Embed Size (px)
Citation preview
[4]. Sam et al . [5] described three generations of a single
family that presented autosomal dominant CMC without
endocrinopathy. In fact, CMC could be considered a syn-
drome that presents different clinical forms, probably
involving different genetic defects. A cellular immune
defect has been suggested as the central factor of CMC.
The disturbance could be located in effector cells (mac-
rophages, natural killer or cytotoxic lymphocytes) or at the
regulatory level, involving T cell cytokines or possibly
antigen presenting cells (APCs), as these are infl uenced by
regulatory cytokines [6 – 8]. The underlying defect is poorly
understood and further studies are required to elucidate the
pathophysiology of CMC.
Case report
NRSP, a 39-year-old Caucasian woman born in 1971
to non-consanguineous parents, was two years old when
she fi rst presented with recurrent severe oral candidiasis
that led to a growth defi cit. When she was three years
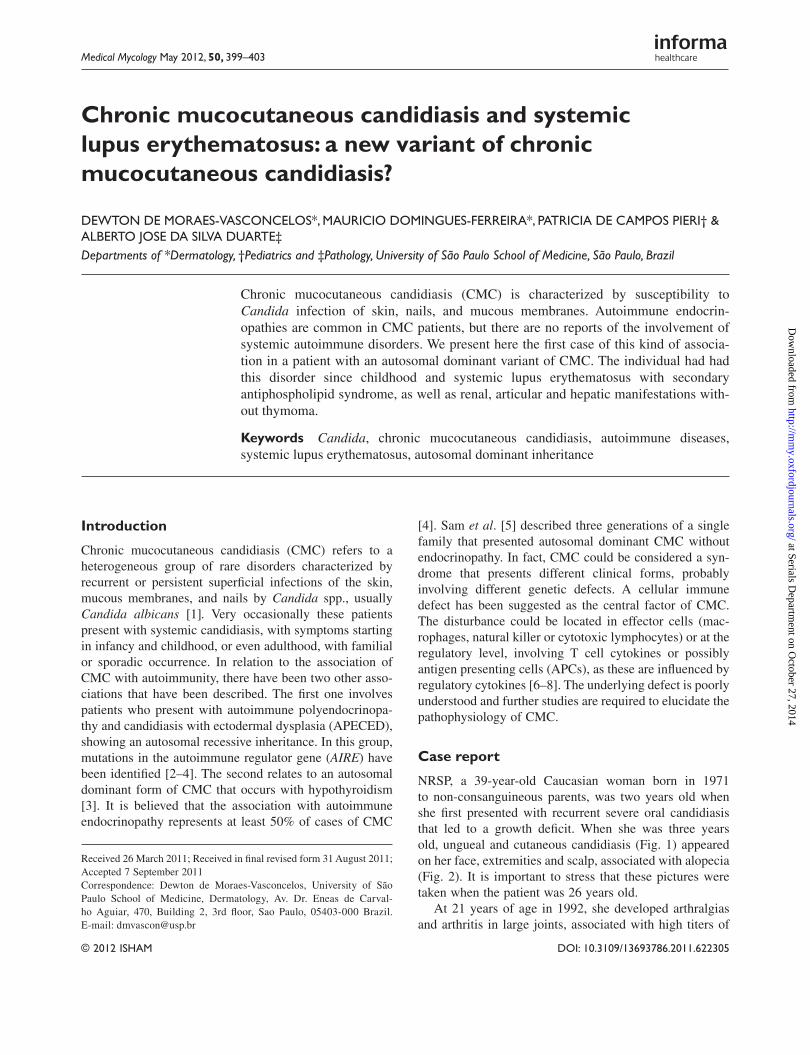
old, ungueal and cutaneous candidiasis (Fig. 1) appeared
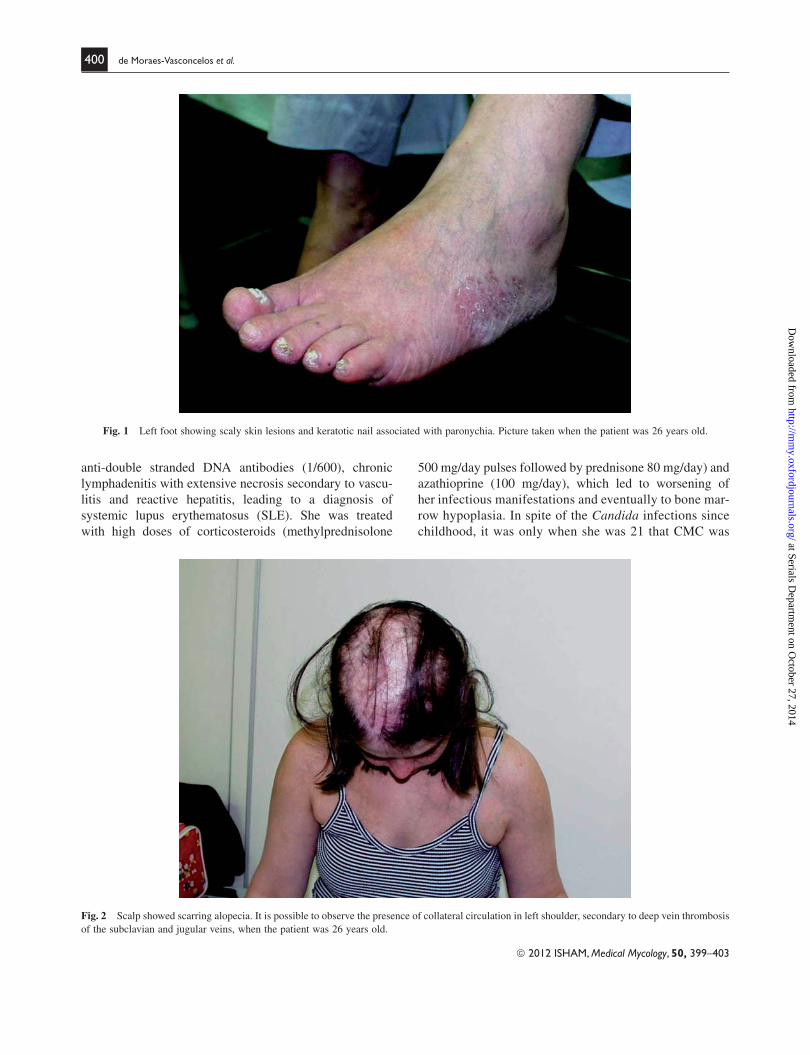
on her face, extremities and scalp, associated with alopecia
(Fig. 2). It is important to stress that these pictures were
taken when the patient was 26 years old.
At 21 years of age in 1992, she developed arthralgias
and arthritis in large joints, associated with high titers of
Received 26 March 2011 ; Received in fi nal revised form 31 August 2011;
Accepted 7 September 2011
Correspondence: Dewton de Moraes-Vasconcelos, University of S ã o
Paulo School of Medicine, Dermatology, Av. Dr. Eneas de Carval-
ho Aguiar, 470, Building 2, 3rd fl oor, Sao Paulo, 05403-000 Brazil.
E-mail: [email protected]
Chronic mucocutaneous candidiasis and systemic
lupus erythematosus: a new variant of chronic
mucocutaneous candidiasis?
DEWTON DE MORAES-VASCONCELOS * , MAURICIO DOMINGUES-FERREIRA * , PATRICIA DE CAMPOS PIERI † &
ALBERTO JOSE DA SILVA DUARTE ‡
Departments of * Dermatology , † Pediatrics and ‡ Pathology , University of S ã o Paulo School of Medicine , S ã o Paulo , Brazil
