Embed Size (px)
Citation preview
Colorectal Cancer Screening Guidelines: Globalizing Evidence, Localizing Implementation Marguerite Koster, MA, MFT Kaiser Permanente, Southern California Region
2
Overview About Kaiser Permanente Southern California (KPSC) Globalizing the Evidence: KP’s National Colorectal Cancer
Screening Guideline The Knowledge-To-Action Framework Localizing Implementation:
• KP Southern California’s Colorectal Cancer (CRC) Framework/Action Plan • CRC Program Overview and Goals • Fecal Immunochemical Test (FIT) Program Implementation
Performance Measurement/Results
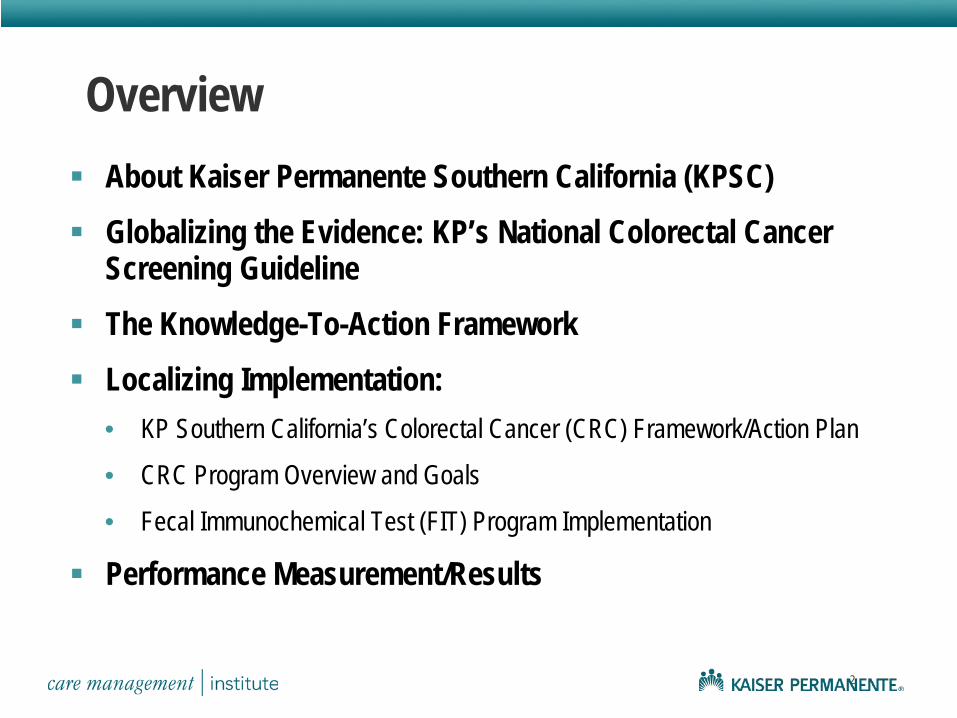
About the KP Southern California (KPSC) Region
150 medical offices 5,300 physicians 18,300 nurses 57,000 employees
3.6 million members 140+ languages spoken 8 counties 13 service areas
KP National Colorectal Cancer (CRC) Screening Guideline Recommendations
KP members at average-risk for CRC: Colorectal cancer screening strongly recommended for all
asymptomatic, average-risk adults aged 50-75. Any of the following tests and frequencies are acceptable
options for screening: • High-sensitivity guaiac fecal occult blood test (gFOBT) every 1-2 years • Immunochemical fecal occult blood test (iFOBT/FIT) every 1-2 years • Flexible sigmoidoscopy at least every 10 years • Colonoscopy every 10 years • A combination of high-sensitivity gFOBT or iFOBT/FIT every 1-2 years and
flexible sigmoidoscopy at least every 10 years.
