-
8/14/2019 Congenital Cardiac Malformations in Relation to
Central
1/7
Congenital cardiac malformationin relation to central venous
accesChristine Thompso
AbstractD u r in g the third and seventh weeks of gestation,
teratogenic exposure maylead to fetal abnormality such as
congenital heart defects or intrauterinedeath. Congenital heart
defects are present from birth, but may appear atany tiine, or only
revealed postniortetn. Often defects are present by degree.Some
defects are life-threatening, while other, less severe conditions,
mayhave tttininial physiological iinpact. Left superior vena cava
exists in earlyembryonic deve lopment , but the vessel degenerates
as the cardiovascularsystem matu res . When not associated with
other malformations, an incidenceof persistent left-sided superior
vena cava (PLSVC) has no clinical signsor sym ptoms . However, tt
may not be as innocuous as it appears due toits association with
the cyanotic defect, tetralogy of Fallot (TOF). Usinga case history
as an illustration it can be shown that all cases of defect
orchromosomal suspicion should be d o c u me n te d as there may be
implicationsfor future interventions.Key words: Cardiovascular
system and disorders Heart disorders
A 46-year-o ld man (KW) of unusual appearanceand manner, with a
previous medical his toryof non-in sulin dep ende nce diabetes and
newlydiagnosed lyniphoma was referred for insertionof a tunnelled
central venous line for the administrationof chemotherapy . There
was significant maternal historyof insulin dependence diabetes and
epilepsy and his fatlierdescribed mild cyanosis when extremely cold
and reported areluctance to exercise in ch i ldhood .ProcedureThe
preferred right-sided approach via the internal jugularvein was
attempted. Under ultrasound visualization the veinappeared to be
small and, although it could be cannulated,venospasm appeared to
occur and the guide wire could notbe advanced. The left internal
jugular vein appeared largeand compressible and therefore a
left-sided approach wasa t tempted . The vessel was cannulated, the
guide wire anddilator passed easily, there were no
electrocardiograph changesan d tbe catheter flinctioned. A
post-procedural chest X-rayshowed the catheter coursing along the
left heart bonier,initially suggesting misplacement; however, the
patient wasasymptoniatic . A contrast injection study confirmed
the
Ciir istint ' Tho mp son , (. l linicjl N iirsi '
SpetKihst.Tunellcd ( 'entr . i l( '.itlietcr ServKC, Cianiuv t'l
(ifntT.il Hospit.il, (il.isj;ii\vAccepted for piihlicalion: January
2006
catheter passing through a persistent left-sided supevena cava
(PLSVC^), thr ou gh the coronary sinns and wth e tip in the upper
right atrium. An abnormal, narrowright superior vena cava (SVC) and
a sliglitiy constricpulmonary artery was detected. Later review of
his mednotes revealed childhood surgery for repair of hypospadiasno
evidence of chmmosomal s tudies . Tbe catheter remaiin position for
5 months and the patient completed his couof chemotherapy without
incident.The patient 's unusual appearance and manner suggesthere
may be genetic or th romosoina l nnp i ica t ions , buview of his
diagnosis, a decision was made to investigatefurther until his
prognosis could be d e te rmin e d .
RW was found to sufl^er from a non-cyanotic congenheart defect
(C"HD}. whieh is one of over 35 doeunienhuman congenital cardiac
malformations. These recognilesions also have many variations. For
example, RW's particcondition (PLSVC) can he complicated by
unroofing ofcoronary sinus wherein cyanosis would be present; this
be discussed later in the text (I'orth, 2002). IncidencesCHI), also
referred to as congenital cardiac malformatare found in equal
measure in every continent. The mcommon congenital defects are
ventricular septal det(VSDs) 2()-25%, atria! septal defects (ASDs)
8-13 % , and p aductus arteriosus (I'DAs) 6-11% (Hanied and Maher,
20Although these lesions will be referred to in tbe course
ofarticle, the author will concentrate specifically on
PLSVCacyanotic malformation which has an incidence of 0.30of the
population and is the most coninion congenital venanomaly of the
SVC system (Leibowitz et al, 1992; Bartramal, 1997), and the
cyanotic defect with which it has a 15-2association, tetralogy of
Fallot (TOF) (Soto et al. 1992;Waet al, 2003; lirzezinski et al,
2005).
What Is a congenital heart defect?A CHI.) can be defined as the
structural, funetionalpositional defect of the heart occurring
either in isolation oa combination ofseveral lesions collectively
Defects areprefrom birth, but may appear at any time after birth,
or noall, often o nly bein g revealed po stm orte m (Lilly, 1998).
