Embed Size (px)
Citation preview

International Journal of Cardiology 224 (2016) 50–56
Contents lists available at ScienceDirect
International Journal of Cardiology
j ourna l homepage: www.e lsev ie r .com/ locate / i j ca rd
Comparison of various scores for predicting success of chronic totalocclusion percutaneous coronary intervention
Aris Karatasakis a,1, Barbara A. Danek a,1, Dimitri Karmpaliotis b,1, Khaldoon Alaswad c,1, Farouc A. Jaffer d,1,Robert W. Yeh e,1, Mitul Patel f,1, John N. Bahadorani f,1, William L. Lombardi g,1, R. Michael Wyman h,1,J. Aaron Grantham i,1, David E. Kandzari j,1, Nicholas J. Lembo j,1, Anthony H. Doing k,1, Catalin Toma l,1,JeffreyW. Moses b,1, Ajay J. Kirtane b,1, Manish A. Parikh b,1, Ziad A. Ali b,1, Santiago Garcia m,1, Pratik Kalsaria a,1,Judit Karacsonyi a,1, Aya J. Alame a,1, Craig A. Thompson n,1, Subhash Banerjee a,1, Emmanouil S. Brilakis a,⁎,1a VA North Texas Health Care System and University of Texas Southwestern Medical Center, Dallas, TX, United Statesb Columbia University, New York, NY, United Statesc Henry Ford Hospital, Detroit, MI, United Statesd Massachusetts General Hospital and Harvard Medical School, Boston, MA, United Statese Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, MA, United Statesf VA San Diego Healthcare System and University of California San Diego, La Jolla, CA, United Statesg University of Washington, Seattle, WA, United Statesh Torrance Memorial Medical Center, Torrance, CA, United Statesi St. Luke's Mid America Heart Institute, Kansas City, MO, United Statesj Piedmont Heart Institute, Atlanta, GA, United Statesk Medical Center of the Rockies, Loveland, CO, United Statesl University of Pittsburgh Medical Center, Pittsburgh, PA, United Statesm Minneapolis VA Health Care System and University of Minnesota, Minneapolis, MN, United Statesn Boston Scientific, Natick, MA, United States
⁎ Corresponding author at: Dallas VA Medical CenterRoad, Dallas, TX 75216, United States.
E-mail address: [email protected] (E.S. Brilakis).1 This author takes responsibility for all aspects of the r
of the data presented and their discussed interpretation.
http://dx.doi.org/10.1016/j.ijcard.2016.08.3170167-5273/Published by Elsevier Ireland Ltd.
a b s t r a c t
a r t i c l e i n f oArticle history:Received 8 June 2016Received in revised form 18 August 2016Accepted 19 August 2016Available online 23 August 2016
Background: Various scoring systems have been developed to predict the technical outcome and proceduralefficiency of chronic total occlusion (CTO) percutaneous coronary intervention (PCI).Methods:We examined the predictive capacity of 3 CTO PCI scores (Clinical and Lesion-related [CL], Multi-center CTO registry in Japan [J-CTO] and Prospective Global Registry for the Study of Chronic Total OcclusionIntervention [PROGRESS CTO] scores) in 664 CTO PCIs performed between 2012 and 2016 at 13 US centers.Results: Technical success was 88% and the retrograde approach was utilized in 41%. Mean CL, J-CTO andPROGRESS CTO scores were 3.9 ± 1.9, 2.6 ± 1.2 and 1.4 ± 1.0, respectively. All scores were inversely asso-ciated with technical success (p b 0.001 for all) and had moderate discriminatory capacity (area under thecurve 0.691 for the CL score, 0.682 for the J-CTO score and 0.647 for the PROGRESS CTO score [p = non-significant for pairwise comparisons]). The difference in technical success between the minimum and max-imum CL score strata was the highest (32%, vs. 15% for J-CTO and 18% for PROGRESS CTO scores). All scorestended to perform better in antegrade-only procedures and correlated significantly with procedure timeand fluoroscopy dose; the CL score also correlated significantly with contrast utilization.Conclusions: CL, J-CTO and PROGRESS CTO scores perform moderately in predicting technical outcome ofCTO PCI, with better performance for antegrade-only procedures. All scores correlate with proceduretime and fluoroscopy dose, and the CL score also correlates with contrast utilization.
Published by Elsevier Ireland Ltd.
Keywords:Chronic total occlusionPercutaneous coronary interventionProcedural successComplicationsTechniquesOutcomes
(111A), 4500 South Lancaster
eliability and freedom from bias
1. Introduction
Successful chronic total occlusion (CTO) percutaneous coronaryintervention (PCI) has been associated with significant clinical benefit[1–3]. However, success of CTO interventions varies widely, dependingon lesion complexity [4–8], patient characteristics [9] and operator

51A. Karatasakis et al. / International Journal of Cardiology 224 (2016) 50–56
experience [4,10]. Accurate pre-procedural assessment of howchallenging a lesion is could help in procedural planning, to estimatethe duration of the procedure and/or the need to refer the patient toanother center with expertise in CTO PCI (for centers early in theirCTO PCI learning curve), as well as in more accurate risk–benefit ratioassessment. Several scores have been developed to predict CTO PCIprocedural success and efficiency, but no comparative analyses havebeen performed to date. We used a contemporary multicenter CTO PCIregistry to perform a comparative analysis of three currently availableCTO PCI scores: Clinical and Lesion-related (CL) score [7], MulticenterCTO Registry in Japan (J-CTO) score [5] and Prospective Global Registryfor the Study of Chronic Total Occlusion Intervention (PROGRESS CTO)score [6].