Chronic mucocutaneous candidiasis (CMC) is characterized by susceptibility to Candida infection of skin, nails, and mucous membranes. Autoimmune endocrin-opathies are common in CMC patients, but there are no reports of the involvement of systemic autoimmune disorders. We present here the fi rst case of this kind of associa-tion in a patient with an autosomal dominant variant of CMC. The individual had had this disorder since childhood and systemic lupus erythematosus with secondary antiphospholipid syndrome, as well as renal, articular and hepatic manifestations with-out thymoma.
Keywords Candida , chronic mucocutaneous candidiasis , autoimmune diseases , systemic lupus erythematosus , autosomal dominant inheritance
Introduction
Chronic mucocutaneous candidiasis (CMC) refers to a
heterogeneous group of rare disorders characterized by
recurrent or persistent superfi cial infections of the skin,
mucous membranes, and nails by Candida spp., usually
Candida albicans [1] . Very occasionally these patients
present with systemic candidiasis, with symptoms starting
in infancy and childhood, or even adulthood, with familial
or sporadic occurrence. In relation to the association of
CMC with autoimmunity, there have been two other asso-
ciations that have been described. The fi rst one involves
patients who present with autoimmune polyendocrinopa-
thy and candidiasis with ectodermal dysplasia (APECED),
showing an autosomal recessive inheritance. In this group,
mutations in the autoimmune regulator gene ( AIRE ) have
been identifi ed [2 – 4]. The second relates to an autosomal
dominant form of CMC that occurs with hypothyroidism
[3]. It is believed that the association with autoimmune
endocrinopathy represents at least 50% of cases of CMC
© 2012 ISHAM DOI: 10.3109/13693786.2011.622305
Medical Mycology May 2012, 50, 399–403
at Serials Departm
ent on October 27, 2014
http://mm
y.oxfordjournals.org/D
ownloaded from
© 2012 ISHAM, Medical Mycology, 50, 399–403
400 de Moraes-Vasconcelos et al .
