Embed Size (px)
Citation preview
Clinical and neurophysiology motivation for rehabilitation robotics
EURON Winter School on Rehabilitation Robotics, March 30th – April 4th 2008
Jane Burridge
Jane Burridge April
2008
Introduction
• Clinical and social drivers
• Basic Anatomy and Physiology
• Neuroplasticity
• Application of knowledge of neurophysiology to rehabilitation robotics
• Evidence for effectiveness
• Future work
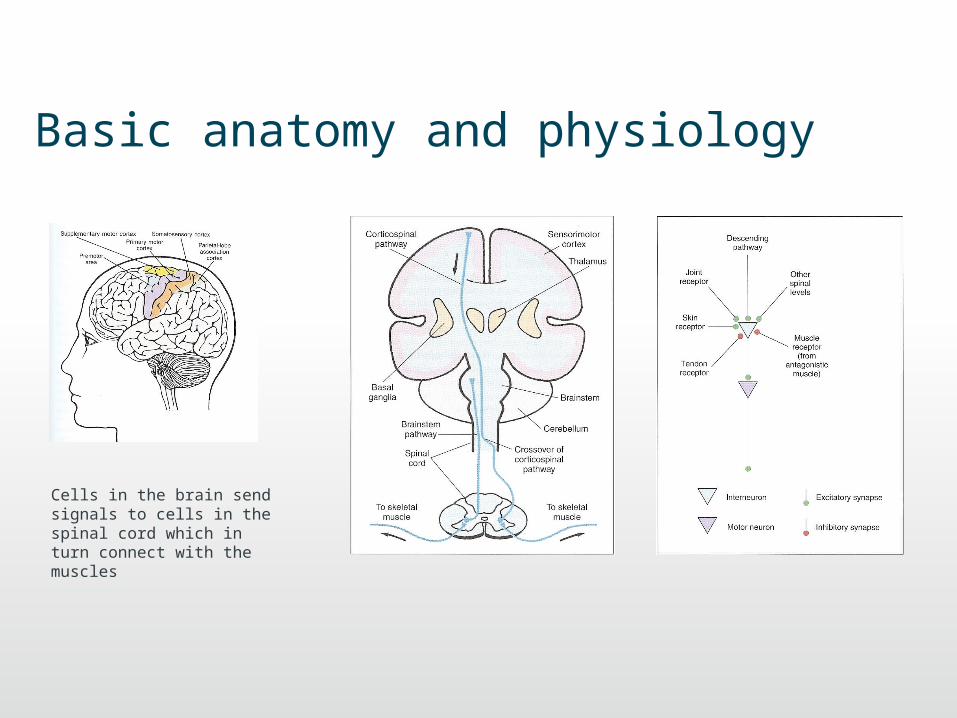
Basic anatomy and physiology
Cells in the brain send signals to cells in the spinal cord which in turn connect with the muscles
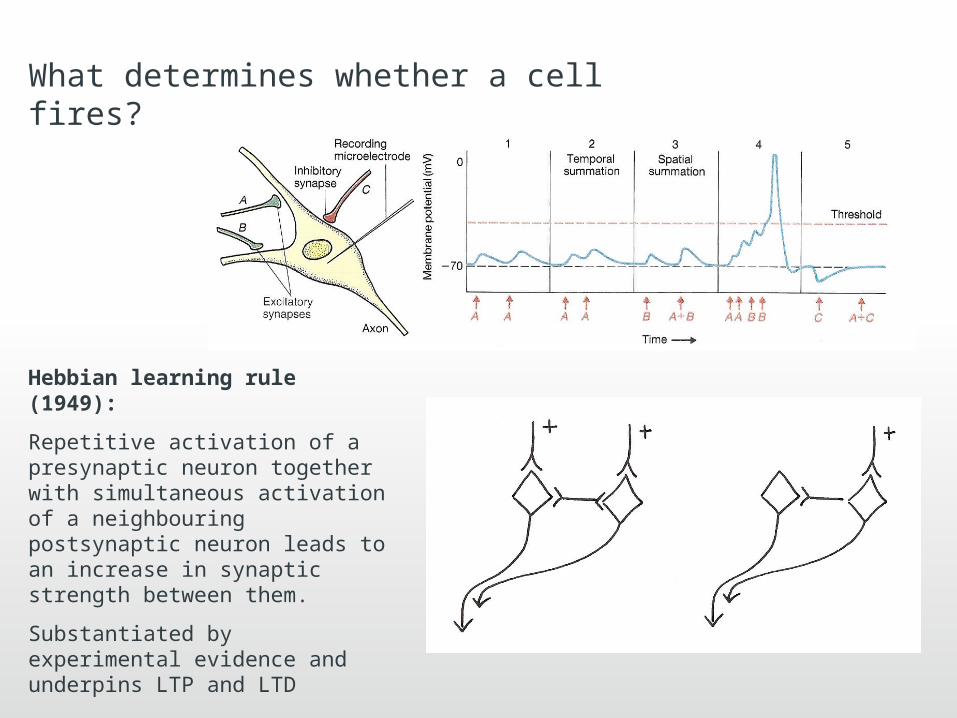
What determines whether a cell fires?