2. Methods
We examined the clinical and angiographic records of patients who underwentCTO PCI between May 2012 and February 2016 by experienced, high volumeoperators at 13 CTO PCI centers in the United States (Supplement). Data collectionwas performed prospectively and retrospectively and recorded in a CTO database(PROGRESS CTO, Clinicaltrials.gov Identifier: NCT02061436) [6,9,11–18]. Somecenters only enrolled patients during part of the study period due to participationin other studies. The study was approved by the institutional review board of eachsite.
Table 1Clinical and angiographic characteristics of the study patients and lesions.
Clinical characteristics (N = 658)
Age (years)a 66 ± 10Male (%) 85Hypertension (%) 89Hyperlipidemia (%) 95Current smoking (%) 18Diabetes mellitus (%) 47History of myocardial infarction (%) 47Prior PCI (%) 61Prior failed CTO PCI (%) 19Prior coronary artery bypass grafting (%) 36History of stroke (%) 13Peripheral arterial disease (%) 17Heart failure (%) 27Ejection fraction (%)a 51 ± 14Clinical presentation
Stable angina (%) 59Acute coronary syndrome (%) 32Asymptomatic (%) 9
Angiographic characteristics (N = 664)
Target vessel
2.1. Definitions
Coronary CTOs were defined as coronary lesions with thrombolysis in myocardialinfarction (TIMI) grade 0 flow of at least 3 months' duration. Estimation of the occlu-sion duration was based on first onset of anginal symptoms, prior history of myocar-dial infarction in the target vessel territory, or comparison with a prior angiogram.Calcification was assessed by angiography as mild (spots), moderate (involving≤50% of the reference lesion diameter) and severe (involving N50% of the referencelesion diameter). Moderate proximal vessel tortuosity was defined as the presenceof at least 2 bends N 70° or 1 bend N 90° and severe tortuosity as 2 bends N 90° or 1bend N 120° in the CTO vessel. Interventional collaterals were defined as collateralsdeemed amenable to crossing by a guidewire and a microcatheter by the operator.A procedure was defined as “retrograde” if an attempt was made to cross the lesionthrough a collateral vessel supplying the target vessel distal to the lesion; if not, theprocedure was classified as “antegrade-only”. Antegrade-only cases utilizedantegrade wire escalation (AWE), or antegrade dissection re-entry (ADR), or bothapproaches. Technical success of CTO PCI was defined as successful CTO revasculari-zation with achievement of b30% residual diameter stenosis within the treatedsegment and restoration of TIMI grade 3 antegrade flow. Procedural success wasdefined as achievement of technical success with no in-hospital major adverse cardi-ac events (MACE). In-hospital MACE included any of the following adverse eventsprior to hospital discharge: death, myocardial infarction (MI), recurrent symptomsrequiring urgent repeat target vessel revascularization with PCI or coronary arterybypass graft surgery (CABG), tamponade requiring either pericardiocentesis orsurgery, and stroke. Peri-procedural and late in-hospital MI were defined accordingto the Third Universal Definition of Myocardial Infarction [19]. Procedure time wascalculated from administration of local anesthetic for vascular access to removal oflast catheter. The CL-score was calculated as described by Alessandrino et al. [7],the J-CTO score was calculated as described by Morino et al. [5] and the PROGRESSCTO score as described by Christopoulos et al. [6] Procedures used for the derivationof the PROGRESS CTO score (n = 521) in the original study were excluded from thepresent analysis.
Right coronary artery (%) 54Left anterior descending artery (%) 25Circumflex artery (%) 21
Estimated CTO length (mm)a 34 ± 26Proximal cap ambiguity (%) 33Blunt stump morphology (%) 53Moderate/severe calcification (%) 53Moderate/severe tortuosity (%) 37Poor distal vessel (%) 36Distal cap at bifurcation (%) 32Lack of interventional collaterals (%) 46In-stent restenosis (%) 13Prediction scores
CL scorea 3.9 ± 1.9J-CTO scorea 2.6 ± 1.2PROGRESS CTO scorea 1.4 ± 1.0
CTO, chronic total occlusion; PCI, percutaneous coronary intervention.a Values are mean ± standard deviation.
2.2. Statistical analysis
Categorical variables were expressed as percentages and compared using theCochran–Armitage test for trendor Pearson's χ2 test. Continuous variableswerepresentedas mean ± standard deviation (normally distributed data) or median (interquartilerange) (non-normally distributed data), and were compared using the Jonckheere–Terpstra test for trend. The effect of prediction scores on efficiency measures was testedusing univariate linear regression; the unstandardized regression coefficient (B) was re-ported. The association between prediction scores and technical outcome was testedusing univariate logistic regression; receiver operating characteristic (ROC) curve andarea under the curve (AUC) were used to assess discriminatory capacity, and theHosmer–Lemeshow (HL) test was used to assess calibration [20]. Differences in AUC be-tween curves were tested as described by Hanley & McNeil [21]. Statistical analysis wasperformed with JMP 12.0 (SAS Institute, Cary, NC), MedCalc 16.4 (Ostend, Belgium) andSPSS 22.0 (IBM Corporation, Armonk, NY). A p value of b0.05 was considered statisticallysignificant.
