Embed Size (px)
Citation preview
Christine Chrisman, APRN-NP, ACNP-BC, HCPN Hospital Medicine
Palliative Care Coordinator
◦ State short-term and long-term effects of long bone and spinal fractures in the geriatric patient
◦ Discuss quality of life after fractures, including potential LTC placement, patient and family teaching
◦ Discuss methods to facilitate family acceptance of the patient’s need for LTC
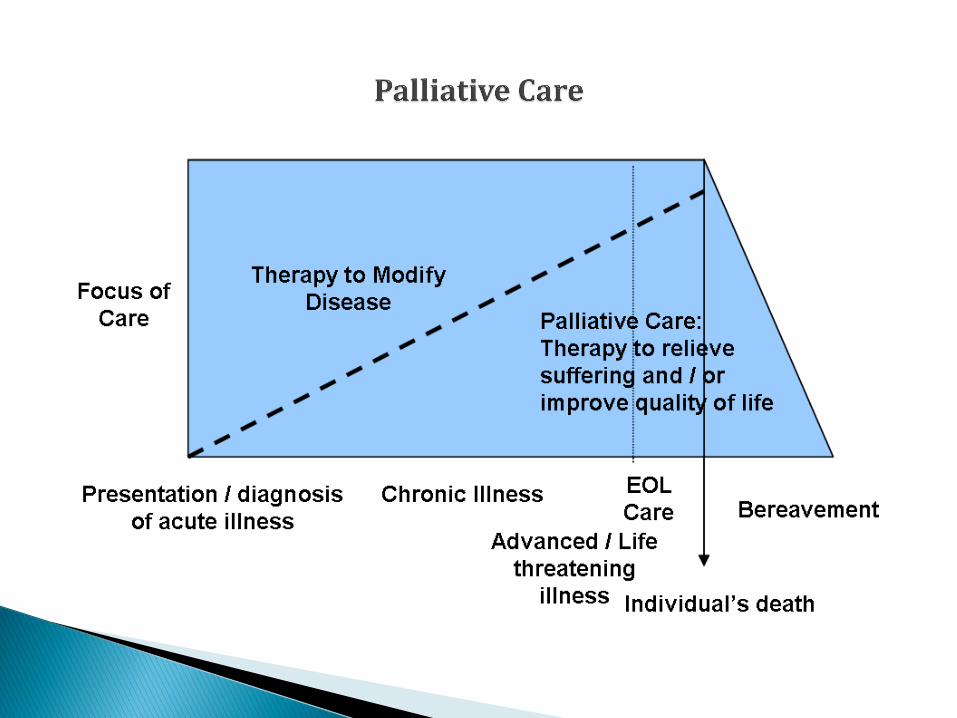
No single definition : multidimensional
Can encompass whole of life
Health- related QOL (HRQOL)
Various measurement tools: Short Form 36; Nottingham Health Profile
Aim is to increase QOL to reduce suffering
Public Health concern –fear of falling and need for earlier screening :
need to touch or hold onto things or people
walks very slowly
takes small steps
limited movement
expresses a fear of falling
increased fear of falling
moves slower
avoids movement – sedentary
muscle weakness/ atrophy/ de-conditioned
decreased strength and endurance
increased risk of falling
Increased risk for falls
Declines in ability to perform ADLS
Declines in gait stability
Increased risk of nursing home admission.
Lower health- related quality of life
Contributes to FRAILTY.

Following screening need for: PREVENTION PT/OT resistance exercise/strengthening/ balance ST for swallowing or cognitive exercises STAR (Survivorship, Training, and Rehab) program Bisphosphonates and Vitamin D PTH Education on home safety, avoid alcohol/nicotine Review medications and avoid polypharmacy Caregiver assistance Vision and nutrition checks
In addition to fear of falling, other predictors: age comorbidities : decreased mobility history of falls previous fracture and hospitalization decreased independence in ADLS more likely to need nursing home placement if
confused or have decreased balance or poor gait or low body mass index or at least 2 chronic conditions [Marks et.al.,2003].
Injury triggers progressive decline in elderly [Farahmand et.al.,2005].
Loss of physiologic reserve /vulnerability or frailty
Impacts mortality: comorbidities : circulatory, cancer, frailty, dementia and age( esp. > 85yrs); risks early and persist up to 5-6 years. [Marks et.al., 2003].
