Embed Size (px)
Citation preview

achri.archildrens.org uams.edu arpediatrics.org
Chronic Lung Disease in the Patient with Neurodisability: Concepts and
Management Strategies
Robert H. Warren, M.D. Adjunct Professor, Department of Pediatrics,
UAMS @ ACH Farrah Jones, BS, RRT
Research Respiratory Therapist Arkansas Children’s Hospital Research Institute
achri.archildrens.org uams.edu arpediatrics.org
Disclosure Information AACPDM 69th Annual Meeting | October 21-24, 2015
Speaker Name: Robert H. Warren, M.D.
Disclosure of Relevant Financial Relationships
I have no financial relationships to disclose.
Disclosure of Off-Label and/or investigative uses:
I will not discuss off label use and/or investigational use in my presentation
achri.archildrens.org uams.edu arpediatrics.org
Presentation Objectives
Understand the pathophysiology of airway secretions in the patient with neurodisability and potential for progressive pulmonary dysfunction
Understand the potential clinical application of the Pulmonary Composite
Understand the basic principles of respiratory care medications and devices.
See, through the use of case presentations, the need for individualization of the respiratory therapy management plan
Admission Criteria for the ACRTDC
Child followed by Pulmonary Section
Diagnosis of any type of neuromuscular disease, chronic lung disease and/or syndromes or conditions causing chronic respiratory insufficiency
Requires ventilator support and/or tracheostomy and/or airway clearance device
MISSION STATEMENT
The Arkansas Center for Respiratory
Technology Dependent Children
(ACRTDC) is committed to providing
specialized care to respiratory
technology dependent children and
enhancing quality of life through
caregiver education, research and
advocacy.
CONGENITAL NEUROLOGICAL DIAGNOSES
Becker Muscular Dystrophy Cerebellar Atrophy Cervicothoracic
Syringomyelia/syrinx CHARGE Syndrome Congenital Muscular Dystrophy Congenital Hypomyelination
Syndrome CFC Syndrome Down Syndrome Duchenne Muscular Dystrophy Fredericks Ataxia Jarcho-Levin Syndrome Neuronal Migration Disorder FSH Muscular Dystrophy Cockayne Syndrome Thoracic Dystrophy
Merosin Deficient Muscular Dystrophy Myotonic Dystrophy Neiman Pick Partial Complex IV Mitochondrial
Disease Pompe Disease Soto Syndrome Spina Bifida Spinal Muscular Atrophy Types I & II Undiagnosed Mitochondrial Disorder Undiagnosed Neurodegenerative
Disorder X-linked Myotubular Myopathy Bethlehem Myopathy Marshall Syndrome Metachromatic Leukodystrophy Congenital Scoliosis
achri.archildrens.org uams.edu arpediatrics.org
Acquired Neurological Diagnoses
NICU
Traumatic Brain Injury Non-accidental
Traumatic Brain Injury/ Spinal Cord Injury Accidental secondary to non-primary pulmonary condition

achri.archildrens.org uams.edu arpediatrics.org
Sources of Excessive Airway Secretions
Ineffective cough
Airway hyposensitivity
Aspiration
Dysphagia
GER
Airway inflammation
Infection
Mucosal gland proliferation and hypertrophy
achri.archildrens.org uams.edu arpediatrics.org
Decrease in airway sensitivity – Change in irritant fiber response
Airway Inflammation
Mucosal gland proliferation and hypertrophy
Infection leading to airway and parenchymal damage
Airway Responses
achri.archildrens.org uams.edu arpediatrics.org
ORIGINATION OF AIRWAY SECRETIONS
INTRODUCED into the airway
PRODUCED in excess in the airway
RETAINED in the airway

achri.archildrens.org uams.edu arpediatrics.org
Pulmonary Composite Of Child With Neurodisability
State of ambulation
Seizure Disorder
Dysphagia with secondary aspiration
GER with secondary aspiration
Hypopneic Breathing Pattern
Spasticity
Hypotonia/Ineffective Cough
Recurrent acute respiratory illness
Drooling – Excessive oral secretions
achri.archildrens.org uams.edu arpediatrics.org