Hebbian learning rule (1949):
Repetitive activation of a presynaptic neuron together with simultaneous activation of a neighbouring postsynaptic neuron leads to an increase in synaptic strength between them.
Substantiated by experimental evidence and underpins LTP and LTD
Cortical maps – ‘use it or lose it’• Topology of the sensory and motor cortex is not fixed but flexible
and adapts to learning and experience (Donoghue 1996).
• Areas with more connections – fine motor control or more acute sensation - have larger representation
• Factors that promote change:
1. Exposure to an enriched environment after ischaemic stroke
2. Amputation of a limb results in a shrinking of the cortical representation
3. Immobilising a limb – for example in a splint results in a decrease in the cortical representation (Liepert 1995) – measured by TMS
• Increase in size is related to increase in skill
Neuroplasticity• Synaptic connections are continually being modified (re-organisation of circuitry)
– In response to demand – learning, memory, disuse– After damage to the CNS
• Cellular level
– Increased sensitivity to neural transmitters– Increase number and branches of dendrites– Increase and strengthening of synaptic connections (Hebbe)– Axon sprouting
• Behavioural level
– Declarative or explicit memory / learning (consciously aware of remembering e.g. facts)
– Non-declarative or implicit memory / learning – motor skills– Associative learning – reward, pleasure, pain – Pavlov’s dog– Non-associative learning – reflex – habituation / sensitisation
Measuring changes in CNS activity• Imaging techniques e.g. fMRI and PET
• TMS / evoked EMG potentials
• Changes following electrical stimulation
• Associated stimuli (Ridding)
• Repetitive strengthening tasks are not enough – must be goal orientated (Nudo 1992)
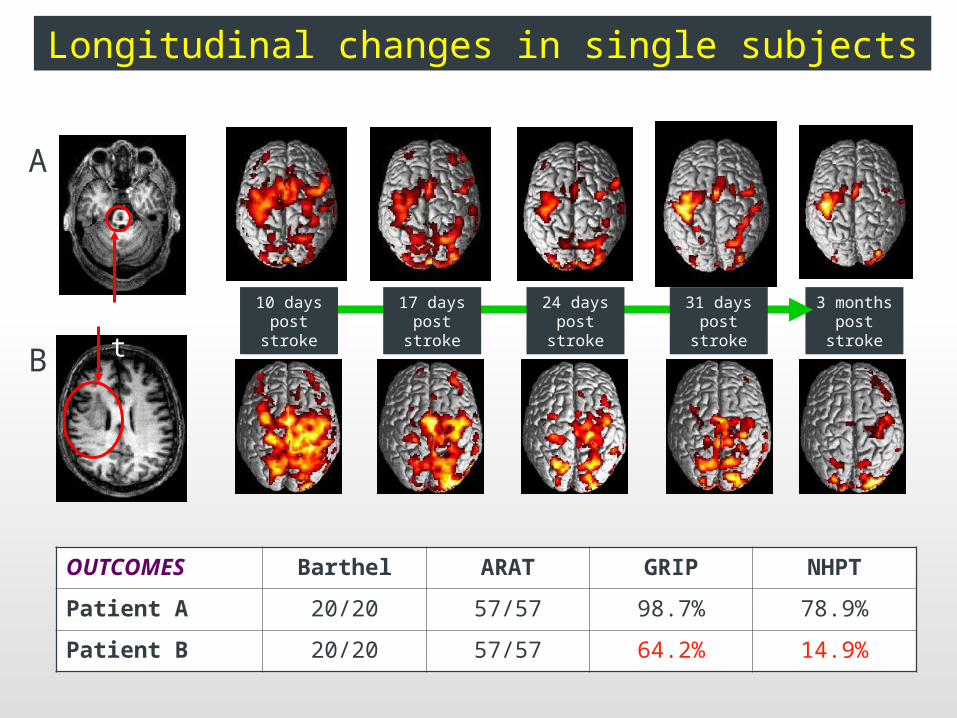
A
B
infarct3 months
post stroke17 days
post stroke24 days
post stroke31 days
post stroke10 days
post stroke
OUTCOMES Barthel ARAT GRIP NHPT
Patient A 20/20 57/57 98.7% 78.9%
Patient B 20/20 57/57 64.2% 14.9%
Longitudinal changes in single subjects
Using the signals from the cortex to drive a robot
Importance of sensory input
• Afferent feedback may be impaired
– Damage to sensory cortex and neuronal connections
– Decrease in sensory input due to deprivation of movement
– Abnormal sensory input due to abnormal postures and movement
• Sensorimotor learning
How may Sensorimotor re-learning be facilitated?• Repetition - goal orientated
• Muscle strengthening and Increased range of movement
• Modulation of spasticity
• Increased sensory input
– Intrinsic - direct stimulation of sensory fibres or secondary, proprioceptive feedback
– Extrinsic - feedback from the experience of movement or the achievement of a goal
Skill acquisition: Implicit and Explicit learning• Explicit learning:
– ‘How to’ – associated with memory, cognition etc.