3. Results
From 1185 CTO PCIs that were enrolled between 2012 and 2016in the PROGRESS CTO registry and had data for calculation of theCL, J-CTO and PROGRESS CTO score, 521 (44%) procedures thatwere used for derivation of the PROGRESS CTO score were excluded.The remaining 664 interventions were performed on 658 patientsand were included in the present analysis. Table 1 shows the clinicaland angiographic characteristics of the study patients and lesions;there was a high prevalence of diabetes mellitus (47%) and priorCABG (36%). The majority of the patients (59%) presented with sta-ble angina. The most common target vessel was the right coronaryartery (RCA, 54%). Mean CTO length was 34 ± 26 mm, and angio-graphic complexity was high (blunt stump: 53%, moderate/severecalcification 53%). Mean J-CTO score was 2.6 ± 1.2, mean CL scorewas 3.9 ± 1.9 and mean PROGRESS CTO score was 1.4 ± 1.0.
Overall technical success rate was 88%, and was most frequentlyachieved with antegrade wire escalation (48%, Table 2). A retrogradeapproach was used in 41% of procedures, and was the initial strategyselected in 19%. A major in-hospital adverse event occurred in 24patients (3.6%).
All three scores exhibited good calibration in our sample: CL scoreHosmer–Lemeshow (HL) χ2 = 4.124, p = 0.846; J-CTO score HL χ2 =5.888, p = 0.117 and PROGRESS CTO score HL χ2 = 5.403, p = 0.067.Technical success was significantly lower for increasing strata of allthree scoring systems (p for trend b 0.001 for all, Fig. 1). However, thedifference in technical success between the smallest and highest strataof CL score (0–8) was the highest (Δ = −32%), followed by the

52 A. Karatasakis et al. / International Journal of Cardiology 224 (2016) 50–56
PROGRESS CTO score (0–4, Δ = −18%) and J-CTO score (0–5,Δ = −15%).
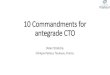
The discriminatory performance of the scoring systems in predictingtechnical outcome was assessed using ROC curves in both antegrade-only and all procedures (Fig. 2). All scores showedmoderate predictivecapacity, as follows: AUC: 0.691, 95%CI 0.633–0.749, p b 0.001 for the CLscore, AUC: 0.682, 95%CI 0.625–0.738, p b 0.001 for the J-CTO score andAUC: 0.647, 95%CI 0.588–0.706, p b 0.001 for the PROGRESS CTO score.All three scores performed numerically better in predicting theoutcome of exclusively antegrade procedures: CL score (AUC: 0.746,95% CI 0.663–0.829, p b 0.001), J-CTO score (AUC: 0.735, 95% CI0.650–0.821, p b 0.001) and PROGRESS CTO score (AUC: 0.692, 95% CI0.610–0.774, p b 0.001). The final successful crossing strategy was lesslikely to be antegrade wire escalation and more likely to be retrogradeor antegrade dissection/re-entry for increasing strata of the CL andJ-CTO scores (Fig. 3).
Procedure time and air kerma fluoroscopy dose were increasedamong higher strata of all three scores (Fig. 4), but only the CL scoreshowed significant association with contrast volume utilization. Usinglinear regression, a 1-point increase in CL score was associated with17.9 additional minutes of procedure time (95% CI 14.7–21.0,p b 0.001), 7.8 ml of contrast (95% CI 2.9–12.8, p = 0.002) and 0.5Gray of radiation (95% CI 0.3–0.6, p b 0.001). A 1-point increase inJ-CTO score was associated with 20.0 additional minutes of proce-dure time (95% CI 14.9–25.2, p b 0.001) and 0.6 Gray of radiation(95% CI 0.4–0.8, p b 0.001), but did not have significant associationwith contrast utilization (p = 0.169). A 1-point increase inPROGRESS CTO score was associated with 7.5 additional minutes ofprocedure time (95% CI 1.1–14.0, p = 0.022) and 0.3 Gray of radiation(95% CI 0.1–0.6, p = 0.001), but did not have significant associationwith contrast utilization (p = 0.389).
4. Discussion
The main findings of our study are that: (i) the CL, J-CTO andPROGRESS CTO scores are all significantly and inversely associatedwith technical success rate and procedural efficiency of CTO PCI; (ii)their performance in predicting technical outcome appears moderatefor procedures performed using the hybrid approach for CTO PCI, and
Table 2Procedural characteristics and in-hospital outcomes of the study patients and procedures.
Procedure time (min)a 143 (95–208)Contrast volume (ml)a 270 (200–357)Air kerma fluoroscopy dose (Gy)a 3.3 (2.1–4.9)Fluoroscopy time (min)a 47 (28–78)Crossing strategies used
Antegrade wire escalation (%) 78Antegrade dissection/re-entry (%) 36Retrograde (%) 41
First crossing strategyAntegrade wire escalation (%) 72Antegrade dissection/re-entry (%) 9Retrograde (%) 19
Technical success (%) 88Antegrade wire escalation (%) 48Antegrade dissection/re-entry (%) 24Retrograde (%) 28
MACE (%) 3.6Death (%) 0.8Myocardial infarction (%) 1.2Stroke (%) 0.5Emergency re-PCI (%) 0.5Emergency coronary artery bypass grafting (%) 0.0Emergency pericardiocentesis (%) 1.4Procedural success (%) 87
MACE, major adverse cardiovascular event; PCI, percutaneous coronary intervention.a Value are median (interquartile range).
(iii) all three scores perform better in predicting the outcome ofantegrade-only (AWE or ADR) procedures, as opposed to proceduresutilizing the retrograde approach.
