-
8/22/2019 Clin. Pharmaco
1/13
Pharmacokinetic-Pharmacodynamic Modelling of theAntihistaminic
(H1) Effect of BilastineNerea Jauregizar,1 Leire de la Fuente,1
Maria Luisa Lucero,2 Ander Sologuren,2 Nerea Leal3 and Monica
Rodrguez3
1 PharmaDatum Data Analisis SL, Bermeo, Spain
2 Clinical Department, Laboratorios FAES FARMA SA, Leioa,
Spain
3 DynaKin, SL Parque Tecnologico de Bizkaia, Derio, Spain
Abstract Objective: To model the pharmacokinetic and
pharmacodynamic relationship of bilastine, a new histamineH
1
receptor antagonist, from single- and multiple-dose studies in
healthy adult subjects.
Methods: The pharmacokinetic model was developed from different
single-dose and multiple-dose studies.
In the single-dose studies, a total of 183 subjects received
oral doses of bilastine 2.5, 5, 10, 20, 50, 100, 120,
160, 200 and 220 mg. In the multiple-dose studies, 127 healthy
subjects received bilastine 10, 20, 40, 50, 80,
100, 140 or 200 mg/day as multiple doses during a 4-, 7- or
14-day period.
The pharmacokinetic profile of bilastine was investigated using
a simultaneous analysis of all concentration-
time data by means of nonlinear mixed-effects modelling
population pharmacokinetic software NONMEM
version 6.1.
Plasma concentrations were modelled according to a
two-compartment open model with first-order
absorption and elimination.
For the pharmacodynamic analysis, the inhibitory effect of
bilastine (inhibition of histamine-induced
wheal and flare) was assessed on a preselected time schedule,
and the predicted typical pharmacokinetic pro-
file (based on the pharmacokinetic model previously developed)
was used. An indirect response model was
developed to describe the pharmacodynamic relationships between
flare or wheal areas and bilastine plasma
concentrations.
Finally, once values of the concentration that produced 50%
inhibition (IC50) had been estimated for wheal
and flare effects, simulations were carried out to predict
plasma concentrations for the doses of bilastine 5, 10
and 20 mg at steady state (7296 hours).
Results: A non-compartmental analysis resulted in linear
kinetics of bilastine in the dose range studied. Bilastine
was characterized by two-compartmental kinetics with a
rapid-absorption phase (first-order absorption rate
constant = 1.50 h-1), plasma peak concentrations were observed
at 1 hour following administration and the
maximal response was observed at approximately 4 hours or later.
Concerning the selected pharmacodynamic
model to fit the data (type I indirect response model), this
selection is attributable to the presence of inhibitory
bilastine plasma concentrations that decrease the input response
function, i.e. the production of the skin reac-
tion. This model resulted in the best fit of wheal and flare
data. The estimates (with relative standard errors
expressed in percentages in parentheses) of the apparent
zero-order rate constant for flare or wheal spontaneousappearance
(kin), the first-order rate constant for flare or wheal
disappearance (kout) and bilastine IC50 values
were 0.44 ng/mL/h (14.60%), 1.09 h-1 (15.14%) and 5.15 ng/mL
(16.16%), respectively, for wheal inhibition, and
11.10 ng/mL/h (8.48%), 1.03 h-1 (8.35%) and 1.25 ng/mL (14.56%),
respectively, for flare inhibition.
The simulation results revealed that bilastine plasma
concentrations do not remain over the IC50 value
throughout the inter-dose period for doses of 5 and 10 mg.
However, with a dose of 20 mg of bilastine
administered every 24 hours, plasma concentrations remained over
the IC50 value during the considered period
for the flare effect, and up to 20 hours for the wheal
effect.
Conclusion: Pharmacokinetic and pharmacodynamic relationships of
bilastine were reliably described with
the use of an indirect response pharmacodynamic model; this led
to an accurate prediction of the pharmaco-
dynamic activity of bilastine.
ORIGINAL RESEARCH ARTICLE Clin Pharmacokinet 2009; 48 (8):
543-50312-5963/09/0008-0543/$49.95 2009 Adis Data Information BV.
All rights reserve
-
8/22/2019 Clin. Pharmaco
2/13
Background
Bilastine (F-96221-BM1, p-[2-[4-[1-(2-ethoxyethyl)-2-benz-
imidazolyl]piperidino]ethyl]-a-methylhydratropic acid) is anew
histamine H1 receptor antagonist (antihistamine) drug
currently under clinical development by FAES FARMA, SA,
Spain, for the treatment of allergic rhinoconjuntivitis
(seasonal
and/or perennial) and urticaria.
The results of in vitro preclinical studies provide evidence
that bilastine has antihistamine activity with high specificity
for
H1 receptors and poor or no affinity for other receptors.[1]
The results of the in vivo pharmacological studies conducted
in animal species corroborate those obtained in the in vitro
receptor binding experiments carried out previously. In this
sense, bilastine potently and selectively binds to H1
receptorswith behaviour similar to that of cetirizine and superior
to that
of fexofenadine.[2]
Understanding of the pharmacokinetics and pharmaco-
dynamics of this new H1 receptor antagonist provides the ob-
jective basis for selection of an appropriate dose and
dosage
interval and the rationale for modification of the dosage
regi-
men as needed in special populations, including elderly
patients, and those with hepatic or renal dysfunction.
The in vivo test in which inhibition of the histamine-
induced skin wheal and flare reactions is measured has been
extensively used to study the antihistaminic activity of several
H1receptor antagonists.[3-7] As was recently stated, this test may
not
be a valid surrogate measure for antihistaminic clinical
efficacy
and should not be used to compare different
antihistamines.[8]
However, it establishes the order of magnitude of the
clinically
efficacious dose. Indeed, phase III studies of bilastine have
shown
that the selected clinically efficacious regimen of 20 mg once
daily
was in accordance with the conclusions of phase I studies.