KPSC CRC Screening Program Challenges and Opportunities CRC screening not a strategic priority before 2005 NCQA accreditation: HEDIS CRC Screening rates were low
(49.5% of eligible population screened) Flexible sigmoidoscopy predominant screening modality
• Issues: No sedation, lack of patient education, “no shows”
Demand for colonoscopy surging • Access to screening colonoscopy a challenge • Region constrained by staffing, facility, other resource limits
Guideline developed, but no region-wide, coordinated implementation effort in place
*National Committee on Quality Assurance (NCQA) **NCQA Health Employer Data Information Set (HEDIS)
KPSC CRC Screening Program Goals and Priorities
Make CRC screening a regional priority – became a So. California Region Clinical Strategic Goal (CSG) in 2005
Implement Fecal Immunochemical Testing (FIT) program Improve colonoscopy throughput Move outreach/inreach efforts from medical center to regional
management Increase provider and patient education efforts Allocate sufficient resources to support screening and outreach
efforts
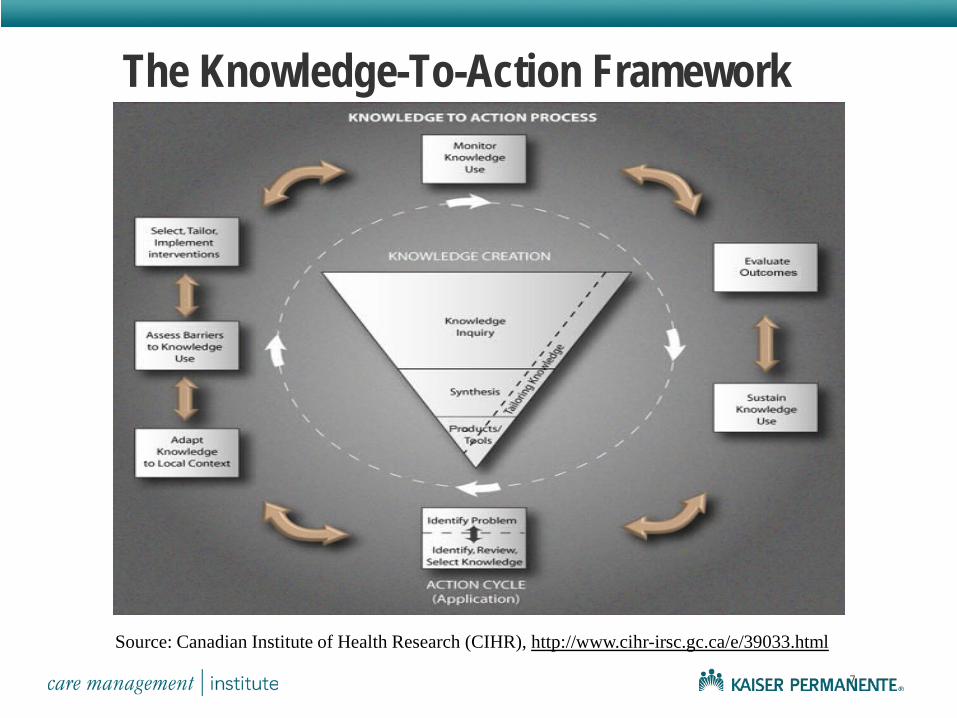
The Knowledge-To-Action Framework
7
Source: Canadian Institute of Health Research (CIHR), http://www.cihr-irsc.gc.ca/e/39033.html
8
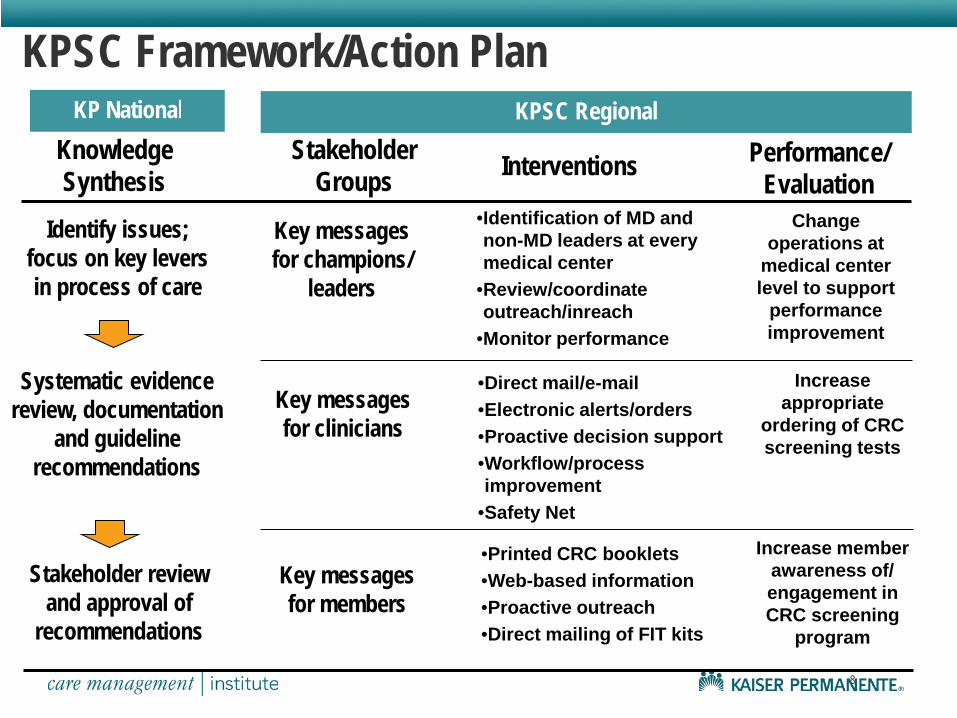
KPSC Framework/Action Plan KP National
Knowledge Synthesis
Stakeholder Groups Interventions Performance/
Evaluation Identify issues;
focus on key levers in process of care
Stakeholder review and approval of
recommendations
Key messages for clinicians
Key messages for members
Key messages for champions/
leaders
•Printed CRC booklets •Web-based information •Proactive outreach •Direct mailing of FIT kits
•Direct mail/e-mail •Electronic alerts/orders •Proactive decision support •Workflow/process improvement
•Safety Net
•Identification of MD and non-MD leaders at every medical center
•Review/coordinate outreach/inreach
•Monitor performance
Increase member awareness of/ engagement in CRC screening
program
Increase appropriate
ordering of CRC screening tests
Change operations at
medical center level to support
performance improvement
Systematic evidence review, documentation
and guideline recommendations
KPSC Regional
Key Message: The Best CRC Screening Method…
…is the One that Gets Done.
