Embed Size (px)
Citation preview

Transfusion and Apheresis Science 42 (2010) 97–99
Contents lists available at ScienceDirect
Transfusion and Apheresis Science
journal homepage: www.elsevier .com/ locate/ t ransc i
Letter to the editor
Circulating endothelial cells in whole blood donationsand the effect of leucodepletion
The existence of circulating endothelial cells (CECs) inhuman peripheral blood was first described in patientswith vascular injury [2] and following the novel identifica-tion of endothelial progenitor cells, EPCs [1], special con-sideration has been directed towards these types of cellsand their role in angiogenesis, postnatal vasculogenesis,restoration of the damaged endothelium and malignantgrowth [10].
In the normal population, low numbers of CEC arepresent in peripheral blood but a normal range has notbeen precisely identified. This could be between 0.01%and 0.0001% of all mononuclear cells [5]. A value of0–20 cells/ml has been suggested using a bead techniquewhile another group, using flow cytometry based method-ology, reported surprisingly high levels of 7900 cells/ml [6]possibly due to counting large platelets [9].
Blood for transfusion is collected from the peripheralcirculation of healthy donors. This suggests that a numberof EPCs and CECs could be collected alongside blood cells.Unless removed during processing of blood by proceduressuch as leucodepletion, such cells could be transfused torecipients of blood transfusion. The clinical significanceof this is not known. However, consideration should be gi-ven to the possible role of these cells in promoting angio-genesis in blood transfusion recipients and triggering theproduction of anti-endothelial cell antibodies which maybe associated with transplant rejection [7]. Also EC canact as a reservoir for blood-born prion protein [8].
This study examined the efficacy of leucodepletion fil-ters in removing endothelial cells present in whole blooddonations.
Venous blood (4 ml) was obtained from 15 healthyvolunteers (F = 9, M = 6, age range = 22–59 years) in tubescontaining sodium ethylenediaminetetraacidic acid(EDTA). Samples were tested by FACS within 2 h. Pre-fil-tered citrated whole blood donations (WBD) from 40 anon-ymous donors (F = 16, M = 24, age range = 17–68 years)were tested similarly. Two millilitres was obtained fortesting from each donation before leucodepletion filtra-tion. Another group of 25 anonymous WBD (F = 12, M =13, age range = 19–64 years) were tested before and afterleucodepletion filtration (Bags R8477 Baxter with RZ-
1473-0502/$ - see front matter � 2009 Elsevier Ltd. All rights reserved.doi:10.1016/j.transci.2009.10.011
2000 Sepacell filters) using an immunomagnetic isolationtechnique. Given the logistics involved, WBD for both tech-niques were obtained 18 h after collection.
Full blood counts were performed on every sampleusing a LH750 analyser (Beckman Coulter, High Wycombe,UK). Donor age, gender and ABO blood group were also col-lected. Scientific and ethical approval was granted for thisstudy by the University of Sheffield Research Ethics Com-mittee (UREC).
EPCs and CECs were enumerated by four colour flowcytometry (FACS Calibur, Becton Dickinson) using a panelof monoclonal antibodies. To count EPCs, 200 lL of periph-eral blood, previously incubated with FcR blocking reagentfor 10 min, was incubated for 20 min in the dark withmonoclonal antibodies against CD45 (PerCp) (to excludehematopoietic cells), CD144 (FITC), CD133 (PE) and VEG-FR2 (APC). Mature CEC markers used were CD144 (FITC),CD34 (PE), CD45 (Per Cp), and CD31 (APC). Isotype controlswere used in each assay. After ErythrolyseTM (Serotec, Ox-ford), the cells were then washed twice (with 1% w/v PBSA,0.6% w/v sodium citrate buffer) and suspended in 0.5% v/vformaldehyde solution. All samples were analysed induplicate. Flow cytometry absolute count standard beadswere used to obtain an absolute number of cells. For FACS,mononuclear cells were first gated and cells were then se-lected from the CD45dim/-ve plus CD34+ or CD133+ popu-lation. These cells were then gated for double staining withdifferent combinations of more specific endothelial cellmarkers. The positive events in the upper right quadrantswere considered to be indicative of CECs or EPCs.
