Embed Size (px)
Citation preview

Coexistence of Chronic Myelogenous Leukemia and Chronic Lymphocytic Leukemia
ZWI A. SCHREIBER, MD,’ MORTON R. AXELROD, MD,t AND LOOL S. ABEBE, MD*
A 55-year-old man is reported who initially developed chronic lymphocytic leukemia. Seven years later, after chemotherapy with chlorambucil, chronic myelogenous leukemia was diagnosed in addition to the chronic lymphocytic leukemia. Four previously reported cases with the same sequence of events are reviewed as well as cases of chronic myelogenous leukemia following chemotherapy alone.
Cancer 54:697-701, 1984.
N CHRONIC LYMPHOCYTIC LEUKEMIA, morphologically I mature lymphocytes accumulate and gradually oblit- erate the lymphoreticular network, appearing in the pe- ripheral blood, bone marrow, lymph nodes, and spleen. l In the majority of these patients, the lymphocyte mor- phology remains the same during the course of the illness. Rarely, however, is chronic lymphocytic leukemia re- ported to have terminated as a “blastic transf~rmation,”~~~ as diffuse histiocytic and acute l e ~ k e m i a . ~ We now report a patient who first developed chronic lymphocytic leukemia, and came back 7 years later with coexisting chronic myelogenous leukemia.
Case Report
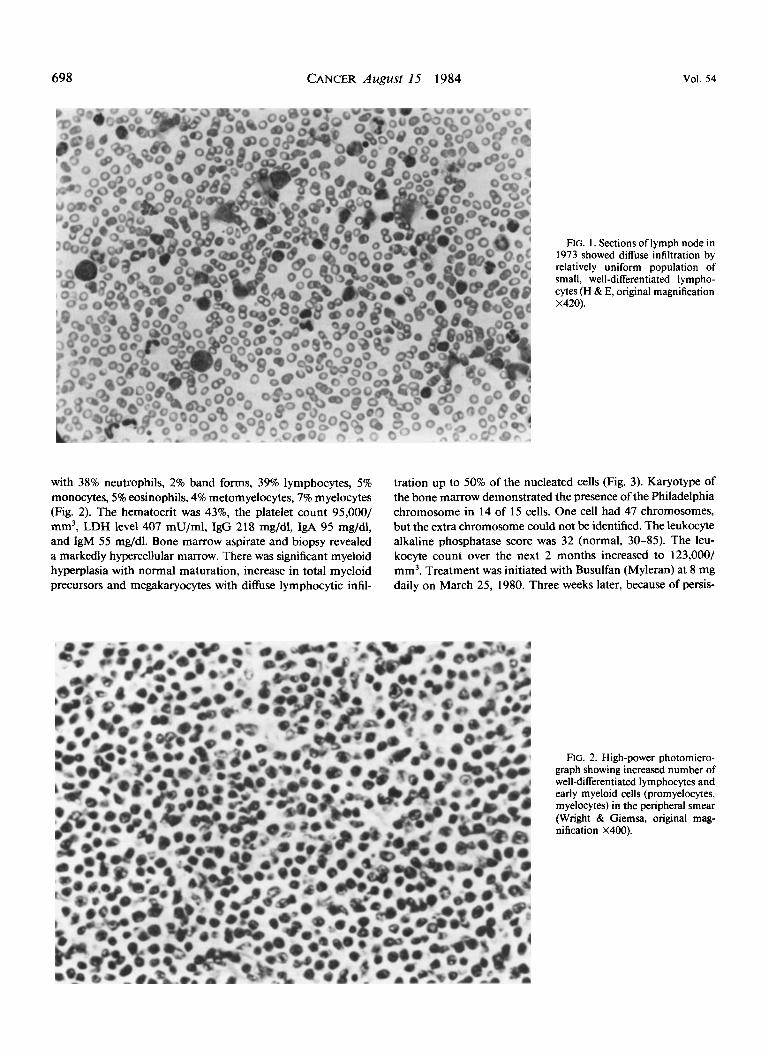
A 55-year-old man was seen in November 1972 because of weakness, easy fatigability, and repeated episodes of sore throat with fever. The past history was unremarkable. On physical examination, he had moderate cervical lymph node enlargement with nonpalpable liver and spleen. Laboratory data revealed a leukocyte count of 10,800/mm3 with 49% neutrophils, 5 1% lymphocytes, hematocrit 45%, and platelet count 1 20,000/mm3. Bone marrow aspirate and biopsy revealed diffuse infiltration by well-differentiated lymphocytes accounting for 50% of the marrow nucleated cells. Cervical lymph node biopsy (Fig. 1)
From the Departments of Medicine and Pathology, Bronx-Lebanon Hospital Center, and the Albert Einstein College of Medicine, Bronx, New York.