CTO PCI success rates are lower than those of non-CTO lesions andhave been highly variable, from a US average of approximately 60%, to90% in experienced, high volume centers [1,4,11,22]. This variabilitycan be attributed to differences in operator experience and commit-ment, setting (e.g. equipment availability, staff training), patient clinicalcharacteristics, and lesion characteristics [4,23–25]. These factors alsodirectly affect efficiency measures, including time, contrast, radiationand equipment required to carry out the procedure, — all of whichmay translate into increased cost. The ability to reliably predict theprobability of success and efficiency of a procedure is an attractive con-cept: (i) first and foremost, it allows for an objective consideration— by
Fig. 1. Technical success rates for different strata of prediction rules. P values for trend.

Fig. 2. Receiver operating characteristic (ROC) curve for predicting technical outcomewitheach prediction rule, for all procedures and for procedures performed without use of aretrograde approach (antegrade-only).
Fig. 3. Final successful crossing strategy (successful procedures only) according todifferent strata of the CL score (panel A), J-CTO score (panel B) and PROGRESS CTO score(panel C).
53A. Karatasakis et al. / International Journal of Cardiology 224 (2016) 50–56
both patient and operator of the risk–benefit ratio of an attempt for per-cutaneous CTO revascularization. This is of particular importance in CTOintervention, due to the inherently higher procedural and in-hospitalcomplication rate, as compared with non-CTO intervention; [8,26] (ii)approximating efficiency measures can be of benefit in multiple ways:estimating time of the procedure can assist with catheterization labora-tory scheduling; predicting dye utilization and combining this informa-tion with established scores [27] can help prevent contrast inducednephropathy; and predicting large (or cumulatively large, in case of re-peat procedures) exposure to radiation can prevent radiation injury;(iii) accurate estimation of PCI difficulty allows operator to select proce-dures appropriate for their skill level in CTOPCI: for example early in thelearning curve easier cases are attempted, with more difficult casesbeing referred to more experienced centers, performed with the assis-tance of a proctor or deferred until later; and (iv) standardization of dif-ficulty level of CTO PCI can help interpret CTO PCI outcomes acrossvarious clinical settings.
The J-CTO score, created by Morino et al. using data from 494 PCIsentered in the J-CTO registry, is the first and most widely used CTOprediction rule (Table 3). The primary endpoint (successful guidewirecrossing within 30 min of entering the coronary circulation) was
selected to eliminate operator bias e.g. from different operator persis-tence. However, while the J-CTO score was validated for prediction oftechnical success in a previous PROGRESS CTO cohort (AUC: 0.705)[12], a study by Nombela-Franco et al. did not replicate this finding(AUC: 0.399) despite further validating this score's merit as a tool topredict quick guidewire crossing (AUC: 0.770) [28]. In the presentstudy, the J-CTO score showed moderate (AUC: 0.682) ability to predicttechnical failure for hybrid CTO PCI. Procedure time remained stronglycorrelated with J-CTO score in our study (20 additional minutes perpoint increase) as did radiation dose (0.6Gray per point), further addingto the evidence that the J-CTO score is a solid predictor of proceduralefficiency. Recently, Tanaka et al. expanded the utility of this score bydemonstrating that J-CTO score correlates strongly with mid-termsuccess rates — a composite of immediate technical success andfreedom from target lesion revascularization at 1-year [29].
The PROGRESS CTO score was derived by Christopoulos et al. usingdata from the PROGRESS CTO registry (this data was not included in

Fig. 4. Relationship between strata of CL, J-CTO and PROGRESS CTO scores and measures of procedural efficiency (procedure time, contrast volume and air kerma fluoroscopy dose). Pvalues for trend.
Table 3Score components and allocated points for the CL, J-CTO and PROGRESS CTOscores.
Score components Points
CL scoreSevere lesion calcification +2Previous CABG +1.5Lesion length ≥ 20 mm +1.5Previous MI +1Blunt stump +1Non-LAD CTO +1
J-CTO scoreBlunt stump +1Lesion calcification (any degree) +1Bending N 45° +1Lesion length ≥ 20 mm +1Previously failed lesion +1
PROGRESS CTO scoreModerate/severe tortuositya +1Circumflex CTO +1Proximal cap ambiguityb +1Absence of interventional collateralsc +1
CABG, coronary artery bypass graft; CTO, chronic total occlusion; LAD, left anteriordescending artery.
a Defined as 2 bends N 70° or 1 bend N 90°.b Defined as inability to unequivocally determine the proximal entry point into
the CTO.c Defined as collaterals deemed amenable to crossing by a wire and a micro-
catheter by the operator.
54 A. Karatasakis et al. / International Journal of Cardiology 224 (2016) 50–56
the present analysis), to predict technical success [6]. The PROGRESSCTO score showed good performance in the validation subset of theindex study (AUC for PROGRESS CTO score: 0.720, vs. 0.746 for theJ-CTO score), is simple (includes 4 angiographic parameters), and isconsistent with the hybrid algorithm for CTO PCI crossing. However,similar to the J-CTO score, in the present study the PROGRESS CTO scorehad moderate predictive capacity for technical success (AUC: 0.647) andprocedure time (7.5 min for each additional point).
Most recently, Alessandrino et al. were the first to include clinicalcharacteristics in a prediction model for CTO PCI, based on observationsindicating that clinical factors can influence the technical outcome ofCTO PCI [7,24,25]. The CL score was derived from a cohort of 1657 pro-cedures (derivation: 1143 and validation: 514), and showed moderatediscriminatory capacity for technical success (AUC: 0.68 for CL scorevs. 0.60 for J-CTO score), similar to our study (AUC: 0.691). The CLscore had the largest difference in technical success between the mini-mum (0) and maximum (8) points on the CL score scale (32%) andwas the only score showing significant correlation with all three mea-sures of procedural efficiency (i.e. including contrast utilization) in ourstudy. The marginally better performance of the CL score as comparedwith the J-CTO and PROGRESS CTO scores may be partly explained bythe higher number of variables examined in the former. As a disadvan-tage, inclusion of more variables with differential weighing may makethe score more difficult to calculate.

