Embed Size (px)
Citation preview


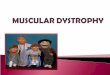
Cogan’s epithelial membrane dystrophy, also named epithelial basement membrane dystrophy (EBMD) and map-dot-fingerprint dystrophy, was first described by Cogan in 1964 as microcystic changes in the corneal epithelium (1), with minute pinpoints and larger, oval, and irregularly shaped grayish white opacities in the superficial corneal epithelium. Guerry completed the clinical description of the typical lesions with the observation of maplike changes, made of irregular, faintly grayish areas, with clear zones interspersed between the millimeter-sized grayish patches (2,3). Trobe and Laibson described in 1972 the complete set of map changes, dots (microcysts) and fingerprints, and highlighted that only few patient present with all typical signs (4). Among 117 patients with a history of recurrent corneal erosions, Hykin et al found EBMD with no previous history of trauma in 23 cases (19.6%)s, and with previous trauma in 8 additional cases (6.8%), while 75 had a history of trauma but no clinical sign of EBMD, and 11 had neither trauma nor EBMD (5).
The primary symptoms of epithelial basement membrane dystrophy are spontaneous recurrent corneal erosions and blurred vision. The pain may persist for days, but it is most often transient and last for only some hours (2). It may be present on awakening, or it can awaken the patient when the eyelids are open during sleep.
The recommended treatments of EBMD is usually based on artificial tears at daytime and lubricating ointments at bedtime, and patching or bandage contact lenses during periods of recurrent erosions. Punctures of abnormal areas may also be used to reinforce the anterior stroma of the cornea (2). However, curing patients with EBMD still remains challenging in most cases.
Heparin sulfate mimetic polymers (HSMP) are usually proposed in corneal matrix diseases inducing epithelial defects, such as neurotrophic keratitis (6, 7, 8). Their mode of action is to mimic the architecture of the extracellular matrix to promote repair of the corneal stroma and then epithelial regeneration. ConsiStent with in vivo confocal microscope results (9), we hypothesized that EMBD could be related to some corneal matrix abnormalities, which in turn could be improved by HSMP.
Introduction
Maps Dots and fingerprints

Method : Prospective, interventional, open-label pilote study
Inclusion criteria:- Objective signs of EBMD (maps and/or dots and/or fingerprints) - Subjective symptoms related to EMBD
(history of recurrent episodes of pain and/or acute episodes of ocular discomfort)- Insufficient efficacy (i.e. no reduction of in the frequency and/or intensity of subjective symptoms
following) of conventional treatments.
Non-inclusion criteria:- Objective or subjective signs of any other disease of the ocular surface (except mild ocular sicca
syndrome and/or mild meibomian gland disease)- Subjects who were breastfeeding or sexually active and who did not fall into 1 of the following
categories (post-menopausal, surgically sterile, following efficient birth control methods)- Subjects participating in any drug or device clinical investigation within 30 days prior to entry into
this study and/or during the period of study participation- Subjects under legal age (18-year-old)- Subjects who were not able and willing to comply with all treatment and follow-up/study procedures
Regimen: Once all inclusion criteria and no inclusion criterion was observed, the patient was given HSMP (Cacicol, THEA), 2 drops per week for at least 3 weeks, in addition to the usual treatment (i.e. artificial tears).Objective and subjective signs were assessed at the end of this run-in period, and regimen was adapted, in accordance with the patient.
Methods
Maps Dots and fingerprints

Results (1)

Results (1)

Conclusions
Maps Dots and fingerprints
Heparan sulfate mimetic polymers seem to have unique properties for alleviating the
subjective symptoms and reducing the frequency of recurrent erosions in epithelial basement
membrane dystrophy. This pilote study needs however to be confirmed by prospective controlled
studies. These results also suggest that EMBD may be related to anterior stromal abnormalities, which
could be improved by heparan sulfate mimetic polymers. This emerging class of topical treatments
appears as promising in such indications.

References
Maps Dots and fingerprints
(1). Cogan DG, Donaldson DD, Kuwabara T, Marshall D. Microcystic dystrophy of the corneal epithelium. Trans. Am. Ophthalmic. Soc. 1964: 63: 213(2) Laibson P. Anterior corneal dystrophies. In Cornea. Fundamentals, Diagnosis and Management. Krachmer JH, Mannis MJ, Holland EJ. Mosby elsevier 2011(3) Guerry D. Observations on Cogan’s microcystic dystrophy on the corneal epithelium. Trans. Am. Ophthalmic. Soc. 1965: 63: 320-334(4) Trobe JD, Laibson PR: Dystrophic changes in the anterior cornea. Arch. Ophthalmol. 1972; 87 : 378-382(5) Hykin PG, Foss AE, Pavesio C, Dart JKG. The natural history and management of recurrent corneal erosion. A prospective randomized trial. Eye 1994; 8 : 35-40(6) Khammari Chebbi C, Kichenin K, Amar N, Warnet JM, Barritault D, Baudouin C. Pilot study of a new matrix therapy agent (RGTA OTR4120) in treatment-resistant corneal ulcers and corneal dystrophy. J Fr Ophtalmol 361 2008;31:465—71.(7) De Monchy I, Pogorzalek N, Gendron G, M’Garrech M, Kaswin G, Labbé A, Labetoulle M: Management of herpes zoster neurotrophic ulcer using a new matrix therapy agent (RGTA): A case report. J. Fr. Ophthalmol. 2012: 35: 187 e1-6(8) Aifa A, Gueudry J, Portmann A, Delcampe A, Muraine M: opical Treatment with a new matrix therapy agent (RGTA) for the treatment of corneal neurotrophic ulcers. Invest Ophthalmol Vis Sci. 2012;53:8181–8185(9) Labbé A , De Nicola R, Dupas B, Auclin F, Baudouin C: Epithelial basement membrane dystrophy, evaluation with the HRT II Rostock cornea module. Ophthalmology 2006;113: 1301–1308.