* Chief, Division of Hematology, Department of Medicine, Bronx- Lebanon Hospital Center, Assistant Professor of Medicine, Albert Einstein College of Medicine.
t Chief, Division of Oncology, Department of Medicine, Bronx-Leb- anon Hospital Center, Assistant Professor of Medicine, Albert Einstein College of Medicine.
$Chief of Hematology Laboratory, Director of Blood Bank, De- partment of Pathology, Bronx-Lebanon Hospital Center, Assistant Pro- fessor of Pathology, Albert Einstein College of Medicine.
Address for reprints: Zwi A. Schreiber, MD, 1650 Selwyn Avenue 3C, Bronx, NY 10457.
Accepted for publication May 27, 1983.
showed obliteration of the lymphoid architecture by similar uniform well-differentiated lymphocytes. Serum immunoglob- ulins values were IgG 750 mg/dl, IgA 87 mg/dl, and IgM 42 mg/dl. Direct and indirect antiglobulin tests were negative.
In March 1973, a bipedal lymphangiogram revealed large retroperitoneal lymph nodes suggestive of lymphomatous in- volvement. During the subsequent 2 years, a progressive increase in the leukocyte count was noted, reaching 28,200/mm3 with 80% lymphocytes and 18% neutrophils on March 5, 1975, and at this time, the splenic tip became palpable. Two years later on May 14, 1977, his leukocyte count increased to 250,000/ mm3 with 9 1% lymphocytes and 3% neutrophils, hematocrit 48%, and platelet count 190,000/mm3. The spleen was palpable 14 cm and the liver 4 cm below their respective costal margins, and he was noted to have moderate generalized lymph node enlargement. On May 14, 1977 he was started on 8 mg of chlorambucil with 40 mg of prednisone daily. Two weeks later, the chlorambucil dose was decreased to 4 mg daily, and the prednisone was reduced to 20 mg daily. Two months later, the prednisone was discontinued because of pedal edema and di- abetes. The chlorambucil was given at a dose of 4 mg daily up to October 13, 1977 when it was discontinued because of a leukocyte count of 5400/mm3. The spleen size decreased to 5 cm and the liver to 2 cm below their respective costal margins. A progressive rise in the leukocyte count as well as an increase in the liver and spleen size occurred over the next 1 year. On December 9, 1978, chlorambucil chemotherapy was resumed at a dose of 4 mg daily because of marked hepatosplenomegaly and a leukocyte count of 1 82,000/mm3, with 94% lymphocytes and 3% neutrophils.