2 Paul A. Harris, Robert Taylor, Robert Thielke, Jonathon Payne, Nathaniel Gonzalez, JoseG. Conde, Research electronic data capture (REDCap) — a metadata-driven methodologyand workflow process for providing translational research informatics support, J BiomedInform. 2009 Apr.;42(2):377–81.
55A. Karatasakis et al. / International Journal of Cardiology 224 (2016) 50–56
Tougher lesions (higher CL and J-CTO score) were more likely torequire a retrograde approach in our study, a finding consistentwith previous reports [11]. The association between PROGRESS CTOscore and final successful strategy was blunted, likely becausepresence of interventional collaterals (that play a major role in thesuccess of the retrograde approach) is part of the PROGRESS CTOscoring scheme. All three scores performed better in predicting theoutcome of antegrade-only procedures, a finding which may beattributable to the lack of retrograde-specific parameters in thescore calculation (with the exception of “lack of interventionalcollaterals” — in the PROGRESS CTO score), and the fact that mostretrograde procedures were performed after antegrade crossinghad already failed. Hence, all 3 scores may be of even greater valuefor antegrade-only CTO PCI operators, and new parameters may benecessary to predict the success rates of retrograde CTO PCI. It isimportant to note that none of the 3 scores showed “good”discriminatory capacity (AUC of ≥0.8) in our study. This impliesthat while scores can be helpful by assisting angiographic review ofthe lesion and providing an estimate of lesion complexity, they canonly be useful as part of a holistic approach to clinical decision-making. Given the higher potential for complications, the decisionto proceed with CTO revascularization and the most appropriatemodality must be based on thorough risk-benefit evaluation and anopen discussion with both the patient and the heart team.
Our study is limited by the observational design, as it is based onregistry data and is subject to selection bias. Angiographicparameters were assessed by the operator without core laboratoryadjudication; there was no clinical event committee adjudication.Some centers contributed data only for parts of the study period.Participating centers had significant expertise in CTO PCI, thus ourfindings might be less applicable to centers with lower volume orantegrade-only operators.
In conclusion, the CL, J-CTO and PROGRESS CTO scores performedmoderately well in predicting technical outcome of CTO PCI in ourcohort. All three scores performed better for procedures in which aretrograde approach was not utilized, and showed significantcorrelation with procedure time and fluoroscopy dose, while the CLscore also correlated with contrast utilization.
Conflict of interest
Dr. Karmpaliotis: speakers’ bureau, Abbott Vascular, Medtronic, andBoston Scientific. Consultant to Bridgepoint Medical. Dr. Alaswad:consulting fees from Terumo, Asahi Intecc and Boston Scientific;consultant, no financial support, Abbott Laboratories. Dr. Jaffer:consultant to Boston Scientific, Siemens, and Merck, nonfinancialresearch support from Abbott Vascular, research grant from NationalInstitutes of Health (HL-R01-108229), Siemens and Kowa. Dr. Yeh:Career Development Award (1K23HL118138) from the National Heart,Lung, and Blood Institute. Consultant for Abbott Vascular, GileadSciences and Boston Scientific. Advisory board of Abbott Vascular. Salarysupport from Harvard Clinical Research Institute. Dr. Patel: speakers’ bu-reau for Astra Zeneca. Dr. Wyman: Honoraria/consulting/speaking feesfrom Boston Scientific, Abbott Vascular, and Asahi. Dr. Lombardi: equitywith Bridgepoint Medical. Consultant to Boston Scientific, Abiomed andAbbott Vascular. Dr. Grantham: Speaking fees, consulting, and honorariafrom Abbott Vascular, Boston Scientific, Asahi Intecc. Research grantsfrom Boston Scientific, Asahi Intecc, Abbott Vascular, Medtronic. Memberof Boston Scientific Executive Physician Leadership Committee. Advisoryboard for BSCI. CTO advisory board for Abbott Vascular. Dr. Kandzari:research/grant support and consulting honoraria from Boston Scientificand Medtronic Cardiovascular, and research/grant support from Abbott.Dr. Lembo: speakers’ bureau: Medtronic; advisory board Abbott Vascularand Medtronic. Dr. Moses: consultant to Boston Scientific and Abiomed.Dr. Kirtane: Institutional research grants to Columbia University fromBoston Scientific, Medtronic, Abbott Vascular, Abiomed, St. Jude Medical,
Vascular Dynamics, GlaxoSmithKline, and Eli Lilly. Dr. Garcia: consultingfees fromMedtronic and Surmodics. Dr. Thompson: employee of BostonScientific. Dr. Banerjee: research grants from Gilead and the MedicinesCompany; consultant/speaker honoraria from Covidien, Merck andMedtronic; ownership in MDCARE Global (spouse); intellectual propertyin HygeiaTel. Educational grant from Boston Scientific (spouse). Dr.Brilakis: consulting/speaker honoraria from Abbott Vascular, Asahi,Elsevier, GE Healthcare, and St Jude Medical; research support fromInfraRedx and Boston Scientific; spouse is employee of Medtronic.Remaining authors: none
Sources of funding
Research reported in this publication was supported by the Clinicaland Translational Science Awards Program of the National Institutes ofHealth (NIH, Bethesda, MD) under grant number UL1-RR024982. Thecontent is solely the responsibility of the authors and does notnecessarily represent the official views of the NIH.
