Colleen Roylance Director of Quality and Education
Slide 2
We are headed into the next century which will focus on quality
.we are leaving one that has been focused on productivity.
8/30/2013 Dr. Joseph M. Juran 1904 - 2008
Slide 3
8/30/2013 Culture of Safety and Quality
PathologicalReactiveBureaucraticProactiveGenerative Systems are
purposefully designed to see no evil, hear no evil and speak no
evil. Actions of improvement only come when necessary to survival
Actions are driven by outside forces and what is perceived to
create negative consequences by regulators or entities with the
power to create such consequences Actions are very task oriented
with most existing to satisfy the rules and requirements of a
bureaucratic structure with little focus on achieving the larger
goal There is a genuine interest in advancing safety and quality
but leaders struggle with cohesively supporting quality as an equal
although safety wins out more and more frequently Safety and
quality are equal to other competing priorities and is an integral
piece of day-to-day operations as leaders recognize its importance
to operational, financial and reputational success
Slide 4
QAPI Defined A systematic approach to assessing services and
improving them on a priority basis Customer Focus Employee
Empowerment Leadership Involvement Data-Informed Practice
Statistical Tools Prevention Over Correction 8/30/2013
Slide 5
What it really boils down to Is this a safe, comfortable place
to receive care? Do people feel comfortable speaking up? How do you
know? 8/30/2013
Slide 6
Lean TQM CQI W. Edwards Deming Joseph Juran SPC DMAIC Taiichi
Ohno 8/30/2013
Slide 7
Slide 8
Value-added actions in the best sequence, without interruption
whenever someone requests them, and perform them more and more
effectively Voice of the Customer and Recognize Waste Visual
Control and 5S Establish Flow: Pull vs. Push and one piece flow
Level the Workload Fool Proof and Standardize LeanSix Sigma
8/30/2013
Slide 9
Slide 10
Quality Product Features Freedom from Deficiencies That
Customers Want Design for Six Sigma At Six Sigma Levels Improve to
Six Sigma 8/30/2013
Slide 11
Lean is about understanding what is important to the customer
Lean increases the activities that add value and decreases or
eliminates those that dont Lean focuses on eliminating waste in
processes (i.e. the waste of time, supplies, transportation) Lean
is about expanding capacity by reducing costs and increasing
process effectiveness What is Lean? 8/30/2013
Slide 12
Key LEAN Leverage Points Eliminate Waste: Eliminate
Inefficiency Standardize Work: Eliminate Variation Key
Implementation Leverage Points Managers and staff working side by
side to solve problems when and where they happen Incremental
improvement over and over and over 8/30/2013
Slide 13
Slide 14
Voice of the Customer ASK: What is the customer paying for? The
answer tells you what adds value and you should keep doing OR what
doesnt add value and you should stop doing. 8/30/2013
Slide 15
3 non-value-adding steps x 3 minutes per step x 25 residents x
3 times per day 675 non-value-adding minutes per day / 60 minutes
in an hour 11.25 hours per day x 365 day per year 4,106.25 hours
per year / 1800 hours in an FTE 2.28 FTEs 8/30/2013
Slide 16
7 Wastes Over production Waiting Motion Inventory 8/30/2013
Transportation Defects Excess processing
Slide 17
7 Wastes: Overproduction Doing what is unnecessary when it is
unnecessary in an unnecessary amount 8/30/2013 Example: Setting up
meal trays for residents only to learn several residents are gone,
thus having to throw out food Solution: Improve communication with
direct care and dietary staff Design form or tear-off for kitchen
when resident(s) leave facility during meal hour (Common on
weekends and during holidays)
Slide 18
7 Wastes: Waiting Staff: For information, approval, supplies
Customers: For assistance, information, supplies, comfort 8/30/2013
Example: Call light not being addressed and residents waiting for
help Solution: Review staffing patterns for timely availability (3
- 5 mins) Staff awareness of high-risk residents patient
safety
Slide 19
7 Wastes: Motion Movement that is too fast, slow or unnecessary
8/30/2013 Example: Not having towels and washcloths in AM for staff
to assist with residents personal hygiene before breakfast
Solution: Night shift stocks towels and washcloths during last
rounds Place at resident bedside as appropriate
Slide 20
7 Wastes: Inventory When anything is retained longer than
necessary 8/30/2013 Example: Outdated supplies or medication
Solution: Design system so medication/supplements and supplies are
checked at least monthly Can be incorporated into night shift
duties while stocking medication carts
Slide 21
7 Wastes: Transportation Transferring or moving unnecessary
items and the problems created 8/30/2013 Example: Supplies are
off-loaded at dock central supply closet floor supply closet
residents room Solution: Solicit supplier to off-load stock to