Since leucodepletion removes most WBCs, FACS cannotbe used for post filtration samples. CEC were determinedpost filtration by a modified immunomagnetic bead isola-tion method [11]. M-450 Dynabeads (Dynal, Norway) werecoated with anti CD146 (Biocytex, France) and mixed withwhole blood (1 ml) and 1 ml of buffer (phosphate bufferedsaline, 0.1% w/v bovine serum albumin, 0.1% w/v sodiumazide, and 0.6% w/v sodium citrate). One hundred andtwenty-five microlitres of antibody-coated Dynabeadsand 20 ll FcR blocking agent (Militenyi, Germany) wereadded and the samples were mixed for 30 min at roomtemperature. After washing, 2 lg/ml of Hoechst 33342stain was added to exclude false counting of any non-spe-cific debris. Ten microlitres of 2 mg/ml Ulex europaeus lec-tin-1 (UAE-1) FITC (Victor labs, UK) was then added for30 min in the dark. Samples were washed and dissolved
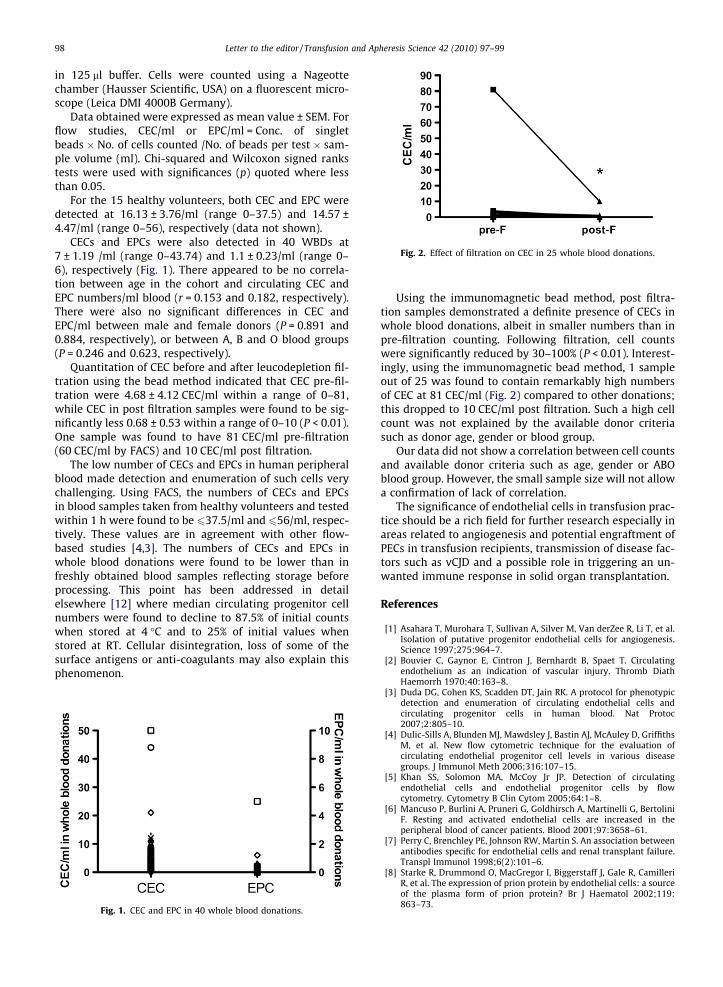
Fig. 2. Effect of filtration on CEC in 25 whole blood donations.
98 Letter to the editor / Transfusion and Apheresis Science 42 (2010) 97–99
in 125 ll buffer. Cells were counted using a Nageottechamber (Hausser Scientific, USA) on a fluorescent micro-scope (Leica DMI 4000B Germany).
Data obtained were expressed as mean value ± SEM. Forflow studies, CEC/ml or EPC/ml = Conc. of singletbeads � No. of cells counted /No. of beads per test � sam-ple volume (ml). Chi-squared and Wilcoxon signed rankstests were used with significances (p) quoted where lessthan 0.05.
For the 15 healthy volunteers, both CEC and EPC weredetected at 16.13 ± 3.76/ml (range 0–37.5) and 14.57 ±4.47/ml (range 0–56), respectively (data not shown).
CECs and EPCs were also detected in 40 WBDs at7 ± 1.19 /ml (range 0–43.74) and 1.1 ± 0.23/ml (range 0–6), respectively (Fig. 1). There appeared to be no correla-tion between age in the cohort and circulating CEC andEPC numbers/ml blood (r = 0.153 and 0.182, respectively).There were also no significant differences in CEC andEPC/ml between male and female donors (P = 0.891 and0.884, respectively), or between A, B and O blood groups(P = 0.246 and 0.623, respectively).
Quantitation of CEC before and after leucodepletion fil-tration using the bead method indicated that CEC pre-fil-tration were 4.68 ± 4.12 CEC/ml within a range of 0–81,while CEC in post filtration samples were found to be sig-nificantly less 0.68 ± 0.53 within a range of 0–10 (P < 0.01).One sample was found to have 81 CEC/ml pre-filtration(60 CEC/ml by FACS) and 10 CEC/ml post filtration.
The low number of CECs and EPCs in human peripheralblood made detection and enumeration of such cells verychallenging. Using FACS, the numbers of CECs and EPCsin blood samples taken from healthy volunteers and testedwithin 1 h were found to be 637.5/ml and 656/ml, respec-tively. These values are in agreement with other flow-based studies [4,3]. The numbers of CECs and EPCs inwhole blood donations were found to be lower than infreshly obtained blood samples reflecting storage beforeprocessing. This point has been addressed in detailelsewhere [12] where median circulating progenitor cellnumbers were found to decline to 87.5% of initial countswhen stored at 4 �C and to 25% of initial values whenstored at RT. Cellular disintegration, loss of some of thesurface antigens or anti-coagulants may also explain thisphenomenon.