[9]
Little pharmacokinetic and pharmacodynamic modelling has
been performed for antihistaminic agents. For most drugs,
the
relationship between exposure and effect is nonlinear and
plasma
drug concentrations cannot usually be (directly) related to
the
drug effect.[10] In the case of antihistaminic drugs, both the
effectcompartment models for norebastine and levocabastine[7]and
the
indirect response models for mizolastine[11] and cetirizine[12]
have
been applied to account for the lag between peak plasma drug
concentrations and pharmacodynamic effects.
In the present study, plasma drug concentration-time pro-
files of single and multiple oral doses of bilastine given
to
healthy subjects were described using an appropriate popula-
tion pharmacokinetic model. The pharmacodynamic effect of
bilastine was modelled by means of a physiological indirect
response model (using the pharmacokinetic model previously
developed). The estimated pharmacokinetic and pharmaco
dynamic parameters of the model are summarized in this
article
Methods
Subjects and Study Design
A total of 310 healthy adult subjects (248 males an
62 females) were included in the study. All participants gav
signed informed consent, and ethical approval was obtained
from the Queens University Research Ethics Committe
(Belfast, Northern Ireland), the Northern Ireland Phase
Research Ethics Committee from the Office for Researc
Ethics Committees Northern Ireland (Belfast, Norther
Ireland) or the Ethical Committee for Clinical Research oSanta
Creu i Sant Pau Hospital (Barcelona, Spain).
Bilastine plasma concentration-time data were availabl
from 12 studies and antihistamine activity was quantified in
two of these studies; all of the studieswere part of a phase I
tria
Study design details are summarized in table I. [13-18] All of
th
available data were analysed simultaneously.
Blood samples from studies 1 and 2 were drawn at th
following sampling times: predose (0 hour) and at 0.5, 1, 1.5,
2
2.5, 3, 3.5, 4, 6, 8, 12, 16, 24, 36, 48, 72 and 96 hours
post-dose
Blood samples from studies 4, 5, 7, 8, 9 and 10 were collected
a
the same sampling times but only up to 48 hours post-dose andup
to 72 hours post-dose for studies 11 and 12. Studies 3, 6 an
10 were multiple-dose studies where samples were available o
day 1 (samples were collected up to 24 hours post-dose)
betwee
96 and 144 hours for study 10, between 168 and 216 hours fo
study 6 and on day 14 (240288 hours) for study 3.
The antihistaminic activity of bilastine was evaluated b
using the effect measurements (wheal and flare) from studie
4 and 5. The inhibitory effect of bilastine (inhibition of
histamine
induced wheal and flare) was assessed at a preselected tim
schedule: predose and at 1.5, 4, 8, 12 and 24 hours
post-dose.
Pharmacokinetics
Blood samples (7 mL) from a suitable antecubital vein wer
collected into green-top/sodium heparin Vacutainer tube
predose and at different post-dose timepoints. Plasma sample
were separated by centrifugation (approximately 2500 rpm 1
minutes at 41C), split into two aliquots and stored in
clearl
labelled containers in a freezer set at or below -201C unt
shipment to MDS Pharma Services in Zurich, Switzerland, fo
analysis.
544 Jauregizar et a
2009 Adis Data Information BV. All rights reserved. Clin
Pharmacokinet 2009; 48 (
-
8/22/2019 Clin. Pharmaco
3/13
Bilastine concentrations were determined in heparinized hu-
man plasma by a validated liquid chromatography-tandem mass
spectrometry (LC-MS/MS) method using a solid-phase extrac-
tion procedure. In brief, using 3-mL disposable glass tubes,
500mL of each plasma sample was spiked with internal
standard(100mL of 500ng/mL of trandolapril in water) and
combined
with 300mL of Millipore water and 100mL of 1% (v/v) aqueous
trifluoroacetic acid. The sample was vortex-mixed and
centrifuged for 1 minute at 3000 rpm. Solid-phase extraction
cartridges (Isolute C8, EC; Biotage AB, Uppsala, Sweden)
were
solvated subsequently with 2 mL of methanol and 2 mL of 0.1%
(v/v) aqueous trifluoroacetic acid. Samples were applied
quanti-
tatively, washed with 2 mL of 0.1% (v/v) aqueous
trifluoroacetic
acid and eluted with 2 mL of 5 mM ammonium acetate in 90%
(v/v) aqueous methanol. The eluent was evaporated using a
vacuum centrifuge (SpeedVac; Savant Instruments, Lif
Sciences International, Runcorn, UK) and the residue wa
reconstituted in 200mL of mobile phase (1% [v/v] formic acid
i
50% [v/v] aqueous acetonitrile), vortex-mixed for 1 minute
an
transferred into a polypropylene auto sampler vial.LC-MS/MS
analysis was performed using a Perkin-Elme
LC system combined with a Sciex API 3000 mass spectromete
equipped with a Turbo Ion Spray source (GenTech Scientific
Inc., Arcade, NY, USA). A 10 mL-aliquot of the reconstitute
sample was injected using a reverse phase column (Water
SymmetryShield RP18, 3.5 mm 2.1 50 mm; Waters Corpo
ration, Milford, MA, USA) at a temperature of 501C and
constant mobile phase flow of 0.15 mL/minute. The retentio
times were 0.7 minutes for bilastine and 0.9 minutes fo
trandolapril. Mass transitions of 464-272 for bilastine an
Table I. Summary of phase I clinical studies, evaluating the
pharmacokinetics of bilastine (BIL), included in the
pharmacokinetic database. The pharmaco
dynamic database was created with data from studies 4 and 5
Study
number
Description Dosing regimen No. of healthy
adult subjects
1 Double-blind, ascending, single-dose study to evaluate the
safety, tolerability and
pharmacokinetics of BIL
SOD: 5, 10, 50 and
100mg
36
2 Pharmacokinetic study to assess the single-dose
bioavailability of BIL under fed and
fasted conditions
SOD: 20 mg 12
3[13] Randomized, multiple-dose study to evaluate the safety and
tolerability and pharmacokinetics
of BIL at escalating doses
MOD: 10, 20, 50 and
100mg/day for 14 days
36
4[14] Randomized, single-dose, placebo-controlled, four-period
crossover study to evaluate the
safety and tolerability, pharmacokinetics and antihistaminic
activity of BIL at five dose levels
compared with cetirizine
SOD: 2.5, 5, 10, 20
and 50 mg
21
5[15] Open-label study to assess the effects of age and gender
on the pharmacokinetics and
pharmacodynamics of BIL
SOD: 20 mg 32
6 Randomized, double-blind, crossover, placebo- and positive
standard-controlled, single-centre
