Embed Size (px)
Citation preview
CPHC Clinical Guidelines 2018
Page 1 of 24
CLINICAL GUIDELINES for Physiotherapists working with persons with Bleeding Disorders:
Appendix/companion document for
CPHC Standards of Physiotherapy Care for Persons with Bleeding Disorders
2018
These guidelines were developed by the Standards working group to augment the CPHC Standards and provide clinical guidance. The working group members were:
Kathy Mulder, Winnipeg Elia Fong, Edmonton Erin McCabe, Edmonton Julia Brooks, Calgary Karen Strike, Hamilton Pam Hilliard, Toronto Sandra Squire, Vancouver Marie-Eve Toussaint, Montreal, Anne Ducharme, Montreal
CPHC Clinical Guidelines 2018
Page 2 of 24
CPHC Clinical Guidelines
Index
Standard 1: The PT is a core team member…………………………………..3
Standard 2: PT assessment of acute injuries…………………………………5
Standard 3: Physiotherapy Treatment after:
3A Acute Injury………………………………………………………….....8
3B Surgery………………………………………………………………..10
Standard 4: The Annual Assessment…………………………………………13
Standard 5: PT Treatment of Musculoskeletal Complications……………..17 Standard 6: Consultation with other care providers…………………………19
Standard 7: Education and health promotion………………………………..20
Standard 8: Continuing Competence…………………………………………22
CPHC Clinical Guidelines 2018
Page 3 of 24
Guidelines for Standard 1: The PT is a core team member Each Canadian comprehensive bleeding disorders care team includes a physiotherapist with protected time dedicated specifically to the Bleeding Disorders program (1, 2).
A physiotherapist is involved in the care of the PWBD from the time of diagnosis
and will participate in the Assessment, Treatment, and Education throughout the
person’s lifespan (1,2,3)
1.1 Assessment includes:
Baseline and longitudinal assessments throughout the lifespan (1,2) Determining the site of an acute bleed and assisting with differential diagnosis
(e.g. joint bleed vs muscle bleed; synovitis vs hemarthrosis; superficial soft tissue bleed vs muscle bleed) (2)
Pre-operative and post-operative assessments (1,2,3)
1.2 Treatment includes management and rehabilitation of all musculoskeletal complications and sequelae of hemophilia (1, 2, 3) including
Acute bleeds Acute and Chronic synovitis Chronic arthropathy Pain Limitations of Function and Participation Post-operative rehabilitation
Also see Guidelines for treatment for Standard 3 and Standard 5.
1.3 Education includes information provided to
Patients and families regarding prevention, identification and management of bleeds and the musculoskeletal complications of bleeding disorders (1,2,3)
Patients and families regarding healthy active lifestyle throughout the lifespan (1,2,3)
School personnel with respect to the appropriate activities for the PWBD, and activity modifications that may be necessary to allow safe participation
All people who are responsible for the patient’s safety, such as babysitters,
teachers, coaches, etc. re: appropriate immediate treatment of a suspected bleed (1,2)
Other core team members regarding identification and management of musculoskeletal complications of bleeding disorders (2)
Other physiotherapists re: management of PWBD (2)
CPHC Clinical Guidelines 2018
Page 4 of 24
References: 1. Srivastava A, Brewer AK, Mauser‐Bunschotten E, et al. (Treatment Guidelines Working
Group) Guidelines for the management of hemophilia. Haemophilia 2013; 19 31‐e47
and available at http://www.wfh.org/en/resources/wfh‐treatment‐guidelines (accessed
March 14, 2018)
2. Canadian Hemophilia Standards Group. Canadian Comprehensive Care Standards for
Hemophilia and other Inherited Bleeding Disorders. First Edition. 2007
http://www.hemophilia.ca/en/care‐and‐treatment/comprehensive‐care‐standards/
accessed March 14, 2018
3. Lobet S, Hermans C, Lambert C. Optimal management of hemophilic arthropathy and hematomas. Journal of Blood Medicine 2014:5 207–218
CPHC Clinical Guidelines 2018
Page 5 of 24
Guidelines for Standard 2: PT assessment of acute injuries The Physiotherapist participates in the assessment of acute musculoskeletal bleeds.
2.1 Musculoskeletal bleeding is a key characteristic of many bleeding disorders and can result in permanent damage to the joints and muscles (1,2). Accurate diagnosis is the key to ensuring correct treatment.
The earliest symptom of a musculoskeletal bleed is pain BUT not all pain is due to bleeding (3,4).
Symptoms of some musculoskeletal bleeds can mimic other conditions (e.g. psoas bleed presenting like appendicitis) (5)
2.2 Assessment of acute bleeds should include: 2.2.1 History of present condition
details of bleed onset and progression of symptoms mechanism of injury factor replacement given to date and response to treatment other treatment (first aid) used and response to treatment pain qualities, location, intensity, aggravating/alleviating factors pain with movement
2.2.2 Past medical history recent joint or muscle bleeds previous target joints; location and number usual activities usual factor replacement regime and usual response to treatment
2.2.3 Specific objective criteria – least invasive first. Observation/inspection: posture, bruising** (see notes below), swelling,
redness Active Movement:
compare to contralateral limb or baseline measurements on file is there pain with movement? Location?