Fig. 1. CEC and EPC in 40 whole blood donations.
Using the immunomagnetic bead method, post filtra-tion samples demonstrated a definite presence of CECs inwhole blood donations, albeit in smaller numbers than inpre-filtration counting. Following filtration, cell countswere significantly reduced by 30–100% (P < 0.01). Interest-ingly, using the immunomagnetic bead method, 1 sampleout of 25 was found to contain remarkably high numbersof CEC at 81 CEC/ml (Fig. 2) compared to other donations;this dropped to 10 CEC/ml post filtration. Such a high cellcount was not explained by the available donor criteriasuch as donor age, gender or blood group.
Our data did not show a correlation between cell countsand available donor criteria such as age, gender or ABOblood group. However, the small sample size will not allowa confirmation of lack of correlation.
The significance of endothelial cells in transfusion prac-tice should be a rich field for further research especially inareas related to angiogenesis and potential engraftment ofPECs in transfusion recipients, transmission of disease fac-tors such as vCJD and a possible role in triggering an un-wanted immune response in solid organ transplantation.
References
[1] Asahara T, Murohara T, Sullivan A, Silver M, Van derZee R, Li T, et al.Isolation of putative progenitor endothelial cells for angiogenesis.Science 1997;275:964–7.
[2] Bouvier C, Gaynor E, Cintron J, Bernhardt B, Spaet T. Circulatingendothelium as an indication of vascular injury. Thromb DiathHaemorrh 1970;40:163–8.
[3] Duda DG, Cohen KS, Scadden DT, Jain RK. A protocol for phenotypicdetection and enumeration of circulating endothelial cells andcirculating progenitor cells in human blood. Nat Protoc2007;2:805–10.
[4] Dulic-Sills A, Blunden MJ, Mawdsley J, Bastin AJ, McAuley D, GriffithsM, et al. New flow cytometric technique for the evaluation ofcirculating endothelial progenitor cell levels in various diseasegroups. J Immunol Meth 2006;316:107–15.
[5] Khan SS, Solomon MA, McCoy Jr JP. Detection of circulatingendothelial cells and endothelial progenitor cells by flowcytometry. Cytometry B Clin Cytom 2005;64:1–8.
[6] Mancuso P, Burlini A, Pruneri G, Goldhirsch A, Martinelli G, BertoliniF. Resting and activated endothelial cells are increased in theperipheral blood of cancer patients. Blood 2001;97:3658–61.
[7] Perry C, Brenchley PE, Johnson RW, Martin S. An association betweenantibodies specific for endothelial cells and renal transplant failure.Transpl Immunol 1998;6(2):101–6.
[8] Starke R, Drummond O, MacGregor I, Biggerstaff J, Gale R, CamilleriR, et al. The expression of prion protein by endothelial cells: a sourceof the plasma form of prion protein? Br J Haematol 2002;119:863–73.

Letter to the editor / Transfusion and Apheresis Science 42 (2010) 97–99 99
[9] Strijbos MH, Kraan J, Sleijfer S, Gratama JW. Cells meeting ourimmunophenotypic criteria of endothelial cells are large platelets.Cytometry B Clin Cytom 2007; Jan 24; 17252604 (P,S,G,E,B,D).
[10] Young PP, Vaughan DE, Hatzopoulos AK. Biologic properties ofendothelial progenitor cells and their potential for cell therapy. ProgCardiovasc Dis 2007;49(6):421–9.
[11] Woywodt A, Goldberg C, Scheer J, Regelsberger H, Haller H, HaubitzM. An improved assay for enumeration of circulating endothelialcells. Ann Hematol 2004;83:491–4.
[12] Woywodt A, Blann AD, Kirsch T, Erdbruegger U, Banzet N, Haubitz M.Isolation and enumeration of circulating endothelial cells byimmunomagnetic isolation: proposal of a definition and aconsensus protocol. J Thromb Haemost 2006;4:671–7.
A. Al-MalkiDepartment of Cardiovascular Science,
The Medical School,University of Sheffield,
UK
S. NewtonFACS Core Facility,
The Medical School,University of Sheffield,
UK
S.E. FrancisDepartment of Cardiovascular Science,
The Medical School,University of Sheffield,
UK
K.El-GharianiNHS Blood and Transplant,
Sheffield Centre, Longley Lane,Sheffield S5 7JN,
UKTel.: +44 0114 2034820; fax: +44 0114 2034910.
E-mail address: [email protected]





























