Embed Size (px)
Citation preview

PII S0730-725X(99)00033-8
● Original Contribution
CLINICAL SIGNIFICANCE OF MAGNETIC RESONANCE IMAGING (MRI) FORFOCAL CHONDRAL LESIONS
RYUJI MORI, MITSUO OCHI, YASUO SAKAI , NOBUO ADACHI, AND YUJI UCHIO
Orthopaedic Department, Shimane Medical University, Shimane, Japan
To evaluate the diagnostic potential of magnetic resonance imaging (MRI) and define its role, focal chondrallesions of the femoral surface of the tibiofemoral joint were examined. Full-thickness defects were well detectedprospectively (93%) with conventional MRIs initially administered for observation reference of ligaments andmenisci. Optimized MRIs, which included right-angled planes to the lesion surface and magnetization transfercontrast (MTC) sequences, delineated the size of lesions (R2 5 0.648,p < 0.0001) and the difference between full-and partial-thickness defects (88% in accuracy). A forward-tilt of 30o to the femoral shaft was the average planeangle that afforded optimal visualization of the chondral lesions. Our findings advocate that routine MRIs aresufficient in detecting severe chondral lesions that require further examination, and the optimized images arehighly useful in facilitating the recently developed therapeutic approaches and follow-up studies for articularcartilage defects. © 1999 Elsevier Science Inc.
Keywords:Chondral lesion; Knee; Image plane; Magnetization transfer contrast.
INTRODUCTION
Chondral lesions are extensively diagnosed by arthros-copy. In addition, recent developments in surgical andpharmacologic methods for the treatment and preventionof chondral degeneration and injury1–5 have arousedheated controversies, leading to emphasis on the neces-sity for a clinical evaluation system to monitor follow-updegenerative and regenerative processes.6
Currently, arthroscopy is extensively considered as astandard in the diagnosis of cartilage lesions since itaffords direct visual inspection and palpation of sus-pected lesions.7–9 The utility of this technique, however,is limited by its invasiveness and expense. Computedtomography (CT) combined with arthrography improvesthe visualization of cartilages and detection of abnormal-ities, but spatial restriction of the CT-gantry limits im-aging resolution in multiple planes.10
Magnetic resonance (MR), by virtue of its superiorsoft tissue contrast, multiplanar capability and its abilityto allow direct visualization of articular cartilage, ap-pears to be the most promising imaging method for
evaluation of articular cartilage. Despite its theoreticaladvantages, however, its role in clinical use remainscontroversial, with inconsistent results in sensitivitiesand specificities, ranging from 50 to 100%.7–9,12,13 Infact, some recent findings on MRI of chondral lesionshave reported the negative effects in clinical use.8,9 Oneof the major problems in determining its efficacy lies inthe inconsistencies of study groups composed of varioussubjects with and without specific findings of physicaland radiographic examinations. The recently introducedtherapeutic strategies for treatment of chondral le-sions1,5,6 make it even more complicated. This studyattempted to evaluate the clinical significance and definethe role of MRI for chondral lesions, which are detect-able only by arthroscopy and/or MRI, besides delineationof lesions with the optimal imaging technique.
MATERIALS AND METHODS
Consecutive focal chondral lesions (0.5–6.0 cm2) de-tected on the femoral surface of the tibiofemoral joint byarthroscopy were examined prospectively, and retrospec-tively through a review of MRIs obtained within one
RECEIVED 10/16/98; ACCEPTED3/23/99.Address correspondence to Mitsuo Ochi, M.D., Ph.D., Or-
thopaedic Department, Shimane Medical University, 89–1,
Enya-cho, Izumo-shi, Shimane, Japan 693-8501. E-mail:[email protected]
Magnetic Resonance Imaging, Vol. 17, No. 8, pp. 1135–1140, 1999© 1999 Elsevier Science Inc. All rights reserved.