anti-double stranded DNA antibodies (1/600), chronic
lymphadenitis with extensive necrosis secondary to vascu-
litis and reactive hepatitis, leading to a diagnosis of
systemic lupus erythematosus (SLE). She was treated
with high doses of corticosteroids (methylprednisolone
500 mg/day pulses followed by prednisone 80 mg/day) and
azathioprine (100 mg/day), which led to worsening of
her infectious manifestations and eventually to bone mar-
row hypoplasia. In spite of the Candida infections since
childhood, it was only when she was 21 that CMC was
Fig. 1 Left foot showing scaly skin lesions and keratotic nail associated with paronychia. Picture taken when the patient was 26 years old.
Fig. 2 Scalp showed scarring alopecia. It is possible to observe the presence of collateral circulation in left shoulder, secondary to deep vein thrombosis
of the subclavian and jugular veins, when the patient was 26 years old.
at Serials Departm
ent on October 27, 2014
http://mm
y.oxfordjournals.org/D
ownloaded from
© 2012 ISHAM, Medical Mycology, 50, 399–403
CMC and systemic lupus erythematosus 401
She was treated and recovered satisfactorily without
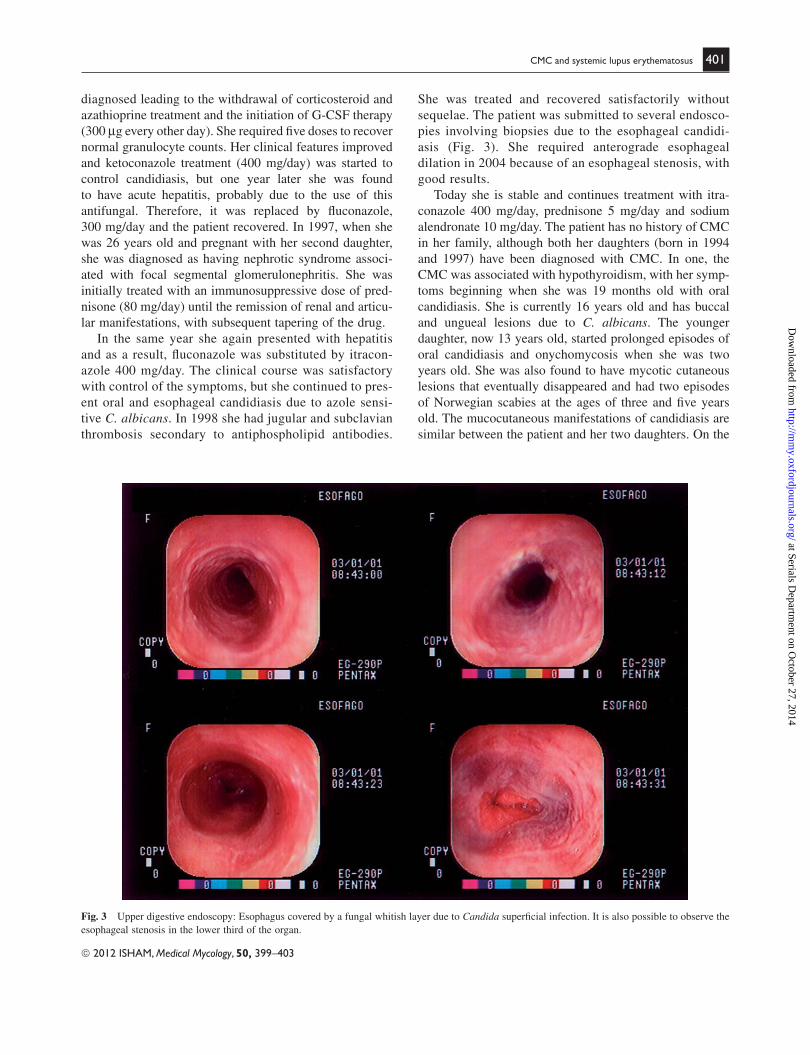
sequelae. The patient was submitted to several endosco-
pies involving biopsies due to the esophageal candidi-
asis (Fig. 3). She required anterograde esophageal
dilation in 2004 because of an esophageal stenosis, with
good results.