+ +
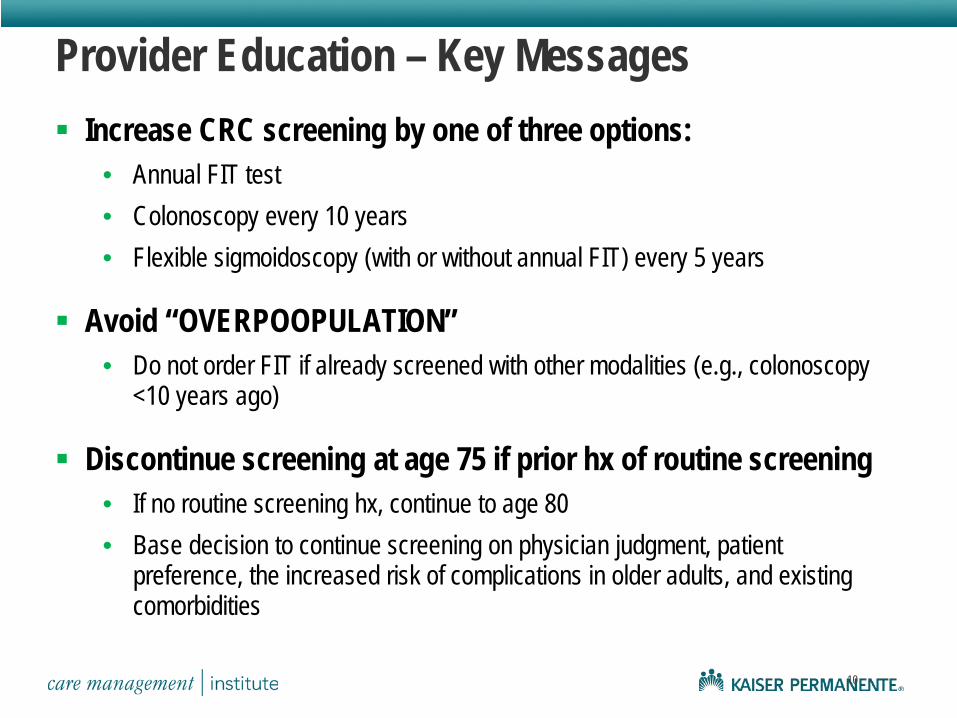
Provider Education – Key Messages Increase CRC screening by one of three options:
• Annual FIT test • Colonoscopy every 10 years • Flexible sigmoidoscopy (with or without annual FIT) every 5 years
Avoid “OVERPOOPULATION” • Do not order FIT if already screened with other modalities (e.g., colonoscopy
<10 years ago)
Discontinue screening at age 75 if prior hx of routine screening • If no routine screening hx, continue to age 80 • Base decision to continue screening on physician judgment, patient
preference, the increased risk of complications in older adults, and existing comorbidities
10
11
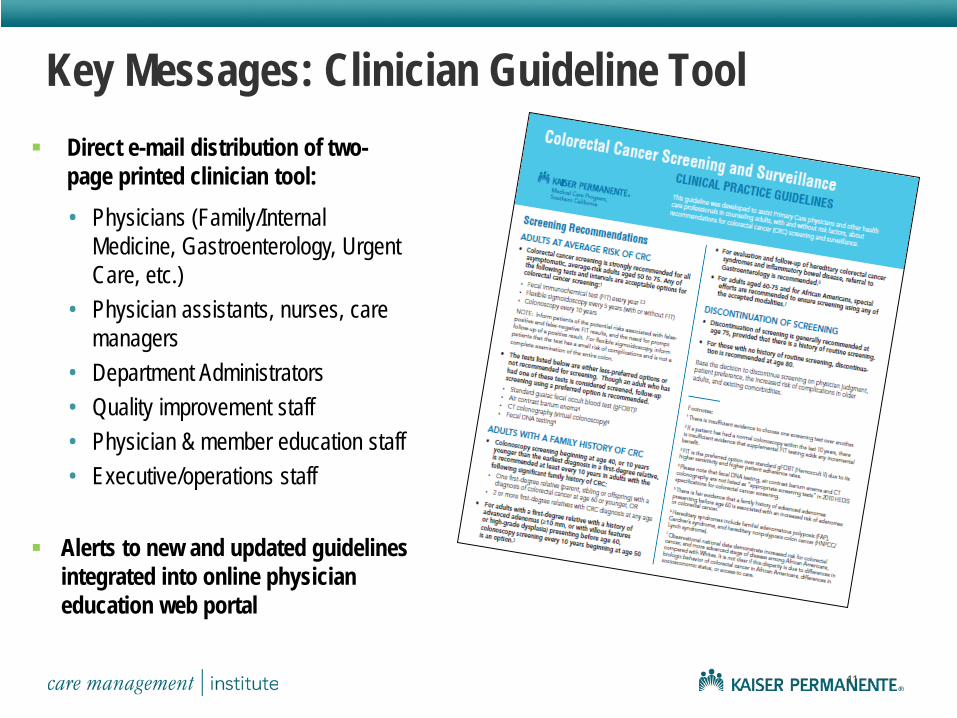
Key Messages: Clinician Guideline Tool
• Physicians (Family/Internal Medicine, Gastroenterology, Urgent Care, etc.)