The chlorambucil was again stopped on March 14, 1979 because of a leukocyte count of 4500/mm3. The total cumulative dose of chlorambucil that the patient ingested was 924 mg. During the years 1977 to 1980, the patient had frequent throat infections, and was hospitalized in 1978 and again in 1980 because of pneumonia. On February 25, 1980, he complained of weakness and enlarging abdominal girth. On examination, he was found to have generalized lymph node enlargement; the liver was palpable 10 cm and the spleen 24 cm below their respective costal margins. The leukocyte count was 68,900/mm3,
697
698 CANCER August 15 1984 VOl. 54
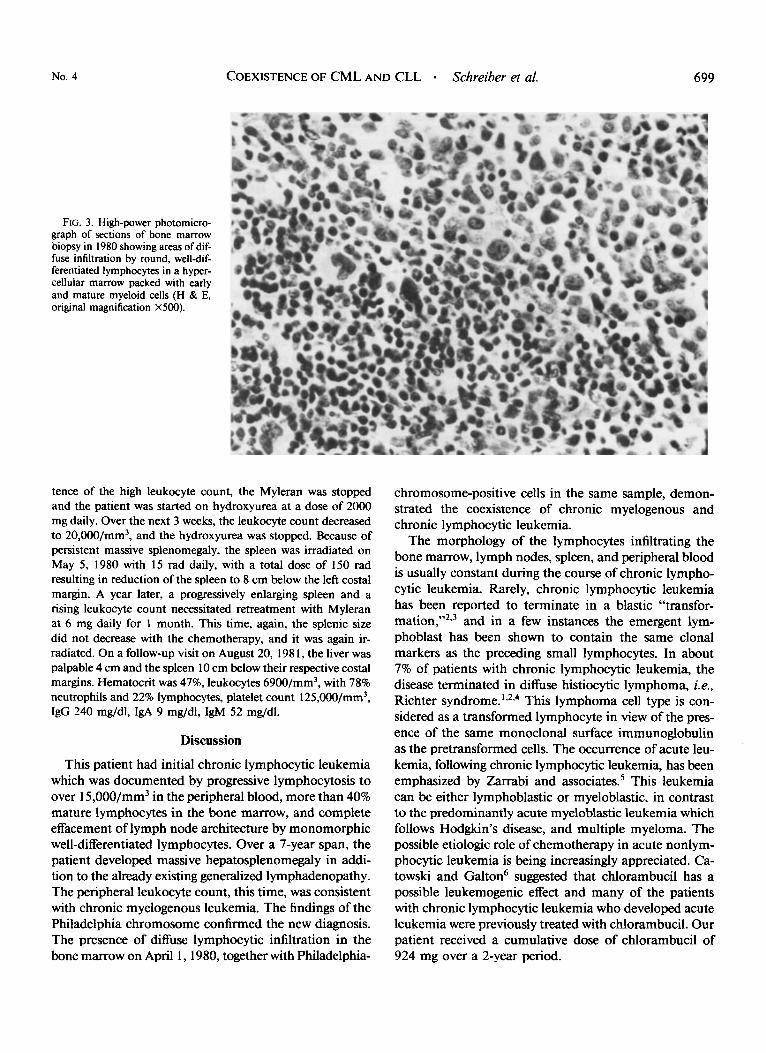
with 38% neutrophils, 2% band forms, 39% lymphocytes, 5% monocytes, 5% eosinophils, 4% metomyelocytes, 7% myelocytes (Fig. 2). The hematocrit was 43%, the platelet count 95,000/ mm3, LDH level 407 mU/ml, IgG 218 mg/dl, IgA 95 mg/dl, and IgM 55 rng/dl. Bone marrow aspirate and biopsy revealed a markedly hypercellular marrow. There was significant myeloid hyperplasia with normal maturation, increase in total myeloid precursors and megakaryocytes with diffuse lymphocytic infil-
FIG. I . Sections of lymph node in 1973 showed diffuse infiltration by relatively uniform population of small, well-differentiated lympho- cytes (H & E, original magnification X420).