Acknowledgement
We would like to thank Jose R. Martinez-Parachini, MD, EricaResendes, MS, Bavana V. Rangan, BDS, MPH and Michele Roesle, RNfor their assistance with the present study.
Study data were collected and managed using REDCap electronicdata capture tools hosted at University of Texas SouthwesternMedical Center.2 REDCap (Research Electronic Data Capture) is asecure, web-based application designed to support data capture forresearch studies, providing 1) an intuitive interface for validateddata entry; 2) audit trails for tracking data manipulation and exportprocedures; 3) automated export procedures for seamless datadownloads to common statistical packages; and 4) procedures forimporting data from external sources.
Appendix A. Supplementary data
Supplementary data to this article can be found online at http://dx.doi.org/10.1016/j.ijcard.2016.08.317.
References
[1] G.E. Christakopoulos, G. Christopoulos, M. Carlino, O.M. Jeroudi, M. Roesle, B.V.Rangan, S. Abdullah, J. Grodin, D.J. Kumbhani, M. Vo, M. Luna, K. Alaswad, D.Karmpaliotis, S. Rinfret, S. Garcia, S. Banerjee, E.S. Brilakis, Meta-analysis of clinicaloutcomes of patients who underwent percutaneous coronary interventions forchronic total occlusions, Am. J. Cardiol. 115 (2015) 1367–1375.
[2] R. Mehran, B.E. Claessen, C. Godino, G.D. Dangas, K. Obunai, S. Kanwal, M. Carlino, J.P.Henriques, C. Di Mario, Y.H. Kim, S.J. Park, G.W. Stone, M.B. Leon, J.W. Moses, A.Colombo, Multinational chronic total occlusion R. Long-term outcome of percutane-ous coronary intervention for chronic total occlusions, JACC Cardiovasc. Interv. 4(2011) 952–961.
[3] L.P. Hoebers, B.E. Claessen, J. Elias, G.D. Dangas, R. Mehran, J.P. Henriques, Meta-analysis on the impact of percutaneous coronary intervention of chronic totalocclusions on left ventricular function and clinical outcome, Int. J. Cardiol. 187(2015) 90–96.
[4] E.S. Brilakis, S. Banerjee, D. Karmpaliotis, W.L. Lombardi, T.T. Tsai, K.A. Shunk, K.F.Kennedy, J.A. Spertus, D.R. Holmes Jr., J.A. Grantham, Procedural outcomes ofchronic total occlusion percutaneous coronary intervention: a report from thencdr (national cardiovascular data registry), JACC Cardiovasc. Interv. 8 (2015)245–253.
[5] Y. Morino, M. Abe, T. Morimoto, T. Kimura, Y. Hayashi, T. Muramatsu, M. Ochiai, Y.Noguchi, K. Kato, Y. Shibata, Y. Hiasa, O. Doi, T. Yamashita, T. Hinohara, H. Tanaka,K. Mitsudo, J.C.R. Investigators, Predicting successful guidewire crossing throughchronic total occlusion of native coronary lesions within 30 minutes: the J-CTO(multicenter CTO registry in Japan) score as a difficulty grading and time assess-ment tool, JACC Cardiovasc. Interv. 4 (2011) 213–221.
[6] G. Christopoulos, D.E. Kandzari, R.W. Yeh, F.A. Jaffer, D. Karmpaliotis, M.R. Wyman,K. Alaswad, W. Lombardi, J.A. Grantham, J. Moses, G. Christakopoulos, M.N. Tarar,

56 A. Karatasakis et al. / International Journal of Cardiology 224 (2016) 50–56
B.V. Rangan, N. Lembo, S. Garcia, D. Cipher, C.A. Thompson, S. Banerjee, E.S. Brilakis,Development and validation of a novel scoring system for predicting technical suc-cess of chronic total occlusion percutaneous coronary interventions: the progressCTO (prospective global registry for the study of chronic total occlusion interven-tion) score, JACC Cardiovasc. Interv. 9 (2016) 1–9.
[7] G. Alessandrino, B. Chevalier, T. Lefevre, F. Sanguineti, P. Garot, T. Unterseeh, T.Hovasse, M.C. Morice, Y. Louvard, A clinical and angiographic scoring system to pre-dict the probability of successful first-attempt percutaneous coronary interventionin patients with total chronic coronary occlusion, JACC Cardiovasc. Interv. 8(2015) 1540–1548.
[8] V.G. Patel, K.M. Brayton, A. Tamayo, O. Mogabgab, T.T. Michael, N. Lo, M. Alomar, D.Shorrock, D. Cipher, S. Abdullah, S. Banerjee, E.S. Brilakis, Angiographic success andprocedural complications in patients undergoing percutaneous coronary chronictotal occlusion interventions: a weighted meta-analysis of 18,061 patients from 65studies, JACC Cardiovasc. Interv. 6 (2013) 128–136.
[9] G. Christopoulos, R.V. Menon, D. Karmpaliotis, K. Alaswad, W. Lombardi, J.A.Grantham, T.T. Michael, V.G. Patel, B.V. Rangan, A.P. Kotsia, N. Lembo, D.E.Kandzari, J. Lee, A. Kalynych, H. Carlson, S. Garcia, S. Banerjee, C.A. Thompson, E.S.Brilakis, Application of the “hybrid approach” to chronic total occlusions in patientswith previous coronary artery bypass graft surgery (from a contemporarymulticen-ter us registry), Am. J. Cardiol. 113 (2014) 1990–1994.