Mortality rate 10-20% and ½ will have long standing disability [Marks et. al.,2003].
Up to 50% do not achieve prefracture level of function at 1 year
< 50% regain ALDs status; [Shumway-Cook et.al. 2005].
80% have difficulty with other activities eg. grocery shopping or driving.
Balance, cognitive ability, & prior functional ability best predictors for return of functional ability 3 months following discharge from rehab facility [Folden & Tappan, 2007].
Timed Up & GO (TUG) predicts 2nd fall in 6months. [Kristensen et.al., 2007].
Femoral /trochanteric hip fractures baseline/4months
- significant deterioration of physical /psychosocial dimensions in elderly; worse with comorbidities. [VanBalen
et.al.,2003]
- partial recovery at end of 4th month with improvement
- 1/3 became totally dependent after injury
- mortality rate of 30% 4months after fracture [Mendonca et.al.,
2008]
Population based case-control study (60) 6-10 months in community s/p hip fx: Short Form 36
All 8 domains adversely affected: physical, social, pain, general health, vitality, and emotional
Required more help with Assisted living tasks and poorer balance. [Jongit et.al., 2003].
Functional Status at hospital discharge
-Most powerful factor influencing QOL
- Surgical emergencies when life threatened or conditions destroy peace/comfort: age should not be a contraindication for surgery [Fierens & Broos, 2006].
QOL after trochanteric femoral fxs treated with gamma nailing
- Good functional results but substantial fall up to 12 months after operation per SHORT FORM-36 for pain, emotional, social, and physical [Giessauf et.al., 2012].
Not always a linear correlation between professionals’ objective functional evaluation and patient’s self-perception of QOL: positive or negative.

Team members and Their Contributions Value of ROUNDS!!
1) Patient/ Family
• Fears – Listen to feelings/coping skills [Gambatesa et.al., 2013]. The elderly hip fracture pt is greater risk for psychological problems r/t trauma.
• Goals: Attention to pain control; Visual Analog Scale; PT/OT goals
• Expectations
• Provide history, activity level, baseline for transitioning to next level of care.
2) Next level of care:
• Safe environment with caregiver assistance
• Provider orders/ recommendations
• Skilled nursing facility or Hospital Swing bed
• Home with Home Care
• Next doctor’s appointment
• Outpatient Rehab Care
• Medication Reconciliation
Find out who the patient is as a person
Get to know them as a family unit to build trust.
Enlist and Communicate with the social worker and chaplain regarding family dynamics, emotions, spiritual life and coping.
Help the patient and family identify and express feelings.
Anxiety “ where will mom go” ? ‘What will happen to (pets)? “Costs?”
Fear: “I’m afraid Dad will give up or die in the nursing home?”
Guilt: “ Why did I not check on Mom?”
Self-blame: “ I should have been more careful”
Sadness/Grief: ( loss) “ I can’t even go to the bathroom by myself”.

Communicate with patient/family during teachable moments to assess perception of patient ability and progress.
Assess patient perceived fear of falling. Explain need for
positive gains to empower patient with self-confidence. Detrimental affect of worry for deconditioning rather than progress.
Nurse/ rehab therapist/case manager: “I know you were hoping to go
home, but it would not be safe for you to return home without getting stronger first. Can you tell me what you hope to accomplish with more strengthening exercises? “
Lack of caregiver ability or assistance
Safety measures
Post op fall risk: Timed Up& Go (TUG); decreased balance or poor gait or pre-existing dementia, confusion/delirium on admission
Multiple chronic conditions needing monitoring and maintenance eg. Dialysis or CHF pts.
Pain control
Poor muscle strength Malnutrition Prefracture poor functional baseline Patient can perform therapy 2-3 hours daily Nondisplaced or minimally displaced fractures
with need for weight bearing but unsafe at home Complications s/p hip surgery Elderly unstable patient with comorbidities &
not a surgical candidate. Hospice candidate
Restore function and balance. Cognizant individuals may limit activity at home if aware of balance deficit to avoid fall.
Rehabilitate to highest level of function: maintain training level so gain is not lost over time.
Pain control
Improve circulation and pulmonary status; preserve skin integrity.
Reduce fatigue/ conserve energy.
Best predictors of success: Balance and cognitive status at 3months following discharge from facility.
Best predictors for return to functional ability following discharge from rehab: balance, cognition, and prior functional ability.