• Physician assistants, nurses, care managers
• Department Administrators • Quality improvement staff • Physician & member education staff • Executive/operations staff
Direct e-mail distribution of two-page printed clinician tool:
Alerts to new and updated guidelines integrated into online physician education web portal
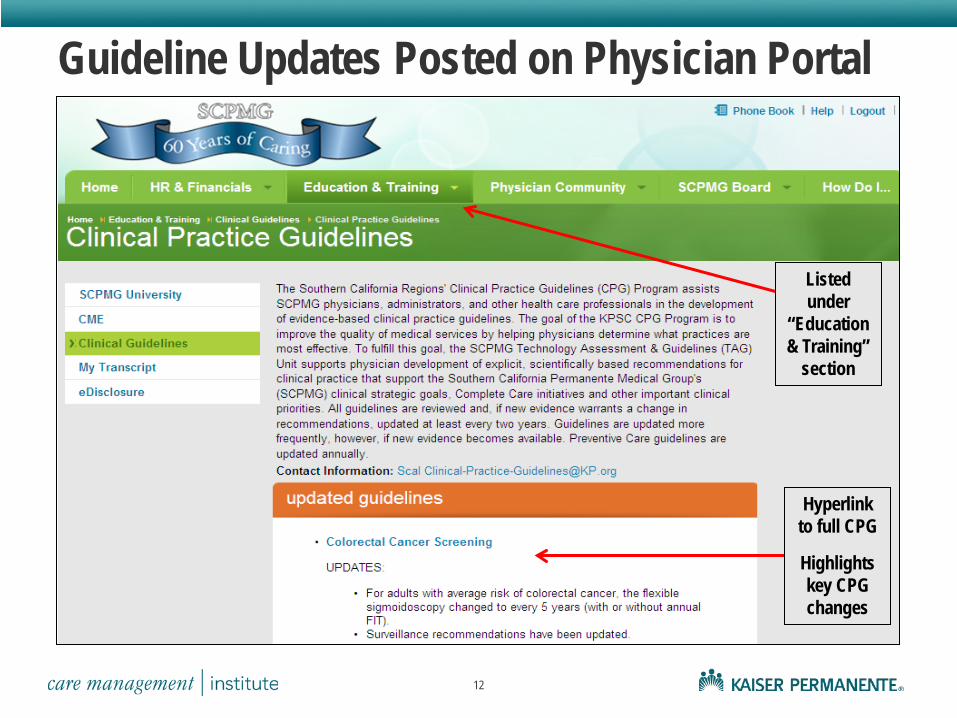
Guideline Updates Posted on Physician Portal
12
Listed under
“Education & Training”
section
Hyperlink to full CPG
Highlights key CPG changes
13
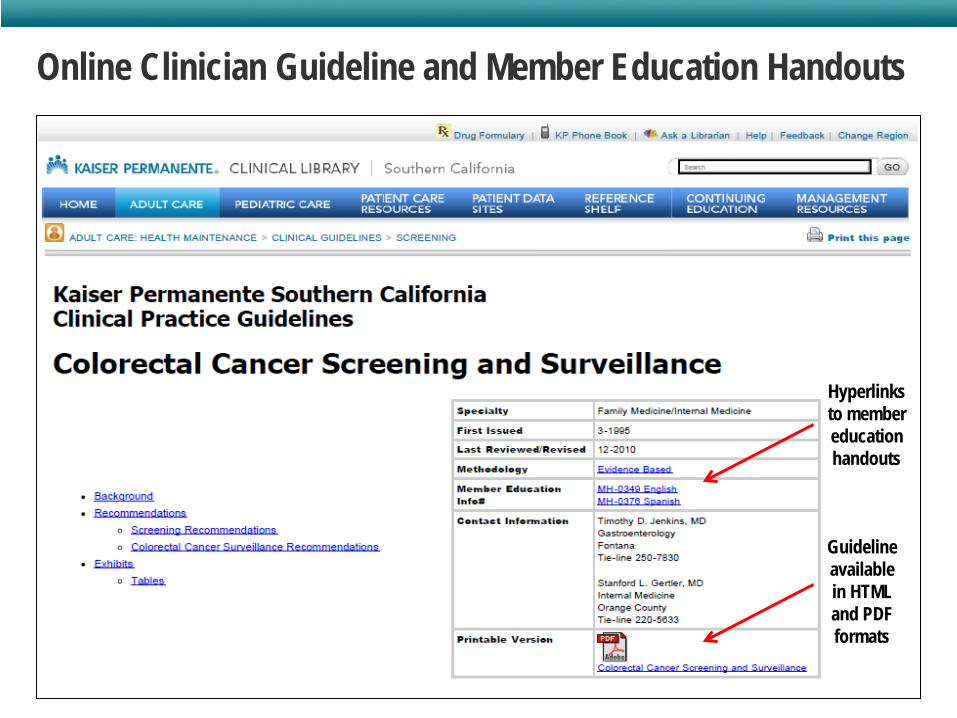
Online Clinician Guideline and Member Education Handouts
Content posted on KP Clinical Library intranet web site:
Hyperlinks to member education handouts
Guideline available in HTML and PDF formats
14
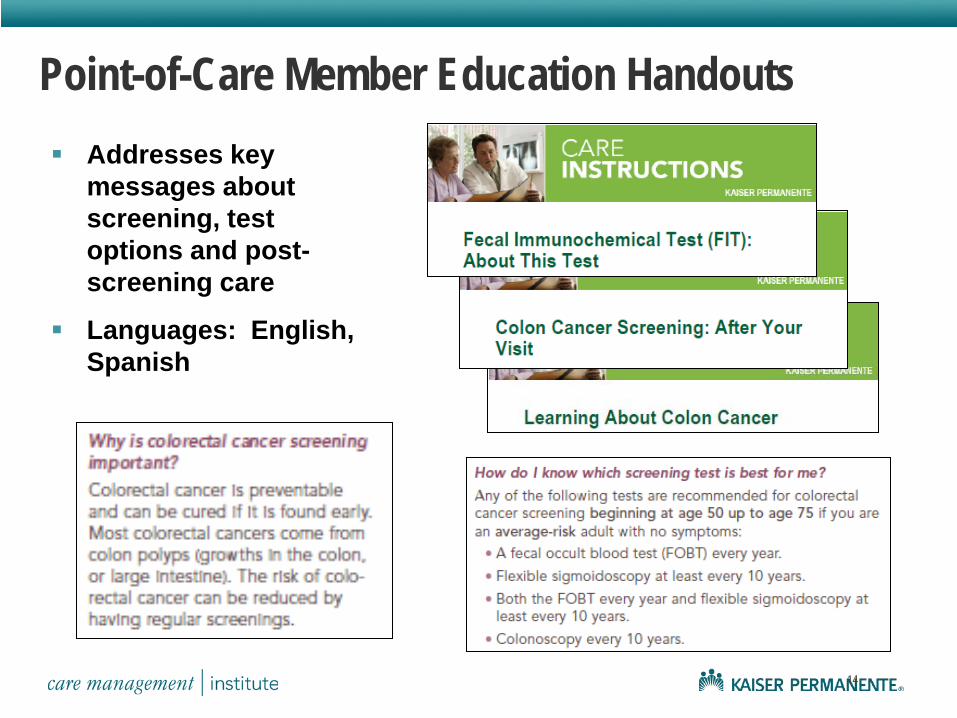
Point-of-Care Member Education Handouts Addresses key
messages about screening, test options and post-screening care
Languages: English, Spanish
