Embed Size (px)
DESCRIPTION
orto
Citation preview

204 THE JOURNAL OF BONE AND JOINT SURGERY
L. J. O’Hara, FRCS, Specialist RegistrarPoole General Hospital, Longfleet Road, Poole, Dorset BH15 2JB, UK.
J. W. Barlow, FRCS Orth, Consultant Orthopaedic SurgeonDorset County Hospital, Williams Avenue, Dorchester, Dorset DT1 2JY,UK.
N. M. P. Clarke, ChM, FRCS, Consultant Orthopaedic SurgeonSouthampton General Hospital, Tremona Road, Southampton SO16 6YD,UK.
Correspondence should be sent to Mr N. M. P. Clarke.
©2000 British Editorial Society of Bone and Joint Surgery0301-620X/00/29570 $2.00
Displaced supracondylar fractures of thehumerus in childrenAUDIT CHANGES PRACTICE
L. J. O’Hara, J. W. Barlow, N. M. P. ClarkeFrom Southampton General Hospital, England
We performed an audit of 71 children withconsecutive displaced, extension-type
supracondylar fractures of the humerus over a periodof 30 months. The fractures were classified accordingto the Wilkins modification of the Gartland system.There were 29 type IIA, 22 type IIB and 20 type III.We assessed the effectiveness of guidelines proposedafter a previous four-year review of 83 supracondylarfractures. These recommended that: 1) an experiencedsurgeon should be responsible for the initialmanagement; 2) closed or open reduction of type-IIBand type-III fractures must be supplemented bystabilisation with Kirschner (K-) wires; and 3) K-wiresof adequate thickness (1.6 mm) must be used in acrossed configuration.
The guidelines were followed in 52 of the 71 cases.When they were observed there were no reoperationsand no malunion. In 19 children in whom they hadnot been observed more than one-third requiredfurther operation and six had a varus deformity.Failure to institute treatment according to theguidelines led to an unsatisfactory result in 11patients. When they were followed the result oftreatment was much better. We have devised aprotocol for the management of these difficult injuries.
J Bone Joint Surg [Br] 2000;82-B:204-10.Received 19 October 1998; Accepted after revision 30 April 1999
Supracondylar fracture of the humerus is the second mostcommon fracture in children (16.6%) and the most frequentbefore the age of seven years.1 In 1959 Gartland2 com-mented that “it is interesting to observe the trepidation withwhich men, otherwise versed in trauma, approach a freshsupracondylar fracture”. The dread of this injury stillremains. Treatment is controversial and often technicallydifficult; complications are common. Cubitus varus is themost frequent problem with a mean incidence of 30% in theseries reviewed by Smith.3 This deformity is due to medialtilting of the distal fragment, associated with rotation.3 Itdoes not remodel with growth,4-6 is not progressive and isnot due to physeal injury.5 Injury to any of the three majornerves around the elbow occurs in 6% to 16% of cases.7
The radial pulse is absent in about 3% after reduction of thefracture.8 Volkmann’s ischaemic contracture is rare, with anincidence of 1.1 in 1000,9 but is still seen.10-12 Stiffness ofthe elbow may occur, particularly after repeated manipula-tion and the use of the posterior approach for open reduc-tion. In most cases, however, there is improvement withtime and the functional result is not greatly impaired.5,6
A variety of methods of treatment for displaced fractureshas been recommended including closed reduction andimmobilisation,2,4,13-18 traction by various methods19-22
and closed23-32 or open reduction33-36 stabilised by Kirsch-ner (K-) wires. Although some authors are not in favour ofclosed reduction and immobilisation,11 particularly forsevere injuries, this treatment remains popular.18 Othersrecommend stabilisation by K-wires for all displacedfractures.31
The aim of treatment is to gain a functional and cosmet-ically acceptable upper limb with a normal range of move-ment.37 Ideally, this should be achieved by one definitiveprocedure. A change in treatment because of loss of reduc-tion may be psychologically traumatic to the child, maygive rise to parental anxiety38 and is associated with anincreased risk of a poor outcome.11
Before October 1994 there were no specific guidelinesfor the treatment of these fractures at our institution. Theywere managed by a number of different regimes whichwere supervised by several orthopaedic/trauma consultantsurgeons. Between January 1990 and July 1994 a retro-spective review of 93 displaced fractures was performedwith adequate follow-up in 83.39 All the injuries were