central supply closet Eliminate floor supply closet and stock
residents rooms
Slide 22
7 Wastes: Defects Related to costs for inspection of defects
8/30/2013 Example: Inadequate communication among shifts Solution:
Improve communication efforts with TeamSTEPPS handoff tools Provide
extra 15 mins between shifts for rounds and questions Utilize
standard handoff tool to address resident safety (i.e., weight
loss, food intake, skin, falls, behavior)
Slide 23
7 Wastes: Excess Processing Unnecessary tasks traditionally
accepted as necessary 8/30/2013 Example: Redundant documentation
for pressure ulcers several different forms and/or documentation
doesnt match Solution: Standardize documentation/assessment form
Wound/treatment binder Keep binder accessible and include policies
and standards
Slide 24
Visual Control Makes abnormalities and waste obvious enough for
anyone to recognize Uses standardized control devices, information,
color coded layout and signboards Successful leadership depends on
visibility of abnormalities 8/30/2013
Slide 25
Method of workplace organization Place for everything;
everything in its place Reduces wastes due: To clutter Time to find
materials and equipment Duplication of equipment Floor space
Inconsistency 5S is essential 8/30/2013
Slide 26
5S Sort: Separate the necessary from the unnecessary Simplify:
Create a place for everything Sweep: Control the work area visually
and physically Standardize: Document agreements made
Self-discipline: Follow through and maintain 8/30/2013
Slide 27
Standardize the least waste way to work Provide low variation
in the output Simplifies training, cross training and sharing
resources Provides a foundation for improvement Standard Operations
Without standard work there can be no improvement. Taiichi Ohno
8/30/2013
Slide 28
Specified Activities Outcome Content Sequence Timing Clear
Connections Every connection must be direct with an unambiguous
yes-or-no way to send requests and receive responses Simple
pathways The pathway for every product and service must be as
simple and direct as possible Basic Principles for Lean
8/30/2013
Slide 29
PDSA and A3 8/30/2013
Slide 30
Slide 31
Project Planning A straightforward project prioritization tool
that effectively ranks projects to ensure the facility is getting
the biggest bang for their buck. 8/30/2013 Projects are mapped on a
spectrum from: Implement immediately Postpone Do not implement
Slide 32
8/30/2013
Slide 33
Dont wait for more than one missed opportunity to evaluate the
process The Power of One 8/30/2013
Slide 34
Root Cause Analysis: Each Time Every Time 8/30/2013 What
Happened? Identify the issue How Did It Happen? Classify the
cause(s) Why Did It Happen? State your findings How Can We Prevent
It from happening again?
Slide 35
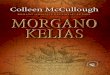
5 Whys Problem Statement: The patient was late to the OR; it
caused a delay. Why? There was a long wait for a transport bed.
Why? A replacement transport bed had to be found. Why? The original
transport beds safety rail was worn and had eventually broken. Why?
It had not been regularly checked for wear. Why? The Root Cause:
There is no equipment maintenance schedule. Setting up a proper
maintenance schedule helps ensure that patients should never again
be late due to faulty equipment. This reduces delays and improves
flow. If you simply repair the bed or do a one-off safety rail
check, the problem may happen again sometime in the future.
8/30/2013
Slide 36
Establish Root Cause(s) A cause and effect diagram, also known
as a fishbone diagram, is a graphic tool used to explore and
display the possible causes of a certain effect.
Slide 37
What Is Failure Mode and Effect Analysis? FMEA is a systematic
method of identifying and preventing problems before they occur.
8/30/2013
Slide 38
RCA vs. FMEA Similarities Interdisciplinary Team Develop Flow
Diagram Focus on systems issues Actions and outcome measures
developed Scoring matrix (severity/probability) Use of cause &
effect diagram, brainstorming Differences Process vs. chronological
flow diagram Prospective (what if) analysis Choose topic for
evaluation Include detectability and criticality in evaluation
Emphasis on testing intervention 8/30/2013
Slide 39
FMEA: Your Crystal Ball FMEA Template 1234567 Step or link in
processList all potential failuresPotential effect Severity of
effect Probability of failure effect Criticality (col. 4x5) Rank by
Criticality 8/30/2013
Slide 40
This material was developed by Mountain-Pacific Quality Health,
the Medicare quality improvement organization for Montana, Wyoming,
Hawaii, Alaska and the Pacific Territories of Guam and American
Samoa and the Commonwealth of the Northern Mariana Islands, under
contract with the Centers for Medicare & Medicaid Services
(CMS), an agency of the U.S. Department of Health and Human
Services. Contents presented do not necessarily reflect CMS policy.
10SOW-MPQHF-WY-IPC-13-10 For More Information: Colleen Roylance
Director of Quality and Education (406) 457-5874
[email protected]