clinical trial for evaluation of CNS effects of BIL at different
doses after single and repeat
oral administration
MOD: 20, 40 and
80mg/day for 7 days
20
7[16] Pharmacokinetic and safety study evaluating the potential
interaction of erythromycin and BIL
under steady-state conditions
SOD: 20 mg 24
8 Pharmacokinetic and safety study evaluating the potential
interaction of ketoconazole and BIL
under steady-state conditions
SOD: 20 mg 24
9[17] Randomized, double-blind, placebo-controlled, sequential
group study to evaluate the safety,
tolerability and pharmacokinetics of single, ascending doses of
BIL and of multiple doses of BIL
SOD: 120, 160, 200
and 220 mg
MOD: 140 and
220mg/day for 7 days
54
10 Randomized, multiple-dose, double-blind, five-way crossover
study of the ECG effects
of bilastine
MOD: 20 and 100 mg/day
for 4 days
30
11 Randomized, open-label, two-way crossover study to evaluate
the effect of grapefruit juice on
the single-dose pharmacokinetics of BIL
SOD: 20 mg 11
12[18] Randomized, open-label, two-way crossover study to
evaluate the effect of diltiazem on the
single-dose pharmacokinetics of BIL
SOD: 20 mg 11
CNS = central nervous system; ECG =electrocardiographic;
MOD=multiple oral doses; SOD= single oral dose.
PK/PD Modelling of Bilastine 54
2009 Adis Data Information BV. All rights reserved. Clin
Pharmacokinet 2009; 48 (
-
8/22/2019 Clin. Pharmaco
4/13
431-234 for trandolapril were selected for quantification in
multiple-reaction monitoring mode.
Signal quantification was performed by the peak area ratio.
The assay was validated over a linear range (0.2200 ng/mL).The
lower limit of quantification was 0.2 ng/mL.
Antihistamine Activity
Antihistamine activity was evaluated by measuring the sur-
face areas of skin wheals and flares for 24 hours. In each
treatment period, histamine skin-prick tests (100 mg/mL his-
tamine in normal saline) were performed on the back of the
subject at the following timepoints: predose and at 1.5, 4, 8,
12
and 24 hours post-dose. At each timepoint, two skin-prick
tests
were performed on matching sites on opposing sides of the
spine. Ten minutes after each skin-prick test, the wheal and
flare areas induced by histamine were outlined directly on
the
back with a green marker and a red marker, respectively, and
transferred onto acetate tracing paper using permanent
marker
pens. Calculation of the wheal and flare areas was performed
manually. An average area of the two sites for each
timepoint
was calculated and used for analysis. Post-treatment,
histamine
time-response (wheal and flare areas expressed in square
cen-
timetres) curves were constructed.
Data Analysis
The first step was to perform a non-compartmental analysis
of
the data in order to evaluate linearity or non-linearity of
the
kinetics. The computational method used to measure areas was
the trapezoidal rule. The analysis was performed
simultaneously
at the different dose levels. This analysis was carried out with
the
use of WinNonlin software (Pharsight Corporation, Cary, NC,
USA). The estimated parameters for the different doses were
compared by analysis of variance (ANOVA) with theuseof SPPS
software version 14 (SPPS, Inc., Chicago, IL, USA).
Afterwards, a population approach was used and the strat-
egy was as follows: the pharmacokinetic model was built
firstand, using the typical disposition characteristics of
bilastine, a
pharmacodynamic model describing the drug effect was
then developed. All analyses were performed with nonlinear
mixed-effects modelling software NONMEM version 6.1
(Globomax LLC, Ellicott City, MD, USA).[19]
For each of the pharmacokinetic or pharmacodynamic
analyses, a basic population model was proposed. Based on a
model that describes mean population and individual tenden-
cies, observations are expressed as follows (equation 1):
OBSij fyi; D;tj eij Eq: 1
where OBSij is the jth observation (bilastine plasma concen
tration or the measured wheal or flare effect) in the ith
ind
vidual, f represents the structural model, yi represents the set
o
parameters (pharmacokinetic or pharmacodynamic) for thith
individual, D is the administered dose, tj is the time at whic
the jth observation was recorded and eij represents the
residua
shift of the observation from model predictions; eij are
random
variables assumed to be symmetrically distributed around 0
with variance denoted by s2. Although, in the previous
expres
sion, an additive model was used to relate observations t
predictions, different models (i.e. the constant coefficient
o
variation [CV] slope/intercept) were also explored.
For each of the elements ofyI, the following model was use
(equation 2):
Pi P eZiP Eq: 2
This equation represents an exponential model to describ
interindividual variability in the model parameters. Pi
denote
the individual parameter estimated forthe ith individual, P is
th
typical value of the parameter estimated for the population
an
Zi is the interindividual error for the ith individual, i.e.
th
difference between the estimated value of P and the typica
value of P for the population. The random variable Zi is as
sumed to be symmetrically distributed around 0 with varianc
of O. Other models that were compared were the additiv
model (constant variance) and the proportional model (th
constant CV).
Different pharmacokinetic models (in the absence of co
variates) were fitted to the available data. The selection
criteri
used in the model-building and selection process include
the minimum value of the objective function provided b
NONMEM defined as -2 times log of maximum likelihood a
a measure of goodness of fit, the Akaike Information
Criterio
(the value that is used to compare hierarchical and non
hierarchical models with the same weighting scheme) and othe
population-parameter values including standard errors of th
estimates, the CV and confidence intervals. Residual plots
ma
also be used as diagnostic tools. In this sense, weighted
annon-weighted residuals versus predicted concentrations and
ver
sus time were analysed since shaped patterns in these plots
ma
indicate problems with the error model (variance or weighting)
o
with the structural model. Other plots that were examined in
cluded predicted versus observed concentration plots, as well
a
predicted and observed concentrations versus time.