Sodefects are life-threatening and require iniiiiediate
surgcorrection or palliation, while other, less severe conditimay
have niininial physiological impact (Lilly, 1998).
C H D s can be broadly classified into two categories: thcausing
little or no cyanosis, classed as acyanotic. and thc-ausing
cyanosis (Lilly, 1998; Porth, 2002).
Eight coniinon lesions account for 85%) of all cw o r ld w id e
and are listed in 'liihlf / .The remain ing 1
-
8/14/2019 Congenital Cardiac Malformations in Relation to
Central
2/7
CARDIAC NURSINGaccounts for a variety rare detects, inckidiiig
PLSVC^ (Lilly,199S; Porth, 2002).Cyanotic and acyanotic defectsIn
the presence of CHDs, pressure gradients between chambersmay be
created which lead to haemodynamic compromise.This effect is
produced by alterations in pulmonary bloodflow and the abnormal
shunting (diversion) of blood from onesystem to another through
aberrant openings between bothsides of the heart. l.,eft-to-right
shunts are mainly acyanoticconditions and push blood from tbe
arterial circulation intotbe venous circulation resulting in
oxygenated blood beingrecycled through the right heart, increasing
the load andleading to enlargement of the right heart. Conversely,
right-to-left shunts produce cyanosis as a result of
deoxygenatedblood being forced into tbe systemic circulation via
the leftheart as in TOF (Forth. 20(12).Causes of CHD( ; H 1 )
occurs with equal frequency in males and femalesand IS the cause ot
S0% ot deaths withm the first year oflife (Hamed and Maher,
2(10(1). Approxima tely 13% of thoseborn with a cardiac detect will
bave another non-cardiac,chromosomal ahnormality (Forth, 2002).The
prevalence ot'maltorniation among the siblings and near relatives
of sucha cbild IS sigiiiticantly higher [ban in the general
population(Hamed and Maher, 2000).
The crticial phase tor tetal heart development is between
thethird and seventh week of gestation (dittenberger-De Grootet al,
2005). During that tune, teratogemc (a tactor increasingthe
incidence of maltoniKition development) exposure maylead to tetal
abnormality such as C^Hl), or intrauterine death ifexposure is
prolonged (Lilly, I 99K; Hamed and Maher,200(l).The involvement of
a heredity tactor associated with theselesions is widely
acknowledged within the literature, withmany sutierers having a
genetic predisposition to disease.Embryonic mesoderm is the source
of the cardiogenic place,giving rise to the future myocardium, and
endocardium,which lines the heart. Genetic cascades are triggered
thatgive rise to interactions between competing chemicalsignals 111
tbe primitive beart and several mutated genes
Table 1. Most commonMalformationVentricular septal detectPatent
ductus arteriosusAtrial septal defectPulmonary valve stenosisAortic
valve stenosisCoarctation of tine aortaTetralogy of
FallotTransposition ot great arteries
lesionsCyanotlc/acyanoticAcyanoticAcyanoticAcyanoticAcyanoticAcyanoticCyanoticCyanoticCyanotic
Adapted from: Lil ly (1998); Porth (2002)
are thought responsible for numerous C^HHs (Bruneau,2003;
Ciittenberger-De Groot et al, 2005). Botb intrinsictranscription
factors that are required for induction of cardiacdifferentiation,
in particular the family NKX2-5, which arerecessive genes, and theT
-box transcription factor TBX5 areimplicated in the development ot
a wide variety of CHUssucb as ASD,VSD, Ebsteins anomaly of the
tricuspid valve,aortic valve stenosis atrioventricular (AV) block,
and TOF.Further, as ditlerent areas ot the developing lieart are
moresensitive to the effect of these agents it is now possibleto
predict at what stage of development the CHI) wasestablished, as
shown in Tahlc 2 (Bruneau, 2003).
Although no one specific cause of all t\'pes of congenitalheart
detects has yet been identified, the currently prevailingnotion,
running in tandem with the above, is that theoccurrence ot a ("HI)
is more likely to be the result of agenetic and environmental
interaction rather than that ot asingle chromosomal abnormality. A
triad of predisposition,vulnerability and teratogemc agents may all
be necessary toproduce sucb detects (Lilly. 1998; Hamed and Maher,
2000;Porth, 2002).There aremany risk factors tor CHI), and theseare
ldentitied in 'Ihhlcs J and4.
In addition to the above, the relevance of lowsocioeconomic
status reflecting maternal nutrition and theissue of matrilineal
transmission have also been recognizedas significant factors m the
development of CHD (Hamedand Maher, 2(.)00).