Today she is stable and continues treatment with itra-
conazole 400 mg/day, prednisone 5 mg/day and sodium
alendronate 10 mg/day. The patient has no history of CMC
in her family, although both her daughters (born in 1994
and 1997) have been diagnosed with CMC. In one, the
CMC was associated with hypothyroidism, with her symp-
toms beginning when she was 19 months old with oral
candidiasis. She is currently 16 years old and has buccal
and ungueal lesions due to C. albicans . The younger
daughter, now 13 years old, started prolonged episodes of
oral candidiasis and onychomycosis when she was two
years old. She was also found to have mycotic cutaneous
lesions that eventually disappeared and had two episodes
of Norwegian scabies at the ages of three and fi ve years
old. The mucocutaneous manifestations of candidiasis are
similar between the patient and her two daughters. On the
diagnosed leading to the withdrawal of corticosteroid and
azathioprine treatment and the initiation of G-CSF therapy
(300 μ g every other day). She required fi ve doses to recover
normal granulocyte counts. Her clinical features improved
and ketoconazole treatment (400 mg/day) was started to
control candidiasis, but one year later she was found
to have acute hepatitis, probably due to the use of this
antifungal. Therefore, it was replaced by fl uconazole,
300 mg/day and the patient recovered. In 1997, when she
was 26 years old and pregnant with her second daughter,
she was diagnosed as having nephrotic syndrome associ-
ated with focal segmental glomerulonephritis. She was
initially treated with an immunosuppressive dose of pred-
nisone (80 mg/day) until the remission of renal and articu-
lar manifestations, with subsequent tapering of the drug.
In the same year she again presented with hepatitis
and as a result, fl uconazole was substituted by itracon-
azole 400 mg/day. The clinical course was satisfactory
with control of the symptoms, but she continued to pres-
ent oral and esophageal candidiasis due to azole sensi-
tive C. albicans . In 1998 she had jugular and subclavian
thrombosis secondary to antiphospholipid antibodies.
Fig. 3 Upper digestive endoscopy: Esophagus covered by a fungal whitish layer due to Candida superfi cial infection. It is also possible to observe the
esophageal stenosis in the lower third of the organ.
at Serials Departm
ent on October 27, 2014
http://mm
y.oxfordjournals.org/D
ownloaded from

© 2012 ISHAM, Medical Mycology, 50, 399–403
402 de Moraes-Vasconcelos et al .
other hand, the patient presents only systemic manifesta-
tions of autoimmunity, without any endocrine organ
affected.
The diagnosis of mucocutaneous candidiasis was con-
fi rmed by identifi cation of C. albicans in cultures inocu-
lated with samples from oral and esophageal lesions, as
well as skin and ungueal specimens. Species identifi cation
was performed at the Laboratory of Mycology (LIM-53)
of the Instituto de Medicina Tropical de S ã o Paulo. Iso-
lated species were subcultured in ChromAgar Candida,
followed by micromorphological observations and bio-
chemical tests.
The patient has always presented normal levels of
plasma cortisol, serum calcium, thyroxin, thyroid-stimulat-
ing hormones and immunoglobulins IgG, IgM, IgA and
IgE. She has had numerous negative HIV tests. She has
shown no alteration in complement proteins C3 and C4,
and APH50 and CH50.
She presented severe proteinuria, up to 23 g of protein
per liter, only when the glomerulonephritis was active. At
that time she presented with ANA (1/1280) and anti-DNA
(104 IU/ml). Her peripheral blood lymphocyte prolifera-
tion test showed a normal response to phytohemagglutinin
(PHA), OKT3 and pokeweed (PWM) and a normal response
to Candida metabolic antigen (CMA), tested by tritiated
thymidine incorporation. Lymphocytes counts of CD3 � ,
CD4 � , CD8 � , CD19 � , CD3-CD16 � CD56 � were all
normal. Her Natural Killer Activity was decreased, as mea-
sured by the K562 lytic assay. The quantifi cation of cytok-
ines by ELISA in culture supernatants of PBMC stimulated
by CMA showed signifi cantly reduced levels of IL-2 and
IFN-gamma, but normal IL-4 and IL-10. The genetic anal-
ysis did not detect any mutation in the AIRE gene, exclud-
ing the possibility of an atypical presentation of
APECED.