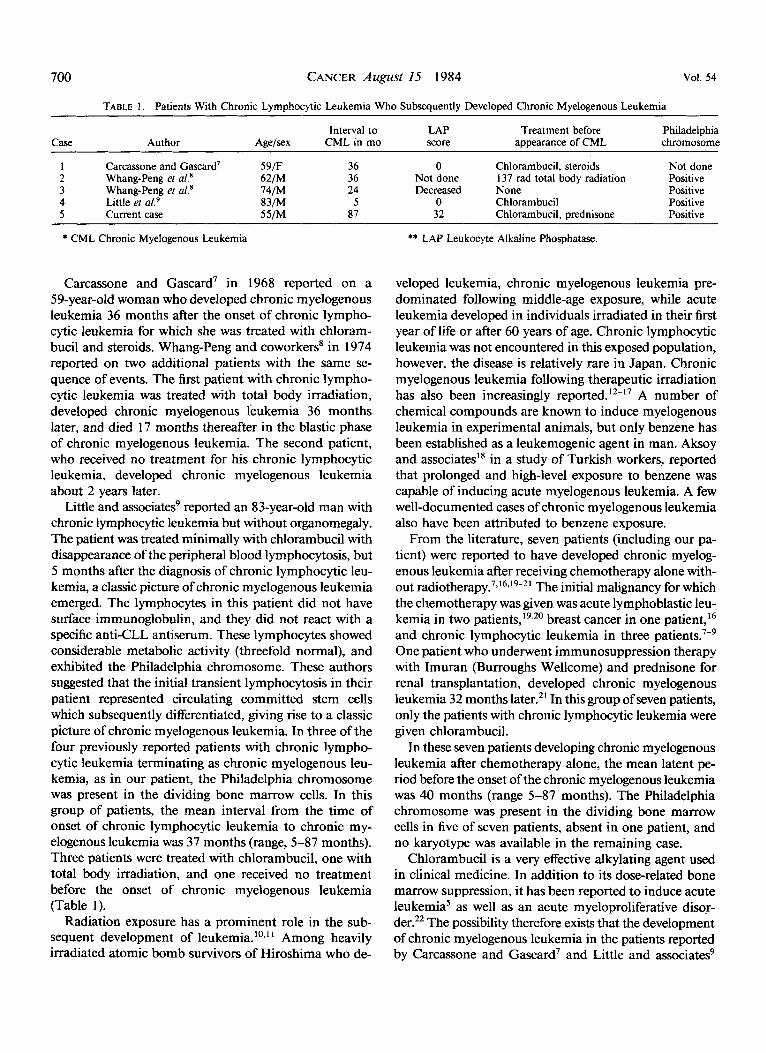
tration up to 50% of the nucleated cells (Fig. 3). Karyotype of the bone marrow demonstrated the presence of the Philadelphia chromosome in 14 of I5 cells. One cell had 47 chromosomes, but the extra chromosome could not be identified. The leukocyte alkaline phosphatase score was 32 (normal, 30-85). The leu- kocyte count over the next 2 months increased to 123,000/ mm3. Treatment was initiated with Busulfan (Myleran) at 8 mg daily on March 25, 1980. Three weeks later, because of persis-
FIG. 2. High-power photomicro- graph showing increased number of well-differentiated lymphocytes and early myeloid cells (promyelocytes, myelocytes) in the peripheral smear (Wright & Giemsa, original mag- nification X400).
No. 4 COEXISTENCE OF CML AND CLL Schreiber et al. 699
FIG. 3. High-power photomicro- graph of sections of bone marrow biopsy in 1980 showing areas of dif- fuse infiltration by round, well-dif- ferentiated lymphocytes in a hyper- cellular marrow packed with early and mature myeloid cells (H & E, original magnification X500).
tence of the high leukocyte count, the Myleran was stopped and the patient was started on hydroxyurea at a dose of 2000 mg daily. Over the next 3 weeks, the leukocyte count decreased to 20,000/mm3, and the hydroxyurea was stopped. Because of persistent massive splenomegaly, the spleen was irradiated on May 5 , 1980 with 15 rad daily, with a total dose of 150 rad resulting in reduction of the spleen to 8 cm below the left costal margin. A year later, a progressively enlarging spleen and a rising leukocyte count necessitated retreatment with Myleran at 6 mg daily for 1 month. This time, again, the splenic size did not decrease with the chemotherapy, and it was again ir- radiated. On a follow-up visit on August 20, 198 1, the liver was palpable 4 cm and the spleen 10 cm below their respective costal margins. Hematwrit was 47%, leukocytes 6900/mm3, with 78% neutrophils and 22% lymphocytes, platelet count 1 25,W/mm3, IgG 240 mg/dl, IgA 9 mg/dl, IgM 52 mg/dl.