classified using the modification of the Gartland system2 byWilkins40 (Table I; Fig. 1). The results were excellent in alltype-IIA injuries. In type-IIB and type-III fractures therewas an unacceptable rate of reoperation of 29% (19 of 65cases) for redisplacement. In total, these 19 patients had 42operations. The indications for reoperation in this retro-spective study were reangulation or redisplacement of thefracture or rotation of the fragments predisposing to medialtilting and subsequent varus deformity. In eight of the 65patients there was an unsatisfactory outcome because of
cubitus varus ranging from 5° to 10°. So far two of thesechildren have required corrective surgery. Analysis of the
205DISPLACED SUPRACONDYLAR FRACTURES OF THE HUMERUS IN CHILDREN
VOL. 82-B, NO. 2, MARCH 2000
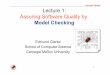
Table I. Classification of supracondylar fractures of the humerusin children after Gartland2 and Wilkins40
Type
I Undisplaced fracture
IIA Greenstick fracture with posterior angulation
IIB Greenstick fracture with malrotation + posterior angulation
III Completely displaced fracture
Fig. 1a Fig. 1b
Fig. 1c
Radiographs of supracondylar fractures of the humerusshowing a) type IIA, displaced with posterior angulation, b)type IIB, displaced with malrotation + posterior angulationand c) type III, completely displaced with no corticalcontact.

patients who required reoperation suggested that the fol-lowing factors led to a suboptimal result.
1) Inexperience of the surgeon responsible for the initialmanagement of the fractures.
2) Failure to supplement closed reduction of type-IIBand type-III fractures with K-wires.
3) The use of K-wires of less than 1.6 mm in diameter.4) The use of a lateral K-wire configuration.As a result the following guidelines for treatment were
proposed.1) An experienced surgeon should be responsible for the
initial management. Such a surgeon was defined as onewho could competently perform initial closed reduction andfixation by crossed K-wires and if necessary open reduc-tion. Traction and conservative methods of treatment werenot considered therapeutic options for type-IIB and type-IIIfractures within these guidelines.
2) Closed or open reduction of type-IIB and type-IIIfractures must be supplemented with stabilisation by K-wires. The indication for open reduction was failure ofclosed manipulation.
3) K-wires of adequate thickness (1.6 mm) must be usedin a crossed configuration.
After the introduction of these guidelines a further auditof 71 consecutive cases of displaced supracondylar fractureof the humerus was carried out over a 30-month period. Wenow report the results in regard to the protocol of treatmentand the provision of resources.
Patients and Methods
Between October 1994 and March 1997, 71 consecutivechildren with displaced, extension-type supracondylar frac-tures of the humerus were entered into the study. Inpatientcare and outpatient follow-up were analysed using hospitalnotes, details of the operation, and plain radiographs.
There were 41 boys and 30 girls with a mean age of sixyears (1 to 11). The fractures were classified according tothe Wilkins40 modification of the Gartland2 system. Therewere 29 type-IIA, 22 type-IIB and 20 type-III fractures.There was one grade-I open injury occurring in a type-IIIfracture and one case of an associated ipsilateral fracture ofthe distal radius.
In six children the radial pulse was absent on presenta-tion, but distal pulses returned after reduction of the frac-ture in five. The sixth child required further intervention.There were neurological complications in five children, inthree palsy of the median nerve and in two injury to theradial nerve. All of which resolved within eight weeks.
The patients were allocated retrospectively into twogroups based on the guidelines for treatment suggested bythe previous four-year audit. In group 1 (52 patients) theguidelines were followed but in group 2 (19) they were notobserved. This allocation was made in a blinded fashionafter assessing the management of a patient but withoutknowledge of the outcome. The two groups were then
compared with regard to the rate of reoperation, the rangeof elbow movement and cosmetic deformity.