– Learning may be very rapid and is tested by questioning
• Implicit learning:
– Motor skills are examples of implicit learning
– Demonstrated by ‘doing’
• Therapists often use explicit learning in training motor skills
• Evidence suggests this may not be effective (Boyd & Winstein Physical therapy Nov 2003)

What is Robot Therapy?

Application of knowledge of neuroplasticity to rehabilitation robotics• Robot will allow the patient to achieve a task
– Repetitive goal orientated practice
– Tasks can be adjusted to provide success at the limit of performance
– Motivating and varied
• Allows intensive and safe training – could be used in conjunction with CIMT (shaping) and could incorporate VR or interaction with computer games
• Appropriate for all levels of ability
Examples of upper limb robotic training systems
• 2D (e.g. MIT Manus) and 3D systems (e.g. Gentle/s) with mechanical active-assisted / progressive-resisted training
• 3D un-weighing systems (Armeo)
• Bilateral arm systems for wrist flex/ext and pro/sup (Bi-Manu-Track)
• Systems that augment error or distort reality (see: Johnson 2005, Patten 2006 and Tang 2007)
What is the evidence for Robot Therapy ?
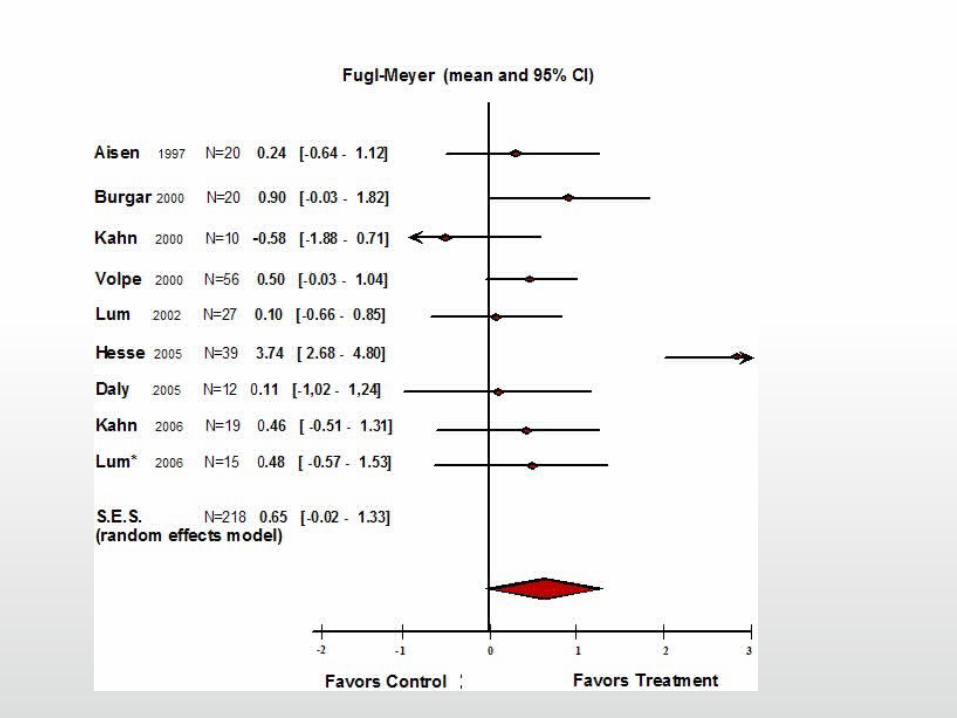