Individual concentration-time profiles were obtained b
post hoc Bayesian estimation using model parameters that ha
been previously obtained. Bayesian estimates of the
individua
pharmacokinetic parameters were obtained by standar
546 Jauregizar et a
2009 Adis Data Information BV. All rights reserved. Clin
Pharmacokinet 2009; 48 (
-
8/22/2019 Clin. Pharmaco
5/13
methods with the estimated values of the population fixed-
and
random-effect parameters.
Visual predictive checks (VPCs) were used as a way to visua-
lize how well the model predicted the profile and the
vari-ability, assuming perfect precision (no uncertainty). VPCs
were
developed by simulating 5000 individual concentration-time
profiles for the selected therapeutic dose (20 mg of
bilastine
given once daily), taking population estimates of fixed
effects
and sampling from random effects distribution to obtain
indi-
vidual profile prediction. Random draws from residual error
distribution were added to each predicted value.
Evaluation of the Relationship between Covariates
and Model Parameters
Theinfluence of covariates on themodel structural parameters
was first assessed by plotting individual empirical Bayesian
esti-
mates of parameters versus all of the preselected potential
co-
variates including demographic data (age, bodyweight, height
and sex), biochemical data (serum albumin, creatinine,
bilirrubin,
g-glutamyltransferase [GGT], aspartate aminotransferase
[AST],
alkaline phosphatase and blood urea nitrogen [BUN] con-
centrations) and vital signs (pulse).
Initially, plots of the interindividual variabilities of
phar-
macokinetic parameters versus each analysed covariate, as
well
as weighted residuals versus covariates, were analysed. Then
a
statistical analysis of covariates was carried out and the
sta-
tistically significant covariates were included in the base
model
by stepwise regressions with an inclusion criterion of p
0.05.
Once the covariates to be included in the model were
selected, this model with covariates was statistically
compared
with the base model.
In the final model selection process, all of the described
issues were considered, as well as the standard error of
esti-
mates, the extent of interindividual variability, and the
corre-
lation matrix of parameters and diagnostic plots (including
covariance among parameters and distribution histograms).
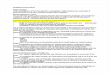
Pharmacokinetic Model
A compartmental analysis showed that a two-compartment
model with first-order absorption and elimination best de-
scribed the kinetics of bilastine after oral administration.
NONMEM subroutine ADVAN4, TRANS4 was used. The
schematic illustration in figure 1 assumes first-order
absorp-
tion, where ka denotes the first-order absorption rate
constant.
This figure shows schematically the time-course of the drug
in the central compartment (compartment 1) and peripheral
compartment (compartment 2) after administration of an ora
dose. The drug is eliminated from the central compartment
where CL denotes drug clearance, and on the other hand, it i
distributed from the central to the peripheral compartmentQ
being the inter-compartmental clearance. Hence, V1 and V
denote the central compartment volume of distribution and th
peripheral compartment volume of distribution, respectively.
Model building and final analysis were performed usin
NONMEM with the first-order conditional estimatio
(FOCE) method. After completing the model-building proces
for the totality of plasma concentration-time data from th
11 studies (single- and multiple-dose studies), population
esti
mates of the fixed effects (y) as well as their relative
standar
errors (ESy), expressed in percentages, were obtained.
Individual concentration-time profiles were obtained byposhoc
Bayesian estimation using the model parameters that ha
been previously obtained. Bayesian estimates of individua
pharmacokinetic parameters were obtained by standar
methods, with estimated values of the population fixed- and
random-effect parameters.
Pharmacodynamic Model
In order to obtain estimates of the pharmacodynami
properties of bilastine, the entire population
pharmacokinetic
were estimated separately and the empirical parameter est
mates, conditional on those subjects with pharmacodynami
kin
1V1
2V2
ka
kout R
D
CL
Q
3 Pharmacodynamics
Pharmacokinetics
Inhibition
Fig. 1. Schematic presentation of the
pharmacokinetic-pharmacodynam
model that best fitted the data (i.e. plasma concentration and
wheal and flar
data) on the time-course of the drug in the central compartment
(compartmen
1) and the peripheral compartment (compartment 2) after
administration of a
oral dose (D). The specified indirect response model is a type I
model o
inhibition of response build-up model; observed effects were
coded as dat
from compartment 3. CL=apparent total body clearance of the drug
from
plasma; ka= first-order absorption rate constant; kin=
zero-order rate consta
for productionof response; kout= first-orderrate constant for
lossof response
Q = intercompartmental clearance; R = response; V1= central
compartme
volume of distribution; V2=peripheral compartment volume of
distribution.
PK/PD Modelling of Bilastine 54
2009 Adis Data Information BV. All rights reserved. Clin
Pharmacokinet 2009; 48 (
-
8/22/2019 Clin. Pharmaco
6/13
measurements, were used to drive the turnover model in
$DES. In this sequential pharmacokinetic-pharmacodynamic
modelling, the corresponding (proportional) sigma for the
pharmacokinetic parameter was fixed to the pharmacokineticmodel
estimate. This approach reduced run times drastically
when compared with simultaneous fitting, which was very time
intensive and did not converge.
A physiological indirect response model with inhibition of
response production[11] was used to describe bilastine
pharma-
codynamics. A schematic illustration of the indirect
response
model is presented in figure 1.
In the population pharmacokinetic-pharmacodynamicmodel,
the following differential equations defining the indirect
res-
ponse model were additionally introduced (equations 3 and
4):
EFF IC50IC50 A1
Eq: 3
dA3
dt kin EFF kout A3 Eq: 4
where EFF corresponds to the effect.