Table 2. Gestatlonal age atOestational aee (days) 15Events
Heart
differentiates
Some of t t ie Not knownCHD occuring
which a congenital heart defect2 0Heart tubeforms.Heart
beats
Cardia bifida,Laterality defect
28Early chambersform andloop to right
Hypoplastic5 L and R tieart
(CHD) may32Chamberb rma t ion .septates
defectivevalves. AVcanal defects.tetraiogyof Fallot
ASD = Atrial septal defect: AV - Aortic valve; DORV = Double
outlet right ventricle: VSD = Ventricuiar septai defect
arise50 +Valves form.Septation occurs.conductionsystems form
,connects togreat vesselsASD. VSD,DORV.tetralogycf
Faliot.conduction defects
Source: Bruneau (2003)
-
8/14/2019 Congenital Cardiac Malformations in Relation to
Central
3/7
Table 3. Congenital heart defect with
chromosomalabnormalitiesChromosomal Name of syndromeabnormality
Type of defect resulting211813XO
trisomytrisomytrisomysyndrome
Down--Turner
s syndrome
"s syndrome
V SDVSD. PDA. DORVDextocardia. VSD,Coarctat ion of the
DORV = Double outlet right ventride: PDA = Patent ductus
arteriosus; VSDAdapted from: L il ly (1998); Hamed and
P D Aaorta, stenosis= Ventricuiar septal defect
Maher (2000); Portf i (2002)
Normal embryonic cardiac development111 rhe limiian emb ryo, the
meso dcrma l germ layer givesrise tothe entire cardiovascular
system. Th e he art developstrom two simple epithelial tubes which
tlise to form a singlechambered heart.Twenty-three days tollowing
conception the single, simpleepithelial heart tube lies within
theembryo's pericardialcavity and is layered with cells which are
known as thecardiac mantle, which eventually give rise to the
epicardiumand myocardium. As development progresses, the
crania!one-third ot the tube dilates toform the aortic sac
whichwill give rise to the aortic arches. The caudal one-thirdalso
dilates to form the early embryonic ventricle aroundthe 2Sth day.
The remaining mid -portion forms the bulbuscordis, which has three
distinct areas of developmen t: Tlie proximal on e-thi rd gives
rise ro the bocly of the riglitventricle The distal section, known
as the trunciis arteriosus,develops into the aortic root and
ascending aorta The rem aining mid portion, the conus cordis,
connects theprimitive right ventricle to the truncus
arteriosus.
The conus cordis partitions to torm the outflow tracts otthe
right and left ventricles.l)-looping (where the heart tube grows
longer and bendsto tbe right) is responsible tor die initial
positioning of tbeprimitive ventricle.Distal to tbe primitive rigbt
ventricle !s an area known asthe conotriincai region
(maldevelopment of this area leadsto TOF) containing tbe conus
cordis and truncus arteriosus.
'fbe conotruncal region and tbe primitive rigbt ventricle
collectively known as tbe bulbus cordis. As growth continthe
conotruncal region moves centrally with torsion twisting, giving
rise to the anatomical curve oi the aoand the pulmonary artery and
aligns the heart in its normposition. By the 56th day, valves and
septation has occurthe conduction system is forming and it is
connected to great vessels {H-^iirc /)(Larson, l'/JS; Lilly, 1998;
Porth, Gittenb erger-Ue Groot et al, 2005).Persistent left-sided
superior vena cavaIbe worldwide incKlence of PLSVCJ is
approximately 0.(Leibowitz et al, 1992; Bartram et al, 1997). In
those with ocongenital cardiac defects the incidence is
considerably higbetween 3% and H*34% and is tbe most commo n anomof
systemic venous return {Leibowitz et al, 1992; 13artram e1997).
Diagnosis is often incidental and in approximately 2of cases it is
associated with TOF and other cardiac as welnon-cardiac
malformations (Bartram et al, 1997).