•Strong evidence for improved motor control (impairment) and some evidence for improved function [Kwakkel 2008, EBRSR & Prange 2006]
•Proximal training = proximal benefit
•Potential for combining functional training with robot training
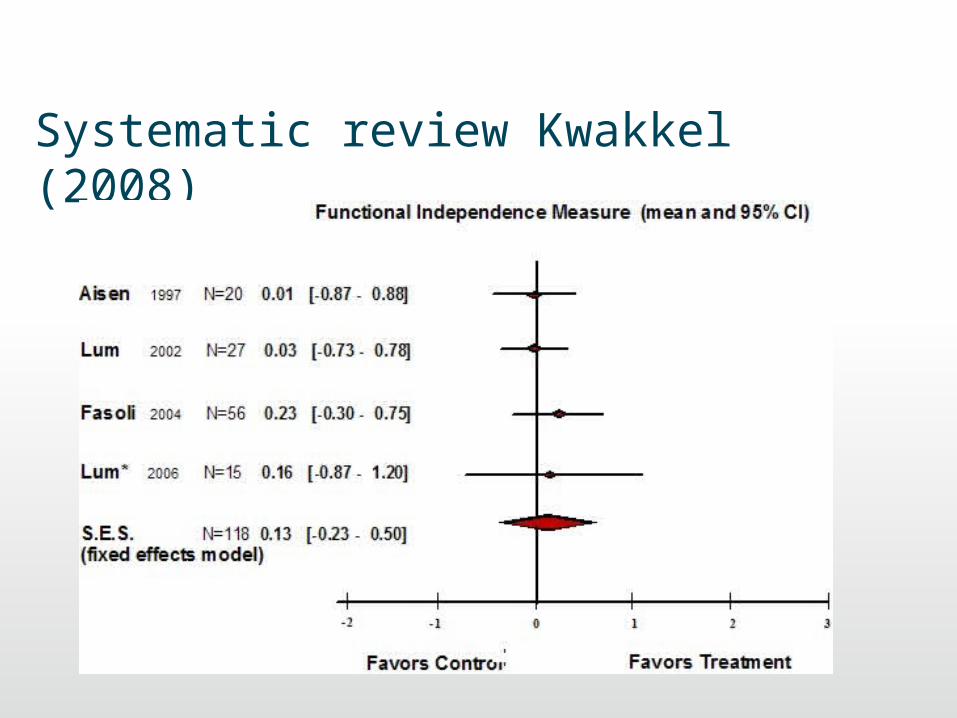
Systematic review Kwakkel (2008)
For upper limb rehabilitation post-stroke to advance we need better outcome measures
• Measurement in clinical practice vs. research
• Functional / behavioural vs. impairment or system level measurement
• Understand mechanisms associated with loss and recovery of function
• Optimise patient selection and decision making in clinical practice
• Systematic basis for the advancement of rehabilitation
– Measure the effect of therapy
– Evaluate new therapies
Future work• Including the wrist and hand
• Wearable robots
• Complex interventions
– with FES– with CIMT– with functional tasks– with pharmacological interventions that regulate the production of
neurotransmitters, promote LTP, neural sprouting and synaptogenesis
• At what stage of rehabilitation?
– Recent evidence that too soon may be detrimental– Improvement even late post-stroke
• What dose?
• Characteristics of patients likely to respond well?