Patients were followed up until there was full recoveryor the clinical situation was stable. This ranged from threemonths to one year on the basis that varus angulationoccurs as a result of malreduction and not abnormalgrowth.
Results
Of the 29 type-IIA fractures, 22 were managed non-oper-atively by a collar and cuff or immobilisation in plaster. Inseven, posterior angulation of the fracture led to a humero-capitellar angle of less than 0° and it was decided toperform a closed reduction. All 29 children in this grouphad an excellent outcome with a full range of movementand a normal carrying angle. No further operation wasrequired after the primary procedure.
Table II gives the methods of treatment used for the 22type-IIB and 20 type-III injuries.
In 31 children fixation was by K-wires. A crossed config-uration was used in 24 and lateral K-wires alone in seven.When a crossed configuration was used the ulnar nerve wasidentified in each case using a medial incision beforeinsertion of the medial wire. There were no cases ofiatrogenic palsy of the ulnar nerve.
The results were unsatisfactory in 11 of the 42 type-IIBand type-III fractures. Seven reoperations were required forredisplacement of the fracture and six for varus deformity.On discharge all the patients had a functional range ofmovement within 10° of the normal arc. Table III sum-marises the results.
When the guidelines for treatment were followed nopatient required reoperation or developed deformity of thecarrying angle. When the guidelines were not observed 11children required reoperation and/or developed a varusdeformity.
206 L. J. O'HARA, J. W. BARLOW, N. M. P. CLARKE
THE JOURNAL OF BONE AND JOINT SURGERY
Table II. Methods of treatment used for type-IIB (22) and type-III(20) fractures
Type of fracture
Treatment IIB III
Plaster immobilisation 3 0
Closed reduction and immobilisation 7 1
Closed reduction and K-wire fixation 7 10
Open reduction and K-wire fixation 5 9
Table III. The results of treatment in the 22 type-IIB and 20type-III fractures
Type of fracture
Outcome* IIB III
Single operation 14 18
Reoperation 5 2
Normal carrying angle (degrees) 20 16
*three type-IIB fractures were treated non-operatively

Analysis of the 11 unsatisfactory results showed thatclosed reduction of type-IIB and type-III fractures withoutstabilisation by K-wires led to an unsatisfactory result infive out of eight patients. They required four further opera-tions for loss of reduction and one for varus deformity. Thisoccurred in a type-IIB fracture which redisplaced and hadno operative treatment.
Use of lateral K-wires alone led to an unsatisfactoryresult in four out of seven patients because of redisplace-ment of the fracture despite an initial anatomical reduction.One of these had no further surgical treatment and devel-oped cubitus varus (Fig. 2). In the other three children whohad a second operation two developed varus malunion. Inone, lateral K-wires were used again and in the othercrossed K-wires failed to engage the proximal cortex.
Non-operative treatment of type-IIB fractures led tocubitus varus in one out of three children treated by thismethod.
Four operations were performed by inexperienced sur-geons. Three of these had further surgery. In one patientpoor reduction of a type-III fracture, stabilised by fixationwith cross wires led to cubitus varus.
There were three complications related to operative treat-ment. Two patients developed pin-site infection whichresponded to antibiotics and one had a postoperative neura-praxia of the radial nerve which resolved spontaneously.There were no cases of infection in those fractures requir-ing open reduction and none of Volkmann’s ischaemiccontracture.
Discussion
The many different methods advocated for supracondylarfractures of the humerus in children suggest that no singletechnique is suitable for all types of fracture. The displacedsupracondylar fracture represents a spectrum of injury fromtype IIA with minor swelling of soft tissues to type III withconsiderable swelling and potential neurovascular compli-cations. A selective approach to treatment is required basedon the classification of the fracture and the soft-tissuecomplications present.