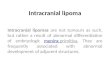
The basis of the I'LSVC ispoorly understood. It resfrom in utero
failure of the left cardinal vein to develop acan take various
forms. In most cases it results in abilatSVC, often with a venous
bridge joining the two, or tmay becompletely separate from eacb
other (Soto e1992). Occasionally the right SVC. is absent and the
venreturn trom the upper body enters the coronary sinus to right
atrium (vvww.pediheart.org). PLSVC draining into right atritiin via
an enlarged coronary sinus, and rarely wan absent rigbt SV C, will
rarely produc e any pbysiologderangement asvenous blood continues
to return toright atrium and, therefore, the condition
requirestreatment, as in the case of the patient l^W (Leibowitz
et1992; Gcrber and Kuzuzo, 2002) {Fi^^mr 2) .More infrequently, a
FLSVC] can be connected to roof of tbe lett atriinn instead of the
coronary sinus whthen continues as an inter-artrial conduit that
ailows venreturn to the left atrium. This is known as 'unroo fing'
andclinically signiticant (Sabiston and Spencer. 1995). A
I'LSdraining into the lett atrium is associated with anAwhich
produces right-to-left shunting and haemodynamcompromise resulting
incyanosis which isusually mild peripheral, and is the main
clinical sign (Bartram et al. 19
Table 4. Environmental factors significantly
increasingmalformationMaternal infectionsMaternal drugsMaternal
diseaseOther maternalfactors
ASD = Atrial septal defect:
Rubella, mum ps, intrauterine infectionAnti convulsants
(phenytoin), vitamin D,anti-depressantsDiabetes, systemic lupus
erythematosis, hypertension .phenylketonuria,
phenylalanaemiaMaternal agePre-natal alcohol consum ptionSmoking
accompanied by low birth weightExposure to X-raysExposure to
toxins
VSD = Ventricular septal delect
incidence of cardiovascular
Pulmonary stenosis, VSD, ASD,endocardial fibroelastosisAortic
stenosisTransposition of greatarteries, congenital heart
blockChromosomal defects (down s syndrome}Fetal alcohoi
syndrome
Adapted from; Lil ly (1998); Hamed and Maher (2000); Porth
(200
-
8/14/2019 Congenital Cardiac Malformations in Relation to
Central
4/7
CARDIAC NURSINGHsu et .tl. 200 4). Associated cardiac ar rhyt
hini .i, p.irticularlyatrioveiitricula r block, com plet e heart
block and ventricularfibrillation, which can instigate atrial
fibrillation, have beenreported and these may be treated by
ablation techniques(I)har ctal. 1998; Sarodia and StoUer, 2
-
8/14/2019 Congenital Cardiac Malformations in Relation to
Central
5/7
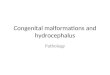
l-'ijiurc 2: Norma ldei'clopment of tin-
stiperiar veua cuni ontill- lij'l lij^iirc ioiiijuin'd
ii'irli pi-rshreni left-sided superior veiui
cai'ii uti the right.IVC-Inferior vetui
caim; Sl'C=Siipcriorvetm Ciii'a.AdiipU'd
from Bergman vi al(2004).
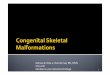
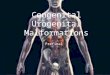
Figure 3: Anatomicalahtiormatities in
tetralogy ofFatlot onleft compared witit
normal heart on right.Adapted front Lilly
(1998).
SubcicMsn vein
atnum
IVC -
jugiiat veins ^^ ^
1 /ghlvemncie):::z3
, Left auium
AF Lefl
Narrowsd SVC
Cwonaiy anus -
- Len SVC
Diirini; fxt-rcisc. increased cardiac output and
decreasedsystemic arcerial resistance result in an increase in the
degreeof right-to-le tt sh unting. Although etfective cardiac outpu
t ismaintained, right-to-lett shunting produces a rapid decreasein
systemic arterial oxygen saturation, resulting in dyspnoci(LiDy,
1998; CTSNet, 2000; Porth, 2002; Sierra ct al, 2001).Sufferers
often assume a squatting position which results in .inincrease in
systemic arteruil resistance caused by compressionof tbe iiKijor
arterial circulation to thelower extremities.This increase in
peripheral resistance reduces rig!it-to-lettshunting and increases
pulnionar^' blood flow, which improvessystemic arterial oxygen
saturation. In mtaiits, tetralot^'speUs (self-limiting spells of
cyanosis) m.iy result from cryingand defecation as both actions
increase pulmonary vascularresistance, increasing right-to-left
shunting and decreasingpulmo nary blood flo w (Portb. 2002; Sierra
et al, 2001).
Treatment is via reparative surgery to close tbe VSl),and the
right-sided obstruction (infundibular stenosis) iscorrected by
remowil of tbe muscle obstructing the flow.
Tbe pulmonary vaKe may be widened or repLiceJ to furrelieve
obstruction and the aortic ontflow may reqrepositioning (Lilly.
1998; Sierra et al, 2001).Diagnosis of cardiac iesionsTil ere is no
treatment available wbicli will altercourse of cardiac malformation
mutero, although tbare many options for prenatal testing including
genamniocentesis, as illustrated in Tahk 5 (C'.iarleglio e2003;
Bhat and Sahn.2004).
Kegardless of the large number of congenital hmalformations,
tbere are a limited number of physiologdisorders caused by th em.