• Better understanding of the mechanisms associated with change in function
Using iterative learning control to modulate electrical stimulation (ES) in a robot workstation tracking task
• 2D pursuit tracking task
• Using ES rather than mechanical error correction
• ILC ensures that minimal ES is applied
• Associated stimuli: voluntary cortical drive and ES
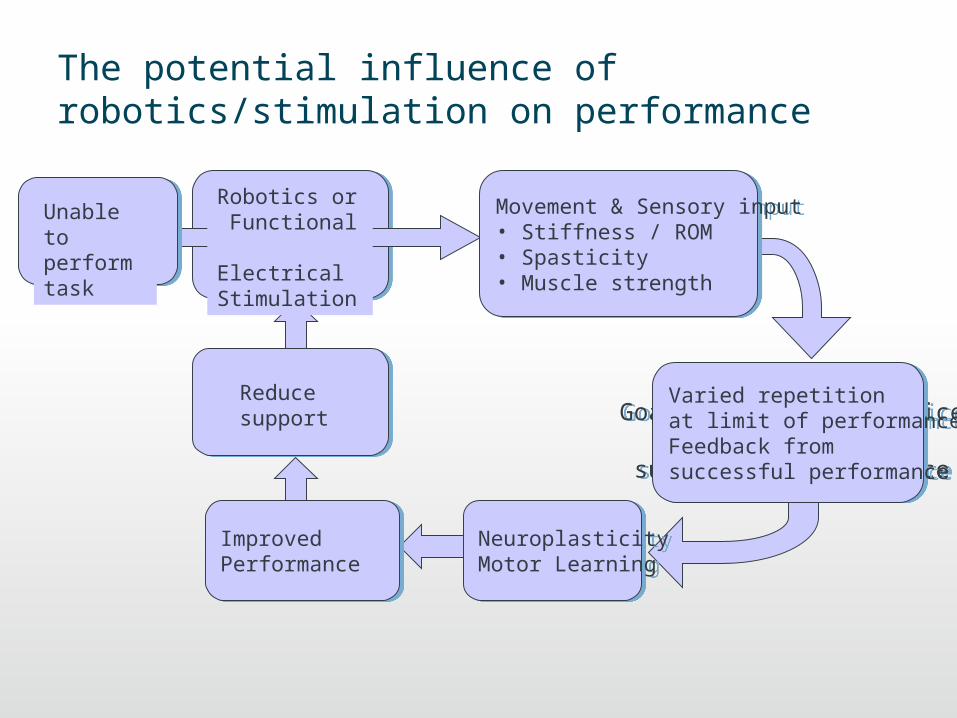
The potential influence of robotics/stimulation on performance
RepetitionGoal orientated practice
Feedback from successful performance
RepetitionGoal orientated practice
Feedback from successful performance
Robotics or Functional Electrical Stimulation
Movement & Sensory input • Stiffness / ROM • Spasticity• Muscle strength
Movement & Sensory input • Stiffness / ROM • Spasticity• Muscle strength
Improved PerformanceImproved Performance