Palpation: warmth, swelling, tenderness, spasm, paresthesis Testing:
Joints: end feel (within limits of pain) Muscles:
muscle length especially two-joint muscles pain and/or weakness with active contraction
Sensation especially if nerve compression is suspected
CPHC Clinical Guidelines 2018
Page 6 of 24
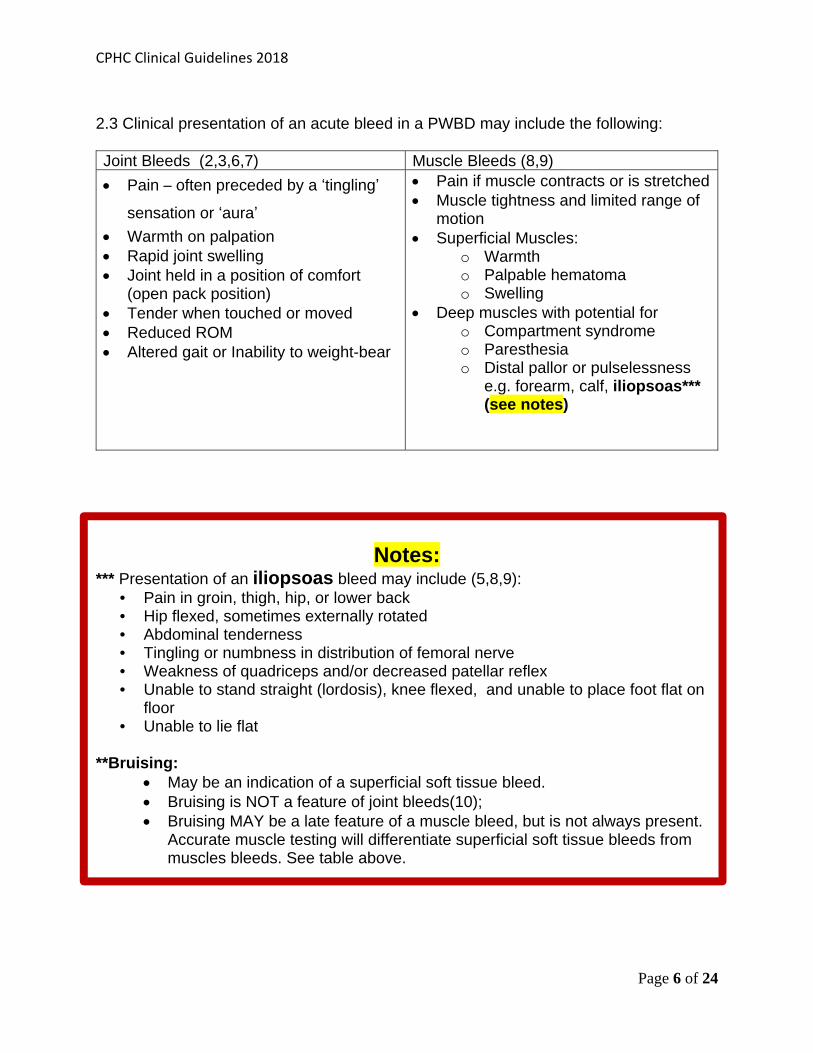
2.3 Clinical presentation of an acute bleed in a PWBD may include the following: Joint Bleeds (2,3,6,7) Muscle Bleeds (8,9)
Pain – often preceded by a ‘tingling’ sensation or ‘aura’
Warmth on palpation Rapid joint swelling Joint held in a position of comfort
(open pack position) Tender when touched or moved Reduced ROM Altered gait or Inability to weight-bear
Pain if muscle contracts or is stretched Muscle tightness and limited range of
motion Superficial Muscles:
o Warmth o Palpable hematoma o Swelling
Deep muscles with potential for o Compartment syndrome o Paresthesia o Distal pallor or pulselessness
e.g. forearm, calf, iliopsoas*** (see notes)
Notes: *** Presentation of an iliopsoas bleed may include (5,8,9):
• Pain in groin, thigh, hip, or lower back • Hip flexed, sometimes externally rotated • Abdominal tenderness • Tingling or numbness in distribution of femoral nerve • Weakness of quadriceps and/or decreased patellar reflex • Unable to stand straight (lordosis), knee flexed, and unable to place foot flat on
floor • Unable to lie flat
**Bruising:
May be an indication of a superficial soft tissue bleed. Bruising is NOT a feature of joint bleeds(10); Bruising MAY be a late feature of a muscle bleed, but is not always present.
Accurate muscle testing will differentiate superficial soft tissue bleeds from muscles bleeds. See table above.
CPHC Clinical Guidelines 2018
Page 7 of 24
2.4 Clinical assessment is usually sufficient to make the diagnosis. Ultrasound or other imaging techniques, if available, can be helpful to confirm the size and location of the hematoma and monitor resolution (4). There is increasing use of point of care ultrasound in Canadian HTCs to corroborate clinical assessment and monitor recovery (11). 2.5 Assessment findings and PT treatment plan should be communicated to the relevant other team members. References:
1. Knobe K and Berntorp E. Haemophilia and joint disease: pathophysiology, evaluation, and management. Journal of Comorbidity 2011; 1:51‐59.
2. Lobet S, Hermans C, Lambert C. Optimal management of hemophilic arthropathy and hematomas. Journal of Blood Medicine 2014:5 207–218
3. Flood E, Pocoski J,. Michaels LA, McCoy A, Beusterien K, Sasan R. Patient‐reported experience of bleeding events in haemophilia. European Journal of Haematology 93 Suppl. 75 (19–28)
4. Ceponis A, Wong‐Sefidan I, Glass CS, Von Drygalski A. Rapid musculoskeletal ultrasound for painful episodes in adult haemophilia patients. Haemophilia (2013), 19, 790–798
5. Srivastava A, Brewer AK, Mauser‐Bunschotten E, et al. (Treatment Guidelines Working Group) Guidelines for the management of hemophilia. Haemophilia 2013; 19 31‐e47 and available at http://www.wfh.org/en/resources/wfh‐treatment‐guidelines (accessed March 14, 2018)
6. Simpson ML, Valentino LA. Management of joint bleeding in hemophilia. Expert Rev. Hematol 2012 Aug;5(4):459‐68.
7. Blanchette VS, Key NS, Ljung LR, Manco‐Johnson MJ, van Den Berg HM, Srivastava A, for the Subcommittee on Factor VIII, Factor IX and Rare Coagulation Disorders. Definitions in hemophilia: communication from the SSC of the ISTH. J Thromb Haemost 2014;12:1935–9.