These lesions usually preseninfancy as cyanosis, heart tailure,
heart murmur, circulashock, tetralogy spells, stridor, respiratory
tract infections failure to tbrive (Lilly, 1998; Sierra etal, 2001
; Porth. 20Gittenberger-l.)e Groot et al, 2005).The investigative
tools that aa' available for diagnosis incl
Chest radiography: can determine cardiac size, contours,
vasculature, beart chambers and tbe aortic arcb Electrocardiogram:
can indicate haemodynamic stand severity of the detect through
identifying tracsuggestive of particular defects.
Echoca rdiograpb : using Uop pler technology', this
evaluhaemodynamic disturbances caused by pressure ditlerenacross
the aortic and pulmonary valves, detect vetficieiicy and shunt
flows and as .i non-invasive procedit has become a very powertiil
tool tor diagnosis of C(Ciarleglio et al, 2003; Bhat and Salm,
2l)O4).ConciusionTbe reported case illustrates tb.ir t!ie presence
of a PLSVshould be considered wben cannulation of tbe cen
AortaPulmonary artet7
SVC
Rightatrium atrium
Leftventricle
Right ventricleTetralogy of Fallot Normal heart
-
8/14/2019 Congenital Cardiac Malformations in Relation to
Central
6/7
to be difficult or results in wbatto be malposition. When this
occurs it is advisable
a contrast study to confirm malpositioning,or further
nialformation.Incidence of PLSVC should be documented as it may
have
for future interventions requiring access toor pulmonary artery
or techniques thatuse of the cardiac veins overlaying tbe left
ventricle,
or percutaneous coronary arteryIn order to minimize tbe effects
of the right-to-left shunt,
be placed in the Trendelenburg positionand should bave
in view ofIn the presence of maternal and other risk factors,
e.g.
oror chromosomal ibnormality,is an increased likelihood
ofC^iHD.Tlierefbre, tbere is a
for genetic counsellint; and echocardiographtbe severity of the
lesion. Diagnostic techniquesbe applied early enougb in pregnancy
for post
as termination to be considered. uH
r a i i iU Vin I 'n iagh S.L mn f j C, H incs M.Bcm ky AS,V;in
I' ra agh R (I W7)Absent right superior vena rava in visLcmatrial
sitiis solitiis, .Hui / (^iiriliol80(2): 175-W I'irru.il
Hospii.illlhi'.imtrtl liuiychp.wJi.iof Htmum AiiaUviiic
liiriatioii: Ojnis 11 : Cardiovafnilar iyitem. Anatomy Atlases.h t
t p : / / w v v w , a n a t o n i y , i t L i s e s . o r g / A n a
t o m i c V a r i a n t s /C ^ a r d i o v a s f u la r /Dire itory
/niR -cton liyA lphj bL't. sliti til (last acccs.sed 17 February
2l)(lfi)1)J (21104) Latest advances and topics in frtal
echocardiography.Cinr Opiii Cardioi 19(2): V7-1II3l!(i (2(Hl3)The
developing heart and t oniienit.il hc.irt d etects: a makeor break
iitiiation. C7i>i Ct-m-t 63: 252- f i !
M, Keller R, Cr ichn ik KH Swaminathan M (2(lllfi) Persistent
leftsuperior vena eava in a patient with a history of tetralog\' of
Fallot. .^iivithAualg\m{5): I26')-7IILJ. ISennett RL . Williamson
J, Mand ellJ B, Marks JH (2(X13) GeneticCouricellini; throughout
the L if e C y i l e J Clin Imv.ft 112: 12S1MSS (1974) Tetralogy-
of Fallot ni the elderly. ('Hii C.anliol7(8): 453-6T S N et
(2110(1) Tetralo gy ot" Fa l lo t . CTSNe t . St Lonis.
wwvv.ctsnet.org/doc/4')7f> (last accessed 23 February 200(,)P.
Kautinan H. Doertl er M.lXidic !' (I')9H) Unusual course of ,i
pnlmonaryartery catheter. / (.lardiotlumu Mi^iAnavsth 12(4):
4X7-9RS (2(Hl2) Persistent SVC demonstrated with multi-slicespira l
computed tomography. Aiucriaiii Hi.m AsfUfiatioii liw 105(14):
79AC;, Bartelings MM. Deruiter Mt;. [\ielnunn RE(2(11)5) Basics of
cardiac development for the Lmderstanding of congenitalheart
malforcnation, liitiriuitioihil Pctliittrh': RcfCiirch
foiiiultitioii 57(2): K)'J-76MA A. Maher KAA (20
-
8/14/2019 Congenital Cardiac Malformations in Relation to
Central
7/7