Neuroplasticity Motor LearningNeuroplasticity Motor Learning
Varied repetitionat limit of performanceFeedback from successful performance
Varied repetitionat limit of performanceFeedback from successful performance
Reduce support
Unable to perform task
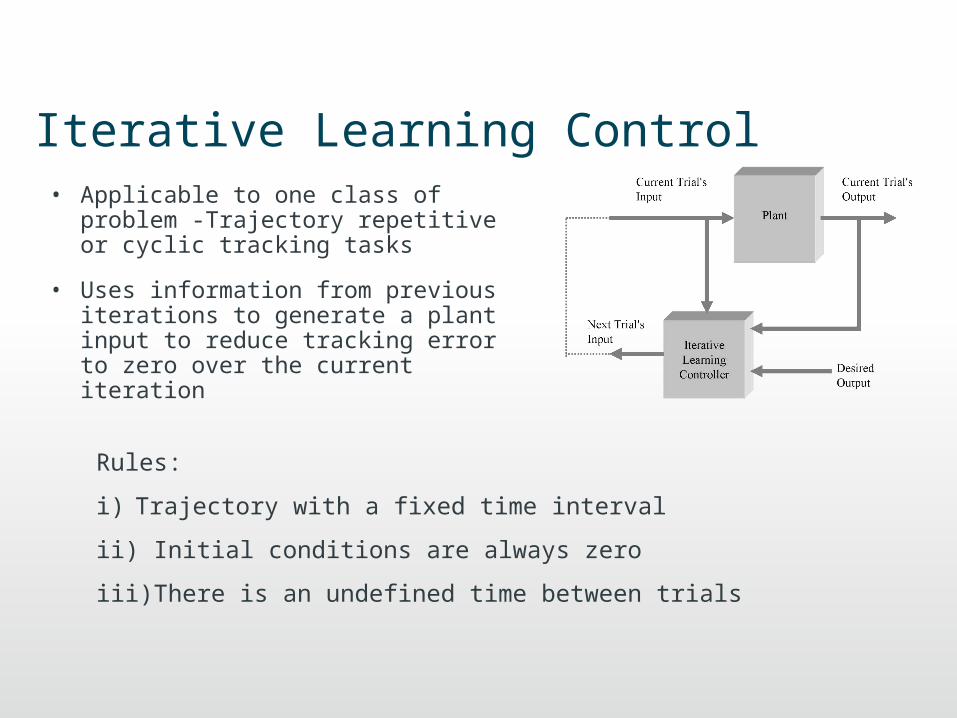
Iterative Learning Control• Applicable to one class of
problem -Trajectory repetitive or cyclic tracking tasks
• Uses information from previous iterations to generate a plant input to reduce tracking error to zero over the current iteration
Rules:
i) Trajectory with a fixed time interval
ii) Initial conditions are always zero
iii) There is an undefined time between trials
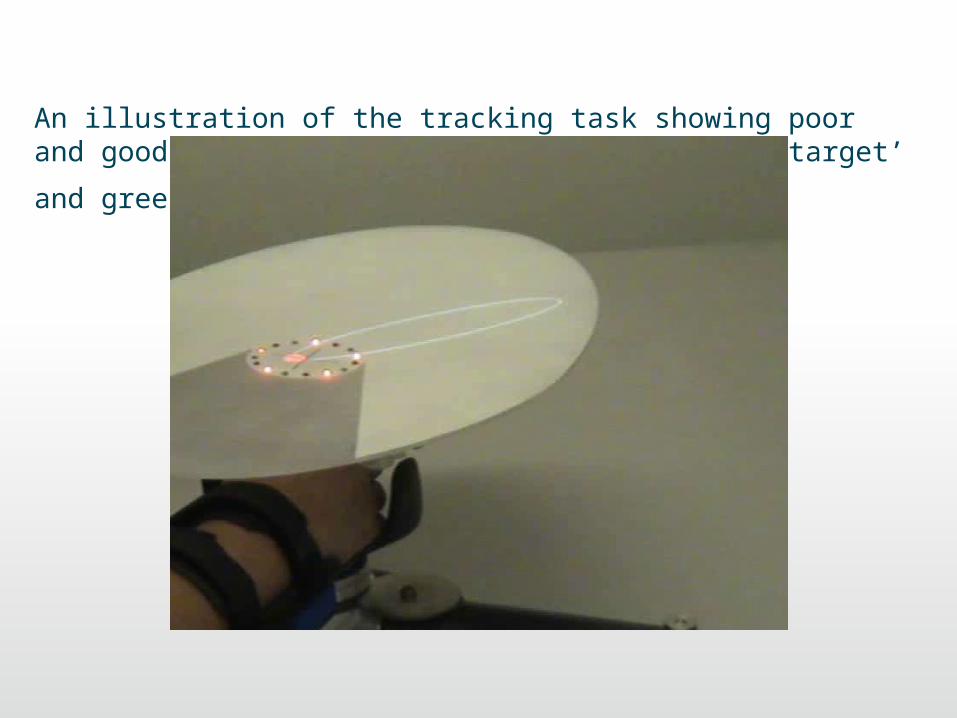
An illustration of the tracking task showing poor and good performance. Red LEDs indicate ‘off target’ and green ‘on
target’
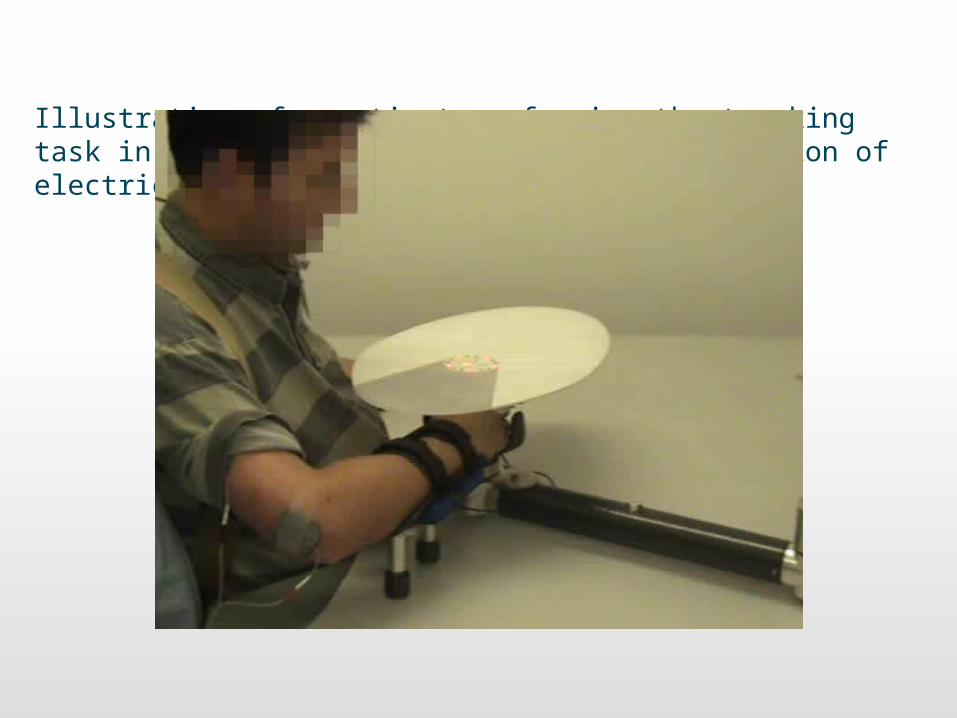
