Embed Size (px)
Citation preview

journal of Hospital Infection (1995) 30 (Supplement), 179-190
Congenital toxoplasmosis: prevention, screening and treatment
R. E. Holliman
Department of Medical Microbiology and Public Health Laboratory, St George’s Hospital, Blackshaw Road, London SW1 7 O&T, UK
Summary: Congenital toxoplasmosis is an established cause of abortion, neonatal disease and ocular defects presenting in later life. Preventative options include health education, immunization and screening of pregnant women and infants with appropriate management of cases found to be at risk. Screening requires a knowledge of the disease, the test, the treatment and the administration of the proposed programme. Treatment can be directed towards the acutely infected mother, the infected fetus or infant and the patient with an acute exacerbation of ocular toxoplasmosis following congenital infection. Harm-benefit assessment of screening programmes designed to prevent congenital toxoplasmosis has produced conflicting res- ults. Further research is required into the incidence of acute toxoplasmosis in pregnancy and subsequent congenital infection, the frequency of neonatal handicap, precise tests for the diagnosis of recent maternal infection and the presence of congenital toxoplasmosis and improved treatment of the infection.
Keywords: Congenital toxoplasmosis; prevention; screening; treatment.
Introduction
Toxoplasma infection of immune competent persons is a benign condition, usually asymptomatic but presenting with self-limiting lymphadenopathy and malaise in a minority of cases. In contrast, infection of im- munocompromised individuals results in significant morbidity and mor- tality. Organ graft recipients, HIV-infected individuals and patients with malignancy may suffer life-threatening toxoplasmosis. However, the fetus represents the largest group of immunocompromised individuals in the population and congenital toxoplasmosis is an established cause of in- trauterine death and severe neonatal disease. Late sequelae of congenital infection include ocular disease and mental retardation.’ In an attempt to reduce the incidence of congenital toxoplasmosis a number of countries, notably France’ and Austria,3 have introduced national prenatal screening programmes for this infection. More recently there have been calls from health care workers and lay groups that similar schemes be adopted in the UK4 and North America.’ In order to assess the merits of this debate it is necessary to consider the clinical condition that is congenital toxoplasmosis, putative preventative measures-particularly prospective screening-and specific treatment of infected mothers and their offspring.6
0195-6701/95/060179+12 $08.00/O
179 0 1995 The Hospital Infection Society

R. E. Holliman
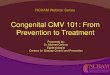
Second t&nester
Not ktlOWll (rare?)
Not known
Fetal infection
Severe disease at birth
Ocular sequelae in later life
Figure 1. Transmission of toxoplasmosis associated with pregnancy.
Congenital toxoplasmosis
Toxoplasmosis is primarily acquired by swallowing one of the life-forms of the parasite. Sporocysts are found in soil contaminated by infected cat faeces and may be carried to the mouth on poorly washed vegetables or fingers. Tissue cysts are present in meat derived from infected animals, notably pork and lamb, and remain viable when the meat is eaten raw or lightly cooked.’ Congenital toxoplasmosis occurs when the parasite establishes an infection of the placenta and subsequently crosses to reach the fetus. Conventional theory is that infection is only transmitted from mother to fetus when maternal toxoplasmosis is first acquired during, or shortly before, conception. This reflects the relatively brief period of parasitaemia after primary exposure when toxoplasma may be carried in the blood to the placenta.7 However, cases of congenital toxoplasmosis associated with maternal infection acquired prior to conception have been reported in both immune compromised and immunocompetent mothers. The incidence of this phenomenon is not established.8 Overall, 40-50% of untreated maternal infections acquired during pregnancy will be passed to the fetus. Transmission is more frequent later in pregnancy. However, the incidence of clinically severe congenital toxoplasmosis is greater when the mother is infected during the first trimester, so that only 10% of infected babies are markedly affected at birth7 (Figure 1).