THE PULMONARY COMPOSITE
Ambulation Retained/Produced
Seizure Disorder Introduced
Dysphagia Introduced
GER Introduced
achri.archildrens.org uams.edu arpediatrics.org
The Pulmonary Composite
Hypopnea Retained/Produced
Spasticity Introduced
Hypotonia Retained/Produced
Recurrent Illness Produced
Excessive oral secretions Introduced
achri.archildrens.org uams.edu arpediatrics.org
Clinical Application of the Pulmonary Composite
Development of a SEVERITY SCORE
Assign “severity score” to each component of the pulmonary composite
Determine ability to decrease the “severity score” for each component
achri.archildrens.org uams.edu arpediatrics.org
Evolution Of Chronic Lung Disease In Children With Neurodisability
Impaired cough and retained secretions
Aspirated secretions from dysphagia and GER
Respiratory infection / atelectasis
Bronchiectasis / pulmonary dysfunction
Diminished oxygenation
Alveolar hypoventilation and CO2 retention
achri.archildrens.org uams.edu arpediatrics.org
“Working up” the patient: Clinical Assessment
History – Using the Pulmonary Composite as a Guide Physical Assessment: Visual observation, listen, auscultation Laboratory Date: Resting Tidal Volume End Tidal CO2 Pulse Oximetry Blood Gas Analysis: ABG – VBG – CBG Transcutaneous O2 and CO2 determination Radiology: Chest imaging Sinus imaging

achri.archildrens.org uams.edu arpediatrics.org
Airway Bacterial Colonization in the Neurodisability Patient
Retrospective study
Total of 93 subjects studied
Charactersitic N (%) unless otherwise noted
Age at time of trach, mean (SD),years 3.0 (4.3)
Length of time with trach, mean (SD) years
6.2 (4.7)
Sex
Male 53 (57.0)
Female 40 (43.0)
Race/Ethnicity
White 58 (62.4)
African American 26 (28.0)
Hispanic 9 (9.7)
Table 1: Demographics of study population, N=93
Table 2: Underlying diagnosis that led to tracheostomy, N=93
Diagnosis Prevalence N (%)
Cerebral Palsy 24 (25.8)
Spina Bifida 5 (5.4)
Moebius Syndrome 3 (3.2)
Laryngomalacia 3 (3.2)
Head Injury 3 (3.2)
Diaphragm Paralysis 2 (2.2)
Mandibular Agenesis 2 (2.2)
Muscular Dystrophy 2 (2.2)

Organism Prevalence N (%)
Pseudomonas aeruginosa 84 (90.3)
Stenotrophomonas maltophilia 72 (77.4)
Serratia marcescens 62 (66.7)
Moraxella catarrhalis 57 (61.3)
MRSA 52 (55.9)
MSSA 43 (46.2)
Haemophilus influenza 41 (44.1)
Group B streptococcus 32 (34.4)
Streptococcus pneumoniae 26 (28.0)
Acinetobacter baumanii 24 (25.8)
Acinetobacter calcoacetuis 13 (14.0)
Serratia liquifacins 9 (9.7)
Haemophilus parainfluenzaw 7 (7.5)
Table 3: Prevalence of pathogens isolated from respiratory cultures of all subjects at any time since trach placement, N=93
Organism N (%) Mean time to isolation, Month (SD)
Mean time to isolation, Range
MSSA 22 5.2 (10.3) 0.2 – 41.7
MRSA 19 6.5 (7.5) 0.2 – 26.4
Pseudomonas aeruginosa
37 7.8 (7.2) 0.2 – 25.1
Stenotrophomonas maltophilia
34 11.0 (10.6) 0.2 – 43.9
Serratia marcescens 22 13.3 (11.7) 0.1 – 38.4
Moraxella catarrhalis
24 16.3 (14.7) 0.1 – 44.3
Haemophilus influenzae
17 16.4 (16.1) 0.1 – 44.4
Table 4: Mean time to isolation after trach for selected organisms, N=45 subjects with respiratory culture after 2006
Figure 1: Organism Prevalence in 2010 based on length of time with tracheostomy (N=90)
Years with tracheostomy
0-1 2-4 5-7 8+
Pe
rce
nt
of
Pa
tie
nts
with
org
an
ism
on
re
sp
ira
tory
cu
ltu
re in
20
10
0
20
40
60
80
100PA
MSSA
MRSA
Serr
Steno
achri.archildrens.org uams.edu arpediatrics.org
Identifying the Presence of a Specific Chronic Lung Disease of Neurodisability
IRB study 203740
Study: Cohort of patients with primary neurodisability diagnosis with NO pulmonary disease at the time of initial diagnosis
Hypothesis: Factors in the Pulmonary Composite produce chronic airway secretion overload with resultant progressive chronic lung disease over time.