Fecal Immunochemical Test (FIT) Program Overview Regional Outreach
• Direct mailing of FIT kits to members
Regional Inreach • Proactive Office Encounter (POE) • Electronic Health System “Best Practice Alerts” • During office visit
Replace Hemoccult with FIT ONLY if due for CRC screening
“Ultimate Inreach” – physician collects fecal sample for FIT kit during digital rectal exam
Positive FIT Safety Net • Case managers track and monitor patients who have positive FOBT/FIT results • Creates a database of the colorectal cancer screening population to ensure
patient with positive tests are not lost to follow-up
Complete Care FIT Outreach Program Centrally Coordinated Outreach Effort:
Supports physician efforts to engage members in actions that improve health outcomes
Targets members aged 50-75 who do not come in for regular visits and/or who have not had a CRC screening test
– No FIT Results in the last 9 months – No Sigmoidoscopy in the last 5 years – No Colonoscopy in the last 10 years
Program Components: Automated phone calls generated to inform members about mailing of FIT Kit FIT Kit mailed to member’s home with instructions on how to complete
the test and mail it back to KPSC Regional Laboratory “Exclusion form” attached to top of outreach letter so members can report
if they have been screened, had a total colectomy or have other reason preventing them from completing the FIT
16
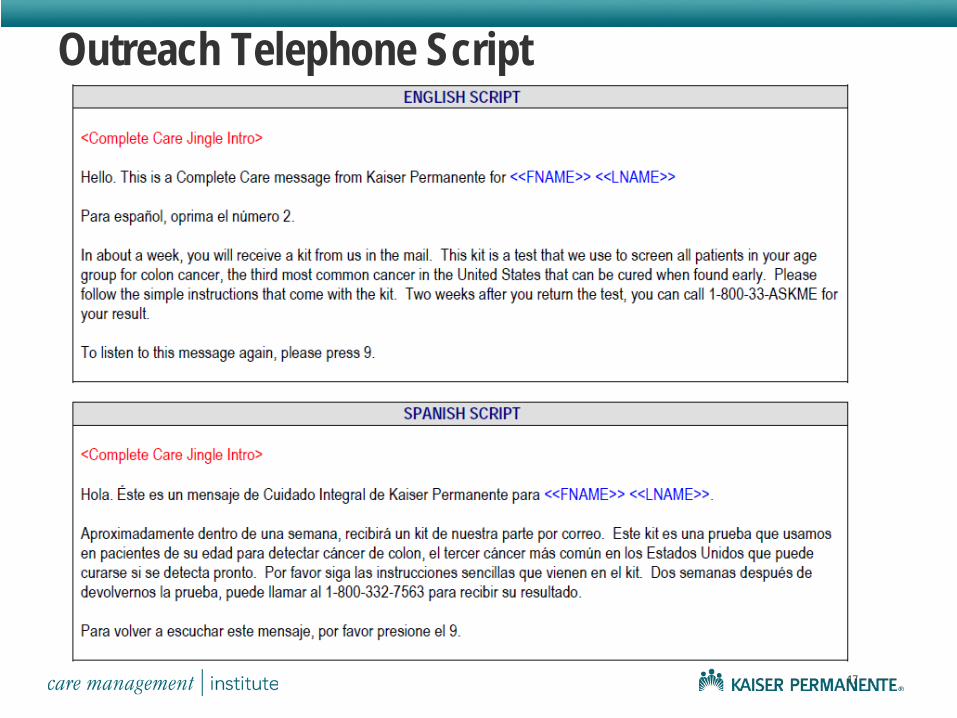
Outreach Telephone Script
17
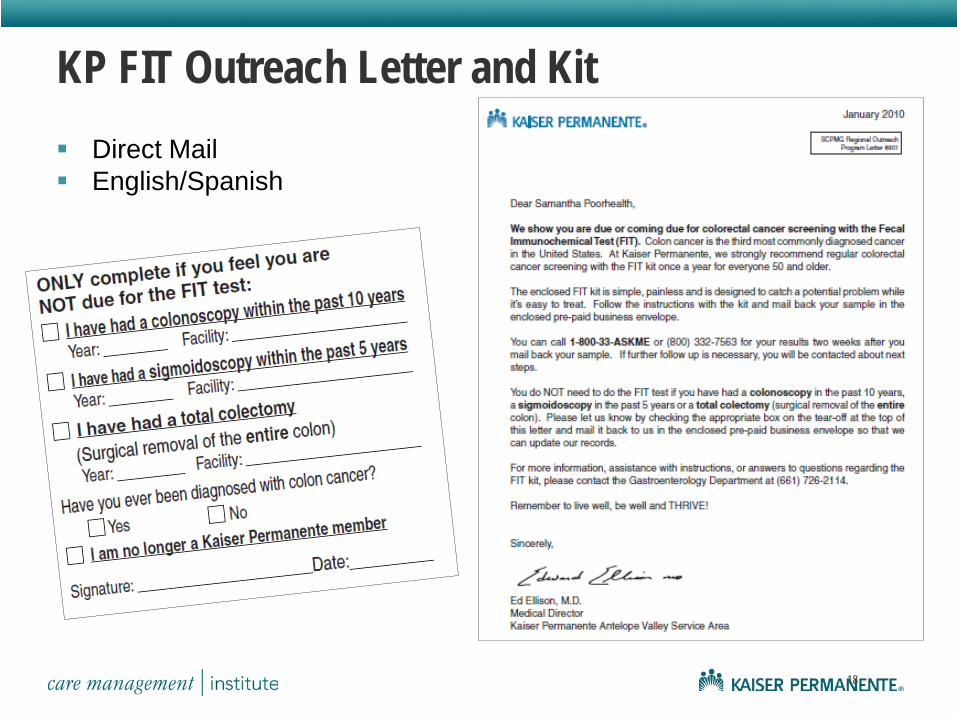
KP FIT Outreach Letter and Kit
18
Direct Mail English/Spanish
19
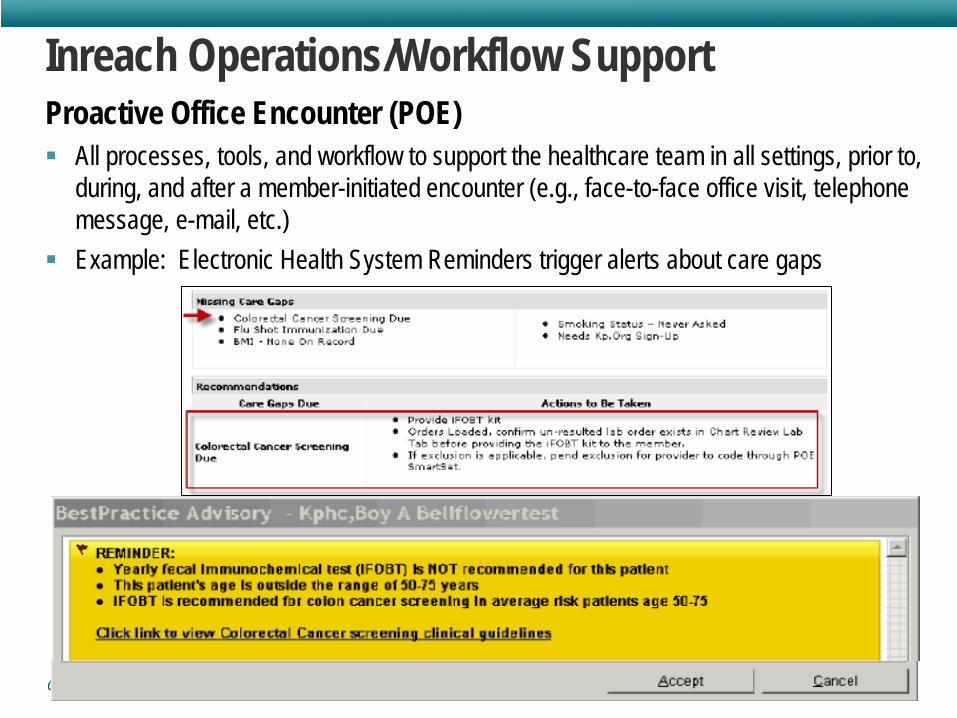
Inreach Operations/Workflow Support Proactive Office Encounter (POE) All processes, tools, and workflow to support the healthcare team in all settings, prior to,
during, and after a member-initiated encounter (e.g., face-to-face office visit, telephone message, e-mail, etc.)