8. Sorenson B, Benson GM, Bladen M, Classey S, Keeling DM, McLaughlin P, Yee, TT, Makris M. Management of muscle hematomas in patients with severe hemophilia in an evidence‐poor world. Hemophilia 2012.18:598‐606
9. Balkan, C., Kavakli, K. and Karapinar, D. Iliopsoas haemorrhage in patients with haemophilia: results from one centre. Haemophilia 2005, 11: 463–467.
10. Ota S, McLimont M, Carcao MD, Blanchette VS, Graham N, Paradis E, Feldman BM. Definitions for haemophilia prophylaxis and its outcomes: The Canadian Consensus Study. Haemophilia 2007 13: 12–20.
11. Lawson W, Uy M, Strike K, et al. Point of care ultrasound in haemophilia: Building a strong foundation for clinical implementation. Haemophilia. 2017;23:648–651. https://doi‐org.uml.idm.oclc.org/10.1111/hae.13269
CPHC Clinical Guidelines 2018
Page 8 of 24
Guidelines for Standard 3: Physiotherapy Treatment
3A: After Acute Musculoskeletal bleeds: 3.1 The primary goal of Physiotherapy treatment following a musculoskeletal bleed is to regain pre-bleed status as soon as possible while preventing new injury or re-bleeding (1,2,3). This includes measures to:
o Reduce pain o Reduce swelling o Restore joint range of motion o Restore muscle length o Restore muscle strength o Return to regular activity, including sports
3.2 Early management may include (3,4):
o Factor replacement, as prescribed by the hematologist o Protection of the injury with splints, slings o Complete rest of the injured area, including:
o no weight bearing for joint or muscle bleeds o no ambulation for psoas bleeds
o Ice for pain relief o Compression o Elevation
3.3 Exercise must be progressed cautiously, within limits of pain, and with attention to signs or symptoms that would indicate new bleeding. After the bleeding has stopped, exercise can be introduced (5-8) to restore:
o Joint motion o Muscle length (may also require serial splinting) o Muscle strength o Proprioception (upper limb as well as lower limb) o Balance o Gait o Function (including ADL and sports)
3.4 Manual techniques (9, 10), electrophysical modalities (4, 11) and acupuncture (12) can be used with caution once bleeding has stopped, and according to the usual clinical indications and contraindications.
CPHC Clinical Guidelines 2018
Page 9 of 24
References: 1. Srivastava A, Brewer AK, Mauser‐Bunschotten E, et al. (Treatment Guidelines Working
Group) Guidelines for the management of hemophilia. Haemophilia 2013; 19 31‐e47 and
available at http://www.wfh.org/en/resources/wfh‐treatment‐guidelines (accessed April
20, 2015)
2. Knobe K and Berntorp E. Haemophilia and joint disease: pathophysiology, evaluation, and
management. Journal of Comorbidity 2011; 1:51‐59.
3. Lobet S, Hermans C, Lambert C. Optimal management of hemophilic arthropathy and
hematomas Journal of Blood Medicine 2014:5 207–218
4. Sorensen B, Benson GM, Bladen M, Classey S, Keeling DM, McLaughlin P, Yee, TT, Makris M.
Management of muscle hematomas in patients with severe hemophilia in an evidence‐
poor world. Hemophilia 2012.18:598‐606
5. Blamey G, Forsyth A, Zourikian N, et al. Comprehensive elements of a physiotherapy
exercise programme in haemophilia – a global perspective. Haemophilia 2010; 16(Suppl.5):
136‐45.
6. Gomis M, Querol F, Gallach JE, González M, Aznar JA. Exercise and sport in the treatment
of haemophilic patients: a systematic review. Haemophilia 2009;15:43‐54.
7. Strike K, Mulder K, Michael R. Exercise for haemophilia. Cochrane Database of Systematic
Reviews 2016, Issue 12. Art. No.: CD011180. DOI: 10.1002/14651858.CD011180.pub2.
8. Mulder K. Exercises for People with Hemophilia. World Federation of Hemophilia 2006.
http://www1.wfh.org/publications/files/pdf‐1302.pdf accessed October 28, 2015
9. Heijnen L, De Kleijn P. Physiotherapy for the treatment of articular contractures in
haemophilia. Haemophilia 1999; 5: 16‐19.
10. Cuesta‐Barriuso R, Gomez‐Conesa A, Lopez‐Pina J. Manual Therapy in the treatment of
ankle hemophilic arthropathy. A randomized pilot study. Physiotherapy theory and
Practice 2014; 30 (8): 534‐539.
11. Watson T. Current concepts in electrotherapy. Haemophilia 2002. 8: 413‐8
12. Lambing A, Kohn‐Converse B, Hanagavadi S, Varma V. (2012), Use of acupuncture in the
management of chronic haemophilia pain. Haemophilia, 18: 613–617.
CPHC Clinical Guidelines 2018
Page 10 of 24
3B. Physiotherapy Treatment Before and After MSK Surgical procedures: In many cases, it will be the HTC physiotherapist who suggests to the rest of the team that all conservative measures have been explored and that surgery should be considered to optimize Musculoskeletal function (1). Surgical options may range from simple (intraarticular steroid injection) to complex (osteotomy, debridement, arthrodesis, or arthroplasty). All members of the core HTC team need to participate in pre-operative planning (2). The surgical team must realize that persons with hemophilia undergoing orthopedic surgery may be different than their usual population (3): They are often younger They may have widespread arthropathy and chronic pain They have been conditioned to interpret pain as a sign of bleeding Pain management may require a multimodal approach (MJP) Progression of rehabilitation is often slower due to fear of bleeding and the poor condition of the surrounding tissues. 3.5 Pre-op preparation (1) The HTC physiotherapist should establish contact with the therapist from the surgical team to coordinate the pre-operative treatment and education which should include:
Discussion with the patient and the surgeon regarding goals and expectations for the surgery.