[Folden & Tappan, 2007].
To support optimal functional recovery at NH:
Care includes prevention of (1) dehydration & electrolyte imbalance ;(2) thromboembolism; (3) pneumonia; (4) decubitus ulcers; (5) elimination dysfunction;(6) confusion and depression.
Chronic disease management and assessment: timely calls for
Clinical interventions for relief of symptom distress, minimize suffering, improve QOL.
Follow up care and reevaluation long term so that gains are not lost overtime contributing to second falls or refracture.
Appropriate level of care assessment following convalescence.
Education
88 y.o. Caucasian female : independent at home with minimal assist from family; no adaptive device. Fell while serving coffee to “younger senior citizens” at the local center. Active with her family and church parish “Sharp as a tack”.
Risks for fractures: advanced age, osteoporosis, several chronic conditions including OSA, COPD, severe pulmonary HTN; moderate degenerative spondylosis for postural changes
Dx subtrochanteric Rt hip fracture: open reduction internal fixation : pain 10/10 Rt hip, groin, abdomen.
Post op ICU care for hypotension : dopamine, dobutamine, Fluids, PRBC, BIPAP support. Treatment of Rt heart failure. Pain control.
LOS 7 days and discharged to swing bed facility then transferred to assisted living facility. Walker and ADLS assistance.
Nurse: How are things going?
Patient: “Not very well. I am feeling like I will never go home.”
Nurse: You seem really discouraged. Can you tell me what happened this morning that has made you feel this way?
Patient: “ The doctor told me some really bad news.”
Nurse: What is your understanding of what happened?
NURSE acronym: Name the emotion; U understanding; R respect; S support; E explore. = TRUST.
Be cured
Live longer
Improve or maintain function/quality of life/ independence
Be comfortable (pain control): relieve symptoms of distress.
Achieve life goals
Provide for family/ caregiver
Typically, must assist patient/ family to modify goals as life draws to end (realistic expectations) with care option talks. [Peereboom &Coyle, 2012].
Patients who have conversations about their wishes for end of life care are more likely to receive care consistent with their preferences.
Goals first in line with beliefs/ values then care options.
Current condition/ disease information /prognosis for informed medical decision-making
Shared decision- making- partnership
Active, therapeutic listening; ask open ended questions
Empathy/ TRUST: both patient and family as a unit
Hope for the Best, prepare for the Worst - Allow patients/ families to face frightening outcomes-
helps with denial. Team approach diffuses anger and says “ We care about YOU”.
Anger is grief (loss) or some other underlying emotion (frustration or fear).
Allow for verbalization of fears and important priorities. Provide hope. Hope can be considered for effective pain
control, time to prepare for EOL goals, family/spiritual time.
80% of communication is non- verbal: relaxed posture, good eye contact, lean into patient or family and eye level; nod head.
Be honest. Cultural differences: age, gender, ethnicity, past
experience, social or economic status, or mistrust of health care system
Family dynamic issues or spiritual considerations-
multidisciplinary support/intervention.
SPIKE: Set up interview (family conference); Patient Perception; Patient Invitation; Knowledge; Emotions/Empathy.
[Baile et.al., 2000]. Multidisciplinary team as needed or desired.
SUMMARY: Art of Communication by Team : meet
patient and family where they are with care and empathy. Guide gently. Provide information. Encourage questions and concerns. Pt/family may need time to consider, talk over, and come to conclusions. Important that providers are in unison about care options presented to avoid confusion.
87 y.o. African-American female and nursing home resident
Hx of multiple CVA/ Rt hemiparesis/ dysphagia with aspiration risks/cachexia, preexisting Lt femur fx with nailing 9/28/2013, bilateral heel ulcers secondary to immobility/WC and severe peripheral arterial disease, A-fib, 95% Lt carotid artery stenosis (not a surgical candidate), chronic depression & pain/ Wt.loss., risk for bleeding and I&D of ulcers not an option, dehydration/prerenal failure = FRAIL ELDER.
Intermittent confusion with acute illness. Recent rehospitalizations x4 ( monthly). Lt femur fx from fall- intramedullary nailing :
Hardware shifted and elected no repair for chronic pain. Narcotics.
Full code. Pt raised grandson who is POA. No artificial feedings desired.
Conference held with pt/ POA for goals of care/education. Pt confusion. Grief support. Revealed poor QOL with sadness prior to hospitalization. Priority: pain control and spiritual/ family life.