Example: Electronic Health System Reminders trigger alerts about care gaps
Diagnosis Detection and Follow Up: Positive FOBT Safety Net
Delays in cancer diagnosis Potential Litigation
Unknown number falling through the cracks No known fix
Risk Management Problem
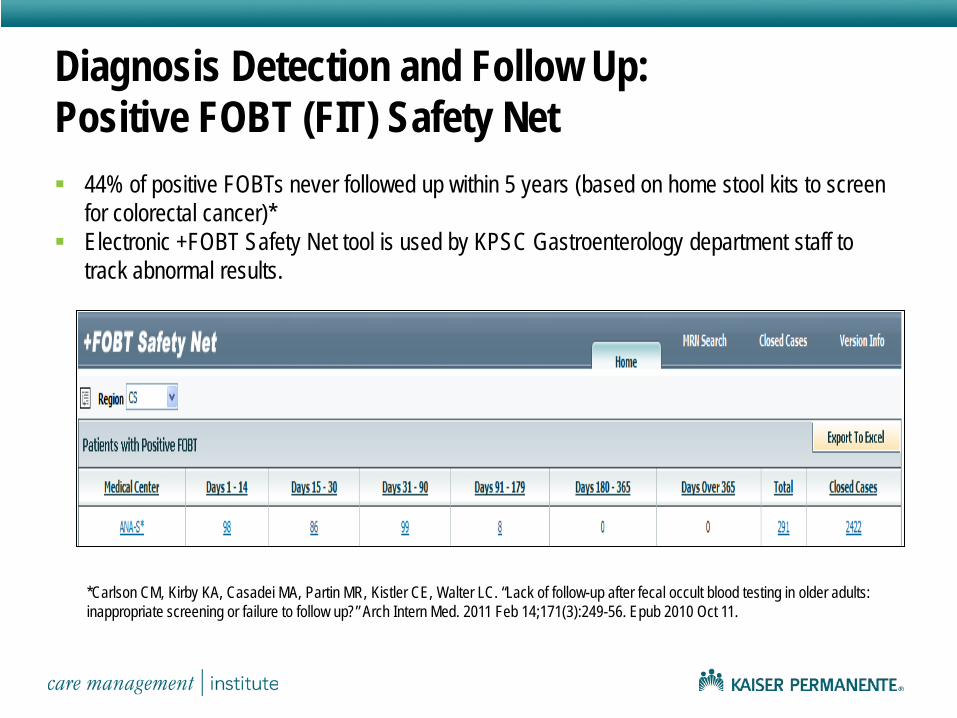
Diagnosis Detection and Follow Up: Positive FOBT (FIT) Safety Net
*Carlson CM, Kirby KA, Casadei MA, Partin MR, Kistler CE, Walter LC. “Lack of follow-up after fecal occult blood testing in older adults: inappropriate screening or failure to follow up?” Arch Intern Med. 2011 Feb 14;171(3):249-56. Epub 2010 Oct 11.
44% of positive FOBTs never followed up within 5 years (based on home stool kits to screen for colorectal cancer)*
Electronic +FOBT Safety Net tool is used by KPSC Gastroenterology department staff to track abnormal results.