A program of physiotherapy to prepare the adjacent joints for the possible increased stress post-operatively
A program of physiotherapy to prepare the operative joint, to optimize the recuperation and maximize the effects of the surgery- unless the joint is too painful.
Determine need for ambulatory aids, adaptive equipment, environmental adaptations, and ensure these are in place.
Education of the patient regarding anticipated length of hospital stay, post-operative therapy requirements, and time to resume physical activities such as driving or sports.
Discuss the out-patient post-operative rehabilitation: o Location
ensure patient has transportation o Frequency o Duration
With the HTC team, determine how factor coverage will be arranged. 3.6 Post-surgery (1,3,4) After the surgery, the physiotherapist of the surgical team will become involved as soon as possible, as discussed with the medical team.
CPHC Clinical Guidelines 2018
Page 11 of 24
Prior to seeing the patient, the Physiotherapist must ascertain: the type of hemophilia and severity
the factor replacement regimen
the detailed procedure of the surgery
the condition of the joint and surrounding muscles observed during the surgery
the range of motion obtained during surgery (if appropriate to the procedure)
3.7 The post-surgical physiotherapist must be aware that: Rehabilitation times after surgery will vary by individual patient and extent of
surgery. Longer than normal hospital admission and rehabilitation time should be
expected. (1,3) PWBD are more likely to develop complications: Pain: Pain management may be complicated: the patient may not be able to
distinguish post-operative pain from pain due to new bleeding (3, 4) Bleeding: The risk of bleeding may postpone the mobilizations and predispose to
ankylosis Delayed wound healing and infections (5) Difficulty regaining pre-operative range of motion, especially after TKA
o CPM may be useful after arthroplasty in PWH, even though the surgical team may not use it routinely (1).
The physiotherapist should be extra cautious to prevent and watch for any signs of bleeding.
o Spontaneous bleeds are common at the end of the first week post op. o If bleeding occurs, stop the rehabilitation program and rest the limb. o Watch for signs and symptoms of infection. o Understand that joint stiffness is more likely to occur due to slower
progression and the state of the extra-articular structures (muscular tightness, joint damages, involvement of the others joints).
Recommended reading re TKA and Hemophilia:
MASAC Recommendations Regarding Physical Therapy Guidelines in Patients with Bleeding Disorders: Total Knee Replacement https://www.hemophilia.org/sites/default/files/document/files/238PTTotalKneeReplacement.pdf accessed Jan 19-2016 Lobet S, Pendeville E, Dalzell R, Defalque A, Lambert C, Pothen D, Hermans, C. (2008), The role of physiotherapy after total knee arthroplasty in patients
CPHC Clinical Guidelines 2018
Page 12 of 24
with haemophilia. Haemophilia, 14: 989–998. doi:10.1111/j.1365-2516.2008.01748.x
References: 1. Lobet S, Pendeville E, Dalzell R, Defalque A, Lambert C, Pothen D and Hermans C. (2008), The role of physiotherapy after total knee arthroplasty in patients with haemophilia. Haemophilia, 14: 989–998. doi:10.1111/j.1365‐2516.2008.01748.x 2. Rodriguez‐Merchan EC (2012), Aspects of current management: orthopaedic surgery in haemophilia. Haemophilia, 18: 8–16. 3.De Kleijn P, Blamey G, Zourikian N, Dalzell R, Lobet S. Physiotherapy following elective
orthopedic procedures. Haemophilia 2006; 12 (Suppl 3) 108‐12
4. De Kleijn P, Fischer K, Vogely H C, Hendriks C and Lindeman E. (2011), In‐hospital
rehabilitation after multiple joint procedures of the lower extremities in haemophilia
patients: clinical guidelines for physical therapists. Haemophilia, 17: 971–978.
doi:10.1111/j.1365‐2516.2011.02527.x
5.Hoffman M, Monroe DM. Wound healing in haemophilia‐breaking the vicious cycle.
Haemophilia 2010; 16 (Suppl 3) 13‐8
CPHC Clinical Guidelines 2018
Page 13 of 24
Guidelines for Standard 4: The Annual Assessment
A complete musculoskeletal assessment will be done annually on each patient regardless of the severity of the bleeding disorder (1, 2)
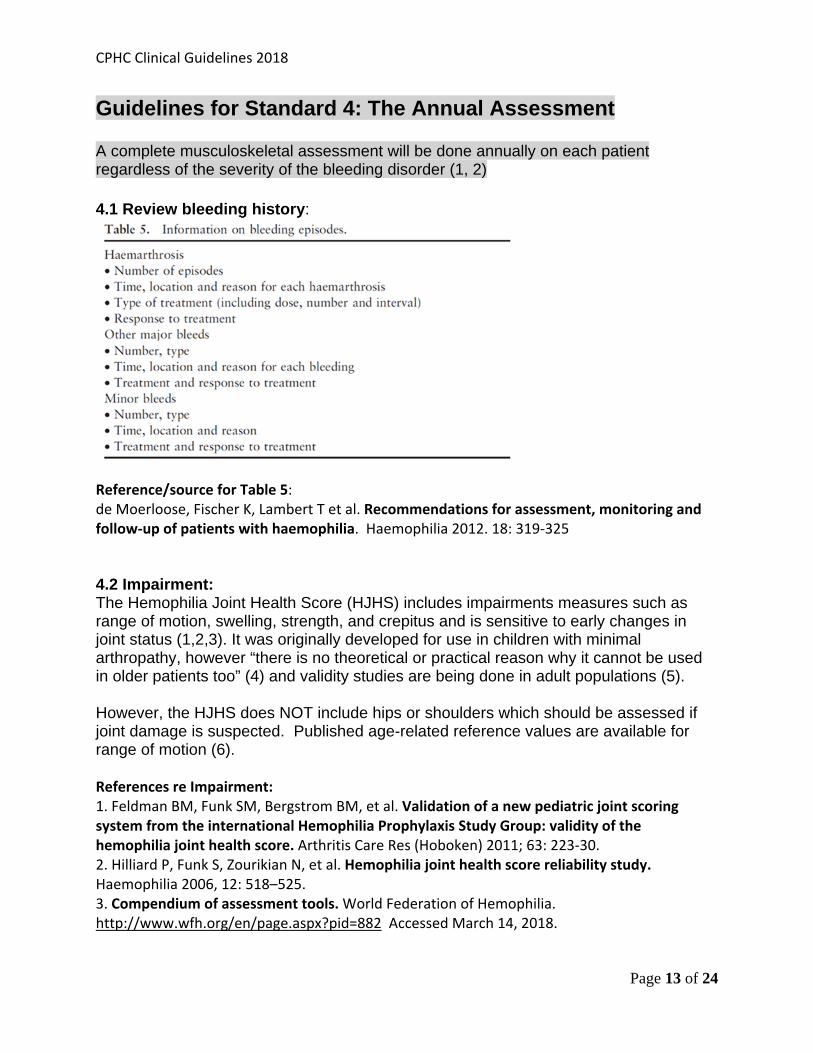
4.1 Review bleeding history:
