Embed Size (px)
Citation preview
10/17/2016
1
Classification of congenital lung cysts and malformations
Minnesota Society of Pathologists Fall MeetingOctober 29 2016October 29, 2016
Megan K. Dishop MDMedical Director, Pediatric Anatomic PathologyChildren’s Hospitals and Clinics of MinnesotaMinneapolis-St. Paul, Minnesota, USA
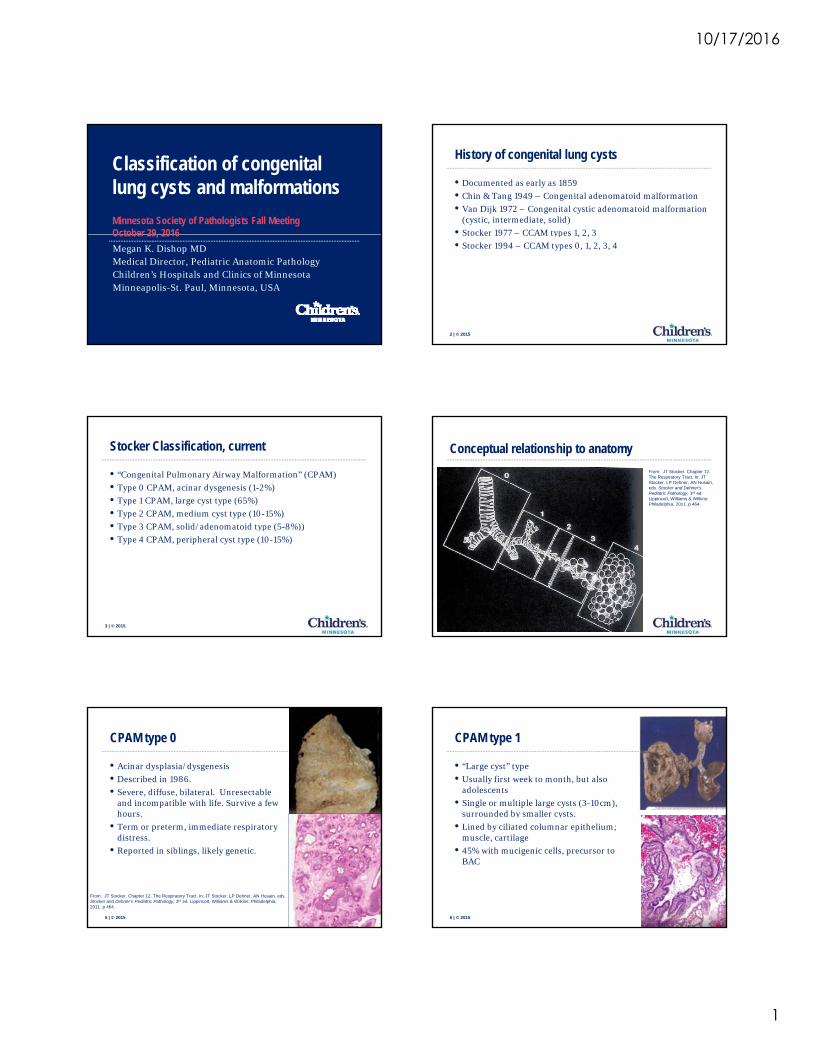
History of congenital lung cysts
• Documented as early as 1859
• Chin & Tang 1949 – Congenital adenomatoid malformation
• Van Dijk 1972 – Congenital cystic adenomatoid malformation (cystic, intermediate, solid)
• Stocker 1977 – CCAM types 1 2 3
2 | © 2015
Stocker 1977 CCAM types 1, 2, 3
• Stocker 1994 – CCAM types 0, 1, 2, 3, 4
Stocker Classification, current
• “Congenital Pulmonary Airway Malformation” (CPAM)
• Type 0 CPAM, acinar dysgenesis (1-2%)
• Type 1 CPAM, large cyst type (65%)
• Type 2 CPAM, medium cyst type (10-15%)
• Type 3 CPAM solid/adenomatoid type (5 8%))
3 | © 2015
• Type 3 CPAM, solid/adenomatoid type (5-8%))
• Type 4 CPAM, peripheral cyst type (10-15%)
Conceptual relationship to anatomy
From: JT Stocker. Chapter 12. The Respiratory Tract. In: JT Stocker, LP Dehner, AN Husain, eds. Stocker and Dehner’s Pediatric Pathology, 3rd ed. Lippincott, Williams & Wilkins: Philadelphia, 2011. p 464.
4 | © 2015
CPAM type 0
• Acinar dysplasia/dysgenesis
• Described in 1986.
• Severe, diffuse, bilateral. Unresectable and incompatible with life. Survive a few hours.
5 | © 2015
• Term or preterm, immediate respiratory distress.
• Reported in siblings, likely genetic.
From: JT Stocker. Chapter 12. The Respiratory Tract. In: JT Stocker, LP Dehner, AN Husain, eds. Stocker and Dehner’s Pediatric Pathology, 3rd ed. Lippincott, Williams & Wilkins: Philadelphia, 2011. p 464.
CPAM type 1
• “Large cyst” type
• Usually first week to month, but also adolescents
• Single or multiple large cysts (3-10cm), surrounded by smaller cysts.