Printed in the USA.0730-725X/99 $–see front matter
1135

month before and after the surgical procedures. Thestudy group was composed of 16 males and 19 femaleswhose ages ranged from 12 to 52 years (average: 38years). In these 35 patients, 40 articular cartilage lesionswere found in 37 knees. Most patients underwent arthro-scopic surgery for anterior cruciate ligament (32 knees)and/or meniscus injuries (14 knees). Extensive chondrallesions, which could be ascertained by physical or rou-tine radiographic examinations, were omitted from thestudy group. A total of 40 lesions were divided into threecategories via arthroscopic and MRI diagnoses (Table 1).The sizes of cartilage defects were measured with botharthroscopy and MRI. The area of softening was notanalyzed since the margin was not well defined evenwith arthroscopy.
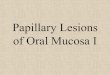
MRI was performed on a 1.5-Tesla unit (Gyroscan,Phillips, CA, USA) with an extremity surface coil, asection thickness of 3 mm without an interslice gap anda 16-cm field-view with an imaging matrix of 5123 512.During imaging, the patient’s knee was extended fully.T1- and T2-weighted images were obtained using thetwo-dimensional gradient-recalled echo (GRE) pulse se-quences while T1-weighted images were obtained withGRE 25/9.2 (repetition time in ms/echo time in ms)sequences at a 50o flip-angle for an acquisition time of5.0 min, T2-weighted images were resolved with GRE500/18 at 35o for 5.9 min, respectively. Proton densityimages were obtained using the spin echo technique1,429/17 for 4.9 min. Magnetization transfer contrast(MTC) images, generated by irradiating the macromo-lecular protons in tissue with a low power off-resonanceradio-frequency field,14 were obtained with GRE 27/9.2at 25o flip-angle for 5.1 min. Pre-operative Images of T1,T2 and proton density on ligaments and menisci initiallyobtained in sagittal and coronal planes were used forreference. Post-operative images, including MTC se-quences, were obtained in at least two planes perpendic-ular to the surfaces of chondral lesions (Fig. 1).
Interpretation of MRI was performed by two ortho-paedic specialists (R.M., Y.S.) who had a least one yearof experience in reading MRI under guidance by radiol-ogists and were “blind” to arthroscopic surgeries previ-ously conducted on the study group. Diagnoses wereconducted 1) prospectively with pre-operative images; 2)retrospectively with pre-operative images; and 3) retro-
spectively with post-operative images. Prospective diag-nosis was performed when knowledge was limited todata from physical examinations and plain radiographsimplying absence of chondral lesions. Retrospective in-terpretation was performed by the same readers afterbeing informed of only the location of lesions from otherorthopaedic surgeons (M.O., N.A., Y.U.) who had pre-viously performed the arthroscopic surgeries. Wherethere were some discrepancies among the readers, agree-ment was obtained by consensus.
Statistical analysis was performed with simple regres-sion analysis.
RESULTS
Data evaluating the prospective and retrospectiveMRIs on all chondral lesions of the knee are summarizedin Table 2. The sensitivity of grade I was low; only 27%even with retrospective readings of post-operative im-ages. The overall retrospective sensitivities for grade IIand III lesions, however, showed a higher value (62%prospectively with pre-operative images, 76% retrospec-tively with pre-operative images, 93% retrospectivelywith post-operative images). The abnormalities of gradeIII lesions were well detected even prospectively (93%).A perfect correlation of grading was obtained 25% pro-
Fig. 1. Pre-operative images were obtained in sagittal andcoronal planes. Post-operative images included at least twoplanes which were perpendicular to the injured surface.
Table 1. Study scheme for grading articular cartilage lesions with magnetic resonance imaging (MRI) and arthroscopy
Arthroscopic findings MRI findings Grade
Normal Normal 0Definite softening and/or superficial fibrillation Cartilage surface smooth, hypo- or hyper-signal ICartilage surface damaged, lesion,100% thickness Surface irregularity and/or focal loss,100% thickness IIBone exposed Focal loss 100% with/without bone reaction III
1136 Magnetic Resonance Imaging● Volume 17, Number 8, 1999

spectively, and 38% retrospectively with pre-operativeimages, and 60% retrospectively with post-operative im-ages. In retrospective readings of grade II and III lesionswith post-operative images, 88% of MRI grading wasconsistent with arthroscopic findings (Table 2). There aretwo different techniques in post-operative imaging fromthe pre-operative approach; viz, right-angled planes tothe joint surface and MTC images. Portraying the right-angled views improved visualization of the lesions, es-pecially at the posterior surface where delineation ofdefect sizes with conventional coronal and sagittal planeswas hitherto impossible (Figs. 2 and 3). Because ofconvexity of the condyles even in the coronal plane,conventional sagittal planes could not always visualizethe lesion clearly (Fig. 1). The average angle at whichchondral lesions contacted the tibial joint surface was 28o
of flexion. MTC also improved the diagnoses, especiallyfor grade II lesions. Four of fifteen lesions of grade IIwere detected only by MTC images. In fact, MTC ren-dered possible detection on all chondral lesions non-detectable by other sequences (Fig. 4).