Discussion
This patient had initial chronic lymphocytic leukemia which was documented by progressive lymphocytosis to over 1 5,000/mm3 in the peripheral blood, more than 40% mature lymphocytes in the bone marrow, and complete effacement of lymph node architecture by monomorphic well-differentiated lymphocytes. Over a 7-year span, the patient developed massive hepatosplenomegaly in addi- tion to the already existing generalized lymphadenopathy. The peripheral leukocyte count, this time, was consistent with chronic myelogenous leukemia. The findings of the Philadelphia chromosome confirmed the new diagnosis. The presence of diffuse lymphocytic infiltration in the bone marrow on April 1,1980, together with Philadelphia-
chromosome-positive cells in the same sample, demon- strated the coexistence of chronic myelogenous and chronic lymphocytic leukemia.
The morphology of the lymphocytes infiltrating the bone marrow, lymph nodes, spleen, and peripheral blood is usually constant during the course of chronic lympho- cytic leukemia. Rarely, chronic lymphocytic leukemia has been reported to terminate in a blastic “transfor- mati~n,”*,~ and in a few instances the emergent lym- phoblast has been shown to contain the same clonal markers as the preceding small lymphocytes. In about 7% of patients with chronic lymphocytic leukemia, the disease terminated in diffuse histiocytic lymphoma, i.e., Richter This lymphoma cell type is con- sidered as a transformed lymphocyte in view of the pres- ence of the same monoclonal surface immunoglobulin as the pretransformed cells. The occurrence of acute leu- kemia, following chronic lymphocytic leukemia, has been emphasized by Zarrabi and associate^.^ This leukemia can be either lymphoblastic or myeloblastic, in contrast to the predominantly acute myeloblastic leukemia which follows Hodgkm’s disease, and multiple myeloma. The possible etiologic role of chemotherapy in acute nonlym- phocytic leukemia is being increasingly appreciated. Ca- towski and Galton6 suggested that chlorambucil has a possible leukemogenic effect and many of the patients with chronic lymphocytic leukemia who developed acute leukemia were previously treated with chlorambucil. Our patient received a cumulative dose of chlorambucil of 924 mg over a 2-year period.
700 CANCER August 15 1984 Vol. 54
TABLE 1. Patients With Chronic Lymphocytic Leukemia Who Subsequently Developed Chronic Myelogenous Leukemia ~~ ~
Interval to LAP Treatment before Philadelphia Case Author Agelsex CML in mo score appearance of CML chromosome
I Carcassone and Gascard' 59/F 36 0 Chlorambucil, steroids Not done 2 Whang-Peng et al.' 62/M 36 Not done 137 rad total body radiation Positive 3 Whang-Peng et al.' 14/M 24 Decreased None Positive 4 Little et aL9 83/M 5 0 Chlorambucil Positive 5 Current case 55/M 81 32 Chlorambucil, prednisone Positive
* CML Chronic Myelogenous Leukemia
Carcassone and Gascard7 in 1968 reported on a 59-year-old woman who developed chronic myelogenous leukemia 36 months after the onset of chronic lympho- cytic leukemia for which she was treated with chloram- bucil and steroids. Whang-Peng and coworkers' in 1974 reported on two additional patients with the same se- quence of events. The first patient with chronic lympho- cytic leukemia was treated with total body irradiation, developed chronic myelogenous leukemia 36 months later, and died 17 months thereafter in the blastic phase of chronic myelogenous leukemia. The second patient, who received no treatment for his chronic lymphocytic leukemia, developed chronic myelogenous leukemia about 2 years later.