Study Group: 136 patients age range x to x and with multiple congenital and acquired neurodisability diagnoses
achri.archildrens.org uams.edu arpediatrics.org
Identifying the Presence of a Specific Chronic Lung Disease of Neurodisability
IRB study 203740
Methodology:
Identify factors at time of initial presentation
to the pulmonary clinic
Follow factor persistence and accumulation
over time.
End points: Progression to pulmonary
insufficiency and mechanical ventilation or
end of study period whichever comes first
achri.archildrens.org uams.edu arpediatrics.org
Identifying the Presence of a Specific Chronic Lung Disease of Neurodisability
IRB study 203740
• Clinical Questions:
Role of pulmonary factors individually and
collectively
Individual contribution in order of
prominence

achri.archildrens.org uams.edu arpediatrics.org
Blucker, R., Elliott, T.R., Warren, R.H., Warren, A.M. (2011). Psychological adjustment of family caregivers of children who have severe neurodisabilites that require chronic respiratory management. Family, Systems & Health, September 2011, Vol 29, No. 3, p.215
achri.archildrens.org uams.edu arpediatrics.org
Trait Resilience and Distress Among Family Caregivers of Children with Severe Disabilities Receiving Pulmonary Services
Courtney Francis1, Ryan T. Blucker1, Robert Warren2, Ann Marie Warren3, Timothy R. Elliott1, and Jack W. Berry4
1Texas A&M University, Department of Educational Psychology, 2Arkansas Children’s Hospital, 3Baylor Institute for Rehabilitation, 4Samford University
Method
Introduction Results
This study is a cross-sectional study of 60 caregivers of children with severe
disabilities who were being followed for chronic pulmonary management.
Caregivers provided informed consent and completed the Big 5 Questionnaire
(BFQ). Participants were family caregivers of children with severe disabilities
who are seen in the Arkansas Center for Respiratory Technology Dependent
Children (ACRTDC) outpatient clinic. The caregivers of these children, and the
focus of this study, are typically parents (either coupled or single), grandparents,
older siblings, or an extended family member. Participants were self- identified
as a primary caregiver of a patient followed in the ACRTDC program. Measures
given include the PHQ (to assess depression and anxiety), the SF-12 (to assess
physical and mental health), and a measure of social problem solving abilities.
First hierarchical clustering with Ward's to get the personality clusters, then we
used a k-means clustering using the results of Ward's method as a starting point.
Differences between the personality prototypes on the adjustment variables were
then examined.
*all p’s < .05
The purpose of this study was to examine personality prototypes among family
caregivers of children with severe disabilities, and the relation of trait resilience
to their distress. Research indicates that as with many caregiver roles, burnout
and psychological distress are commonplace. Furthermore, the literature
suggests that the Big Five personality factors (John & Srivastava, 1999), can be
reliable predictors of functioning in important domains of life such as
psychological adjustment and coping (McCrae, 1991; McCrae & Costa, 1986),
overall happiness and satisfaction with life (Costa & McCrae, 1980; Myers &
Diener, 1995), and general physical health and wellness behaviors (Booth-
Kewley & Vickers, 1994). More recently, the Big Five personality can be used
to determine personality prototypes, including trait resilience, that may be
associated with adjustment and coping in times of stress (Berry, Elliott &
Rivera, 2007). Trait resilience has yet to examined among family caregivers,
generally, and specifically among caregivers of children with severe
neurodisabilities who require chronic pulmonary management.