Closed reduction and immobilisation require 120° ofelbow flexion to maintain stable reduction.15 There are twodisadvantages to this method, described by McLaughlin41
as the “supracondylar dilemma”. Flexion to 120° in aswollen elbow may compromise the circulation but lessflexion predisposes to loss of reduction. This method has ahigh incidence of poor results when used for all types offracture.6,11 Some authors have used manipulation andimmobilisation in plaster as their first line of treatment andthen remanipulate or change their treatment if there is lossof reduction. Further manipulation, however, predisposes tostiffness and myositis ossificans.5 Mitchell and Adams6
reported an incidence of 60% of cubitus varus deformityusing this method; 19% of their patients had three manip-ulations. Eleven of their patients had less severe injuries,however, equivalent to Gartland-Wilkins type IIA of whomnine had satisfactory results. Pirone et al11 found that only51% of patients had excellent results using manipulation
207DISPLACED SUPRACONDYLAR FRACTURES OF THE HUMERUS IN CHILDREN
VOL. 82-B, NO. 2, MARCH 2000
Fig. 2a Fig. 2b Fig. 2c
Radiographs showing a) a type-III fracture in a nine-year-old boy, b) after treatment by closed reduction and parallel lateralpercutaneous K-wires and c) loss of anatomical reduction with no further surgical treatment leading to a cubitus varus deformity.

and plaster and concluded that its use was inappropriate forthe displaced supracondylar fracture. Their series, however,did not provide individual results for type-IIA and type-IIBfractures. Recently, Hadlow et al18 have recommendedmanipulation and immobilisation in plaster for all types offracture, despite 31% of children requiring further operativetreatment and the development of a number of varusdeformities when loss of position was unrecognised withtype-III fractures treated in plaster.
We believe that closed reduction and immobilisation aresatisfactory for type-IIA fractures only. This fracture usual-ly presents with mild swelling and vascular complicationsare infrequent.2,20 Eight patients in our series with type-IIBand type-III fractures had non-guideline treatment byclosed reduction without fixation and in six of these thefracture redisplaced. Type-IIA fractures usually do not haveneurovascular complications or major swelling and can bemanaged in flexion in a collar and cuff or plaster. They maynot even require reduction provided that the angle of thedistal humeral articular surface measures at least 0° withthe shaft.2 We treated 22 type-IIA fractures with immo-bilisation alone and all had satisfactory results. We did notencounter a situation where there was sufficient elbow
swelling to compromise the circulation. If this had occurredwe would consider this to be an indication for K-wirestabilisation of a type-IIA fracture.
Skin traction19,20 and skeletal traction21,22 have beenrecommended particularly when there is concern regardingswelling of soft tissues. The incidence of cubitus varus,however, may be high when compared with percutaneouspinning.42 Hospital stay is likely to be longer withincreased costs.42,43 Volkmann’s contracture has beenreported.12 We have not found marked swelling to be anobstacle to closed pinning or open reduction and dis-continued using traction after our initial audit because ofpoor results in over half of our cases.
Closed reduction and percutaneous pinning are nowwidely recommended. Wilkins31 has advocated stabilisationby K-wires for all displaced fractures. The inpatient stay isreduced and the elbow can be immobilised in a moreextended position reducing concern about limb perfusion ininjuries with major swelling of soft tissues. Flynn et al5
found no evidence of physeal injury secondary to insertionof K-wires when smooth wires were used. Pin-track infec-tion occurred in only two pins in our series without seque-lae. Iatrogenic injury to the ulnar nerve5,27,44,45 may occureven when the medial epicondyle is palpable.31 Lateral K-wires have been recommended to avoid this complica-tion.27-30,32 Biomechanical studies46,47 have shown,however, that a crossed medial and lateral K-wire config-uration is more stable than lateral pins alone. Redisplace-ment of the fracture has been reported to be significant afterthe use of lateral K-wires.30,32 A lateral K-wire configura-tion may not allow full extension of the elbow thus prevent-ing examination of the carrying angle at operation.37 In ourstudy redisplacement occurred in four out of seven patientswhen a lateral pin configuration was used. We wouldtherefore recommend identification of the ulnar nerve witha medial incision and crossed K-wire stabilisation. We hadno iatrogenic injuries to the ulnar nerve.