Reference/source for Table 5: de Moerloose, Fischer K, Lambert T et al. Recommendations for assessment, monitoring and follow‐up of patients with haemophilia. Haemophilia 2012. 18: 319‐325 4.2 Impairment: The Hemophilia Joint Health Score (HJHS) includes impairments measures such as range of motion, swelling, strength, and crepitus and is sensitive to early changes in joint status (1,2,3). It was originally developed for use in children with minimal arthropathy, however “there is no theoretical or practical reason why it cannot be used in older patients too” (4) and validity studies are being done in adult populations (5). However, the HJHS does NOT include hips or shoulders which should be assessed if joint damage is suspected. Published age-related reference values are available for range of motion (6). References re Impairment: 1. Feldman BM, Funk SM, Bergstrom BM, et al. Validation of a new pediatric joint scoring system from the international Hemophilia Prophylaxis Study Group: validity of the hemophilia joint health score. Arthritis Care Res (Hoboken) 2011; 63: 223‐30. 2. Hilliard P, Funk S, Zourikian N, et al. Hemophilia joint health score reliability study. Haemophilia 2006, 12: 518–525. 3. Compendium of assessment tools. World Federation of Hemophilia. http://www.wfh.org/en/page.aspx?pid=882 Accessed March 14, 2018.
CPHC Clinical Guidelines 2018
Page 14 of 24
4. Fischer, K. and de Kleijn, P. (2013), Using the Haemophilia Joint Health Score for assessment of teenagers and young adults: exploring reliability and validity. Haemophilia, 19: 944–950. doi:10.1111/hae.12197 5. Buckner, T. W., Wang, M., Cooper, D. L., Iyer, N. N., & Kempton, C. L. (2017). Known‐group validity of patient‐reported outcome instruments and hemophilia joint health score v2.1 in US adults with hemophilia: results from the Pain, Functional Impairment, and Quality of life (P‐FiQ) study. Patient Preference & Adherence, 111745‐1753. doi:10.2147/PPA.S141392 6. Soucie JM, Wang C, Forsyth A, et al. Range of motion measurements: reference values and a database for comparison studies. Haemophilia 2011; 17: 500‐7. 4.3 Pain: Pain is a prominent feature in persons with bleeding disorders, and can be due to diverse factors including acute bleeds, venous access, and chronic joint disease (1,2). Pain status should be monitored in PWBD so that appropriate management (non-pharmacological or pharmacological) can be instituted (3,4,5,6)
Examples of pain measurement scales commonly used in care of PWBD include: Visual Analog Scale/Numeric Pain Rating Scale (7,8) FACES (9,10) S-LANSS - Leeds Assessment of Neuropathic Symptoms and Signs (11) Brief Pain Inventory Scale (12,13) Functional Disability Inventory (14) McGill Pain Questionnaire (SF-MPQ) (15)
References re Pain: 1. Van Genderen FR, Fischer K, Heijnen L et al. Pain and functional limitations in patients with severe haemophilia. Haemophilia (2006), 12, 147–153 2. Hilberg T, Czepa D, Freialdenhoven D, Boettger MK. Joint pain in people with hemophilia depends on joint status. Pain 2011. 152:2029‐2035 3. de Moerloose, Fischer K, Lambert T et al. Recommendations for assessment, monitoring and follow‐up of patients with haemophilia. Haemophilia 2012. 18: 319‐325 4. Donfield SM, Astermark J, Lail AE, Gilbert SA, Berntorp E; Fenoc Study Group. Value added: increasing the power to assess treatment outcome in joint haemorrhages. Haemophilia. 2008 Mar;14(2):276‐80 5. Srivastava A, Brewer AK, Mauser‐Bunschotten E, et al. (Treatment Guidelines Working Group) Guidelines for the management of hemophilia. Haemophilia 2013; 19 31‐e47 and available at http://www.wfh.org/en/resources/wfh‐treatment‐guidelines (accessed March 20, 2018 ) 6. Buckner TW, Wang M, Cooper D L, Iyer NN, & Kempton CL (2017). Known‐group validity of patient‐reported outcome instruments and hemophilia joint health score v2.1 in US adults with hemophilia: results from the Pain, Functional Impairment, and Quality of life (P‐FiQ) study. Patient Preference & Adherence, 111745‐1753. doi:10.2147/PPA.S141392
CPHC Clinical Guidelines 2018
Page 15 of 24
7. Rehabilitation Measures Data Base https://www.sralab.org/rehabilitation‐measures/numeric‐pain‐rating‐scale (accessed March 20, 2018) 8. Physiopedia http://www.physio‐pedia.com/Visual_Analogue_Scale (accessed March 20, 2018) 9. Rambod M, Forsyth K, Sharif F, Khair K. Assessment and management of pain in children and adolescents with bleeding disorders: a cross‐sectional study from three haemophilia centres. Haemophilia. 2015 Jul 20. 10. Tomlinson D, Von Baeyer Cl, Stinson JN, Sung L. A Systematic Review of Faces Scales for the Self‐report of Pain Intensity in Children. Pediatrics, 2010 Nov, Vol.126(5), pp.E1168‐E1198 11. Bennett MI, Smith BH, Torrance N, Potter J. The S‐LANSS score for identifying pain of predominantly neuropathic origin: validation for use in clinical and postal research. Pain. 2005 Mar;6(3):149‐58. 12. Physiopedia: http://www.physio‐pedia.com/Brief_Pain_Inventory_‐_Short_Form (accessed March 20, 2018) 13. Mendoza T, Mayne T, Rublee D, Cleeland C. Reliability and validity of a modified Brief Pain Inventory short form in patients with osteoarthritis. Eur J Pain. 2006 May;10(4):353‐61. 14. Claar RL, Walker LS. Functional assessment of pediatric pain patients: Psychometric properties of the Functional Disability Inventory. Pain. 2006;121(1‐2):77‐84. 15. Melzack R. The short‐form McGill Pain Questionnaire. Pain. 1977; 30:191‐197 4.4 Function and Participation: Repeated musculoskeletal bleeding can cause altered movement patterns in the early years, and chronic hemophilic arthropathy with advancing age (1). Changes are often insidious and subtle. The Annual Physiotherapy assessment allows identification and early intervention as new problems arise (2,3). The Physiotherapist will use standardized tools to assess participation in