A series of one-way ANOVAs revealed that the resilient caregivers
reported significantly lower levels of anxiety (p=.035) and greater
mental health (p=.001) than caregivers characterized as
uncontrolled or overcontrolled (See Table 1).
Overcontrolled caregivers reported significantly greater tendencies
to avoid problems, and a more negative problem-solving orientation
than other caregivers. Resilient caregivers reported more rational
problem-solving abilities and a more positive orientation than
others. These findings are consistent with the Berry et al study of
personality prototypes. As the literature suggests the characteristics
found in resilient prototypes do not uniquely predispose an
individual to better health and adjustment nor do the characteristics
found in overcontrolled and undercontrolled types predispose one to
distress.
Cluster analysis of BFQ yielded 3 cluster prototypes: 22
caregivers were characterized as resilient, 17 were
uncontrolled types, and 17 were overcontrolled types.
As referenced in Figure1, the resilient caregiver group is
a perfect reflection of what is typically found in trait
resilience: high extraversion, low neuroticism, and
above average on openness, conscientiousness, and
agreeableness. The undercontrolled group is high on
extraversion, but also high in neuroticism, and below
average in agreeableness and conscientiousness. The
overcontrolled group is low on extraversion and high
neuroticism (the signature feature of this type).
Discussion Family caregivers who have resilient personality styles may be less likely to have anxiety issues. Caregivers who are more overcontrolled may be particularly predisposed to distress and lack effective problem-
solving skills. Although the study is limited by its cross-sectional nature and its reliance on self-report measures, the results indicate that trait resilience may be identified among family caregivers, and caregivers
have characteristics associated with an overcontrolled personality style may be prone to distress and adjustment problems. This information may be useful in developing strategic programs for caregivers who may be
at risk for distress.
Figure 1. Table 1.
achri.archildrens.org uams.edu arpediatrics.org
Discussion
Results indicate that resilient characteristics may derive from common and normative
personality traits. Resilient caregivers defined in this manner appear to have
significantly lower levels of depression and anxiety than other caregivers. Resilient
caregivers are also more likely to endorse resilient tendencies than caregivers who
tend to have overcontrolled personality styles. Resilient caregivers are also more
likely than overcontrolled caregivers to have supportive social relationships that help
them cope and that maintain their self esteem. However, resilient caregivers may not
differ from other caregivers in other coping behaviors, indicating that their ongoing
and enduring personality style may have a greater influence on their ability to adjust
than any single coping activity.
Conclusions
Although the study is limited by its cross-sectional nature and its
reliance on self-report measures, the results indicate that trait resilience
may be identified among family caregivers, and caregivers have
characteristics associated with an overcontrolled personality style may
be prone to distress and adjustment problems. This information may be
useful in identifying family caregivers at risk for distress and for
developing strategic programs for them.
Results
We conducted a cluster analysis of the Big Five personality measure to classify caregivers as a resilient
prototype (N = 22), an overcontrolled prototype (N = 22) or as an undercontrolled prototype (N = 19), based on an a
priori model of trait resilience. As depicted below, resilient caregivers were characterized by higher z-score
averages on Agreeableness and Conscientiousness, and low z-score averages on Neuroticism. Undercontrolled
caregivers had the highest z-score averages on Extraversion. Overcontrolled caregivers had the highest average
z-scores on Neuroticism.
A series of comparisons revealed that the Resilient caregivers differed from the other prototypes on several
variables.
Resilient caregivers were significantly less
Depressed on the PHQ2 screen (M = .05, SD = .22)
than overcontrolled caregivers (M = 1.48, SD = 2.20). Resilient caregivers also had a significantly
lower score on the PHQ item to screen for anxiety
than undercontrolled caregivers (M = .38, SD = .59;
M = 1.00, SD = .87; respectively). Resilient
caregivers had a significantly higher score on the
Conner-Davidson measure of resilience (M = 88.16,
SD = 7.23) than Overcontrolled caregivers (M =
75.02, SD = .13.79).Resilient caregivers were significantly more likely to cope by maintaining
social support, self esteem and psychological
stability (as measured by the CHIPS; M = 32.14,
SD = 7.73) than overcontrolled caregivers (M =
25.14, SD = 8.12). No other differences were found
between the caregiver personality prototypes on the other coping measures.