[10] T.T. Michael, D. Karmpaliotis, E.S. Brilakis, E. Fuh, V.G. Patel, O.Mogabgab, M. Alomar,B.L. Kirkland, N. Lembo, A. Kalynych, H. Carlson, S. Banerjee, W. Lombardi, D.E.Kandzari, Procedural outcomes of revascularization of chronic total occlusion of na-tive coronary arteries (from amulticenter United States registry), Am. J. Cardiol. 112(2013) 488–492.
[11] G. Christopoulos, D. Karmpaliotis, K. Alaswad, R.W. Yeh, F.A. Jaffer, R.M. Wyman,W.L. Lombardi, R.V. Menon, J.A. Grantham, D.E. Kandzari, N. Lembo, J.W. Moses,A.J. Kirtane, M. Parikh, P. Green, M. Finn, S. Garcia, A. Doing, M. Patel, J.Bahadorani, M.N. Tarar, G.E. Christakopoulos, C.A. Thompson, S. Banerjee, E.S.Brilakis, Application and outcomes of a hybrid approach to chronic total occlusionpercutaneous coronary intervention in a contemporary multicenter us registry,Int. J. Cardiol. 198 (2015) 222–228.
[12] G. Christopoulos, R.M. Wyman, K. Alaswad, D. Karmpaliotis, W. Lombardi, J.A.Grantham, R.W. Yeh, F.A. Jaffer, D.J. Cipher, B.V. Rangan, G.E. Christakopoulos, M.A.Kypreos, N. Lembo, D. Kandzari, S. Garcia, C.A. Thompson, S. Banerjee, E.S. Brilakis,Clinical utility of the Japan-chronic total occlusion score in coronary chronic totalocclusion interventions: results from a multicenter registry, Circ. Cardiovasc. Interv.8 (2015), e002171.
[13] J. Karacsonyi, A. Karatasakis, D. Karmpaliotis, K. Alaswad, R.W. Yeh, F.A. Jaffer, M.R.Wyman, W.L. Lombardi, J.A. Grantham, D.E. Kandzari, N. Lembo, J.W. Moses, A.J.Kirtane, M.A. Parikh, P. Green, M. Finn, S. Garcia, A. Doing, M. Patel, J. Bahadorani,J.R. Martinez Parachini, E. Resendes, B.V. Rangan, I. Ungi, C.A. Thompson, S.Banerjee, E.S. Brilakis, Effect of previous failure on subsequent procedural outcomesof chronic total occlusion percutaneous coronary intervention (from a contempo-rary multicenter registry), Am. J. Cardiol. (2016).
[14] G. Christopoulos, R.V. Menon, D. Karmpaliotis, K. Alaswad, W. Lombardi, A.Grantham, V.G. Patel, B.V. Rangan, A.P. Kotsia, N. Lembo, D. Kandzari, H. Carlson, S.Garcia, S. Banerjee, C.A. Thompson, E.S. Brilakis, The efficacy and safety of the"hybrid" approach to coronary chronic total occlusions: insights from a contempo-rary multicenter us registry and comparison with prior studies, J. Invasive Cardiol.26 (2014) 427–432.
[15] G. Christopoulos, D. Karmpaliotis, K. Alaswad, W.L. Lombardi, J.A. Grantham, B.V.Rangan, A.P. Kotsia, N. Lembo, D.E. Kandzari, J. Lee, A. Kalynych, H. Carlson, S.Garcia, S. Banerjee, C.A. Thompson, E.S. Brilakis, The efficacy of “hybrid” percutane-ous coronary intervention in chronic total occlusions caused by in-stent restenosis:insights from a us multicenter registry, Catheter. Cardiovasc. Interv. 84 (2014)646–651.
[16] G. Christopoulos, D. Karmpaliotis, M.R. Wyman, K. Alaswad, J. McCabe, W.L.Lombardi, J.A. Grantham, S.P. Marso, A.P. Kotsia, B.V. Rangan, S.A. Garcia, N.Lembo, D. Kandzari, J. Lee, A. Kalynych, H. Carlson, C.A. Thompson, S. Banerjee, E.S.Brilakis, Percutaneous intervention of circumflex chronic total occlusions is associ-ated with worse procedural outcomes: insights from a multicentre US registry,Can. J. Cardiol. 30 (2014) 1588–1594.
[17] J. Sapontis, G. Christopoulos, J.A. Grantham, R.M. Wyman, K. Alaswad, D.Karmpaliotis, W.L. Lombardi, J.M. McCabe, S.P. Marso, A.P. Kotsia, B.V. Rangan, G.E.
Christakopoulos, S. Garcia, C.A. Thompson, S. Banerjee, E.S. Brilakis, Procedural fail-ure of chronic total occlusion percutaneous coronary intervention: insights from amulticenter us registry, Catheter. Cardiovasc. Interv. 85 (2015) 1115–1122.
[18] K. Alaswad, R.V. Menon, G. Christopoulos, W.L. Lombardi, D. Karmpaliotis, J.A.Grantham, S.P. Marso, M.R. Wyman, N.R. Pokala, S.M. Patel, A.P. Kotsia, B.V.Rangan, N. Lembo, D. Kandzari, J. Lee, A. Kalynych, H. Carlson, S.A. Garcia, C.A.Thompson, S. Banerjee, E.S. Brilakis, Transradial approach for coronary chronictotal occlusion interventions: insights from a contemporary multicenter registry,Catheter. Cardiovasc. Interv. 85 (2015) 1123–1129.