school/work physical activities and /or sports leisure activities social activities self-care
Hemophilia Specific tools include:
Hemophilia Activities List and Pediatric Hemophilia Activities List (4,5,6) Functional Independence Scale for Hemophilia (4)
Other tools, that are not specific to hemophilia, may also be useful to assess overall physical functioning. Some examples of these are:
Children: Alberta Infant Motor Scale (7) Movement Assessment of Infants (7) Peabody Developmental Gross Motor Scale (7)
CPHC Clinical Guidelines 2018
Page 16 of 24
Adults: Community Balance and Mobility Scale (8) Timed Up and Go (9) 6 minute Walk test (9)
References re Function and Participation: 1. Lobet S, Hermans C, Lambert C. Optimal management of hemophilic arthropathy and hematomas Journal of Blood Medicine 2014:5 207–218 2. de Moerloose, Fischer K, Lambert T et al. Recommendations for assessment, monitoring and follow‐up of patients with haemophilia. Haemophilia 2012. 18: 319‐325 3. Srivastava A, Brewer AK, Mauser‐Bunschotten E, et al. (Treatment Guidelines Working Group) Guidelines for the management of hemophilia. Haemophilia 2013; 19 31‐e47 and available at http://www.wfh.org/en/resources/wfh‐treatment‐guidelines (accessed March 20, 2018) 4. Compendium of assessment tools. World Federation of Hemophilia. http://www.wfh.org/en/page.aspx?pid=882 (Accessed March 20, 2018) 5. Van Genderen FR, van Meeteren NL, van der Bom JG, et al. Functional consequences of haemophilia in adults: the development of the Haemophilia Activities List. Haemophilia 2004; 10: 565-71. 6. Groen WG, van der Net J, Helders PJ, Fischer K. Development and preliminary testing of a paediatric version of the Haemophilia Activities List (pedhal). Haemophilia 2010; 16: 281‐9. 7. Darrah J, Piper M, Watt M‐J. Assessment of gross motor skills of at‐risk infants: predictive validity of the Alberta Infant Motor Scale. Developmental Med Child Neurol 1998; 40: 458‐491 8. Balasubramanian C. The Community Balance and Mobility Scale Alleviates the Ceiling Effects Observed in the Currently Used Gait and Balance Assessments for the Community‐Dwelling Older Adults. Journal Of Geriatric Physical Therapy [serial online]. April 2015;38(2):78‐89 12p. Available from: CINAHL Plus with Full Text, Ipswich, MA. Accessed November 9, 2015 9. Physiopedia http://www.physio‐pedia.com/Category:Outcome_Measures (Accessed March 20, 2018) 4.5 Patient Reported Outcomes These tools are useful because they allow individuals to identify issues that are important and meaningful to them. Examples include:
Patient Specific Functional Scale, https://www.physio‐pedia.com/Patient_Specific_Functional_Scale
Canadian Occupational Performance Measure: http://www.thecopm.ca/
Goal Attainment Scale. Recht, M. , Konkle, B. A., Jackson, S. , Neufeld, E. J., Rockwood, K. and Pipe, S. (2016), Recognizing the need for personalization of haemophilia patient‐reported outcomes in the prophylaxis era. Haemophilia, 22: 825‐832. doi:10.1111/hae.13066
CPHC Clinical Guidelines 2018
Page 17 of 24
Guidelines for Standard 5: PT Treatment of Musculoskeletal Complications of Bleeding Disorders
5.1 Features of arthropathy include joint pain and stiffness, contracture and deformity, muscle imbalance and atrophy, and alterations in the individual’s ability to function and participate normally (1).
5.2 Most physiotherapy interventions can be applied according to the usual clinical indications and precautions and as long as there is no active bleeding, including:
Exercise program to maintain or improve range of motion, strength, flexibility, balance or exercise tolerance (1,2,3,4,5)
Joint protection techniques such as proper body mechanics, ergonomic adaptations, orthotics or bracing (1,6)
Hydrotherapy (7) Prescription and instruction re mobility aids Consultation with Occupational Therapy regarding adaptations to the individual’s
environment. Consultation with orthopedics and preparation for surgery (8,9,10) Use of splinting/low load prolonged passive stretching techniques/devices (serial
splinting/ casting) (11,12) Manual therapy (12,13) Electrophysical agents (14) Acupuncture (15)
References: 1. Lobet S, Hermans C, Lambert C. Optimal management of hemophilic arthropathy and
hematomas. Journal of Blood Medicine 2014:5 207–218 2. Blamey G, Forsyth A, Zourikian N, et al. Comprehensive elements of a physiotherapy
exercise programme in haemophilia – a global perspective. Haemophilia 2010; 16(Suppl.5): 136‐45.