The specified indirect response model is a type I model or
inhibition of response build-up model, where k in is the
zero-
order constant for response production, while kout
represents
the first-order constant for loss of response. IC50 can be
defined as the drug concentration that achieves 50% of
maximum inhibition. Note that in the NONMEM data file,
the observed wheal or flare effects were coded as data from
compartment 3 [A(3)].
Initial values for the pharmacodynamic parameters of k in,
kout, IC50 and maximum inhibition (Imax) were estimated as
follows: kout was set to log2 divided by the effect
half-life,
roughly estimated from the data; kin was calculated taking
into
account that the baseline value of the response (the
observed
baseline value at time 0) equals k in/kout; the IC50 was set to
the
plasma concentration corresponding to the time of maximum
effect; and Imax was set to 1.
The FOCE method was applied in the pharmacokinetic-
pharmacodynamic modelling process.
Simulations
Finally, computer simulations were carried out with the aim
of selecting the optimal dose and dosing regimen of
bilastine.
The selected times to perform the simulations were between
72
and 96 hours, i.e. those corresponding to day 4 in a
multiple-
dose regimen. This time selection was based on the value of
the
elimination half-life obtained previously, and simulated
con-
centrations were at steady state. Mean plasma concentration-
time profiles of bilastine were simulated for daily doses of
5, 10 and 20 mg. IC50 values, estimated separately for whea
and flare, were used as thresholds for dose selection via
simu
lation. Proposed dosing regimens should maintain the con
centration levels within the thresholds during the entire
regimeinterval.
Results
Pharmacokinetic Study
The non-compartmental pharmacokinetic analysis reveale
that bilastine presents linear pharmacokinetics in the
studie
dose range (2.5220 mg/day). Both the maximum concentra
tion and the area under the plasma concentration-time curv
(AUC) of bilastine increased proportionally to the administered
doses. The terminal elimination half-life as well as th
other pharmacokinetic parameters of bilastine remained con
stant over the entire studied dosing range. The ANOVA wit
Scheffe post hoc confirmed that the pharmacokinetics of bi
lastine are linear in the dose range of 2.5220 mg/day.
After completing the model-building process for the totalit
of the plasma concentration-time data from the different
stud
ies (single- and multiple-dose studies), population estimates
o
the fixed effects (y) as well as their ESy values, expressed
i
percentages, were obtained and are presented in table II.
Thes
standard errors denote the precision in parameter estimation
concluding with an acceptable precision in estimation (
-
8/22/2019 Clin. Pharmaco
7/13
shown) and high residual values that increased with
predicted
concentrations were observed. This situation led to a cone-
shaped plot, suggesting the use of a weighting factor. The
addition of a weight factor helped to overcome this effect.
In
fact, as the cone shape disappeared, residual values
declined
considerably, and residual distribution became random around
the 0 line. In conclusion, this variance model is suitable.
Addi-
tionally, the time-course profiles of non-weighted and
weighted
residuals were studied (data not shown). The adequacy of the
weighting scheme was again demonstrated. Residual values
were acceptable, as well as random distribution of residual
around the 0 line throughout the analysed time range.
The VPC for the 20 mg dose is shown in figure 4.
Pharmacodynamic Study
The results of the population pharmacokinetic-pharmaco
dynamic modelling for wheal and flare effects are summarized
in table III. These ESy values are related to estimation
preci
sion, which were quite acceptable (14.60%, 15.14% and 16.16%
for kin, kout and IC50, respectively).
Model parameter Z values, expressed as CV%, are als
presented in this table. It can be observed that the IC50 wa
associated with a higher interindividual variability than th
other parameters.Intra-individual variability (e) had a value of
0.011
(ESy= 6.28%). As a result of the error model that was
selecte
(additive error), this e is defined as a standard deviation
(in
contrast to the CV% in the pharmacokinetic model) and ac
counts for model mis-specification or measurement erro
Hence, the obtained value is acceptable, as it is of the sam
order as the available wheal effects.
The model-predicted individual effect on histamine-induce
wheal as a function of time was in close proximity to th
time-course profile of the observed effects (figure 5). A
simila
congruence was observed for flare inhibition (figure 6).
Pharmacodynamic parameter final estimates and their ES
values for flare are also presented in table III. kin values
wer
different for flare and wheal; this can be explained by the fact
tha
Table II. Population pharmacokinetic-model fit to plasma
concentration-
time data from all available studies. Population
pharmacokinetic-parameter
estimates (with relative standard errorsa [ESy] expressed as %)
and inter-
individual variability expressed as the percentage of the
coefficient of varia-tion (CV [%])
Parameter Estimate y (ESy) CV% (ESy)
CL (L/h) 18.1 (1.8) 29.0 (8.7)
V1 (L) 59.2 (2.2) 35.4 (9.6)
Q (L/h) 1.59 (3.9) 56.5 (10.3)
V2 (L) 30.2 (5.1) 73.1 (9.6)
ka (h-1) 1.50 (3.2) 35.4 (16.9)
s (%) [ESy] 28.6 (6.1)
a The relative standard error is the standard error divided by
the parameter
estimate.
CL=
apparent total body clearance of the drug from plasma; ka=
first-orderabsorption rate constant; Q=apparent
intercompartmental clearance;
V1= central compartment volume of distribution;
V2=peripheralcompartment
volume of distribution.
0
1000
2000
3000
4000
5000
6000
7000
8000
0 2000 4000 6000 8000
Observed concentration (ng/mL)
Population-predictedco
ncentration(ng/mL)
Fig. 2. Population-predicted concentrations vs observed
concentrations with the line of identity.
PK/PD Modelling of Bilastine 54
2009 Adis Data Information BV. All rights reserved. Clin
Pharmacokinet 2009; 48 (
-
8/22/2019 Clin. Pharmaco
8/13
flare areas were larger than wheal areas. The kout value was
ap-
proximately 1 h-1 for both wheal and flare, and the IC50
values
(5.15 ng/mL for wheal and 1.25 ng/mL for flare) were lower
for
flare than for wheal by a ratio of approximately 4 and were
low
compared with the bilastine concentrations obtained after
oral
administration.