6 | © 2015
y y
• Lined by ciliated columnar epithelium; muscle, cartilage
• 45% with mucigenic cells, precursor to BAC
10/17/2016
2
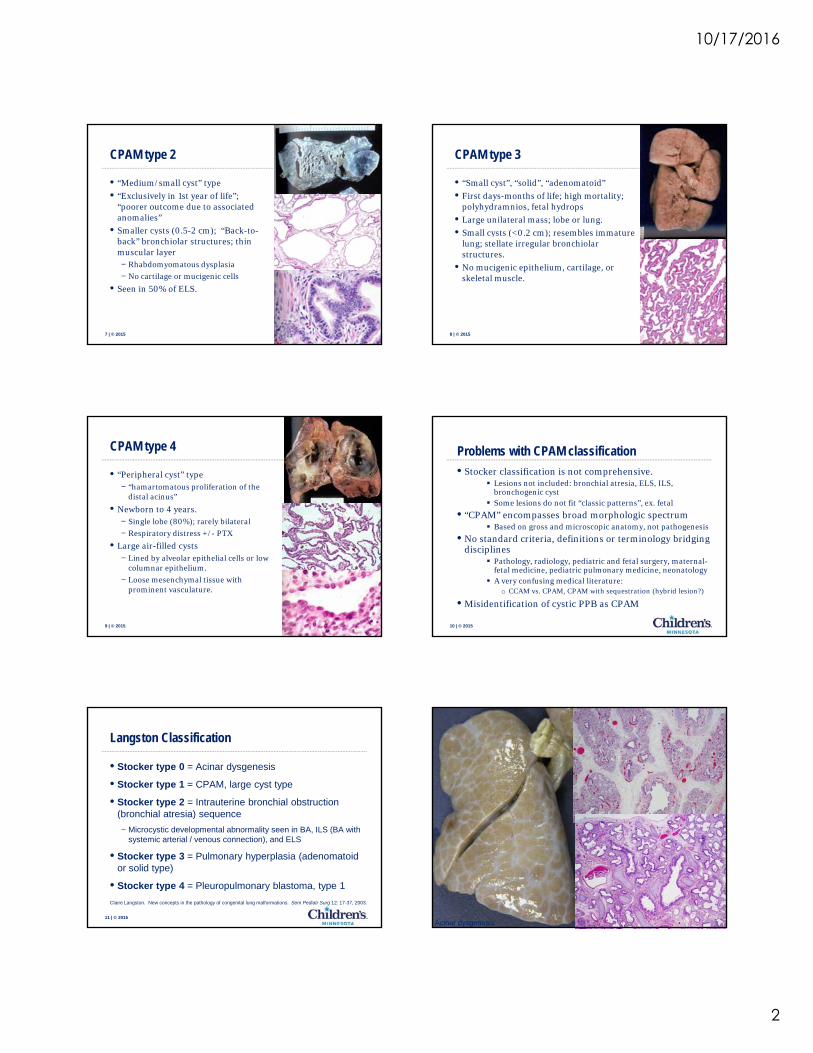
CPAM type 2
• “Medium/small cyst” type
• “Exclusively in 1st year of life”; “poorer outcome due to associated anomalies”
• Smaller cysts (0.5-2 cm); “Back-to-
7 | © 2015
y ( 5 );back” bronchiolar structures; thin muscular layer− Rhabdomyomatous dysplasia
− No cartilage or mucigenic cells
• Seen in 50% of ELS.
CPAM type 3
• “Small cyst”, “solid”, “adenomatoid”
• First days-months of life; high mortality; polyhydramnios, fetal hydrops
• Large unilateral mass; lobe or lung.
• Small cysts (<0 2 cm); resembles immature
8 | © 2015
Small cysts (<0.2 cm); resembles immature lung; stellate irregular bronchiolar structures.
• No mucigenic epithelium, cartilage, or skeletal muscle.
CPAM type 4
• “Peripheral cyst” type− “hamartomatous proliferation of the
distal acinus”
• Newborn to 4 years.− Single lobe (80%); rarely bilateral
9 | © 2015
− Respiratory distress +/- PTX
• Large air-filled cysts− Lined by alveolar epithelial cells or low
columnar epithelium.
− Loose mesenchymal tissue with prominent vasculature.
Problems with CPAM classification
• Stocker classification is not comprehensive. Lesions not included: bronchial atresia, ELS, ILS,
bronchogenic cyst Some lesions do not fit “classic patterns”, ex. fetal
• “CPAM” encompasses broad morphologic spectrum Based on gross and microscopic anatomy not pathogenesis
10 | © 2015
Based on gross and microscopic anatomy, not pathogenesis
• No standard criteria, definitions or terminology bridging disciplines
Pathology, radiology, pediatric and fetal surgery, maternal-fetal medicine, pediatric pulmonary medicine, neonatology
A very confusing medical literature:o CCAM vs. CPAM, CPAM with sequestration (hybrid lesion?)
• Misidentification of cystic PPB as CPAM
Langston Classification
• Stocker type 0 = Acinar dysgenesis
• Stocker type 1 = CPAM, large cyst type
• Stocker type 2 = Intrauterine bronchial obstruction (bronchial atresia) sequence
11 | © 2015
( ) q
− Microcystic developmental abnormality seen in BA, ILS (BA with systemic arterial / venous connection), and ELS
• Stocker type 3 = Pulmonary hyperplasia (adenomatoid or solid type)
• Stocker type 4 = Pleuropulmonary blastoma, type 1
Claire Langston. New concepts in the pathology of congenital lung malformations. Sem Pediatr Surg 12: 17-37, 2003.
