Embed Size (px)
Citation preview

612
Clinical Correlates of Doppler/UltrasoundErrors in the Detection of Internal Carotid
Artery Occlusion
Samuel L. Bridgers, MD
One recognized limitation of carotid Doppler/uitrasound is its accuracy in differentiatingocclusion from near-total occlusion of the internal carotid artery, which is a crucial issue inmanagement decisions. Clinical histories were reviewed in 58 patients with apparent occlusionof an internal carotid artery diagnosed by Doppler/uitrasound who also underwent angiogra-phy. False-positive results were detected in eight patients, for an overall accuracy of 86%.Among a group of 25 patients with acute cerebral or ocular events ipsilateral to an apparentlyoccluded artery, false-positive results occurred in seven (accuracy of 72%). Among a group of33 patients with asymptomatic or remotely symptomatic apparent occlusions, only onefalse-positive occurred, for an accuracy of 97%. This difference in accuracy between groups wassignificant. Thus, a Doppler/uitrasound diagnosis of occlusion was most inexact in those patientsfor whom the detection of continued patency was most likely to influence management. (Stroke1989;20:612-615)
Ultrasound examination of the carotid arter-ies has become a standard procedure forevaluating patients with suspected carotid
or cerebrovascular disease. With increasing techni-cal sophistication and clinical experience, carotidDoppler/uitrasound has become a substitute forcarotid angiography in the minds of many who usethe former. However, comparative studies of thetwo have demonstrated consistent limitations to theaccuracy of Doppler/ultrasound. One problematicarea has been the differentiation of an occludedinternal carotid artery from one that is severelystenotic.'-4 Definition of different levels of accuracyfor detecting internal carotid artery occlusion invarying clinical circumstances would allow the cli-nician attempting to base management decisions onDoppler/uitrasound information to know when toaccept that information with reasonable confidenceand when to regard it with suspicion.
Subjects and MethodsThis study was conducted through the Neurovas-
cular Laboratory of the Stroke Unit, NeurologyService, Veterans Administration Medical Center,
From the Neurology Service, Veterans Administration Medi-cal Center, West Haven and the Department of Neurology, YaleUniversity School of Medicine, New Haven, Connecticut.
Address for correspondence: Samuel L. Bridgers, MD, Neu-rology Service (127), VA Medical Center, West Spring Street,West Haven, CT 06516.
Received August 19, 1988; accepted November 16, 1988.
West Haven, Connecticut. Clinical circumstancessurrounding carotid Doppler/ultrasound examina-tion were reviewed in all patients with internalcarotid artery occlusion identified by Doppler/ultra-sound who also underwent carotid angiography.Fifty-eight such men were identified in 5Yi years.During this time, 123 patients were diagnosed byultrasound as having internal carotid artery occlu-sion. The 65 who did not undergo angiographyincluded patients in whom no possibility of surgicalintervention existed, patients unwilling to undergoangiography, and patients whose referring physi-cian believed angiography was not indicated.
Carotid Doppler/ultrasound examinations wereperformed using a mechanically aligned and elec-tronically switchable real-time B-mode two-dimensional imaging system with a 7.5-MHz trans-ducer (High Stoy SP1200B, Lake Success, NewYork) and a 4-MHz continuous-wave Doppler trans-ducer. Thus, the Doppler beam was aimed in align-ment with the B-mode image, although this was nota typical duplex system with B-mode and pulsedDoppler signals emanating from the same trans-ducer. Ultrasound examinations were performed byeither of two trained and experienced neurologists.Occlusion of the internal carotid artery was identi-fied contingent on the recognition of a Dopplersignal without diastolic flow in the common carotidartery, failure to obtain any Doppler signal from thevicinity of an internal carotid artery lumen identifi-able on B-mode imaging, and longitudinal move-
by guest on May 19, 2018
http://stroke.ahajournals.org/D
ownloaded from

