halstead SB , Scanlon JE , Umpaivit P , et al . Dengue and Chikungunya virus infection in man in Thailand, 1962 – 1964. IV. Epidemiologic studies in the Bangkok metropolitan area . Am J Trop Med Hyg 1969 ; 18 : 997 – 1021 .
10. Laras K , Sukri NC , Larasati RP , et al . Tracking the re-emergence of epidemic chikungunya virus in Indonesia . Trans R Soc Trop Med Hyg 2005 ; 99 : 128 – 141 .
11. Porter KR , Tan R , Istary Y , et al . A serological study of chikungunya virus transmission in Yogyakarta, Indonesia: evidence for the fi rst outbreak since 1982 . Southeast Asian J Trop Med Public Health 2004 ; 35 : 408 – 415 .
12. Lam SK , Hua KB , Hooi PS , et al . Chikungunya in-fection — an emerging disease in Malaysia . South-east Asian J Trop Med Public Health 2001 ; 32 : 447 – 451 .
13. Thaung U , Ming CK , Swe T , et al . Epidemiological features of dengue and chikungunya infections in Burma . Southeast Asian J Trop Med Public Health 1975 ; 6 : 276 – 283 .
14. Neogi DK , Bhattacharya N , Mukherjee KK , et al . Sero-survey of chikungunya antibody in Calcutta metropolis . J Commun Dis 1995 ; 27 : 19 – 22 .
15. Ravi V . Re-emergence of Chikungunya virus in India . Indian J Med Microbiol 2006 ; 24 : 83 – 84 .
16. Munasinghe DR , Amarasekera PJ , Fernando CF . An epidemic of dengue-like fever in Ceylon (Chikungu-nya) — a clinical and haematological study . Ceylon Med J 1966 ; 11 : 129 – 142 .

J Travel Med 2007; 14: 320–325
324 Seneviratne et al.
17. Centers for Disease Prevention and Control . Chi-kungunya fever among U.S. Peace Corps volun-teers — Republic of the Philippines . MMWR 1986 ; 35 : 573 – 574 .
18. Ampos LE , San Juan A , Cenabre LC , et al . Isolation of chikungunya virus in the Philippines . Acta Med Philipina 1969 ; 46 : 235 – 242 .
19. Macasaet FF . Further observation on chikungunya fever . J Philipp Med Assoc 1970 ; 46 : 235 – 242 .
20. Malavige GN , Fernando S , Fernando DJ , et al . Dengue viral infections . Postgrad Med J 2004 ; 80 : 588 – 601 .
21. Seneviratne SL , Malavige GN , de Silva HJ . Patho-genesis of liver involvement during dengue viral in-fections . Trans Roy Soc Trop Med Hyg 2006 ; 100 : 608 – 614 .
22. Cordel H , Quatresous I , Paquet C , et al . Imported cases of chikungunya in metropolitan France, April 2005 – February 2006 . Euro Surveill 2006 ; 11(4) : E060420.3 .
23. Pfeffer M , Locher T . Cases of chikungunya imported into Europe . Euro Surveill 2006 ; 11(3) : E060316 .2 .
24. Enserink M . “ Massive outbreak draws fresh atten-tion to little-known virus ” . Science 2006 ; 311 : 1085 .
25. World Health Organization . Chikungunya and Dengue in the south-west Indian Ocean . Epidemic and Pandemic Alert and Response (EPR) . Geneva:WHO, 2006 .
26. Centers for Disease Control . Chikungunya Fever in India . Travelers ’ Health Outbreak Notice April 21 , 2006 .
27. Quatresous I . Chikungunya outbreak in Reunion, a French ‘ overseas department ’ . Euro Surveill 2006 ; 11 : 060202 .
28. Paquet C , Quatresous I , Solet JL , et al . Chikungunya outbreak in Reunion: epidemiology and surveillance, 2005 to early January 2006 . Euro Surveill 2006;11:060202 .
29. Cordel H . Chikungunya outbreak on Reunion: up-date . Euro Surveill 2006 ; 11 : 060302 .
30. Depoortere E , Coulombier D , on behalf of the ECDC Chikungunya risk assessment group. Chi-kungunya risk assessment for Europe: recommen -dations for action . Euro Surveill 2006 ; 11 : 060511 .
31. Shah KV , Baron S . Laboratory infection with chikungunya virus: a case report . Indian J Med Res 1965 ; 53 : 610 – 613 .
32. Ramachandra RT , Singh KR , Pavri KM . Laboratory transmission of an Indian strain of Chikungunya vi-rus . Curr Sci 1964 ; 33 : 235 – 236 .
33. Karabatsos N . International catalogue of Arbovi-ruses . 3rd Ed . San Antonio, TX : American Society of Tropical Medicine and Hygiene , 1985 .
34. Blackburn NK , Besselaar TG , Gibson G . Antigenic relationship between Chikungunya virus strains and O ’ nyong nyong virus using monoclonal antibodies . Res Virol 1995 ; 146 : 69 – 73 .
35. Khan AH , Morita K , Parquet Md Mdel C , et al . Complete nucleotide sequence of chikungunya virus and evidence for an internal polyadenylation site . J Gen Virol 2002 ; 83 : 3075 – 3084 .
36. Powers AM , Brault AC , Tesh RB , et al . Re- emergence of Chikungunya and O ’ nyong-nyong viruses: evi-dence for distinct geographical lineages and distant evolutionary relationships . J Gen Virol 2000 ; 81 : 471 – 479 .