SP15 RESILIENCE AMONG FAMILY CAREGIVERS OF CHILDREN WITH SEVERE NEURODISABILITIES REQUIRING CHRONIC RESPIRATORY MANAGEMENT
Timothy R. Elliott1, Robert H. Warren2, Ryan Blucker3, Jack W. Berry4, Jessica Chang1, Ann Marie Warren5
1Educational Psychology, Texas A&M University, College Station, TX; 2Pediatrics, University of Arkansas for Medical Sciences, Little Rock, Arkansas, AR; 3Pediatrics, University of Oklahoma Health Sciences Center, Oklahoma City, OK; 4Psychology, Samford University, Homewood, AL; 5Trauma, Baylor University
Medical Center, Dallas, TX
Objectives
The study was conducted to identify the characteristics of
resilient caregivers of children with severe neurodisabilities who
require chronic respiratory management. Differences in the
psychological adjustment and coping styles of caregivers
classified as resilient, overcontrolled and undercontrolled were
also examined.
Methods
Design: Cross-sectional, correlational study.
Participants and Setting: 68 family caregivers of children
receiving care at the Arkansas Center for Respiratory
Technology Dependent Children outpatient clinic. All children had chronic pulmonary symptoms that required daily respiratory
plans and all had either acquired or congenital neurodisabilities.
Sixty-eight caregivers consented to participate in the study. All
but one were women, and the sample ranged in age from 24 to
60. Over 75% of the participants were Caucasian; the rest were
African-American.
Material and Methods: Consenting caregivers were given a packet containing the study questionnaires and these were
returned to clinic staff. Study instruments including a
personality measure of the Big Five Inventory of personality
traits; the Connor-Davidson measure of resilience; the two-item
depression screen on the Patient Health Questionnaire; and two
measures of coping: the Family Crisis Oriented Personal
Evaluation Scales (FACES) and the Coping Health Inventory for Parents (CHIPS).
Contact information: Timothy R. Elliott, PhD.,[email protected] Robert Warren, MD, [email protected]

achri.archildrens.org uams.edu arpediatrics.org
Disclosure Information AACPDM 69th Annual Meeting | October 21-24, 2015
Speaker Name: Farrah Jones, BS, RRT
Disclosure of Relevant Financial Relationships
I have no financial relationships to disclose.
Disclosure of Off-Label and/or investigative uses:
I will not discuss off label use and/or investigational use in my presentation
achri.archildrens.org uams.edu arpediatrics.org
The Individual Respiratory Care Plan
Step 1: Patient Assessment
Step 2: Medication/Device selection
Step 3: Determine Frequency of Therapy
Step 4: Ongoing Evaluation
achri.archildrens.org uams.edu arpediatrics.org
Creating The Respiratory Care Plan: Individualization Is The Key
1. Selection of aerosol medications: Bronchodilators, decongestants, anti-inflammatories, mucolytics, antibiotics
2. Delivery systems: MDI & spacer or updraft nebulizer possibly including use of hyperinflation delivery