Bridgers Clinical Correlates of Doppler Errors 613
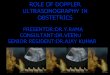
FIGURE 1. Typical results ofDopplerlultrasound examina-tion of occluded internalcarotid artery. A: Commoncarotid artery Doppler flowsignal with no diastolic com-ponent. No internal carotidartery signal was detected.Horizontal calibrations repre-sent 0.1 second; vertical cali-brations represent 1 KHz. B:Real-time two-dimensionalimage with transducer in pos-terolateral position revealingno obvious evidence of signif-icant lesion in proximal inter-nal carotid artery. C: Angiog-raphy (lateral view) revealingocclusion of internal carotidartery.
ment of the artery coinciding with the cardiac cycle(Figure 1). Others have confirmed these criteria foridentifying occlusion of the internal carotid artery.45
Angiographic examinations included selectivecarotid injections in all but three patients, in whomdigital intravenous angiography was performed.
ResultsAngiography confirmed the Doppler/ultrasound
diagnosis of occlusion in 50 of the 58 patients (86%).Among eight angiographically patent arteries that
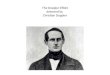
appeared to be occluded by Doppler, the presenceof near-total occlusion was demonstrated by angi-ography in seven. Figure 2 illustrates a typicalexample. In the single patient without disease, theapparently occluded artery turned deep and awayfrom the bifurcation at nearly a right angle. Thisanomaly, coupled with an absent diastolic signal inboth carotid systems presumably related to lowcardiac output, was believed to explain the Doppler/ultrasound error.
Correlations between the circumstances leadingto a Doppler/ultrasound examination and the accu-racy of a diagnosis of carotid occlusion are indi-cated in Table 1. Twenty-five of the 58 patientswere referred for Doppler/ultrasound during thecourse of hospital admissions for acute ischemicevents attributable to the vascular territory of theartery found to be occluded by noninvasive testing.The remainder were similarly distributed amongpatients with no history of cerebrovascular disease,patients who had been admitted for acute symptomsthat could not be attributed to the apparentlyoccluded artery, and patients who had experienced
remote symptoms attributable to the apparentlyoccluded artery. Patients with acute ipsilateral eventswere significantly more likely to receive a false-positive Doppler/ultrasound diagnosis of occlusionthan other patients (p=0.016, Fisher's exact test).This appeared to be largely represented in thosepatients with acute hemispheric ischemic events(p=0.006, Fisher's exact test), while the false-positive rate in patients with acute ipsilateral ocularevents was not significantly different from that inpatients with no acute ipsilateral symptoms. One ofthe patients in the ocular-event subgroup was theone in whom angiography revealed no significantcarotid disease. A more stringent comparison ofpatients with acute ipsilateral symptoms to thosewith no ipsilateral symptoms at any time still yieldeda significant increase in false-positive results amongthe former (p=0.021, Fisher's exact test).
DiscussionAlthough the surgical approach to management of
internal carotid artery disease has been subjected torecent criticism, it is widely practiced.6-7 The great-est unanimity surrounds a tightly stenotic internalcarotid artery associated with ipsilateral mild ortransient events. Even in an asymptomatic patient,the discovery of a very tight stenosis often results inendarterectomy. These tightest of carotid lesions areregarded as unstable and dangerous. Once an arteryhas occluded completely, however, it is regarded asless of a risk.8 At any rate, it is no longer certain tobe amenable to surgical intervention.
If carotid surgery is to be considered, the suredifferentiation of tightly stenotic from occluded inter-
by guest on May 19, 2018
http://stroke.ahajournals.org/D
ownloaded from

614 Stroke Vol 20, No 5, May 1989
FIGURE 2. False-positiveDoppler/ultrasound diagnosis ofoccluded internal carotid artery.A: Common carotid arteryDopplerftow signal with no dia-stolic component. No internalcarotid signal was detected.Horizontal calibrations repre-sent 0.1 second; vertical cali-brations represent 1 KHz. Real-time two-dimensional imagewas similar to that in FigureIB. B: Contralateral commoncarotid artery Dopplerftow sig-nal with well-defined diastolicDoppler shift. C: Angiography(anterior view) revealing near-occlusion of internal carotidartery just above bifurcation.
nal carotid arteries becomes crucial. If noninvasivemethods are expected to make this differentiation,their limitation must be known. In our hands, carotidultrasound has been far from perfect in this regard.The reasonably consistent nature of mistakes madesuggests that this reflects technical limitations, ratherthan human error. While it might be suspected thatthe use of continuous-wave Doppler rather than oneof the currently popular pulsed-Doppler duplexdevices influenced the results, previous comparisonsof both techniques with angiography have indicatedsimilar results with the two Doppler techniques4 orsuperior performance for this specific purpose withcontinuous-wave Doppler.9
TABLE 1. Correlation of Clinical Circumstances and Doppler/Ultrasound Remits
Clinical circumstances
All patientsAcute ipsilateral events
HemisphericStrokeTransient ischemic attack
OcularNo acute ipsilateral event
AsymptomaticEvent outside territoryRemote ipsilateral event
n
5825
14104
1133
12119
False-positiveresults
No.8753221100
%
1428363050183800
%of n.
This report differs from previous comparisons ofcarotid Doppler/ultrasound and angiography by plac-ing the detection of a specific error in a specificclinical context. The overall false-positive rate of14% is consistent with that reported by others,1410
yet division of patients into those with and thosewithout acute events appropriate to the apparentlyoccluded artery reveals distinct and very discrepantlevels of accuracy. The data indicate that the differ-entiation of a minimally patent from a totallyoccluded internal carotid artery by Doppler/ultra-sound is least reliable in the clinical situation inwhich that differentiation is most likely to affectmanagement—in the setting of acute ipsilateral symp-toms. On the other hand, when carotid occlusion isan incidental finding on ultrasound, it is very likely tobe correct. The current results are consistent withthe 97% accuracy in Doppler/ultrasound diagnosis ofcarotid occlusion achieved in the longitudinal studyof asymptomatic patients reported by Roederer etal," in contrast to the general experience in unse-lected patients reported by that group1 and others.Presumably, very tight stenosis is difficult to differen-tiate from occlusion, regardless of the clinical circum-stances, and it is the increased likelihood of encoun-tering very severe stenosis in the setting of acuteipsilateral symptoms that leads to the discrepancy.
Without acute ipsilateral symptoms, the likeli-hood that a decision for angiography will provebeneficial to the patient with apparent occlusion byDoppler/ultrasound is very low. Nevertheless, angi-ography will always be necessary when the diagno-
by guest on May 19, 2018
http://stroke.ahajournals.org/D
ownloaded from