37. Schuffenecker I , Iteman I , Michault A , et al . Genome microevolution of Chikungunya viruses causing the Indian Ocean outbreak . PloS Medicine 2006 ; 3 : e263 .
38. Diallo M , Thonnon J , Traore-Lamizana M , et al . Vectors of Chikungunya virus in Senegal: current data and transmission cycles . Am J Trop Med Hg 1999 ; 60 : 281 – 286 .
39. Vanlandingham D , Tsetsarkin K , Klingler KA , et al . Determinants of vector specifi city of O ’ nyong nyong and chikungunya viruses in Anopheline and Aedes mosquitoes . Am J Trop Med Hyg 2006 ; 74 : 663 – 669 .
40. Vanlandingham D , Hong C , Klingler KA , et al . Dif-ferential infectivities of O ’ nyong-nyong and chikun-gunya virus isolates in Anopheline Gambiae and Aedes aegypti mosquitoes . Am J Trop Med Hyg 2005 ; 72 : 616 – 621 .
41. Jadhav M , Namboodripad M , Carman RH , et al . Chikungunya disease in infants and children in Vellore: a report of clinical and haematological features of virologically proved cases . Indian J Med Res 1965 ; 53 : 764 – 776 .
42. Kennedy AC , Fleming J , Solomon L . Chikungunya viral arthropathy: a clinical description . J Rheumatol 1980 ; 7 : 231 – 236 .
43. Brighton SW , Prozesky OW , de la Harpe AL. Chikungunya virus infection. A retrospective study of 107 cases . S Afr Med 1983 ; 63 : 313 – 315 .
44. Chatterjee SN , Chakravarti SK , Mitra AC , et al . Viro-logical investigation of cases with neurological com-plications during the outbreak of haemorrhagic fever in Calcutta . J Indian Med Assoc 1965 ; 45 : 314 – 316 .
45. Robillard PY , Boumahni B , Gerardin P , et al . Verti-cal maternal fetal transmission of the Chikungunya virus . Ten cases among 84 pregnant women . Presse Med 2006 ; 35 : 785 – 788 .
46. Carey DE . Chikungunya and dengue: a case of mis-taken identity? J Hist Med Allied Sci 1971 ; 26 : 243 – 262 .
47. Myers RM , Carey DE . Concurrent isolation from patient of two arboviruses, Chikungunya and dengue type 2 . Science 1967 ; 157 : 1307 – 1308 .
48. Nimmannitiya S , Halstead SB , Cohen SN , Margiotta MR . Dengue and chikungunya virus infec-tion in man in Thailand, 1962-1964. I. Observations on hospitalised patients with haemorrhagic fever . Am J Trop Med Hyg 1969 ; 18 : 954 – 971 .

325
J Travel Med 2007; 14: 320–325
Chikungunya Infections in Travelers
49. Sarkar JK , Chatterjee SN , Chakravarty SK . Haemorrhagic fever in Calcutta: some epidemio-logical observations . Indian J Med Res 1964 ; 52 : 651 – 659 .
50. Shah KV , Gibbs CJ Jr , Banerjee G . Virological in-vestigation of the epidemic of haemorrhagic fever in Calcutta: isolation of three strains of Chikungunya virus . Indian J Med Res 1964 ; 52 : 676 – 683 .
51. Mourya DT , Thakare JP , Gokhale MD , et al . Isola-tion of Chikungunya from Aedes aegypti mosquitoes collected in town of Yawat , Pune district, Maharash-tra State, India. Acta Virol 2001 ; 45 : 305 – 309 .
52. Hasebe F , Parquet MC , Pandey BD , et al . Combined detection and genotyping of Chikungunya virus by a specifi c reverse transcription-polymerase chain re-action . J Med Virol 2002 ; 67 : 370 – 374 .
53. Pfeffer M , Linssen B , Parker MD , et al . Specifi c de-tection of Chikungunya virus using a RT-PCR/nested PCR combination . J Vet Med B: Infect Dis Vet Public Health 2002 ; 49 : 49 – 54 .
54. Yadav P , Shouche YS , Munot HP , et al . Genotyping of chikungunya virus isolates from India during 1963 – 2000 by reverse transcription-polymerase chain reaction . Acta Virol 2003 ; 47 : 125 – 127 .
55. Pastorino B , Bessaud M , Grandadam M , et al . Devel-opment of a TaqMan RT-PCR assay without the RNA extraction step for the detection and quan-tifi cation of African Chikungunya viruses . J Virol Methods 2005 ; 124 : 65 – 71 .
56. Brighton SW . Chloroquine phosphate treatment of chronic Chikungunya arthritis. An open pilot study . S Afr Med J 1984 ; 66 : 217 – 218 .
57. Edelman R , Tacket CO , Wasserman SS , et al . Phase II safety and immunogenicity study of live Chikun-gunya virus vaccine TSI-GSD-218 . Am J Trop Med Hyg 2000 ; 62 : 681 – 685 .
58. Nelson MJ , Self LS , Pant CP , Slim U . Diurnal peri-odicity of attraction to human bait of Aedes aegyp ti in Jakarta, Indonesia . J Med Entomol 1978 ; 14 : 504 – 510 .
This rash appeared on day 2 of a febrile illness in a patient who presented with myalgia and arthralgia after visiting Mauritius. Chikungunya was confi rmed serologically. Richard Foster, Michael Richardson, Stephen Toovey, South Africa.