DISCUSSION
The overall prospective sensitivity of MRI was low,especially when a lesion was not a full-thickness defectand located at the posterior surface of condyles or on thetangential surface to the image planes. Although somemight conclude from this result that MRI was not sensi-tive enough to survey mild chondral lesions,8,9 the full-thickness defects in this study were well detected, evenprospectively with conventional MRIs initially adminis-tered for observations of ligaments and menisci. Further-more, the present approach revealed those lesions lack-
ing any specific findings on physical and routineradiographic examinations, confirming thus the efficacyand superiority of MRI.
In surgical decision making on localized cartilagelesions, the diagnosis of full-thickness defects plays animportant role, since recently innovated surgical inter-
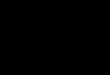
Fig. 2. Comparison of lesion sizes (cm2) between MRI andarthroscopy. Retrospective diagnoses with pre-operative (A andB) and post-operative (C) imaging. Chondral lesions werelocated at the weight-bearing site with the knee at 0–30° (E)and 31–60° (Œ) of flexions.
Table 2. Comparison of lesion grading between MRI andarthroscopy
MRI
Arthroscopy
0 I II III
P-Pre 0 \ 9 10 1I 2 1 1 1II 3 1 2 5III 0 0 2 7
R-Pre 0 \ 8 7 0I 3 1 2 0II 1 2 4 4III 0 0 2 10
R-Post 0 \ 8 2 0I 2 2 0 0II 0 1 10 2III 0 0 3 12
P-Pre: Prospective readings with preoperative images.R-Pre: Retrospective readings with preoperative images.R-Post: Retrospective readings with postoperative images.
Focal chondral lesions● R. MORI ET AL. 1137

ventions such as implantation of chondrocytes,1 osteo-chondral grafting,2,3 periosteum grafting4 may be re-sorted to exclusively for correcting full-thicknessdefects. Although softening and partial thickness defectsare not always detectable by MRI, they usually do notcause any symptoms or further damage.15 Therefore,MRI is highly beneficial for routine clinics in decidingwhether invasive therapy or examination such as arthro-scopy is necessary.
Furthermore, optimized MRI for articular cartilagenot only delineates the size of a lesion but also discrim-inates the differences between full- and partial-thicknessdefects when the location is known. It is of great signif-icance to be able to follow the natural progression ofchondral lesions and their responses to newly developedtherapies. Although the state of the art is changing dra-matically in regard to therapeutic approaches, diagnosticprocedures have yet to be established well enough toattain a universal standard. Previous discrepancies ofarthroscopy in locating the critical size of very small
full-thickness defects assumed to have healed spontane-ously from animal studies16 are not favorable since theinvasive technique is not applicable repeatedly, espe-cially in situations where a large group of subjects are
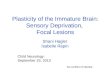
Fig. 3. A grade II lesion, located at the weight-bearing surfaceat 35° of flexion, is displayed as magnetization transfer contrastimages (MTC). The right-angled plane (A) delineates margin ofa defect (arrow), although conventional coronal plane (B) doesnot reveal the abnormalities.
Fig. 4. Sagittal MR images of a grade II lesion. Good carti-lage-fluid contrast of MTC (A) afforded delineation of a smalldefect (arrow), while P (B) and T2-weighted images (C) did notreveal any abnormalities.