Little and associates' reported an 83-year-old man with chronic lymphocytic leukemia but without organomegaly. The patient was treated minimally with chlorambucil with disappearance of the peripheral blood lymphocytosis, but 5 months after the diagnosis of chronic lymphocytic leu- kemia, a classic picture of chronic myelogenous leukemia emerged. The lymphocytes in this patient did not have surface immunoglobulin, and they did not react with a specific anti-CLL antiserum. These lymphocytes showed considerable metabolic activity (threefold normal), and exhibited the Philadelphia chromosome. These authors suggested that the initial transient lymphocytosis in their patient represented circulating committed stem cells which subsequently differentiated, giving rise to a classic picture of chronic myelogenous leukemia. In three of the four previously reported patients with chronic lympho- cytic leukemia terminating as chronic myelogenous leu- kemia, as in our patient, the Philadelphia chromosome was present in the dividing bone marrow cells. In this group of patients, the mean interval from the time of onset of chronic lymphocytic leukemia to chronic my- elogenous leukemia was 37 months (range, 5-87 months). Three patients were treated with chlorambucil, one with total body irradiation, and one received no treatment before the onset of chronic myelogenous leukemia (Table 1).
Radiation exposure has a prominent role in the sub- sequent development of leukemia. ' Among heavily irradiated atomic bomb survivors of Hiroshima who de-
** LAP Leukocyte Alkaline Phosphatase.
veloped leukemia, chronic myelogenous leukemia pre- dominated following middle-age exposure, while acute leukemia developed in individuals irradiated in their first year of life or after 60 years of age. Chronic lymphocytic leukemia was not encountered in this exposed population, however, the disease is relatively rare in Japan. Chronic myelogenous leukemia following therapeutic irradiation has also been increasingly rep~rted. '~- '~ A number of chemical compounds are known to induce myelogenous leukemia in experimental animals, but only benzene has been established as a leukemogenic agent in man. Aksoy and associates" in a study of Turkish workers, reported that prolonged and high-level exposure to benzene was capable of inducing acute myelogenous leukemia. A few well-documented cases of chronic myelogenous leukemia also have been attributed to benzene exposure.
From the literature, seven patients (including our pa- tient) were reported to have developed chronic myelog- enous leukemia after receiving chemotherapy alone with- out radi~therapy.','~~''-~' The initial malignancy for which the chemotherapy was given was acute lymphoblastic leu- kemia in two patient^,'',^' breast cancer in one patient,16 and chronic lymphocytic leukemia in three One patient who underwent immunosuppression therapy with Imuran (Burroughs Wellcome) and prednisone for renal transplantation, developed chronic myelogenous leukemia 32 months later." In this group of seven patients, only the patients with chronic lymphocytic leukemia were given chlorambucil.
In these seven patients developing chronic myelogenous leukemia after chemotherapy alone, the mean latent pe- riod before the onset of the chronic myelogenous leukemia was 40 months (range 5-87 months). The Philadelphia chromosome was present in the dividing bone marrow cells in five of seven patients, absent in one patient, and no karyotype was available in the remaining case.
Chlorambucil is a very effective alkylating agent used in clinical medicine. In addition to its dose-related bone marrow suppression, it has been reported to induce acute leukemia5 as well as an acute myeloproliferative disoF- der.22 The possibility therefore exists that the development of chronic myelogenous leukemia in the patients reported by Carcassone and Gascard7 and Little and associatesg

No. 4 COEXISTENCE OF CML AND CLL - Schreiber el a/. 70 1
and in our patient is due to the preceding chlorambucil chemotherapy.
REFERENCES
I. Sweet DJ, Golomb H, Ultmann JE. The clinical features of chronic lymphocytic leukemia. Clin Haematol 1977; 6: 185-202.
2. Brouet JC, Seligmann M. Chronic lymphocytic leukemia as an immunoproliferative disorder. Clin Haematol 1977; 6: 168-1 84.