Congenital toxoplasmosis 181
In most countries the incidence of toxoplasmosis acquired in pregnancy and congenital infection is not established. Based on estimates of maternal infection of two per 1000 pregnancies, it was calculated that 30-40 seriously affected cases of congenital toxoplasmosis may occur in the UK each year.’ This estimate was found to be discordant with the observation of only 14 cases, not all seriously affected, reported to the British Paediatric Sur- veillance Unit between 1989-1990.6 Furthermore, there is evidence that the rate of community exposure to toxoplasma has fallen over recent years, lo possibly associated with changes in farming practice and the consumption of previously deep frozen meats (toxoplasma cysts are inactivated at low temperatures). Consequently the percentage of susceptible women acquiring toxoplasmosis in pregnancy may fall, although the susceptible population will have increased.
Primary toxoplasma infection of pregnant women is asymptomatic or accompanied by a mild, self-limiting non-specific illness of malaise and lethargy in over three-quarters of cases. As a result, acute maternal infection is rarely clinically apparent, unlike other infections which threaten the fetus such as rubella and varicella. Over 90% of congenitally-infected infants are asymptomatic at birth. The classical triad of congenital toxoplasmosis (hydrocephalus, intracranial calcification and choroidoretinitis) is very much the extreme and less usual clinical presentation. Non-specific signs of congenital toxoplasmosis include hepatosplenomegaly, jaundice, thrombo- cytopenia, growth retardation and rash,i’ but these are rarely seen in the absence of the more characteristic features. Acute maternal toxoplasmosis can result in intrauterine death, particularly when acquired early in preg- nancy. Cases of chronic maternal toxoplasmosis resulting in spontaneous abortion have also been described, but the incidence of these sequelae are not known.’ Long-term follow-up of initially asymptomatic children with congenital toxoplasmosis is vital to establish the frequency of late onset disease associated with the condition. Due to the low numbers of identified cases and the need to monitor for several decades, only a few, small studies have been completed. A Dutch study found that four of five symptomatic treated children, and four of six asymptomatic, untreated children developed ocular lesions, some appearing as late as 18 years after birth.12,13 In a second, North American study, seven of 13 asymptomatic children with congenital toxoplasmosis were treated prospectively. Of these 13 children three de- veloped unilateral blindness, five showed bilateral retinitis and three de- veloped unilateral retinitis. Five children developed neurological defects.14
Prevention of congenital toxoplasmosis
Congenital infection may be prevented by intervention at a number of stages in the progression of the disease. Primary prevention seeks to eliminate toxoplasma infection of the pregnant women and could be achieved by vaccination or health education programmes. If maternal infection has

182 R. E. Holliman
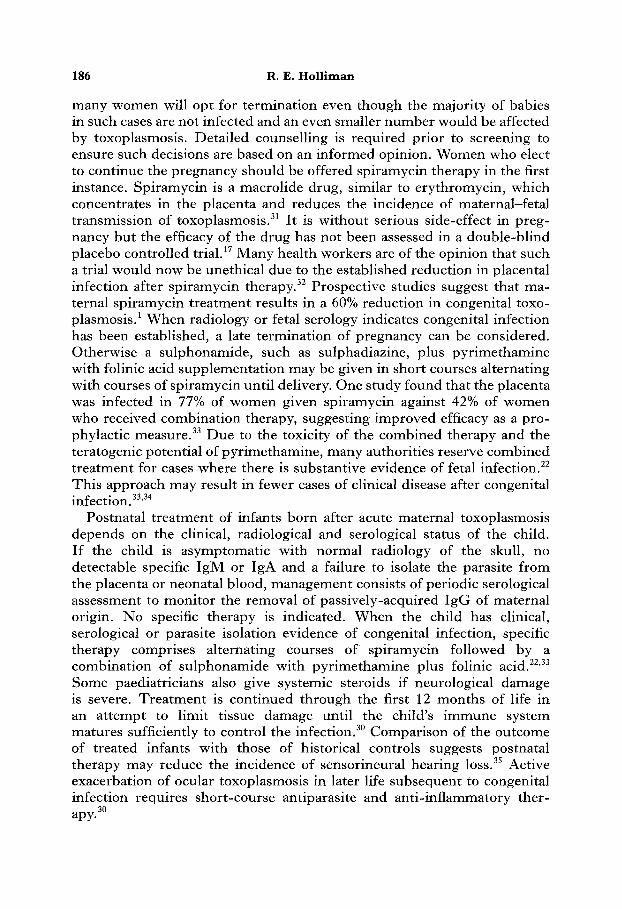
Health education -) +- Vaccination - Cats - Food animals - Human
Maternal screening Prz;;;;ptual
Therapeutic treatment until delivery
Acute - Termination Infection - Prophylactic detected Drug therapy
until delivery
Termination
Short-course treatment -b during episodes of active 1
+- Therapeutic treatment until aged 12 months
Ocular disease
Figure 2. Prevention of congenital toxoplasmosis.
occurred, those pregnancies ‘at risk’ might be identified by systematic screening. Secondary prevention involves treatment or termination of preg- nancies found to be at risk during systemic screening. Tertiary prevention attempts to identify the infected fetus or baby and to manage such cases by termination of pregnancy or specific treatment. At this level ‘prevention’ aims to reduce the number of affected cases rather than to reduce the incidence of infection. A programme aimed at reducing the incidence of clinically apparent congenital toxoplasmosis may include any or all of the measures indicated in Figure 2.
Vaccination There are a number of approaches to the prevention of toxoplasmosis by vaccination. Live vaccines incorporate avirulent strains of toxoplasma attenuated by irradiation or temperature sensitivity. These preparations are more immunogenic than vaccines using extracts or homogenates of killed parasite. Heterologous immunization uses the cross-reactivity of closely related organisms, such as Hammondia hammondi, to induce resistance to toxoplasma infection. Other methods include induction of non-specific immunity with adjuvant preparations or the injection of toxoplasma nucleic acid.” None of the vaccines is suitable for use in humans due to problems of chronic infection with subsequent reactivation, toxicity, or lack of solid long-lasting immunity to ‘wild strain’ infection. A temperature sensitive mutant of toxoplasma (S48) has been used to protect sheep in field trialsI and may limit one source of human infection.
Health education Human toxoplasmosis is acquired by swallowing tissue cysts in raw or partially cooked meats or from ingestion of sporocysts contaminating soil