The indications for open reduction and pin fixationinclude a fracture which is irreducible by closed methods;an open fracture and vascular injury. Open reduction hasbeen advocated as the primary procedure in all cases.33-36
Others have condemned this approach because of concernsabout infection and loss of movement.4,6 Those serieswhich demonstrated significant loss of movement, how-ever, were reported by surgeons who used a posterior
208 L. J. O'HARA, J. W. BARLOW, N. M. P. CLARKE
THE JOURNAL OF BONE AND JOINT SURGERY
Fig. 3
Radiograph showing a type-III fracture treated by closed reduction andcrossed K-wire stabilisation.
Fig. 4
The Southampton protocol for the treatment ofpaediatric supracondylar fracture of the humerus.

approach or resorted to surgery only after repeated closedmanipulations.33,35 Open reduction was required in 14 outof 31 patients stabilised by K-wires. There were no epi-sodes of superficial or deep infection and no functional lossof movement.
Four patients in our series were treated initially byinexperienced surgeons and all had a poor result with eitherreoperation or development of a cubitus varus. Surgeons ofadequate experience were available on these particularoccasions but there was a failure to request advice orassistance. The other patients were treated by experiencedsurgeons, but the results were poor when the guidelineswere not followed. These problems have since beenaddressed. These fractures are now managed by two con-sultant paediatric orthopaedic surgeons who should beinformed of all patients undergoing operative treatment.
There was a clear difference in results when the guide-lines were not followed. Although a satisfactory outcomemay be obtained in terms of limb function with furthersurgery after the primary operation, we believe that initialtreatment should be definitive. A second surgical procedureis more difficult to perform and can be associated with anadverse outcome.11 Is it acceptable for a child to be sub-jected to the psychological trauma of a second operationbecause of inappropriate initial treatment? Based on ourguidelines we have now introduced a treatment protocol(Figs 3 and 4) for use at this hospital.
Although the audit loop may not have been technicallyclosed we feel that the difference in outcome between theguideline and non-guideline groups is so clear that a furtheraudit to define the best clinical management would beinappropriate. In effect this would be an audit of whethersurgeons are capable of following guidelines. Our study haspinpointed the deficiencies in both the operative manage-ment of the supracondylar fracture of the humerus inchildren as well as flaws in the appropriate use of availableresources. These deficiencies have both now beenaddressed with the introduction of a formal treatment proto-col as well as an alteration in the emergency senior cover ofinjuries in children as discussed above.
No benefits in any form have been received or will be received from acommercial party related directly or indirectly to the subject of thisarticle.
References1. Cheng JC, Shen WY. Limb fracture pattern in different pediatric age
groups: a study of 3350 children. J Orthop Trauma 1993;7:15-22.2. Gartland JJ. Management of supracondylar fractures of the humerus
in children. Surg Gynecol Obstet 1959;109:145-54.3. Smith L. Deformity following supracondylar fractures of the humerus.
J Bone Joint Surg [Am] 1960;42-A:235-52. 4. Attenborough CG. Remodelling of the humerus after supracondylar
fractures in childhood. J Bone Joint Surg [Br] 1953;35-B:386-95. 5. Flynn JC, Matthews JG, Benoit RL. Blind pinning of displaced
supracondylar fractures of the humerus in children: sixteen years'experience with long-term follow-up. J Bone Joint Surg [Am]1974;56-A:263-72.
6. Mitchell WJ, Adams JP. Supracondylar fractures of the humerus inchildren: a ten-year review. JAMA 1961;175:573-7.
7. Cramer KE, Green NE, Devito DP. Incidence of anterior inter-osseous nerve palsy in supracondylar humerus fractures in children.J Pediatr Orthop 1993;13:502-5.