1138 Magnetic Resonance Imaging● Volume 17, Number 8, 1999

under study at any one time. However, noninvasive ex-aminations using MRI can achieve this purpose besidesfacilitating selection of a constructive and appropriatesurgical approach before intervention. Both autogenousosteochondral and chondrocyte grafts are applicable onlyto minor lesions because of their limited donor sites.5,6 Inaddition, although joint replacements for extensive le-sions with artificial materials and allogeneic osteochon-dral grafts3 are available, a complete preparation is re-quired beforehand. Thus, in cases where cartilage defectsare implied by conventional MRI, further evaluation ofthe grade and estimation of the size with the optimal MRItechnique are prerequisites to drafting a surgical plan. Moreimportantly, the technique is applicable and useful to thefollow-up of known and presumably treated lesions.
To optimize MRI, there are two attributable tech-niques in post-operative images; right-angled planes tothe articular surface and MTC sequences. Although pre-vious studies did not mention the imaging planes indetail,8,9 our data showed that these findings are criticalfor improving the clinical significance of MRI. The exactlocation of lesions must be considered to obtain reliableand useful MRIs, because posterior aspects of the fem-oral condyles can not be delineated precisely with con-ventional coronal and sagittal planes. The average con-tact angle of chondral lesions with the tibial joint surfacewas about 30o of flexion in the study group. Thus, werecommend taking a coronal section tilted at 30o to thefemoral shaft if the location of lesions is not known. Theplane is concurrently adjusted17 vertical to the tibialsurface with the knee at 40o of flexion (Fig. 5).
MTC improves the cartilage/fluid contrast14,18 anddelineates remaining thin cartilage layers, establishingthus an effective avenue in discriminating full-thicknessfrom partial thickness defects. This information is criticalfor the indication of invasive therapies. Because thesignal intensity of articular cartilages approximates tothat of synovial fluid in T1- and T2-weighted gradient-echo images and proton density spin echo images, theoutline of cartilage is difficult to define without MTCimages. Although some investigators have reported a
subtraction technique involving images performed withand without MTC,13,14,18we utilized the imaging tech-nique without subtraction and obtained satisfactory visu-alizations because we minimized the acquisition timeand avoided artifacts due to movement of patients todepict small lesions. Fat-suppressed images are alsopowerful for cartilage,19 and the sensitivity and accuracyare similar to those of MTC images.13,18 One of thesesequences should be applied to chondral lesions whenfurther investigation is required.
In summary, routine MRIs are sufficient in daily clin-ics to detect severe chondral lesions that require furtherexamination, and the optimized images are of great ben-efit in regard to recently developed surgical therapies forarticular cartilage defects and the follow-up of knownand presumably treated lesions.
Acknowledgments—The authors thank Hideaki Kawamitsu, R.T., of theMRI Center, and Eiji Fukuba, M.D. of the Department of Radiology fortheir superb technical assistance and discussion. No benefits in anyform have been received or will be received from a commercial partyrelated directly or indirectly to this article. No funds were received insupport of this study.
REFERENCES
1. Brittberg, M.; Lindahl, A.; Nilsson, A.; Ohlsson, C.; Isaks-son, O.; Peterson, L. Treatment of deep cartilage defects inthe knee with autologous chondrocyte transplantation.N. Engl. J. Med. 331:889–895; 1994.
2. Convery, F.R.; Meyers, M.H.; Akerson, W.H. Fresh osteo-chondral allografting of the femoral condyle. Clin. Orthop.273:139–145; 1991.
3. Garrett, J.C. Fresh osteochondral allograft for treatment ofarticular defect in osteochondritis dissecans of the lateralfemoral condyle in adults. Clin. Orthop. Rel. Res. 303:33–37; 1994.
4. O’Driscoll, S.W.; Keeley, F.W.; Salter, R.B. Durability ofregenerated articular cartilage produced by free autogenousperiosteal grafts in major full-thickness defects in jointsurfaces under the influence of continuous passive motion.J. Bone Joint Surg. 70-A:595–606; 1998.
5. Adams, M.E.; Atkinson, M.H.; Lussier, A.J.; Schulz, J.I.;Siminovitch, K.A.; Wade, J.P.; Zummer, M. The role ofviscosupplementation with hylan G-F 20 (Synvisc) in thetreatment of osteoarthritis of the knee: A Canadian multi-center trial comparing hylan G-F 20 alone, hylan G-F 20 w,hylan G-F 20 with non-steroidal anti-inflammatory drugs(NSAIDs) and NSAIDs alone. Osteoarthritis Cartilage.3:213–225; 1995.