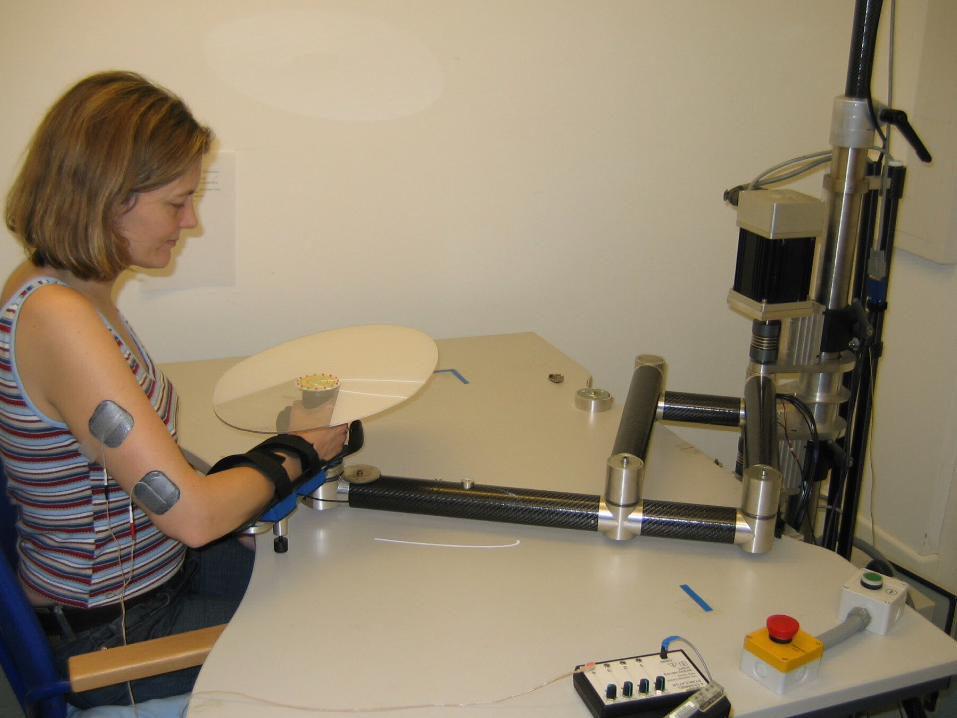
Illustration of a patient performing the tracking task in the robot with and without ILC mediation of electrical stimulation of triceps
Method
• The workstation uses a robotic arm to:
1) Constrain the arm to move in the horizontal plane 2) Recreate the effect that the subject is moving a simple
point mass with damping 3) Provide additional assistance if error cannot be reduced by
FES
• Elliptical trajectories are projected onto a target above the patient’s hand
• FES to triceps for elbow extension
• ILC is used to modulate stimulation output (timing and pulse-width) using an algorithm that uses data from all previous trials of the task
• Minimal stimulation is applied to encourage voluntary effort
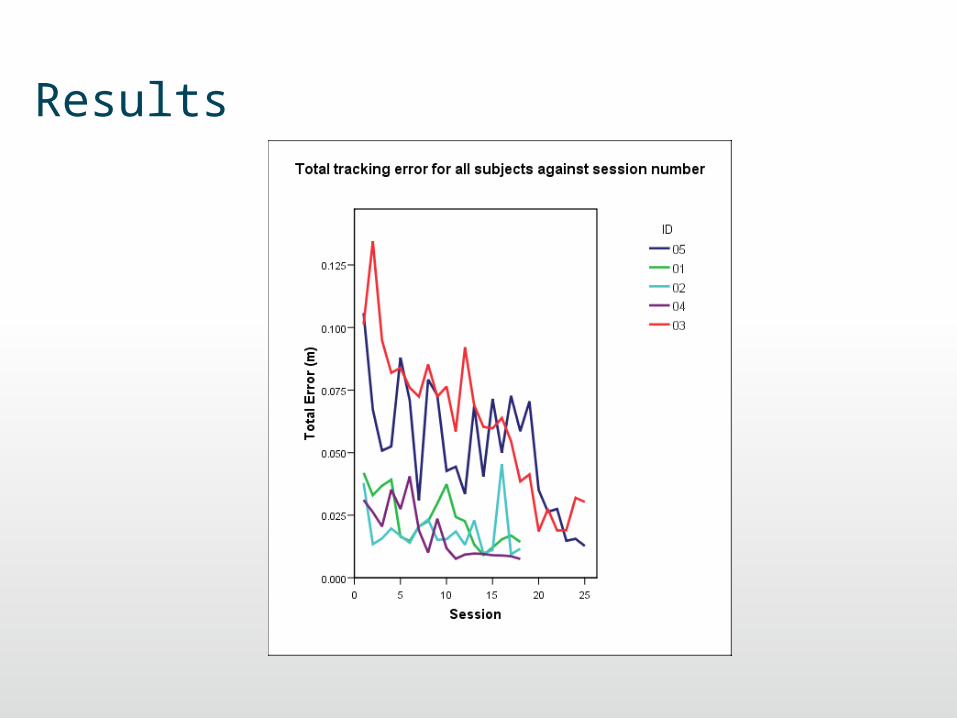
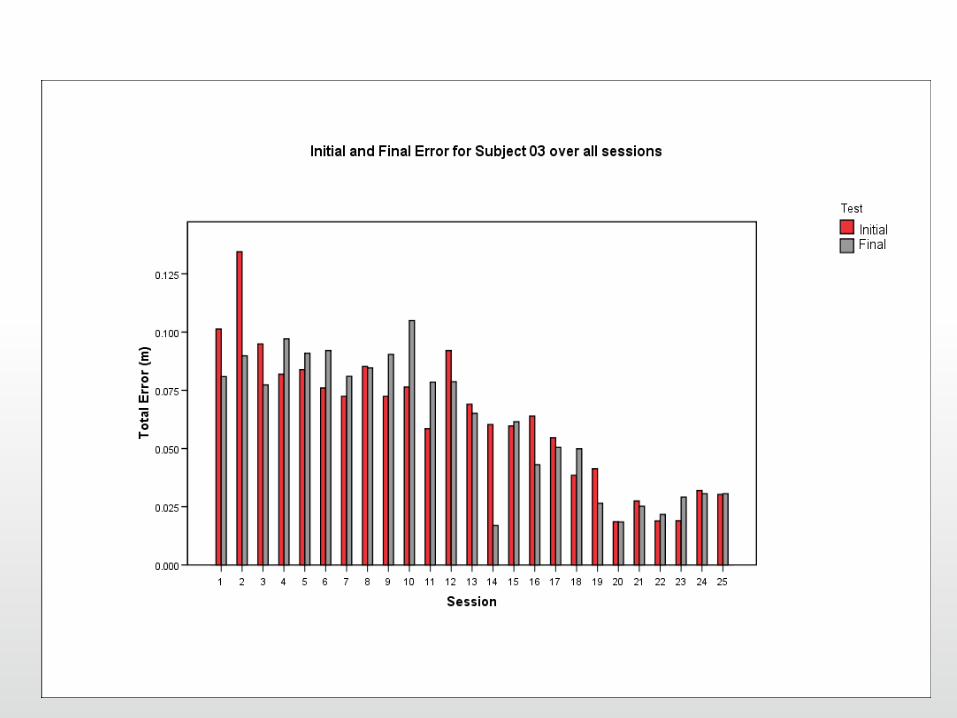
Results
Conclusion
Early results suggested iterative learning control mediated by FES could be used to enable normal subjects to accurately track a trajectory within six iterations
Preliminary analysis of results with stroke patients suggests that motor tracking is improved over a course of 18 sessions
Future Work
If successful the concept could be used for other neurological conditions, such as cerebral palsy and incomplete spinal cord injury

Summary• Clinical and social drivers
• Evidence that intensive practice leads to better outcomes
• Evidence for neuroplasticity in animal models has been demonstrated in human subjects
• Neuroplastic changes are associated with improved function
• Augmented therapy using rehabilitation robots shows evidence for improved motor control
• Complex interventions may add value to improve functional outcomes





