12 | © 2015Acinar dysgenesis
10/17/2016
3
CPAM, large cyst typeCPAM, large cyst type4 day old infant girl with cystic lung lesion. Right lower lobectomy.4 day old infant girl with cystic lung lesion. Right lower lobectomy.
14 | © 2015
Bronchial Atresia - the hidden pathology
• Bronchial atresia sequence− Pattern of maldevelopment widely associated with airway
obstruction (bronchial atresia, ILS, ELS)
− Rarely without identifiable airway obstruction
• Common finding in many types of developmental lung lesions− 22/25 lung resections of IUUS identified lesions at Children’s
15 | © 2015
22/25 lung resections of IUUS identified lesions at Children s Hospital Boston assessed for bronchial atresia 14 CPAM, 9/13 assessed with BA 3 CLO, 2/3 with BA 1 ELS with BA 1 ILS (not assessed) 6 CPAM/seq 5/5 assessed with BA
Kunisaki et al. Bronchial atresia: the hidden pathology within a spectrum of prenatally diagnosed lung masses. J Ped Surg 2006; 41:61-65
Segmental bronchial atresiaSegmental bronchial atresia
RLL segmental BA with microcystic maldevelopment8 day old
ExtralobarExtralobar sequestrationsequestration
Left-sided ELS with microcystic maldevelopmentand lymphangiectasisassociated with RLL ILS; prenatal dx, resected at 3 months
BronchopulmonaryBronchopulmonary foregut foregut malformationmalformation
Infradiaphragmatic mass seen by prenatal US, accessory lung with esophageal bronchus
Bronchial Atresia
• Isolated− Segmental or subsegmental− Formerly rarely seen in infancy
Later presentations: incidental x-ray finding, recurrent pneumonia, or dyspnea
− Now common pathology of many IUUS lesions
17 | © 2015
Now common pathology of many IUUS lesions Usually asymptomatic at birth
− Gross pathology Lobar enlargement, sometimes pseudofissures Bulge at hilum sometimes marks atretic bronchus Subhilar mucocele and mucus in regional airways Microcystic parenchymal maldevelopment, hyperinflation
18 | © 2015
BRONCHIAL ATRESIABRONCHIAL ATRESIA
9 month old male infant with lung lesion 9 month old male infant with lung lesion identified on prenatal ultrasound. No identified on prenatal ultrasound. No
respiratory problems at birth; RLL respiratory problems at birth; RLL removed electively at 9 months. removed electively at 9 months.
Lobe weight 74.2 gm. Lobe weight 74.2 gm.
Expected R lung wt 53 gm.Expected R lung wt 53 gm.
10/17/2016
4
19 | © 2015
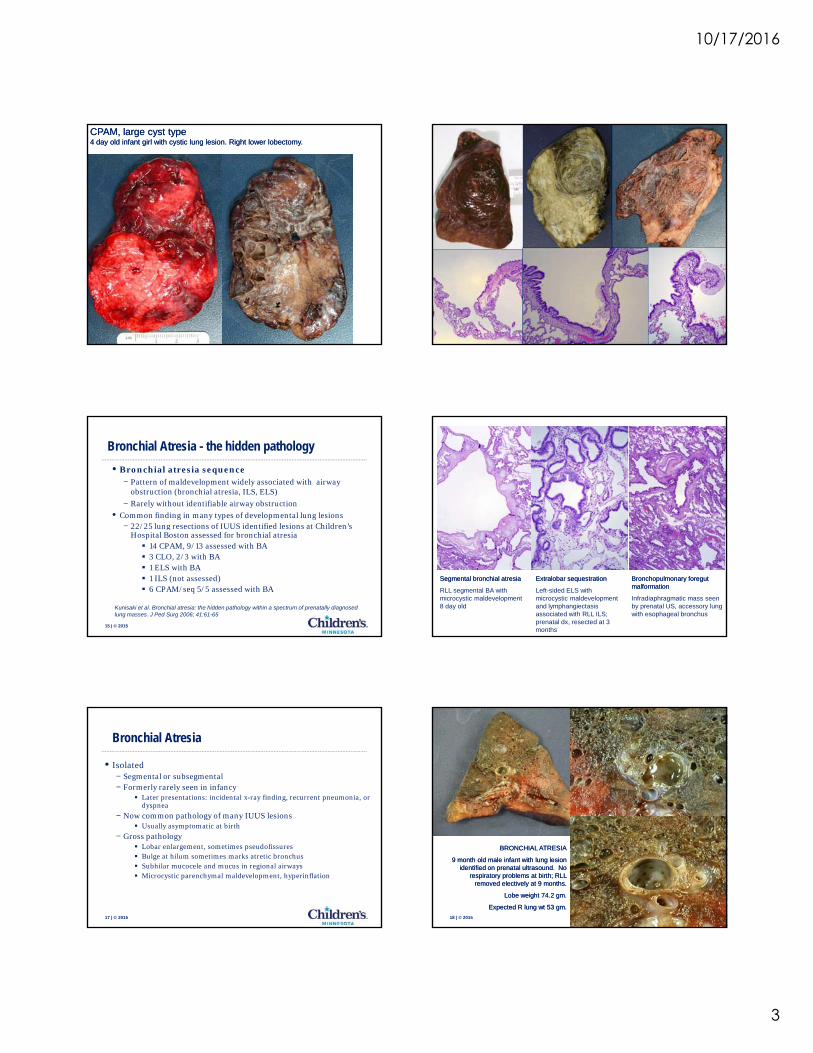
Bronchial Bronchial atresiaatresia
13 year old boy with shortness of breath
while playing trumpet.