Bridgers Clinical Correlates of Doppler Errors 615
sis of internal carotid artery stenosis must be madewith certainty. The current results also provide auseful context for judging studies that seek to definethe clinical correlates of carotid occlusion. Somesuch studies already have relied, at least in part, onDoppler/ultrasound alone in classifying carotidlesions.l213 It is important to recognize that a groupof acutely symptomatic patients with internal carotidartery occlusion so defined probably will include asignificant portion with still-patent arteries, whereasa group of asymptomatic patients probably will not.
AcknowledgmentsSome of the Doppler/ultrasound examinations
reviewed in this study were performed by JanWallace, MD. Statistical analysis was provided byEmmanuel Lerner, MS.
References1. Fell G, Phillips DJ, Chikos PM, Harley JD, Thiele BL,
Strandness DE: Ultrasonic duplex scanning for disease ofthe carotid artery. Circulation 1981 ;64:1191-1195
2. Zweibel WJ, Crummy AB: Sources of error in Dopplerdiagnosis of carotid occlusive disease. Am J Neuroradiol1981 ;2:231-242
3. Levien LJ, Voll CL, Lithgow-Jolly P, Fritz VU: The valueof noninvasive investigation in the diagnosis of total occlu-sion of the internal carotid artery. Stroke 1985;16:945-949
4. Bomstein NM, Beloev ZG, Norris JW: The limitations ofdiagnosis of carotid occlusion by Doppler ultrasound. AnnSurg 1988;207:315-317
5. Bodily KC, Phillips DJ, Thiele BL, Strandness DE: Nonin-vasive detection of internal carotid occlusion. Angiology1981^32:517-521
6. Dyken ML: Carotid endarterectomy studies: A glimmeringof science. Stroke 1986;17:355-358
7. Winslow CM, Solomon DH, Chassin MR, Kosecoff J, Mer-rick NJ, Brook RH: The appropriateness of carotid endar-terectomy. N Engl J Med 1988;3l8:721-727
8. Furlan AJ, Whisnant JP, Baker HL: Long term prognosisafter carotid artery occlusion. Neurology 1980;30:986-988
9. Hennerici M, Freund HJ: Efficacy of continuous-wave Dopp-ler and duplex system examinations for the evaluation ofextracranial carotid disease. J Clin Ultrasound 1984;12:155-161
10. Brown PM, Johnston KW, Douvill Y: Detection of occlusivedisease of the carotid artery with continuous wave Dopplerspectral analysis. Surg Gynecol Obstet 1982;155:183-186
11. Roederer GO, Langlois YE, Jager KA, Primozich JF, BeachKW, Phillips DJ, Strandness DE: The natural history ofcarotid arterial disease in asymptomatic patients with cervi-cal bruits. Stroke 1984;I5:6O5-613
12. Ringlestein EB, Zeumer H, Angelou D: The pathogenesis ofstrokes from internal carotid artery occlusion. Diagnosticand therapeutic implications. Stroke 1983; 14:867-875
13. Bogousslavsky J, Regli F: Borderzone infarctions distal tointernal carotid artery occlusion: Prognostic implications.Ann Neurol 1986;20:346-350
KEY WORDS • carotid artery diseases • ultrasonics
by guest on May 19, 2018
http://stroke.ahajournals.org/D
ownloaded from

S L Bridgersocclusion.
Clinical correlates of Doppler/ultrasound errors in the detection of internal carotid artery
Print ISSN: 0039-2499. Online ISSN: 1524-4628 Copyright © 1989 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Stroke doi: 10.1161/01.STR.20.5.612
1989;20:612-615Stroke.
http://stroke.ahajournals.org/content/20/5/612World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://stroke.ahajournals.org//subscriptions/
is online at: Stroke Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer available in the
Permissions in the middle column of the Web page under Services. Further information about this process isOnce the online version of the published article for which permission is being requested is located, click Request
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Stroke Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on May 19, 2018
http://stroke.ahajournals.org/D
ownloaded from