3. Brouet JC, Preud‘Homme JL, Seligmann M, Bernard J. Blast cells with monoclonal surface immunoglobulin in two cases of acute blast crisis supervening on chronic lymphocytic leukemia. Br Med J 1973;
4. Trump LD, Mann RB, Phelps R, Roberts H, Conley CL. Richter’s Syndrome: Diffuse histiocytic lymphoma in patients with chronic lym- phocytic leukemia. Am J Med 1980; 68539-548.
5 . Zarrabi MH, Grunwald HW, Rosner F. Chronic lymphocytic leu- kemia terminating in acute leukemia. Arch Intern Med 1977; 137: 1059- 1064.
6. Catovsky D, Galton DAG. Myelomonmytic leukemia supervening on chronic lymphocytic leukemia. Lancet 1971; 1:478-479.
7. Carcassone Y, Gascard E. Leucemie myeloide succedant a une leucemie lymphoide. Marseille Midical 1968; 105:339-34 I .
8. Whang-Peng J, Gralnick HR, Johnson RE, Lee EC, Lear A. Chronic granulocytic leukemia (CGL) during the course of chronic lymphocytic leukemia (CLL): Correlation of blood, marrow, and spleen morphology and cytogenetics. Blood 1974; 43:333-339.
9. Little T, Faguet GB, Agee JF, Garver FA. Chronic myelogenous leukemia emerging from chronic lymphatic leukemia: Evidence for the evolution of a singie clone (Abstr). Blood 1981; (Suppl) 58:145a.
10. Heyssel R. Leukemia in Hiroshima atomic bomb suMvors. Blood
I I . Bizzozera OJ, Johnson KG, Ciocco A, Kawasaki S, Toyoda S.
IV23-24.
1960; 15~313-33 1.
Radiation related leukemia in Hiroshima and Nagasaki 1946-1964. Ann Intern Med 1967; 66522-530.
12. Faber M, Borum C. Leukemia and a malignant tumor in the same patient. Br J Haematol 1962; 8:313-321.
13. Ezdinli EZ, Sokel JE, Aungst CW, Kum U, Sandkrg AA. Myeloid leukemia in Hodglun’s disease: Chromosomal abnormalities. Ann Intern Med 1969; 71:1097-1104.
14. Johnson FD, Jacobs EM, Wood DA. Hodglun’s disease termi- nating in chronic myeloid leukemia. Cal Med 1966; 104:479-484.
15. Swain WR, Windschitl HE, Doscherholmen A, Bankole RO, Bates HA. Chronic myelogenous leukemia in Hodglun’s disease. Cancer
16. Rosner F, Carey RW, Zarrabi MH. Breast cancer and acute leu- kemia: Report of 24 cases and review of the literature. Am J Hematol 1978; 4:151-172.
17. Rosner F, Grunwald H. Hodgkin’s disease and acute leukemia: Report of eight cases and review of the literature. Am J Med 1975;
18. Aksoy M, Erdem S, Dincol G. Types of leukemia in chronic benzene poisoning: A study in thirty-four patients. Acta Haematol (Base0
19. Kelsen DP, Gee TS, Chaganti RSK. Philadelphia positive chronic myelogenous leukemia developing in a patient with acute lymphoblastic leukemia. Cancer 1979; 43:1782-1787.
20. Jenkins DW, Rivera HP, Coltmann CA. Case report: Acute lym- phatic leukemia followed by a clinical picture indistinguishable from chronic granulocytic leukemia in the same patient. Am JMed Sci 1972; 264:329-333.
2 1. Lubinsky R, Meyers AM, Disler PB, MacPhail AP, Myburgh JA, Katz J. Chronic granulocytic leukemia in a patient with a renal allograft. Arch Intern Med 1978; 138:1429-1430.
22. Steigbigel RT, Kim H, Potolsky A, Schrier S. Acute myelopro- liferative disorder following long term chlorambucil therapy. Arch Intern Med 1974; 134728-731.
197 1; 27~569-573.
58~339-353.
1976; 55:65-72.





