21 | © 2015Asymptomatic 10 month old girl with cystic lesion on imaging
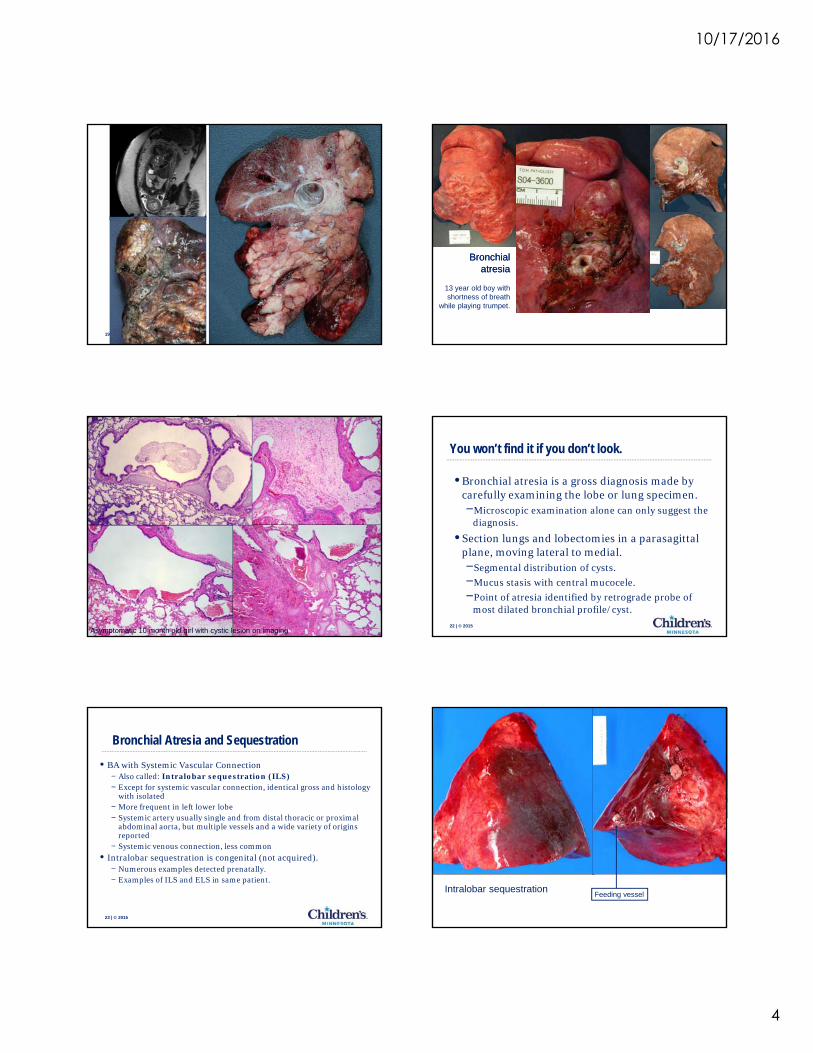
You won’t find it if you don’t look.
• Bronchial atresia is a gross diagnosis made by carefully examining the lobe or lung specimen.−Microscopic examination alone can only suggest the
diagnosis.
22 | © 2015
g
• Section lungs and lobectomies in a parasagittal plane, moving lateral to medial.−Segmental distribution of cysts.
−Mucus stasis with central mucocele.
−Point of atresia identified by retrograde probe of most dilated bronchial profile/cyst.
Bronchial Atresia and Sequestration
• BA with Systemic Vascular Connection− Also called: Intralobar sequestration (ILS)− Except for systemic vascular connection, identical gross and histology
with isolated− More frequent in left lower lobe− Systemic artery usually single and from distal thoracic or proximal
23 | © 2015
Systemic artery usually single and from distal thoracic or proximal abdominal aorta, but multiple vessels and a wide variety of origins reported
− Systemic venous connection, less common• Intralobar sequestration is congenital (not acquired).
− Numerous examples detected prenatally.− Examples of ILS and ELS in same patient.