3. Gomis M, Querol F, Gallach JE et al. Exercise and sport in the treatment of haemophilic patients: a systemic review. Haemophilia 2009. 15: 43‐54‐ 15
4. Negrier C, Seuser A, Forsyth A. The benefits of exercise for patients with haemophilia and recommendations for safe and effective physical activity. Haemophilia. 2013;19(4):487–498.
5. Strike K, Mulder K, Michael R. Exercise for haemophilia. Cochrane Database of Systematic Reviews 2016, Issue 12. Art. No.: CD011180. DOI: 10.1002/14651858.CD011180.pub2.
6. Querol F, Aznar JA, Haya S, Cid A. Orthoses in haemophilia. Haemophilia 2002. 8:407‐12 7. Von Mackensen S, Eifrig B, Zach D, Kalnins J, Wieloch A, Zeller W. (2012) The impact of a
specific aqua‐training for adult haemophilic patients – results of the WATERCISE study (WAT‐QoL). Haemophilia, 18: 714–721.
CPHC Clinical Guidelines 2018
Page 18 of 24
8. McDonald S, Page MJ, Beringer K, Wasiak J, Sprowson A. Preoperative education for hip or knee replacement. Cochrane Database of Systematic Reviews 2014, Issue 5. Art. No.: CD003526.
9. Forsyth A and Zourikian N. (2012) How we treat: considerations for physiotherapy in the patient with haemophilia and inhibitors undergoing elective orthopaedic surgery. Haemophilia, 18: 550–553.
10. Lobet S, Pendeville E, Dalzell R, Defalque A, Lambert C, Pothen D and Hermans C. (2008), The role of physiotherapy after total knee arthroplasty in patients with haemophilia. Haemophilia, 14: 989–998. doi:10.1111/j.1365‐2516.2008.01748.x
11. . Sorenson B, Benson GM, Bladen M, Classey S, Keeling DM, McLaughlin P, Yee, TT, Makris M. Management of muscle hematomas in patients with severe hemophilia in an evidence‐poor world. Hemophilia 2012. 18:598‐606
12. Heijnen L, De Kleijn P. Physiotherapy for the treatment of articular contractures in haemophilia. Haemophilia 1999; 5: 16‐19.
13. Cuesta‐Barriuso R, Gomez‐Conesa A, Lopez‐Pina J. Manual Therapy in the treatment of ankle hemophilic arthropathy. A randomized pilot study. Physiotherapy theory and Practice 2014; 30 (8): 534‐539.
14. Watson T. Current concepts in electrotherapy. Haemophilia 2002. 8: 413‐8. 15. Lambing A, Kohn‐Converse B, Hanagavadi S, Varma V. Use of acupuncture in the
management of chronic haemophilia pain. 2012 Haemophilia, 18: 613–617.
CPHC Clinical Guidelines 2018
Page 19 of 24
Guidelines for Standard 6: Consultation with other care providers There are many circumstances where PWBD may receive Physiotherapy assessment and treatment from physiotherapists who are not affiliated with a comprehensive Hemophilia treatment center (HTC). These circumstances may include, but are not limited to:
the PWBD requires therapy outside the skill set of the HTC therapist (e.g. pediatric therapist seeing adult patients and vice versa, orthopedic therapist seeing PWBD with neurological impairment)
Surgery is done in a facility different from the HTC, and the therapists at the surgical center have specialized skills and knowledge re the post-op rehab requirements.
The PWBD lives too far away from the HTC and will see a therapist in his/her home community
The FTE allocation of the HTC therapist is not sufficient to meet all the needs of the PWBDs within the program: (e.g. time is allocated for annual review only so patients requiring ongoing treatment must access physiotherapy services elsewhere)
In these circumstances the HTC therapist will be available for consultation (1) to assist the treating therapist to:
be familiar with contraindications and precautions to be observed when treating any PWBD
be familiar with known chronic impairments and limitations specific to the PWBD being treated that may not be amenable to treatment
verify the factor replacement regimen/schedule recommended by the HTC team for the patient
recognize signs and symptoms of new bleeding and modify treatment accordingly
facilitate communication between the treating therapist and the rest of the team including a plan for prophylactic factor replacement if needed, and a plan for treatment of new bleeding
be aware of educational resources and other leaning opportunities pertinent to the management of bleeding disorders
Reference:
1. Canadian Hemophilia Standards Group. Canadian Comprehensive Care Standards for Hemophilia and other Inherited Bleeding Disorders. First Edition. 2007 http://www.hemophilia.ca/en/care-and-treatment/comprehensive-care-standards/ accessed March 14,2018 pages 9, 16.
CPHC Clinical Guidelines 2018
Page 20 of 24
Guidelines for Standard 7: Education and health promotion
An active healthy lifestyle promotes cardiovascular fitness, healthy body weight, psychological well-being, and ability to maintain independence (7,8,9).
Physiotherapists provide education regarding selection of sports and activities that are enjoyable to the individual but minimize the risk of injury (1-5). There are a number of resources that have been developed as guidelines for selection of physical activities (see list below). Many of these attempt to classify sports and activities according to risk and the recommendations made may not be suitable in all instances. “In the Driver’s Seat” is designed “to guide adults with bleeding disorders through an organized and thoughtful approach to decision-making around physical activities.”