3. Assessment for airway clearance devices: In-exsufflator, high frequency oscillation, intrapulmonary percussionator
4. Ventilator support
achri.archildrens.org uams.edu arpediatrics.org
Bronchodilators
Albuterol (Proventil, Ventolin, Proair) Dosage: MDI – 2 puffs QID Nebulizer – 0.03 mL / kg QID Levalbuterol (Xopenex) Dosage: MDI – 2-4 puffs Q 6 hours
Nebulizer - 0.63 mg every 6 hours Ipratropium Bromide (Atrovent) Dosage: MDI - 2 to 4 puffs QID Nebulizer – 250 to 500 mcg QID
achri.archildrens.org uams.edu arpediatrics.org
Anti-inflammatory
Fluticasone Propionate (Flovent)
Dosage: 88mcg to 880mcg BID
Budesonide (Pulmicort Respules)
Dosage: 0.25mg to 0.5mg BID nebulized
Beclamethasone Dipropionate (Qvar)
Dosage: 80mcg to 160mcg BID
achri.archildrens.org uams.edu arpediatrics.org
Mucolytics
Acetylcysteine (Mucomyst) Dosage: 2 mL of 10% or 20% in 3mL of saline. Always give bronchodilator concurrently Dornase alfa (Pulmozyme) Dosage: 2.5 mg/unit dose Sodium Bicarbonate (Na HCO3 8.4%) Dosage: 1 mL in 3 mL normal saline given up to 4 times a day

achri.archildrens.org uams.edu arpediatrics.org
Antibiotics
Tobramycin Inhalation (Tobi) Trade name: TOBI Dosage: 300 mg nebulized BID Tobramycin for injection Dosage: 80 mg nebulized BID (albuterol given prior) Ceftazadime (Fortaz) Dosage: 1 or 2 grams nebulized BID
achri.archildrens.org uams.edu arpediatrics.org
Special Considerations
Delivery Devices
Order of medications
Financial/insurance
achri.archildrens.org uams.edu arpediatrics.org
Delivery Devices

achri.archildrens.org uams.edu arpediatrics.org
Order of Medications
• Bronchodilators
• Mucolytics
• Anti-inflammatories
• Antibiotics
achri.archildrens.org uams.edu arpediatrics.org
Mucus Mobilization Airway Secretion
Clearance
Manual physical therapy techniques
Mechanical devices - Vibrators - HFCWO - IPV - M/I-E
achri.archildrens.org uams.edu arpediatrics.org
achri.archildrens.org uams.edu arpediatrics.org
Special considerations
Order of therapies
Tracheostomy considerations
Financial / insurance barriers
Caregiver limitations
Patient tolerance
Ability to clear secretions after secretion mobilization techniques
achri.archildrens.org uams.edu arpediatrics.org
Skills Validation Quality Improvement Project
Presently ongoing in caregivers of children with a primary neurodisability who have secondary acute and chronic pulmonary symptoms
achri.archildrens.org uams.edu arpediatrics.org
Skills Validation Quality Improvement Project
Notification of the caregiver prior to clinic visit
The caregiver must bring their own equipment
Perform skills validation at the end of the clinic visit
Remedial education will be provided if needed
Certificate of completion
Pre and post surveys for caregiver feedback
achri.archildrens.org uams.edu arpediatrics.org
Skills Validation Quality Improvement Project Preliminary Results
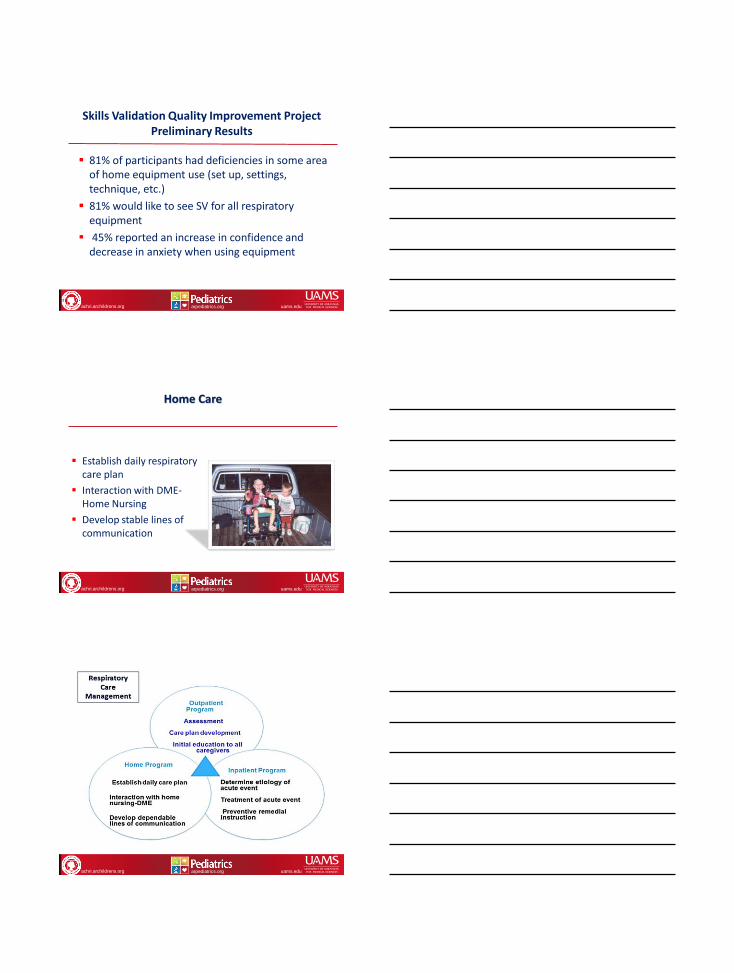
81% of participants had deficiencies in some area of home equipment use (set up, settings, technique, etc.)