Feeding vesselIntralobar sequestration
10/17/2016
5
Intralobar sequestration
25 | © 2015
Intralobar sequestration
26 | © 2015
27 | © 2015
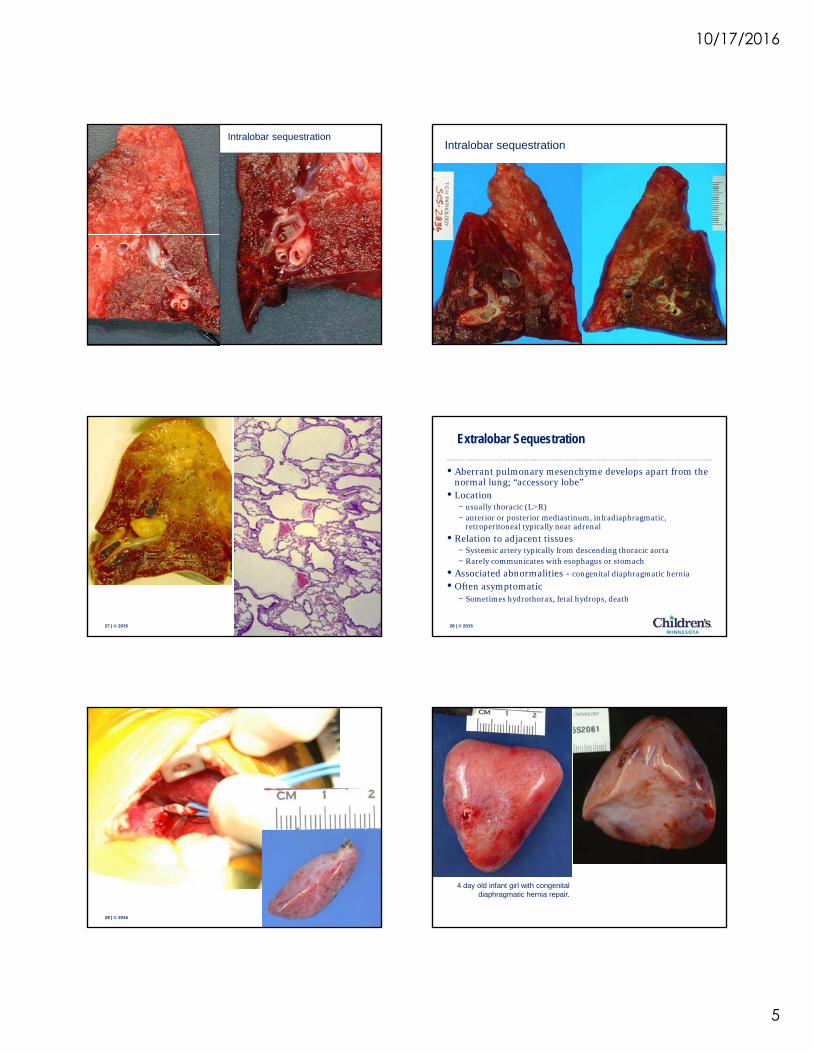
Extralobar Sequestration
• Aberrant pulmonary mesenchyme develops apart from the normal lung; “accessory lobe”
• Location− usually thoracic (L>R)− anterior or posterior mediastinum, infradiaphragmatic,
retroperitoneal typically near adrenal
28 | © 2015
retroperitoneal typically near adrenal
• Relation to adjacent tissues− Systemic artery typically from descending thoracic aorta− Rarely communicates with esophagus or stomach
• Associated abnormalities - congenital diaphragmatic hernia