Finally, the results of simulations of plasma concentrations
corresponding to doses of 5, 10 and 20 mg and for a
preselected
time schedule that ranged from 72 to 96 hours were analysed
(figure 7). The time selection was carried out under th
assumption of being at steady state. Taking into account tha
the estimated IC50 values for wheal and flare effects wer
5.15 ng/mL and 1.25ng/mL, respectively, bilastine plasm
concentrations reached after a dose of 20 mg remained over
th
IC50 value for the flare effect throughout the entire
inter-dos
period (24 hours). Bilastine plasma concentrations decrease
to less than the mean estimated IC50 value for the whea
effect between 20 and 24 hours only. This means that th
0
1000
2000
3000
4000
5000
6000
7000
8000
0 1000 2000 3000 4000 5000 6000 7000 8000
Observed concentration (ng/mL)
Individual-predictedconcentration(ng/mL)
Fig. 3. Individual-predicted concentrations vs observed
concentrations with the line of identity.
0
100
200
300
400
500
600
700
800
900
1000
0 2 4 6 8 10 12 14 16 18 20 22 24
Time (h)
Bilastineplasm
aconcentration(ng/mL)
Observed concentrationMedian predicted interquartile
95% predicted interval
Fig. 4. Predicted and observedconcentration-time profiles of
bilastine after a single oral doseof 20 mg. The simulations
usedfixed effects point estimates an
were performed across, between and within subject
variability.
550 Jauregizar et a
2009 Adis Data Information BV. All rights reserved. Clin
Pharmacokinet 2009; 48 (
-
8/22/2019 Clin. Pharmaco
9/13
main part of the antihistaminic activity lasts nearly for
the
entire duration between two once daily dosing intervals.
However, for doses of 5 and 10 mg, plasma drug concentra-
tions were below the wheal IC50 value for a few hours before
administration of the next dose (10 hours for a 10 mg dose
and 16 hours for a 5 mg dose). Hence it can be concluded
that the optimal dosing regimen for bilastine is 20 mg every
24 hours.
Discussion
The purpose of this study was to characterize the relation-
ship between the pharmacokinetics and the antihistaminic ac-
tivity of bilastine in healthy adult subjects. This is
importantnot
only to establish adequate dosage regimens,[20] but also
to understand the actual mechanism of action involved in the
in-vivo drug effect.[21]
In this study, the pharmacokinetics and pharmacodynamics
of bilastine after oral administration were studied using
thepopulation pharmacokinetic-pharmacodynamic approach. The
non-compartmental pharmacokinetic analysis revealed that
bilastine displays linear pharmacokinetics in the studied
dose
range.
Bilastine was characterized by two-compartmental kinetics
with a rapid-absorption phase (ka= 1.50 h-1); peak plasma
concentrations were observed at 1 hour following oral admin-
istration and the elimination half-life was approximately
14 hours. Bilastine and most orally administered new H1receptor
antagonists are well absorbed and appear to be
extensively distributed into body tissues; many are highly
pro
tein bound. Most new H1 receptor antagonists do not accu
mulate in tissues during repeated administration.[3] The sam
result was observed for bilastine: according to the ratio of
thAUC obtained from multiple-dose studies (i.e. the accumula
tion ratio between the AUC from 312 to 336 hours and th
AUC from 0 to 24 hours = 1) [results not shown], it can b
inferred that bilastine does not undergo accumulation after
th
studied dosing regimens.
The effect of bilastine on raw wheal and flare areas, ex
pressed as square centimetres, was modelled. Measurement o
wheal and flare skin reactions to assess the pharmacodynamic
of antihistaminic drugs has been extensively used.
[4,10,11,22-24]
Little pharmacokinetic and pharmacodynamic modellin
has been performed for antihistaminic agents. The mechanismof
action of bilastine corresponds to an inhibition of build-up
turnover pharmacodynamic model,[25,26] and this model wa
successfully applied in this study. In fact, indirect
respons
models have been successfully used to describe the pharmaco
dynamics of antihistaminic drugs such as mizolastine[10] an
cetirizine.[12]
In this study, the peak plasma concentration was rapidl
reached in approximately 1 hour and the maximal respons
was observed later at approximately 4 hours or longer. Here
the measurement site is the skin; therefore, the observe
delay could be attributed to diffusion to the skin of the
anti
histamine. The indirect-effect model intrinsically addresses
thi
delay.[20]
The pharmacokinetic-pharmacodynamic model that wa
developed showed good performance in describing both th
mean population tendency and individual effect profiles. Th
0.1
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0 10 20 30
Time (h)
Predictedandobservedwhealareas(cm
2)
Observed wheal effect
Predicted wheal effect
Fig. 5. Predicted and observed wheal effects vs time for
individuals wh
participated in study 5.
Table III. Pharmacokinetic-pharmacodynamic population model fit
of the
wheal and flare effects
Parameter kin
[ng/mL/h]
kout
[h-1]
IC50
[ng/mL]
Wheal
Estimatea 0.44 (14.60) 1.09 (15.14) 5.15 (16.16)
Zb 29.36 (32.95) 14.04 (81.22) 55.95 (45.05)
Flare
Estimatea 11.10 (8.48) 1.03 (8.35) 1.25 (14.56)
Zb 24.02 (45.41) 26.98 (26.65) 65.65 (29.93)
a Values are expressed as estimate (%ESy). The ESy is the
standard error
divided by the parameter estimate.
b Values are expressed as %CV (%ES).
g = interindividual variability;ES = standard error; ESh=
relative standarderror
of the pharmacodynamic parameter; IC50= estimated concentration
produ-cing 50% inhibition; kin= zero-order rate constant for
production of response;
kout= first-order rate constant for loss of response.
PK/PD Modelling of Bilastine 55
2009 Adis Data Information BV. All rights reserved. Clin
Pharmacokinet 2009; 48 (
-
8/22/2019 Clin. Pharmaco
10/13
pharmacodynamic parameters had reasonable estimates. Dif-
ferences in kin values for flare and wheal, as well as lower
IC50values for flare than for wheal, have also been observed
with
mizolastine,[11] cetirizine[12] and other antihistaminic drugs
in
an analysis in which an effect compartment model was used.