[19] K. Thygesen, J.S. Alpert, A.S. Jaffe, M.L. Simoons, B.R. Chaitman, H.D. White, JointESCAAHAWHFTFftUDoMI, H.A. Katus, B. Lindahl, D.A. Morrow, P.M. Clemmensen,P. Johanson, H. Hod, R. Underwood, J.J. Bax, R.O. Bonow, F. Pinto, R.J. Gibbons, K.A.Fox, D. Atar, L.K. Newby, M. Galvani, C.W. Hamm, B.F. Uretsky, P.G. Steg, W. Wijns,J.P. Bassand, P. Menasche, J. Ravkilde, E.M. Ohman, E.M. Antman, L.C. Wallentin,P.W. Armstrong, M.L. Simoons, J.L. Januzzi, M.S. Nieminen, M. Gheorghiade, G.Filippatos, R.V. Luepker, S.P. Fortmann, W.D. Rosamond, D. Levy, D. Wood, S.C.Smith, D. Hu, J.L. Lopez-Sendon, R.M. Robertson, D. Weaver, M. Tendera, A.A. Bove,A.N. Parkhomenko, E.J. Vasilieva, S. Mendis, Third universal definition of myocardialinfarction, Circulation 126 (2012) 2020–2035.
[20] S. Lemeshow, D.W. Hosmer Jr., A review of goodness of fit statistics for use in the de-velopment of logistic regression models, Am. J. Epidemiol. 115 (1982) 92–106.
[21] B.J. McNeil, J.A. Hanley, Statistical approaches to the analysis of receiver operatingcharacteristic (ROC) curves, Med. Decis. Making 4 (1984) 137–150.
[22] A.R. Galassi, S.D. Tomasello, N. Reifart, G.S. Werner, G. Sianos, H. Bonnier, H. Sievert,S. Ehladad, A. Bufe, J. Shofer, A. Gershlick, D. Hildick-Smith, J. Escaned, A. Erglis, I.Sheiban, L. Thuesen, A. Serra, E. Christiansen, A. Buettner, L. Costanzo, G. Barrano,C. Di Mario, In-hospital outcomes of percutaneous coronary intervention in patientswith chronic total occlusion: insights from the ERCTO (European Registry of ChronicTotal Occlusion) registry, EuroIntervention 7 (2011) 472–479.
[23] C.A. Thompson, J.E. Jayne, J.F. Robb, B.J. Friedman, A.V. Kaplan, B.D. Hettleman, N.W.Niles, W.L. Lombardi, Retrograde techniques and the impact of operator volume onpercutaneous intervention for coronary chronic total occlusions an early U.S. expe-rience, JACC Cardiovasc. Interv. 2 (2009) 834–842.
[24] T. Teramoto, E. Tsuchikane, H. Matsuo, Y. Suzuki, T. Ito, T. Ito, M. Habara, K. Nasu, M.Kimura, Y. Kinoshita, M. Terashima, Y. Asakura, T. Matsubara, T. Suzuki, Initialsuccess rate of percutaneous coronary intervention for chronic total occlusion in anative coronary artery is decreased in patients who underwent previous coronaryartery bypass graft surgery, JACC Cardiovasc. Interv. 7 (2014) 39–46.
[25] T.T. Michael, D. Karmpaliotis, E.S. Brilakis, S.M. Abdullah, B.L. Kirkland, K.L. Mishoe,N. Lembo, A. Kalynych, H. Carlson, S. Banerjee, W. Lombardi, D.E. Kandzari, Impactof prior coronary artery bypass graft surgery on chronic total occlusionrevascularisation: insights from a multicentre US registry, Heart 99 (2013)1515–1518.
[26] A. El Sabbagh, V.G. Patel, O.M. Jeroudi, T.T. Michael, M.E. Alomar, O. Mogabgab, E.Fuh, M. Roesle, B.V. Rangan, S. Abdullah, J.L. Hastings, J. Grodin, D.J. Kumbhani, D.Alexopoulos, P. Fasseas, S. Banerjee, E.S. Brilakis, Angiographic success and proce-dural complications in patients undergoing retrograde percutaneous coronarychronic total occlusion interventions: a weighted meta-analysis of 3482 patientsfrom 26 studies, Int. J. Cardiol. 174 (2014) 243–248.
[27] R. Mehran, E.D. Aymong, E. Nikolsky, Z. Lasic, I. Iakovou, M. Fahy, G.S. Mintz, A.J.Lansky, J.W. Moses, G.W. Stone, M.B. Leon, G. Dangas, A simple risk score for predic-tion of contrast-induced nephropathy after percutaneous coronary intervention:development and initial validation, J. Am. Coll. Cardiol. 44 (2004) 1393–1399.
[28] L. Nombela-Franco, M. Urena, M. Jerez-Valero, C.M. Nguyen, H.B. Ribeiro, Y. Bataille,J. Rodes-Cabau, S. Rinfret, Validation of the J-Chronic Total Occlusion score forchronic total occlusion percutaneous coronary intervention in an independent con-temporary cohort, Circ. Cardiovasc. Interv. 6 (2013) 635–643.
[29] H. Tanaka, Y. Morino, M. Abe, T. Kimura, Y. Hayashi, T. Muramatsu, M. Ochiai, Y.Noguchi, K. Kato, Y. Shibata, Y. Hiasa, O. Doi, T. Yamashita, T. Morimoto, T.Hinohara, T. Fujii, K. Mitsudo, Impact of J-CTO score on procedural outcome and tar-get lesion revascularisation after percutaneous coronary intervention for chronictotal occlusion: a substudy of the J-CTO registry (Multicentre CTO Registry inJapan), EuroIntervention 11 (2016) 981–988.