8. Sabharwal S, Tredwell SJ, Beauchamp RD, et al. Management ofpulseless pink hand in pediatric supracondylar fractures of humerus.J Pediatr Orthop 1997;17:303-10.
9. Walloe A, Egund N, Eikelund L. Supracondylar fracture of thehumerus in children: review of closed and open reduction leading to aproposal for treatment. Injury 1985;16:296-9.
10. Mubarak SJ, Carroll NC. Volkmann's contracture in children: aetiol-ogy and prevention. J Bone Joint Surg [Br] 1979;61-B:285-93.
11. Pirone AM, Graham HK, Krajbich JI. Management of displacedextension-type supracondylar fractures of the humerus in children. JBone Joint Surg [Am] 1988;70-A:641-50.
12. Copley LA, Dormans JP, Davidson RS. Vascular injuries and theirsequelae in pediatric supracondylar humeral fractures: towards a goalof prevention. J Pediatr Orthop 1996;16:99-103.
13. Charnley JC. The closed treatment of common fractures. 3rd ed.Edinburgh, etc: Churchill Livingstone, 1961.
14. Khare GN, Gautam VK, Kochhar VL, Anand C. Prevention ofcubitus varus deformity in supracondylar fractures of the humerus.Injury 1991;22:202-6.
15. Millis MB, Singer IJ, Hall JE. Supracondylar fracture of the humerusin children: further experience with a study in orthopaedic decisionmaking. Clin Orthop 1984;188:90-7.
16. Hart GM, Wilson DW, Arden GP. The operative management of thedifficult supracondylar fracture of the humerus in the child. Injury1977;9:30-4.
17. Buhl O, Hellberg S. Displaced supracondylar fractures of the humer-us in children. Acta Orthop Scand 1982;53:67-71.
18. Hadlow AT, Devane P, Nicol RO. A selective treatment approach tosupracondylar fracture of the humerus in children. J Pediatr Orthop1996;16:104-6.
19. Dodge HS. Displaced supracondylar fractures of the humerus inchildren: treatment by Dunlop's traction. J Bone Joint Surg [Am]1972;54-A:1408-18.
20. Piggot J, Graham HK, McCoy GF. Supracondylar fractures of thehumerus in children: treatment by straight lateral traction. J Bone JointSurg [Br] 1986;68-B:577-83.
21. Worlock PH, Colton CL. Displaced supracondylar fractures of thehumerus in children treated by overhead olecranon traction. Injury1984;15:316-21.
22. Palmer EE, Niemann KMW, Vesely D, Armstrong JH. Supracondy-lar fracture of the humerus in children. J Bone Joint Surg [Am]1978;60-A:653-6.
23. Swenson AL. The treatment of supracondylar fractures of the humerus byKirschner-wire transfixion. J Bone Joint Surg [Am] 1948;30-A:993-7.
24. Haddad RJ, Saer JK, Riordan DC. Percutaneous pinning of dis-placed supracondylar fractures of the elbow in children. Clin Orthop1970;71:112-7.
25. Nacht JL, Ecker ML, Chung SMK, Lotke PA, Das M. Supracondy-lar fractures of the humerus in children treated by closed reduction andpercutaneous pinning. Clin Orthop 1983;177:203-9.
26. Mehserle WL, Meehan PL. Treatment of the displaced supracondylarfracture of the humerus (type III) with closed reduction and percuta-neous cross pin fixation. J Pediatr Orthop 1991;11:705-11.
27. Gjerloff C, Sojbjerg JO. Percutaneous pinning of supracondylarfractures of the humerus. Acta Orthop Scand 1978;49:597-9.
28. Fowles JV, Kassab MT. Displaced supracondylar fractures of theelbow in children: a report on the fixation of extension and flexionfractures by two lateral percutaneous pins. J Bone Joint Surg [Br]1974;56-B:490-500.
29. Aronson DD, Prager BI. Supracondylar fractures of the humerus inchildren: a modified technique for closed pinning. Clin Orthop1987;219:174-84.