Decision made by POA for pt. to go back to nursing home on hospice care. DNR/DNI.
1. Baile, WF, Buchman, R., Lenzi, R. et. al. SPIKES: a six-step protocol for delivering bad news. The Oncologist. 2000. (5) 4: 302-311.
2. Bentler, S., Liu, L, Obrizan, M. et. al. The aftermath of hip fracture: discharge placement, functional status change, and mortality. Am. Jnl of Epidemiol. 2009. 170: 1290-99.
3. Farahmand, B.,Michaelsson, K., Ahlbom, A., Junghall,S., Baron, J. Survival after hip fracture. Osteoporosis Int. 2005.16:1583-1590.
4. Fierens, J. & Broos, P. Quality of life after hip fracture surgery in the elderly. Acta Chir.Belg. 2006. 106: 393-396.
5. Folden, S. & Tappan, R. Factors influencing function and recovery following hip repair surgery. Orthopedic Nursing. July/Aug. 2007. (26) 4: 234-241.
6. Gambatesa,M., D’Ambrosio, A., D’Antonio,D. et.al., Counseling, quality of life, and acute postoperative pain in elderly patients with hip fracture. Journal of Multidisciplinary Healthcare. 2013. (6): 335-346.
7. Gantz, S., Peterson, M, Russon, P, Guccione, A. Functional recovery after hip fracture in subacute setting. HSSJ. 2007. 3: 50-57.
8. Giessauf, C., Glehr, M., Bernhardt, G. et. al. Quality of life after pertrochanteric femoral fractures treated with a gamma nail: a single center study of 62 patients. BMC. Musculoskeletal Disorders. 2012. (13): 214-220.
9. Jongjit, J., Komsopapong, L., Songjakkaew, P., Kongsakon, R. Health- related quality of life after hip fracture in the elderly community –dwelling. Southeast Asian J Trop Med Public Health. 2003. (34) 3: 670-674.
10 Kristensen, M., Foss, N, Henrik, K. Timed “ Up & GO” Test as a predictor of falls within 6 months after hip fracture surgery. Physical Therapy. 2007. 87: 24-30.
11. Liebson, C., Toteson, A., Gabriel, S., Ransom, J., Melton,J. Mortality, disability, and nursing home use for persons with and without hip fracture: a population- based study. Jnl of the American Geriatrics Society. 2002. 50: 1644-50.
12. Marks, K., Allegrante, J., MacKenzie, C, Lane, J. Hip fractures among the elderly: causes, consequences, and control. Aging Research Review. 2003. 2: 57-93.
13.Mendonca, T., da Silva, C. Canto, R. et.al. Evaluation of the health related quality of life in elderly patients according to the type of hip fracture: femoral neck and trochanteric. Clinician. 2008. 63 (5): 607- 12.
14. National Hospital Discharge 2011. National Center for Health Statistics available at www. cdc.gov/nchs/nhds.html
15.Peereboom, K. & Coyl, N. Facilitating goals-of-care discussions for patients with life-limiting diseases- communication strategies for nurses. Journal of Hospice and Palliative Nursing. June 2012. (14) 4: 251-258.
16.Shumway- Cook, A., Ciol, M, Gruber, W, Robinson, C. Incidence of at risk factors for falls following hip fracture in community- dwelling older adults. Physical Therapy. 2005. 85: 648-655.
17.VanBalen, R. Essink- Bot, M. Steyerberg, E. Cools, H., Habbema, D. Quality of life after hip fractures: a comparison of 4 health status measures in 208 patients. Disability and Rehabilitation. 2003. 25. (10): 507-19.
Reference: www.rand.org/health/surveys_tools/mos_core_36 item.html or www.sf-36.org/demos/SF-36.html
Self-reported patient well-being assessment of 8 domains: General health Vitality Bodily pain Physical Functioning Role Limitation, physical Role Limitation, emotional Social functioning Mental health Tool is valid, reliable, sensitive for hip fractures, reproducible, easy Nottingham Health Profile: www.primarycare.core.org/PDF 38 items/ 6 domains emotion, social isolation, physical mobility, pain, energy, and
sleep. Yes or no answers; likert scale ; reliable, valid, sensitive, easy. TUG www.unmc.edu/media/intmed/geriatrics/nebgec/pdf/frailelderly/ july09/toolkits