It is the opinion of CPHC that personal activity plans should be INDIVIDUALIZED and should take into account each individual’s bleeding tendency, physical capabilities and interests. This requires discussion between the individual/family and the team. Resources: Hemophilia Organizations: In the Driver’s Seat: A Workbook designed to guide personalized decision-making
about physical activities. Canadian Hemophilia Society. http://www.hemophilia.ca/files/In%20the%20Drivers%20Seat%20-%20EN_LR.pdf
Playing it Safe. National Hemophilia Foundation (USA) https://www.hemophilia.org/sites/default/files/document/files/PlayingItSafe.pdf
Bleeding Disorders: Precautions. Canadian Hemophilia Society. http://www.hemophilia.ca/en/bleeding-disorders/hemophilia-a-and-b/precautions/ (updated in 2008)
All About Hemophilia: Chapter 12: Physical Activity, Exercise and Sports
http://www.hemophilia.ca/files/Chapter%2012.pdf Playing Sport:
http://www.haemophiliacare.co.uk/pdfs/08_Playing_Sport.pdf (2008) London Ontario treatment center
http://www.lhsc.on.ca/Patients_Families_Visitors/Bleeding_Disorders/Physiotherapy/Activity_Choices.htm (London Ontario)
CPHC Clinical Guidelines 2018
Page 21 of 24
Resources: Pharmaceutical Companies: Bayer Pharmaceuticals; http://www.livingwithhemophilia.ca/managing/fitness-
exercise.php
Baxalta: http://baxaltahematology.com/us/hemophilia-info/hemophilia-sports-and-exercise.html
References:
1. Lobet S, Hermans C, Lambert C. Optimal management of hemophilic arthropathy and hematomas. Journal of Blood Medicine 2014:5 207–218
2. Negrier C, Seuser A, Forsyth A. The benefits of exercise for patients with haemophilia and recommendations for safe and effective physical activity. Haemophilia. 2013;19(4):487–498.
3. Gomis M, Querol F, Gallach JE, González M, Aznar JA. Exercise and sport in the treatment of haemophilic patients: a systematic review. Haemophilia. 2009; 15:43-54.
4. Wittmeier K and Mulder K. (2007), Enhancing lifestyle for individuals with haemophilia through physical activity and exercise: the role of physiotherapy. Haemophilia, 13: 31–37.
5. Riske B. (2007), Sports and exercise in haemophilia: benefits and challenges. Haemophilia, 13: 29–30.
CPHC Clinical Guidelines 2018
Page 22 of 24
Guidelines for Standard 8: Continuing Competence There are many Hemophilia Specific learning opportunities available to physiotherapists. Journal:
Haemophilia: the Official Journal of the World Federation of Hemophilia. Can be searched on line via the WFH website: http://onlinelibrary.wiley.com/journal/10.1111/%28ISSN%291365-2516/issues Some articles can be downloaded at no cost. CPHC members have full access to the journal: contact the Secretary for password information.
Educational Materials: World Federation of Hemophilia: www.wfh.org. Numerous resources are
available for download, including: o Guidelines for the management of Hemophilia o Compendium of Assessment tools o Treatment of Hemophilia monograph series o Web-casts of congress sessions
Canadian Hemophilia Society www.hemophilia.ca. Resources include: o All About Hemophilia o Comprehensive Care Standards (2007) o Contact information for all HTCs across Canada
National Hemophilia Foundation (USA) https://www.hemophilia.org/Bleeding-Disorders Resources include:
o Medical and Scientific Advisory Council recommendations https://www.hemophilia.org/Researchers-Healthcare-
Providers/Medical-and-Scientific-Advisory-Council-MASAC/MASAC-Recommendations/MASAC-Recommendations-Regarding-Physical-Therapy-Guidelines-in-Patients-with-Bleeding-Disorders
Hemophilia Foundation of Australia o http://www.haemophilia.org.au/publications/haemophilia-resources
Hemophilia-specific Conferences: In Canada:
CHS New team member workshops: designed for Hemophilia Treatment Center team members with 3 years or less of experience.
CHS Rendez-vous: held in even-numbered years. Medical symposium and combined meetings of all core team member groups:
CPHC Clinical Guidelines 2018
Page 23 of 24
o Association of Hemophilia Clinic Directors of Canada (AHCDC) o Canadian Association of Nurses in Hemophilia Care (CANHC) o Canadian Physiotherapists in Hemophilia Care (CPHC) o Canadian Social Workers in Hemophilia Care (CSWHC)
Annual meetings of core team member groups: held in odd-numbered years.
Outside Canada:
World Federation of Hemophilia (WFH) World Congress o Held in even numbered years. o Attended by care team members, researchers and people with
bleeding disorders o Program has Medical, Multi-disciplinary, and Musculoskeletal streams.
WFH Musculoskeletal Congress
o Held in odd-numbered years. o attended mainly by team members and researchers o excellent opportunity for interaction between orthopedic surgeons and
physiotherapists
WFH Global Forum on Research and Treatment Products for Bleeding Disorders – held in odd numbered years in Montreal.
o Topics vary. Check website for program details.
Congress of the European Association for Haemophilia and Allied Disorders. o Annual meeting; recent formation of a physiotherapy committee o http://eahad.org/
National Hemophilia Foundation (USA)
https://www.hemophilia.org/Events-Educational-Programs o Annual meeting and conference o Attended by people with bleeding disorders, team members and
researchers
Other Hematology Conferences: International Society of Thrombosis and Hemostasis (ISTH)
https://www.isth.org/ o “At the ISTH Congress, thousands of the world’s leading experts on
thrombosis, haemostasis and vascular biology come together to present the most recent advances, exchange the latest science and
CPHC Clinical Guidelines 2018
Page 24 of 24
discuss the newest clinical applications designed to improve patient care.”
o Congresses held in odd-numbered years
American Society of Hematology (ASH) http://www.hematology.org/ o “The Society's mission is to further the understanding, diagnosis,
treatment, and prevention of disorders affecting the blood, bone marrow, and the immunologic, hemostatic and vascular systems, by promoting research, clinical care, education, training, and advocacy in hematology.”





