[7]
When using typical pharmacokinetic parameters, the inter-
individual variability associated with pharmacodynamic
parameters is likely to be overestimated, since variability
of
the absorption and disposition processes is also involved.
However, the estimates of variability were not extremely
high: 29.36% for kin, 14.04% for kout and 55.95% for IC50
forthe
wheal effect; and 24.02%, 26.98% and 65.65%, respectively,
for the flare effect.
The NONMEM run, by itself, estimated population
mean values and variances of parameter values within such a
population, as well as residual error variance. Populatio
means were then used as a priori estimates for individual
pos
hoc parameters by the Bayesian analysis in every iteration o
minimizing the objective function. The population mixedeffects
approach with Bayesian analysis is a powerful tool fo
accounting for interindividual variability and, hence,
allowin
for the description of the time-course of the antihistamini
effect for each individual. These results demonstrate tha
pharmacokinetic-pharmacodynamic analysis, as stated b
Levy,[20] can reflect the actual mechanism of action involved
in
the pharmacological response of a given drug.
Finally, with the use of the population-pharmacokineti
model, computer simulations were performed to obtain bilas
tine plasma concentrations at steady state after the adminis
tration of 5, 10 or 20 mg once daily. Bilastine
concentrationreached after a dose of 20 mg are over the IC50 value
for th
flare effect throughout the entire inter-dose period (24
hours)
Such concentrations decreased to less than the mean estimate
IC50 value for wheal between 20 and 24 hours only. This
implie
that the main part of the antihistaminic activity lasts nearly
fo
the entire duration between two once-daily dosing intervals
which suggests that the optimal dosing regimen for bilastine
i
20 mg every 24 hours. Pharmacokinetic and pharmacodynami
relationships of bilastine were reliably described with the use
o
a physiological indirect response model; this led to an
accurat
prediction of bilastine pharmacodynamic activity. Further
more, although this model has no predictive value for de
termining the clinical superiority of one antihistaminic dru
over another, it provides relevant information regarding
which
drug dosages, based on the drug concentration-response i
terms of the rate and duration of inhibition, could be anti
cipated to be below the desired pharmacodynamic response an
1
10
100
1000
0 12 24 36 48 60 72 84 96
Time (h)
Simulatedbilastine
plasma
concentration(ng
/mL)
IC50 of wheal effect
IC50 of flare effect
Fig. 7. Simulation of population mean bilastine plasma
concentrations corresponding to four consecutive 20 mg doses and,
thus, being at steady state. Th
estimated concentration producing 50% inhibition (IC50) values
for wheal and flare effects (5.15 ng/mL and 1.25 ng/mL,
respectively) are also shown. Plasm
concentrations of bilastine after a dose of 20 mg are over the
IC50 value for the flare effect throughout the inter-dose period
(24 hours).
10
0
10
20
30
0 10 20 30
Time (h)
Predictedandobservedflareareas(cm
2)
Observed flare effect
Predicted flare effect
Fig. 6. Predicted and observed flare effects vs time for
individuals who
participated in study 5.
552 Jauregizar et a
2009 Adis Data Information BV. All rights reserved. Clin
Pharmacokinet 2009; 48 (
-
8/22/2019 Clin. Pharmaco
11/13
which dosage should be the potential candidate for further
development in clinical trials. This should be determined on
the
basis of more clinically relevant endpoints.[26]
Conclusion
Bilastine displayed linear pharmacokinetics in the studied
dose range (2.5220 mg/day). The population-pharmacokinetic
model that resulted in the best fit of plasma
concentration-time
data was a two-compartmental model with first-order absorp-
tion and elimination. No significant relationship could be
detected between pharmacokinetic parameters and any of the
covariates that were analysed (age, bodyweight, height, sex,
serum albumin, creatinine, bilirubin, GGT, AST, BUN and
alkaline phosphatase concentrations, as well as pulse).
Ingeneral, no covariate had a substantial role in explaining
the
variability of the model parameters.
The pharmacokinetic-pharmacodynamic model that yielded
the best fit of time-effect data was a type I indirect
response
model, also known as a model for inhibition of response pro-
duction. In fact, the selected population model fits
success-
fully both wheal-and flare-effect data. The estimated IC50values
were 5.15 ng/mL for the wheal effect and 1.25 ng/mL
for the flare effect. Therefore, with 20 mg of bilastine
given
every 24 hours, plasma drug concentrations at steady state
would be maintained over the IC50 value (to inhibit thewheal and
flare effects) throughout almost the entire dosing
interval.
Acknowledgements
The authors would like to thank Deirdre McLaverty and A.J.
Stewart
(MDS Pharma Services Belfast, Northern Ireland), and M.J.
Barbanoj,
R.M. Antonijoan and C. Garca-Gea (Centre dInvestigacio de
Medica-
ments, Institut de Recerca de lHospital de la Santa Creu i Sant
Pau,
Barcelona, Spain) as the principalinvestigators of the different
studies. The
authors received no funding forthe conduct of this study.Nerea
Jauregizar
and Leire de la Fuente are employees of Pharma Datum Data Ana
lisis SL;
Nerea Leal and Mo nica Rodrguez are employees of DynaKin; andM.
Luisa Lucero and Ander Sologuren are employees of FAES FARMA
SA The authors have no other conflicts of interest that are
directly relevant
to the content of this study.
References1. Corco stegui R, Labeaga L, Innera rity A, et al.