81% would like to see SV for all respiratory equipment
45% reported an increase in confidence and decrease in anxiety when using equipment
achri.archildrens.org uams.edu arpediatrics.org
Home Care
Establish daily respiratory care plan
Interaction with DME-Home Nursing
Develop stable lines of communication
achri.archildrens.org uams.edu arpediatrics.org

achri.archildrens.org uams.edu arpediatrics.org
Goals for the Child with Neurodisability
Provide clinical stability
Prevent acute exacerbations of illness
Reduce or halt the progression of pulmonary disease
Reduce/prevent emergency room visits
Reduce/prevent hospitalizations for acute pulmonary illness
Allow the patient to be integrated into the family unit
achri.archildrens.org uams.edu arpediatrics.org
Case Study: 9 month old Caucasian male Diagnosis: Neurodisability secondary to Kernicterus
Pulmonary Composite Factors: Seizures, Dysphagia, Drooling, GER, Infective cough, extreme spasticity
Pulmonary Symptoms: cough, airway secretion accumulation (audible airway noise)
Challenges to the Respiratory Care Management Plan: resistance to all devices to deliver medications and airway clearance devices
achri.archildrens.org uams.edu arpediatrics.org
What is your plan for this patient?
Medications?
Devices?
Frequency?
achri.archildrens.org uams.edu arpediatrics.org
Case study: AF 17 year old Caucasian female Diagnosis: Merosin Deficient Muscular Dystrophy
• Pulmonary Composite Factors: GER, dysphagia, non-ambulatory, hypopneic breathing pattern
• Symptoms: chronic hypoventilation, but no other respiratory symptoms
• Challenges to respiratory care management plan: significant (100 degree) scoliosis with lung restriction, continuous NG tube, no tracheostomy
achri.archildrens.org uams.edu arpediatrics.org
What is your plan for this patient?
Medications?
Devices?
Frequency?
Ventilation?
achri.archildrens.org uams.edu arpediatrics.org
Case study: 19 year old Caucasian female Diagnosis: Lissencephaly
• Pulmonary Composite Factors: non-ambulatory, GER, dysphagia, seizures, hypotonia, hypopneic breathing pattern
• Pulmonary Symptoms: chronic hypoventilation, copious amount of thick secretions, colonization with pseudomonas aeruginosa, occasional wheeze
• Challenges to Respiratory Care Management Plan: copious amount of secretions, insurance/financial barriers, large patient size, chronic bacteria colonization

achri.archildrens.org uams.edu arpediatrics.org
What is your plan for this patient?
Medications?
Devices?
Frequency?
Ventilation?
achri.archildrens.org uams.edu arpediatrics.org
Case Study: 16 year old Caucasian male Diagnosis: Ulrich’s Muscular Dystrophy
Pulmonary Composite Factors: non-ambulatory, hypotonia, hypopneic breathing pattern
Pulmonary Symptoms: the need to create an aggressive pre-op respiratory care plan for spinal surgery to improve VC
Challenges to the Respiratory Management Plan: Currently on non-invasive ventilation for 8 hrs/night, albuterol MDI followed by cough assist BID
achri.archildrens.org uams.edu arpediatrics.org
What is your plan for this patient?
Medications?
Devices?
Frequency?
Ventilation?