• Often asymptomatic− Sometimes hydrothorax, fetal hydrops, death
29 | © 2015
4 day old infant girl with congenital diaphragmatic hernia repair.
10/17/2016
6
31 | © 2015
Complex Bronchopulmonary Foregut Malformation
32 | © 2015
33 | © 2015
Bronchogenic CystBronchogenic Cyst
34 | © 2015
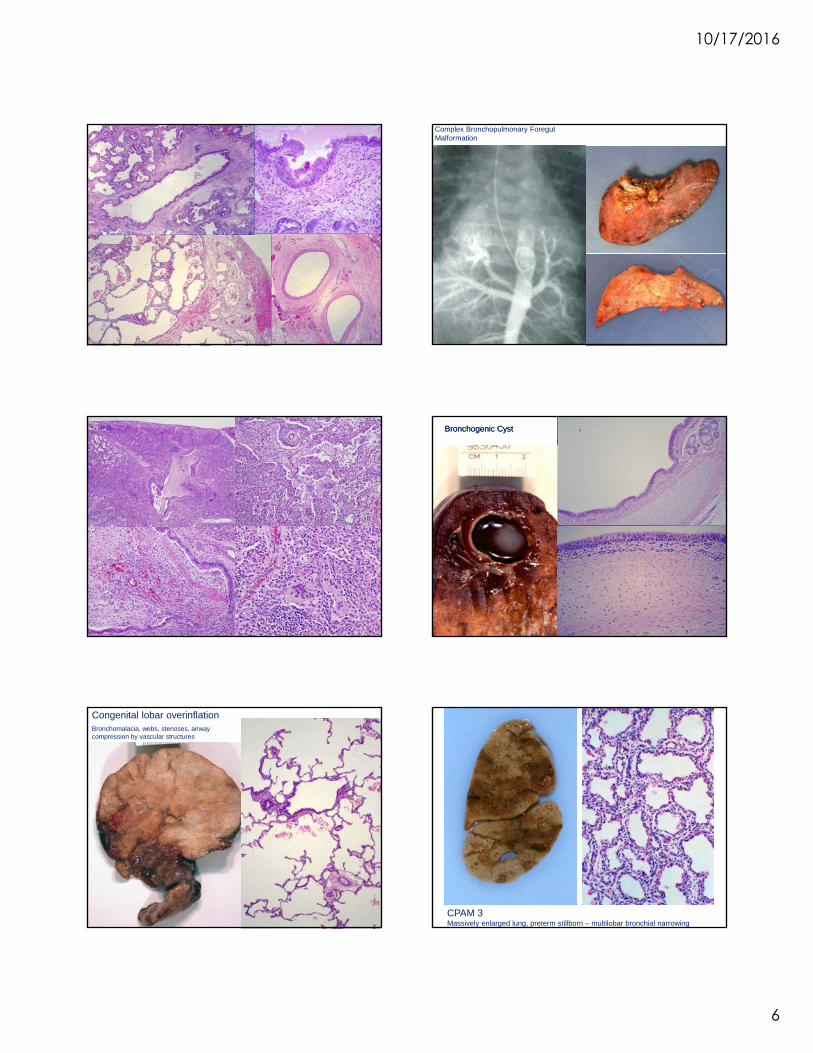
Congenital lobar overinflationBronchomalacia, webs, stenoses, airway compression by vascular structures
35 | © 2015CPAM 3Massively enlarged lung, preterm stillborn – multilobar bronchial narrowing
10/17/2016
7
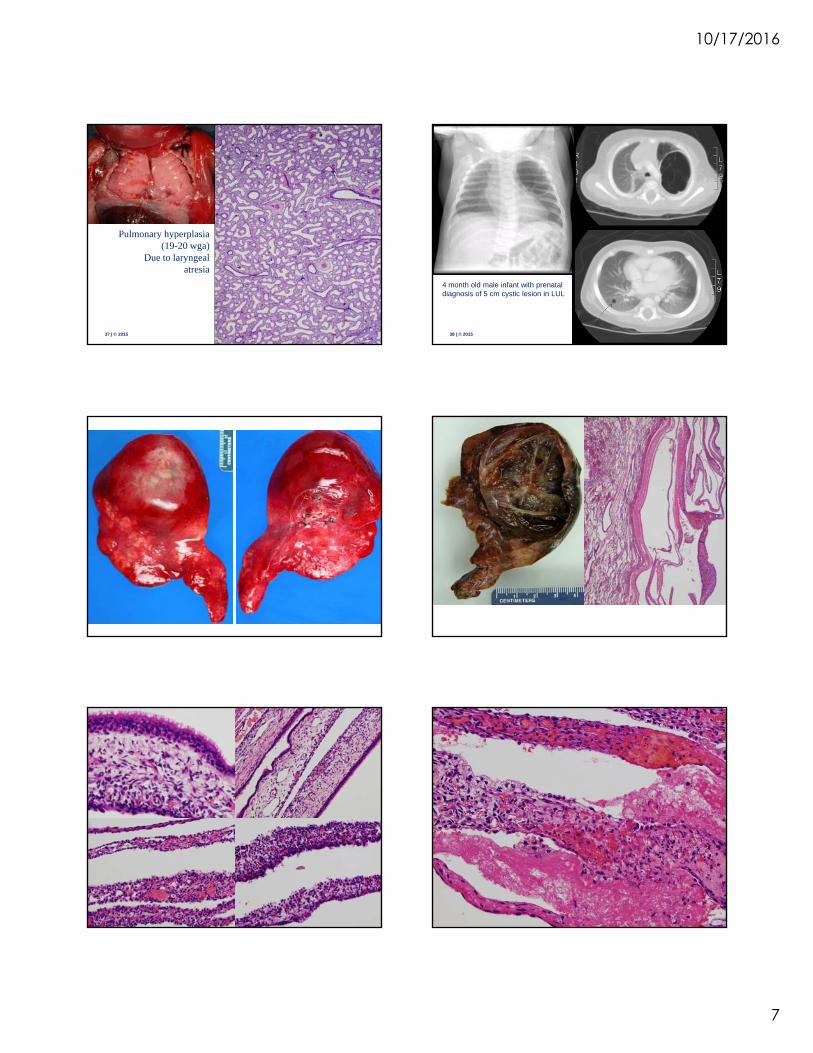
Pulmonary hyperplasia
37 | © 2015
Pulmonary hyperplasia (19-20 wga)