6. Messner, K.; Gillquist, J. Cartilage repair: A critical re-view. Acta. Orthop. Scand. 67:523–529; 1996.
7. Recht M.P.; Piraino D.W.; Paletta G.A.; Schils J.P.; Bel-hobek, G.H. Accuracy of fat-suppressed three-dimensionalspoiled gradient-echo FLASH MR imaging in the detec-tion of patellofemoral articular cartilage abnormalities. Ra-diology 198:209–212; 1996.
8. Gelb, H.J.; Glasgow, S.G.; Sapega, A.A.; Torg, J.S. Mag-
Fig. 5. Recommended image plane tilted at 30° to the femoralshaft with the knee at 40° of flexion, when the location ofchondral lesions is unknown.
Focal chondral lesions● R. MORI ET AL. 1139

netic resonance imaging of knee disorders; Clinical valueand cost-effectiveness in a sports medicine practice. Am. J.Sport Med. 24:99–103; 1996.
9. Munk, B.; Madsen, F.; Lundorf, E.; Staunstrup, H.;Schmidt, S.A.; Bolvig, L.; Hellfritzsch, M.B.; Jensen, J.Clinical magnetic resonance imaging and arthroscopicfindings in knees: A comparative prospective study ofmeniscus anterior cruciate ligament and cartilage lesions.Arthroscopy 14:171–175; 1998.
10. Hayes, C.W.; Conway, W.F. Evaluation of articular carti-lage: Radiographic and cross-sectional imaging tech-niques. Radiographics 12:409–428; 1992.
11. Recht, M.P.; Resnick, D. Magnetic resonance imaging ofarticular cartilage: Tthe state of the art. J. Rheumatol.43(Suppl.):52–55; 1995.
12. Ochi, M.; Sumen, Y.; Kanda, T.; Ikuta, Y.; Itoh, K. Thediagnostic value and limitation of magnetic resonance im-aging on chondral lesions in the knee joint. Arthroscopy10:176–183; 1994.
13. Brossmann, J.; Frank, L.R.; Pauly, J.M.; Boutin, R.D.;Pedowitz, R.A.; Haghighi, P.; Resnick, D. Short echo timeprojection reconstruction MR imaging of cartilage: Com-parison with fat-suppressed spoiled GRASS and magneti-
zation transfer contrast MR imaging. Radiology 203:501–507; 1997.
14. Wolff, S.D.; Chesnick, S.; Frank, J.A.; Lim, K.O.; Bala-ban, R.S. Magnetization transfer contrast. MR imaging ofthe knee. Radiology 179:623–628; 1991.
15. Mankin, H.J. The reaction of articular cartilage to injuryand asteoarthritis. Part 1 and 2. N. Engl. J. Med. 291:1285–1292:1335–1340; 1974.
16. Shapiro, F.; Koide, S.; Melvin, J.G. Cell origin and differ-entiation in the repair of full-thickness defects of articularcartilage. J. Bone Joint Surg. 75A:532–553; 1993.
17. Rosenberg, T.D.; Paulos, L.E.; Parker, R.D.; Coward,D.B.; Scott, S.M. The forty-five-degree posteroanteriorflexion weight-bearing radiograph of the knee. J. BoneJoint Surg. 70A:1479–1482; 1988.
18. Peterfy, C.G.; Majumdar, S.; Lang, P.; Van Dijke, C.F.;Sack, K.; Genant, H.K. MR imaging of the arthritic knee:Improved discrimination of cartilage, synovium, and effu-sion with pulsed saturation transfer and fat-suppressedT1-weighted sequences. Radiology 192:413–419; 1994.
19. Disler, D.G. Fat-suppressed three-dimensional spoiled gra-dient-recalled MR imaging: Assessment of articular andphyseal hyaline cartilage. Am. J. Roentgenol. 169:1117–1123; 1997.
1140 Magnetic Resonance Imaging● Volume 17, Number 8, 1999