22
Performance Measurement Strategies
Bimonthy Clinical Strategic Goals reports
Overall screening rates, by medical center and region Provider-specific screening rates report – shared unblinded
Access for procedures and appointments Colonoscopy throughput
Successful “capture” rates, rates by medical center (on a "report card")
23
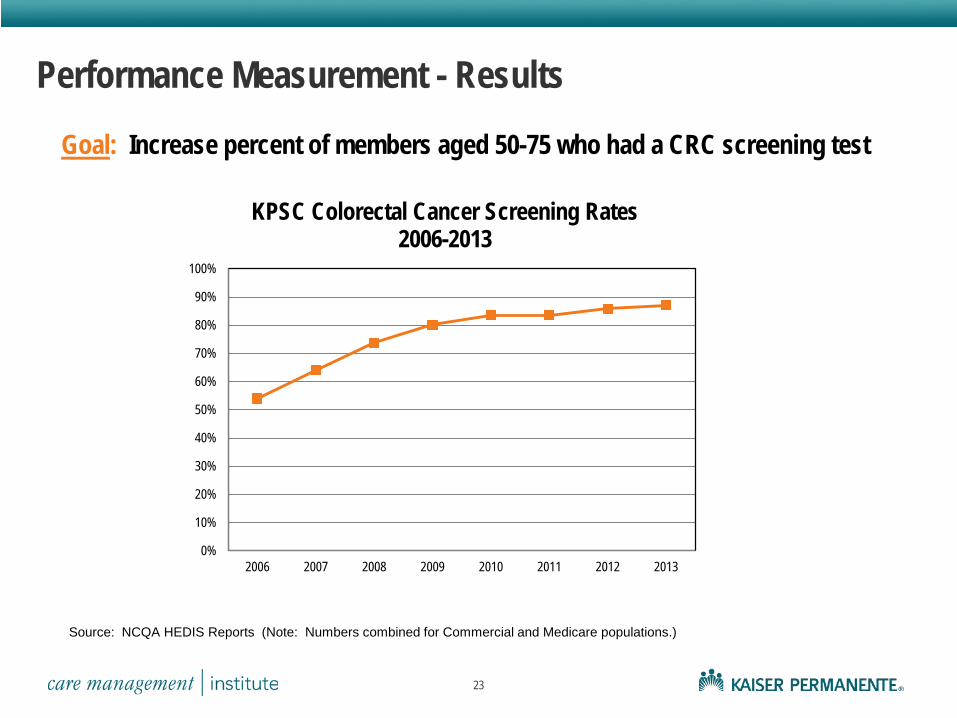
Performance Measurement - Results
Goal: Increase percent of members aged 50-75 who had a CRC screening test
Source: NCQA HEDIS Reports (Note: Numbers combined for Commercial and Medicare populations.)
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
2006 2007 2008 2009 2010 2011 2012 2013
KPSC Colorectal Cancer Screening Rates 2006-2013
24
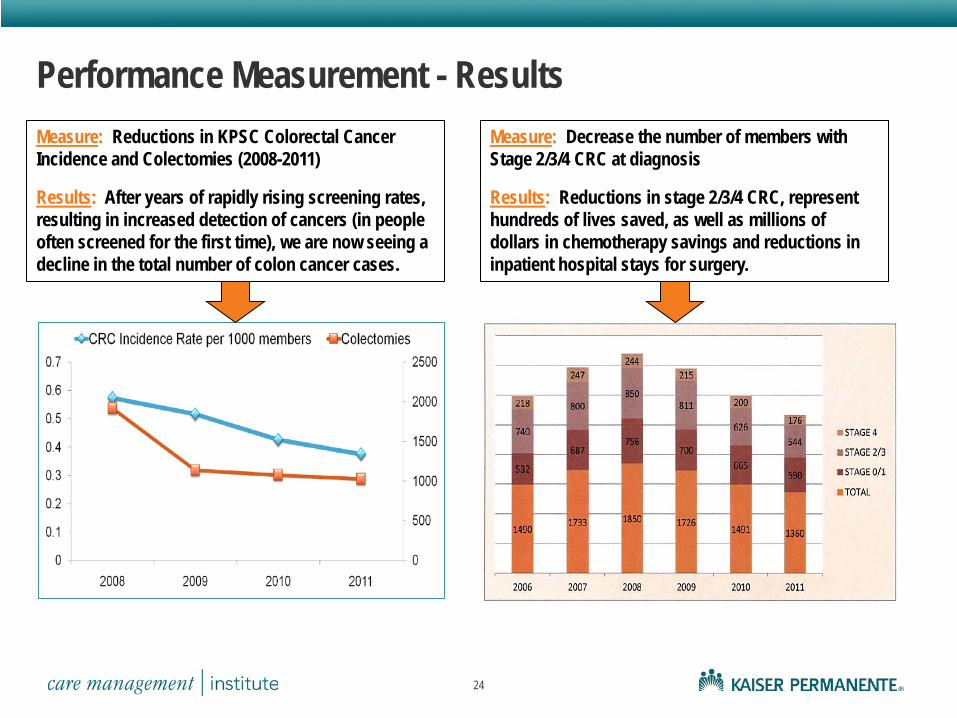
Measure: Reductions in KPSC Colorectal Cancer Incidence and Colectomies (2008-2011) Results: After years of rapidly rising screening rates, resulting in increased detection of cancers (in people often screened for the first time), we are now seeing a decline in the total number of colon cancer cases.
Performance Measurement - Results Measure: Decrease the number of members with Stage 2/3/4 CRC at diagnosis Results: Reductions in stage 2/3/4 CRC, represent hundreds of lives saved, as well as millions of dollars in chemotherapy savings and reductions in inpatient hospital stays for surgery.
Conclusions
25
Centralized guideline development, coupled with coordinated implementation efforts and performance monitoring, can substantially increase screening rates, decrease the incidence of colorectal cancer and improve survival.
After years of rapidly rising screening rates, resulting in increased detection of cancers (in people often screened for the first time), we are now seeing a decline in the total number of colon cancer cases.
The decline in CRC (lower than the U.S. average) makes a powerful case for continuing colorectal cancer guideline and implementation efforts.
The declines in CRC cases from 2008 peak to 2012 levels, particularly reductions in stage 2/3/4 CRC, represent hundreds of lives saved, as well as millions of dollars in chemotherapy savings and reductions in inpatient hospital stays for surgery.