Due to laryngeal atresia
38 | © 2015
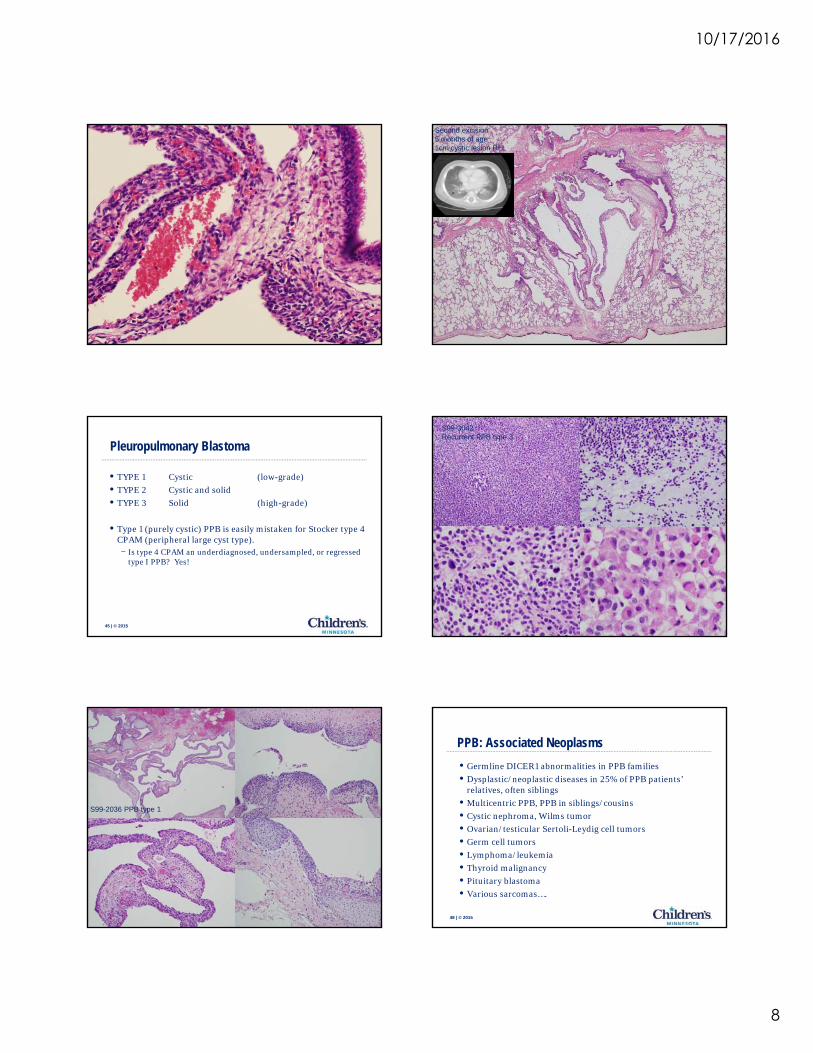
4 month old male infant with prenatal diagnosis of 5 cm cystic lesion in LUL
41 | © 2015 42 | © 2015
10/17/2016
8
43 | © 2015
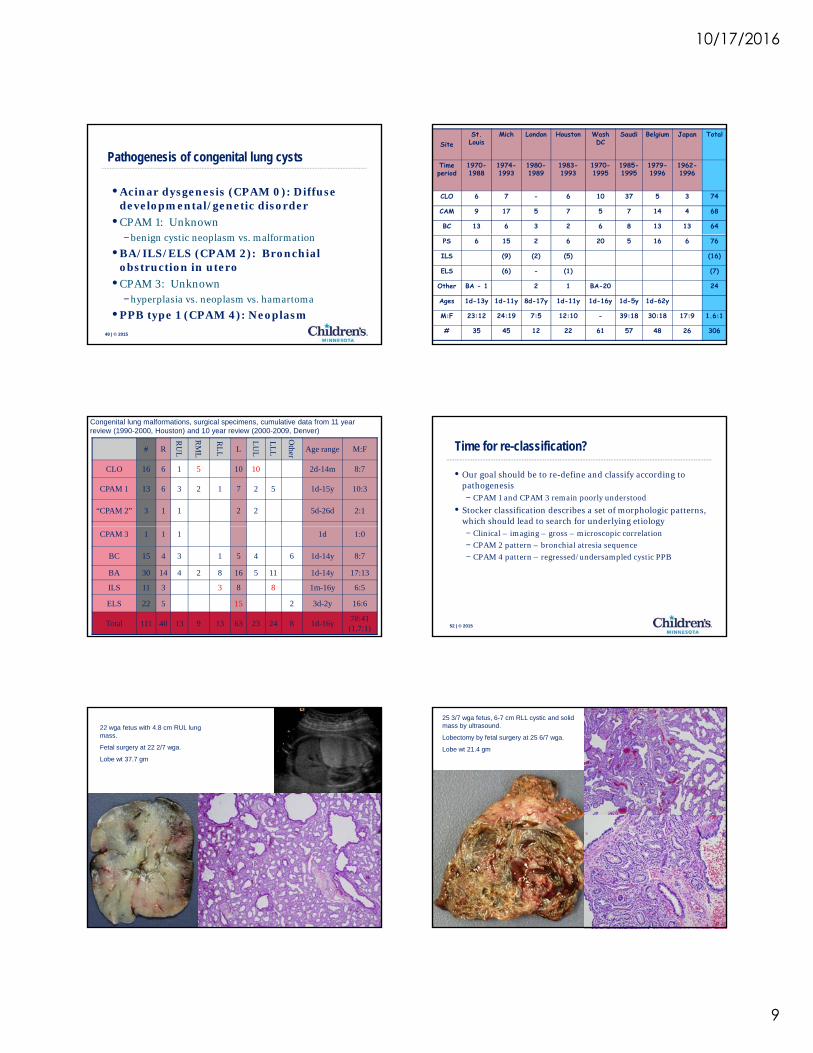
Second excision5 months of age 1cm cystic lesion RLL
44 | © 2015
Pleuropulmonary Blastoma
• TYPE 1 Cystic (low-grade)
• TYPE 2 Cystic and solid
• TYPE 3 Solid (high-grade)
T ( l ti ) PPB i il i t k f St k t
45 | © 2015
• Type 1 (purely cystic) PPB is easily mistaken for Stocker type 4 CPAM (peripheral large cyst type).− Is type 4 CPAM an underdiagnosed, undersampled, or regressed
type I PPB? Yes!