Preclinical pharmaco-
logy of bilastine, a new selective histamine H1 receptor
antagonist:
receptor selectivity and in vitro antihistaminic activity. Drugs
2005; 6:
371-87
2. Corco stegui R, Labeaga L, Innera rity A, et al. In vivo
pharmacological
characterisation of bilastine, a potent and selective histamine
H1 receptor
antagonist. Drugs 2006; 7: 219-31
3. Simons FER, Simons KJ. Clinical pharmacology ofnew histamine
H1 recepto
antagonists. Clin Pharmacokinet 1999; 36: 329-52
4. Rosenzweig P, Caplain H, Chaufour S, et al. Comparative wheal
and flar
study of mizolastine vs terfenadine, cetirizine, loratadine and
placebo i
healthy volunteers. Br J Clin Pharmacol 1995; 40: 459-65
5. Harvey RP, Schocket AL. The effect of H1 and H2 blockade on
cut
neous histamine response in man. J Allergy Clin Inmunol 1980;
6
136-9
6. Simons FER, Mc Millan JL, Simons KJ. A double-blind, single
dose, cros
over comparison of cetirizine, terfenadine, loratadine,
astemizole, and chlor
pheniramine versus placebo: suppressive effects on
histamine-induced whea
and flares during 24 hours in healthy subjects. J Allergy Clin
Inmunol 1990
86: 540-7
7. Heykants JJP, Snoeck E, Awouters F, et al. Antihistamines.
In: Van Boxtel C
Holford NHG, Danhof M, editors. The in vivo study of drug
actio
Amsterdam: Elsevier Science Publishers, 1992: 337-56
8. Devillier P, Bousquet J. Inhibition of the histamine-induced
weal and flar
response: a valid surrogate measure for antihistamine clinical
efficacy? Cli
Exp Allergy 2007; 37: 400-14
9. Kuna P, Nowacki Z, van Cauwenberge P, et al. A phase study
com
paring the efficacy and safety of once daily bilastine with
cetirizine an
placebo for the treatment of seasonal allergic rhinitis. Allergy
2007; 6
132-3
10. Holford NHG, Sheiner LB. Understanding the
concentration-effect relation
ship: clinical application of pharmacokinetic-pharmacodynamic
model
Clin Pharmacokinet 1981; 6: 429-53
11. Deschamps C, Dubruc C, Mentre F, et al. Pharmacokinetic and
pharmaco
dynamic modeling of mizolastine in healthy volunteers with an
indire
response model. Clin Pharmacol Ther 2000; 68: 647-57
12. Urien S, Tillement JP, Ganem B. A
pharmacokinetic-pharmacodynam
modelling of the antihistaminic (H1) effects of cetirizine. Int
J Clin Pharmaco
Ther 1999; 37: 499-502
13. Roupe K, Sologuren A, Crean C, et al. The pharmacokinetics
of bilastine aftsingle and 14 days once daily administration
[abstract]. Basic Clin Pharmaco
Toxicol 2007; 101 Suppl. 1: 148
14. Sologuren A, Valiente R, Crean C, et al. Relationship of
dose to inhibitio
ofwhealandflarefor 5 dosesof bilastineand10
mgcetirizine[abstract no. 69
J Clin Pharmacol 2007; 47 (9): 1198
15. Roupe K, Sologuren A, Crean C, et al. Effect of age and
gender on the pha
macokinetics and pharmacodynamics of bilastine [abstract no.
70]. J Cli
Pharmacol 2007; 47 (9): 1198
16. Antonijoan RM, Garca-Gea C, Puntes M, et al. Estudio
farmacocine tic
y de actividad antihistamnica H1 de bilastina tras su
administracio n unica
repetida en voluntarios sanos. XIX Congress of the Spanish
Society o
Clinical Pharmacology; 2004 Oct 28-30; Santander
17. Sologuren A, Crean C, Valiente R, et al. The drug-drug
interaction o
ketoconazole on bilastine pharmacokinetics [abstract plus poster
no. 476
Basic Clin Pharmacol Toxicol 2007; 101 Suppl. 1: 148
18. Crean C, Valiente R, Sologuren A, et al. Effect of
grapefruit juice on th
pharmacokinetics of bilastine [abstract no. 71]. J Clin
Pharmacol 2007; 47 (9
1198
19. Beal SL, Boeckmann AJ, Sheiner LB, editors. NONMEM user
guides. Sa
Francisco (CA): NONMEM Project Group, University of California,
1992
20. Levy G. Mechanism-based pharmacodynamic modelling. Clin
Pharmac
Ther 1994; 56: 356-8
21. Purohit A, Melac M, Pauli G, et al. Comparative activity of
cetirizine an
mizolastine on histamine-induced skin wheal and flare responses
at 24 h. Br
Clin Pharmacol 2002; 53: 250-4
22. Bousquet J, Chanal I, Murrieta M, et al. Lack of sensitivity
to mizolastine ove
8-week treatment. Allergy 1996; 51: 251-6
PK/PD Modelling of Bilastine 55
2009 Adis Data Information BV. All rights reserved. Clin
Pharmacokinet 2009; 48 (
-
8/22/2019 Clin. Pharmaco
12/13
23. Pinquier JL, Caplain H, Cabanis MJ, et al. Inhibition of
histamine-induced
skin wheal and flare after 5 days of mizolastine. J Clin
Pharmacol 1996; 36:
72-8
24. Devalia JL, De Vos C, Hanotte F, et al. A randomized,
double-blind cross-
over comparison among cetirizine, levocetirizine, and UCB 28557
on
histamine-induced cutaneous responses in healthy adult
volunteers. Allergy
2001; 56: 50-7
25. Dayneka NL, Garg V, Jusko WJ. Comparison of four basic
models of indirect
pharmacodynamic responses. J Pharmacokinet Biopharm 1993; 21:
457-78
26. Sharma A, Jusko WJ. Characteristics of indirect
pharmacodynamic mode
and applications to clinical drug responses. Br J Clinical
Pharmacol 1998; 45
229-39
Correspondence: Ms M. Luisa Lucero, FAES FARMA SA, Maxim
Aguirre 14, 48940, Leioa (Vizcaya), Spain.
E-mail: [email protected]
554 Jauregizar et a
2009 Adis Data Information BV. All rights reserved. Clin
Pharmacokinet 2009; 48 (
-
8/22/2019 Clin. Pharmaco
13/13