30. Ariño VL, Lluch EE, Ramirez AM, et al. Percutaneous fixation ofsupracondylar fractures of the humerus in children. J Bone Joint Surg[Am] 1977;59-A:914-6.
31. Wilkins KE. Supracondylar fractures of the humerus. In: Operativemanagement of upper extremity fractures in children. AA monographseries, 1994.
32. Kallio PE, Foster BK, Paterson DC. Difficult supracondylar elbowfractures in children: analysis of percutaneous pinning technique.J Pediatr Orthop 1992;12:11-5.
209DISPLACED SUPRACONDYLAR FRACTURES OF THE HUMERUS IN CHILDREN
VOL. 82-B, NO. 2, MARCH 2000

33. Carcassonne M, Bergoin M, Hornung H. Results of operativetreatment of severe supracondylar fractures of the elbow in children.J Pediatr Surg 1972;7:676-9.
34. Ramsey RH, Griz J. Immediate open reduction and internal fixationof severely displaced supracondylar fractures of the humerus inchildren. Clin Orthop 1973;90:130-2.
35. Weiland AJ, Meyer S, Tolo VT, Berg HL, Mueller J. Surgicaltreatment of displaced supracondylar fractures of the humerus inchildren: analysis of fifty-two cases followed up for five to fifteenyears. J Bone Joint Surg [Am] 1978;60-A:657-61.
36. Furrer M, Mark G, Ruedi T. Management of displaced supracondy-lar fractures of the humerus in children. Injury 1991;22:259-62.
37. Wilkins KE. The operative management of supracondylar fractures.Orthop Clin North Am 1990;21:269-89.
38. Zuckerberg AL. Perioperative approach to children. Pediatr ClinNorth Am 1994;41:15-29.
39. Barlow IW, Kolay I, Clarke NMP. Displaced supracondylar humeralfractures in children. J Bone Joint Surg [Br] 1997;79-B:Suppl I, 101.
40. Wilkins KE. Fractures and dislocations of the elbow region. In:Rockwood CA, Wilkins KE, King RE, eds. Fractures in children. Vol.3. Philadelphia: JB Lippincott Co, 1984:363-575.
41. McLaughlin HL. Trauma. Philadelphia: WB Saunders Co, 1959.
42. Prietto CA. Supracondylar fractures of the humerus: a comparativestudy of Dunlop's traction versus percutaneous pinning. J Bone JointSurg [Am] 1960;42-A:425-8.
43. Sutton WR, Greene WB, Georgopoulos G, Dameron TB. Displacedsupracondylar humeral fractures in children: a comparison of resultsand costs in patients treated by skeletal traction versus percutaneouspinning. Clin Orthop 1992;278:81-7.
44. Ikram MA. Ulnar nerve palsy: a complication following percutaneousfixation of supracondylar fractures of the humerus in children. Injury1996;27:303-5.
45. Royce RO, Dutkowsky JP, Kasser JR, Rand FR. Neurologiccomplications after K-wire fixation of supracondylar humerus frac-tures in children. J Pediatr Orthop 1991;11:191-4.
46. Herzenberg JE, Koreska J, Carroll NC, et al. Biomechanical testingof pin fixation techniques for pediatric supracondylar elbow fractures.Orthop Trans 1988;12:678-9.
47. Zionts LE, McKellop HA, Hathaway R. Torsional strength of pinconfigurations used to fix supracondylar fractures of the humerus inchildren. J Bone Joint Surg [Am] 1994;76:253-6.
210 L. J. O'HARA, J. W. BARLOW, N. M. P. CLARKE
THE JOURNAL OF BONE AND JOINT SURGERY
![Exchange of papers between Leibniz and Clarke · Leibniz-Clarke papers G. W. Leibniz and Samuel Clarke Clarke 1: 26.xi.1715) ... [i.e. Newton and his followers] allow that there are](https://img.pdfslide.net/doc/110x75/5c100fb309d3f2a8238bfbb4/exchange-of-papers-between-leibniz-and-clarke-leibniz-clarke-papers-g-w-leibniz.jpg)