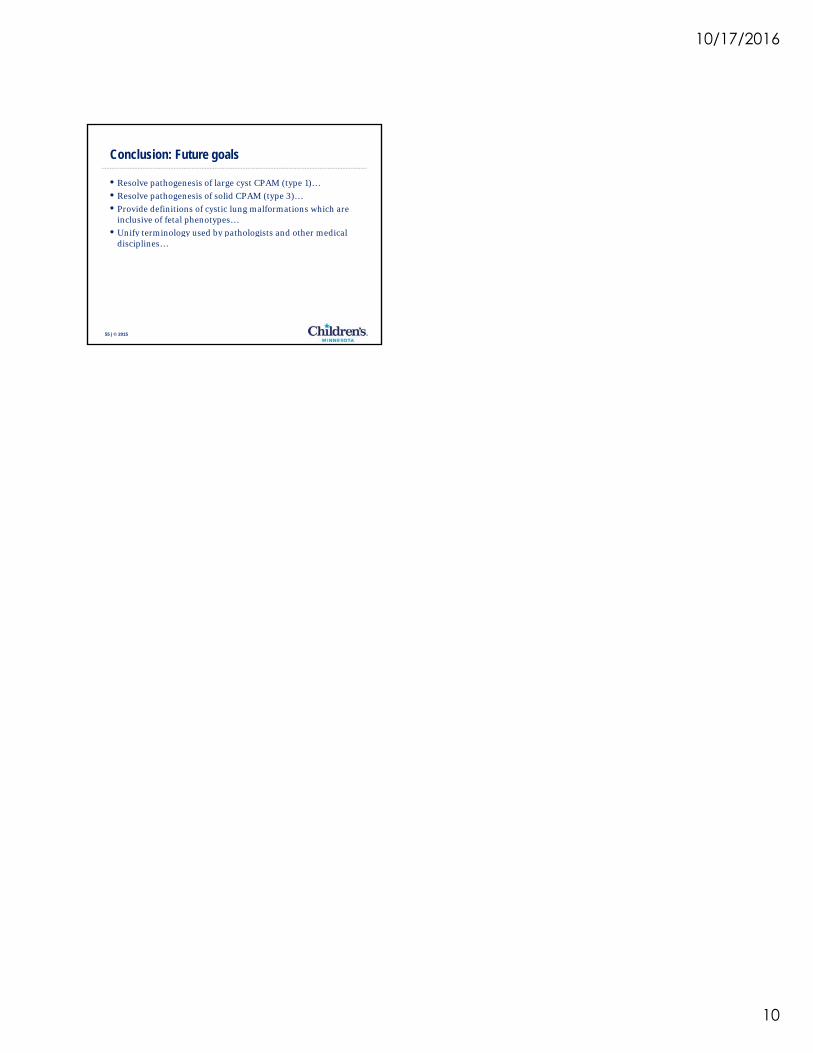
S99-3042Recurrent PPB type 3
46 | © 2015
S99-2036 PPB type 1
47 | © 2015
PPB: Associated Neoplasms
• Germline DICER1 abnormalities in PPB families
• Dysplastic/neoplastic diseases in 25% of PPB patients’ relatives, often siblings
• Multicentric PPB, PPB in siblings/cousins
• Cystic nephroma Wilms tumor
48 | © 2015
Cystic nephroma, Wilms tumor
• Ovarian/testicular Sertoli-Leydig cell tumors
• Germ cell tumors
• Lymphoma/leukemia
• Thyroid malignancy
• Pituitary blastoma
• Various sarcomas….
10/17/2016
9
Pathogenesis of congenital lung cysts
• Acinar dysgenesis (CPAM 0): Diffuse developmental/genetic disorder
• CPAM 1: Unknownb i ti l lf ti
49 | © 2015
−benign cystic neoplasm vs. malformation
• BA/ILS/ELS (CPAM 2): Bronchial obstruction in utero
• CPAM 3: Unknown−hyperplasia vs. neoplasm vs. hamartoma
• PPB type 1 (CPAM 4): Neoplasm
SiteSt. Louis
Mich London Houston Wash DC
Saudi Belgium Japan Total
Time period
1970-1988
1974-1993
1980-1989
1983-1993
1970-1995
1985-1995
1979-1996
1962-1996
CLO 6 7 - 6 10 37 5 3 74
CAM 9 17 5 7 5 7 14 4 68
BC 13 6 3 2 6 8 13 13 64
PS 6 15 2 6 20 5 16 6 76
ILS (9) (2) (5) (16)
ELS (6) - (1) (7)
Other BA - 1 2 1 BA-20 24
Ages 1d-13y 1d-11y 8d-17y 1d-11y 1d-16y 1d-5y 1d-62y
M:F 23:12 24:19 7:5 12:10 - 39:18 30:18 17:9 1.6:1
# 35 45 12 22 61 57 48 26 306
# R
RU
L
RM
L
RL
L L
LU
L
LL
L
Other Age range M:F
CLO 16 6 1 5 10 10 2d-14m 8:7
CPAM 1 13 6 3 2 1 7 2 5 1d-15y 10:3
“CPAM 2” 3 1 1 2 2 5d-26d 2:1
Congenital lung malformations, surgical specimens, cumulative data from 11 year review (1990-2000, Houston) and 10 year review (2000-2009, Denver)
51 | © 2015
CPAM 3 1 1 1 1d 1:0
BC 15 4 3 1 5 4 6 1d-14y 8:7
BA 30 14 4 2 8 16 5 11 1d-14y 17:13
ILS 11 3 3 8 8 1m-16y 6:5
ELS 22 5 15 2 3d-2y 16:6
Total 111 40 13 9 13 63 23 24 8 1d-16y70:41 (1.7:1)
Time for re-classification?
• Our goal should be to re-define and classify according to pathogenesis− CPAM 1 and CPAM 3 remain poorly understood
• Stocker classification describes a set of morphologic patterns, which should lead to search for underlying etiology
52 | © 2015
− Clinical – imaging – gross – microscopic correlation
− CPAM 2 pattern – bronchial atresia sequence
− CPAM 4 pattern – regressed/undersampled cystic PPB
22 wga fetus with 4.8 cm RUL lung mass.
Fetal surgery at 22 2/7 wga.
Lobe wt 37.7 gm
53 | © 2015
25 3/7 wga fetus, 6-7 cm RLL cystic and solid mass by ultrasound.
Lobectomy by fetal surgery at 25 6/7 wga.
Lobe wt 21.4 gm
54 | © 2015
10/17/2016
10
Conclusion: Future goals
• Resolve pathogenesis of large cyst CPAM (type 1)…
• Resolve pathogenesis of solid CPAM (type 3)…
• Provide definitions of cystic lung malformations which are inclusive of fetal phenotypes…
• Unify terminology used by pathologists and other medical
55 | © 2015
Unify terminology used by pathologists and other medical disciplines…