Discussion
The diagnosis of CMC in this patient was characterized by
her history of persistent oral, esophageal and ungueal can-
didiasis and the absence of other causes of immunodefi -
ciencies, such as diabetes mellitus, cancer, AIDS, Di
George syndrome and severe combined immune defi cien-
cies. Her symptoms of chronic candidiasis began when she
was two years old, but no autoimmune manifestation
occurred until she was 21 years old. At that time, systemic
autoimmune manifestations were observed, such as arth-
ralgias and arthritis in large joints, chronic lymphadenitis
with extensive necrosis secondary to vasculitis and reactive
hepatitis, followed by nephrotic syndrome at the age of 26,
due to SLE. This diagnosis was established by the high
levels of anti-DNA (104 IU/ml) and ANA (1/1280) titers,
associated with clinical features, such as arthralgias and
arthritis; later on glomerulonephritis and eventually jugular
and subclavian thrombosis secondary to anti-phospholipid
antibodies.
Organ-specifi c endocrine autoimmunity is common
in patients with CMC, but systemic manifestations are
very rare events. In the medical literature, only one case
report of sporadic CMC associated with systemic auto-
immune manifestation (SLE), hypergammaglobulinemia
and thymoma has been described [6]. In this case, thy-
moma could explain the presence of the systemic auto-
immune manifestation. Moreover, the autoimmune
manifestations preceded the onset of candidiasis by
two years, which was followed three years later by thy-
moma. Recently, it was shown that CMC with thymoma
present autoantibodies to several cytokines of the IL-17
family [7,8].
The disorder seems to be different in our patient in
that she had manifestations of candidiasis since child-
hood, followed by autoimmune manifestations after
nearly 20 years. Her case demonstrates CMC associated
with SLE without thymoma. She has two daughters, both
of whom present CMC, characterizing a hereditary dis-
ease. One of them has CMC associated with hypothyroid-
ism, an organ-specifi c autoimmune manifestation, and
the other has only shown CMC up to now. This genetic
transmission characterizes an autosomal dominant inher-
itance, different from the variants previously described
[5,7]. This unique case is probably a new form of CMC
that is characterized by systemic autoimune manifesta-
tion associated with an autosomal dominant inheritance.
Follow-up on this family will continue, in an attempt to
extend our evaluation involving the genetic aspects of
this disorder.
To our knowledge this is the fi rst described case of auto-
somal dominant CMC with Systemic Lupus erythematosus.
Acknowledgements
This work was partially supported by Funda ç ã o de Amparo
a Pesquisa de S ã o Paulo (FAPESP) grant number,
02/00024-2 and 99/07399-7.
Declaration of interest : The authors report no confl icts of
interest. The authors alone are responsible for the content
and writing of the paper.
References
Kirkpatrick CH. Chronic mucocutaneous candidiasis. 1 Pediatr Infect Dis J 2001; 20 : 197 – 206.
Villase ñ or J, Benoist C, Mathis D. AIRE and APECED: molecular 2
insights into an autoimmune disease. Immunol Rev 2005; 204 : 156 – 164.
at Serials Departm
ent on October 27, 2014
http://mm
y.oxfordjournals.org/D
ownloaded from

© 2012 ISHAM, Medical Mycology, 50, 399–403
CMC and systemic lupus erythematosus 403
Sam WM, Snyderman R, Jegasothy BV, 5 et al . Chronic mucocutaneous
candidiasis. Immunologic studies of three generations in a single fam-
ily. Am J Med 1979; 67 : 948 – 958.
San Filippo J. Chronic mucocutaneous candidiasis associated with 6
malignant thymoma and systemic lupus erythematosus with hyper-
gammaglobulinemia: a case report and literature review. Cutis 2006;
78 : 57 – 60.
Atkinson TP, Schaffer AA, Grimbacher B, 3 et al . An immune defect
causing dominant chronic mucocutaneous candidiasis and thyroid
disease maps to chromosome 2p in a single family. Am J Hum Genet 2001; 69 : 791 – 803.
Coleman R, Hay RJ. Chronic mucocutaneous candidosis associated 4
with hypothyroidism: a distinct syndrome? Br J Dermatol 1997; 136 :
24 – 29.
This paper was fi rst published online on Early Online on 10 October 2011.
at Serials Departm
ent on October 27, 2014
http://mm
y.oxfordjournals.org/D
ownloaded from