Congenital toxoplasmosis
Table I. Health education to reduce exposure to Toxoplasma gondii
183
Objective: Action: Specifics:
Avoid swallowing the parasite Basic hygiene is sufficient Wash hands after handling raw meat or gardening. Wear gloves if possible
Only eat meat which is well cooked. Do not eat raw or undercooked meat or drink unpasteurized milk
If possible let someone else clean cat-litter trays. Otherwise, clean daily wearing gloves and wash hands immediately afterwards
Table II. Screening options for toxoplasmosis associated with pregnancy
Population screened Target group to be identified Action
Women Not exposed pre-conception to toxoplasma
Pregnant Acute toxoplasma women infection
Health education (vaccination)
Termination Specific therapy Fetal assessment
Neonates Congenital toxoplasmosis
Specific therapy in early life. Ophthalmic supervision
or vegetables. The relative importance of the different routes of transmission are not established and may vary from one region to another.17 Broad health education with emphasis on good hygiene” is offered to pregnant women in an attempt to reduce the incidence of acute toxoplasmosis (Table I). Although widely promoted, the efficacy of this approach is not fully evaluated. Appropriate health education can alter the behaviour of pregnant women in such a way as to reduce potential exposure to the parasite” but the effect on the acquisition of toxoplasmosis has not been studied. Poorly designed information may be counterproductive by raising anxiety levels. Effective communication with the patient population requires planning, a selective content and must pay careful attention to the use of language. Illustrations are of lesser value.”
Screening
Screening for congenital toxoplasmosis can be performed in a number of ways, each with distinct objectives (Table II). Screening of women before conception attempts to identify those at risk of subsequent acute infection and to offer these persons appropriate health education or, in the future, vaccination. Screening of pregnant women is designed to recognize those

184 R. E. Holliman
with acute toxoplasmosis who may benefit from specific therapy and can be offered further tests to determine the status of the fetus. Screening of samples from neonates tries to identify congenitally-infected babies who require drug therapy in early life, followed by ophthalmic supervision. The widely publicized French national screening programme is based on pre- conception testing of women, followed by periodic assessment of susceptible individuals throughout pregnancy looking for seroconversion.2,21 When acute infection is detected, ultrasound investigation and testing of fetal blood obtained by cordocentesis is performed.22 Fetal blood sampling is associated with significant morbidity and mortality and the general validity of this technique has been questioned.23 When applied to toxoplasmosis associated with pregnancy, the sensitivity of detecting congenital infection was found to be 93%22 and a lack of specificity has been reported.24
When results of pre-conception tests are not available, difficulties arise in the estimation of the duration of maternal infection. The kinetics and magnitude of the individual’s serological response to toxoplasma infection are variable, as are the sensitivity and specificity of different tests to detect acute infection. Consequently, women may be falsely reassured as being chronic infected or inappropriately managed as acutely infected in early pregnancy. At present there is no precise test of recent toxoplasma infection other than seroconversion; estimation of parameters such as IgM and IgG avidity are not sufficiently reliable for population screening.25
Postnatal screening for congenitally-infected infants has been performed in New England since 1986.26 Although this approach does not allow therapeutic intervention during the pregnancy it has the advantages of reduced screening costs and avoidance of controversy over therapeutic abortion. It is particularly appropriate in regions where immunity in the pregnant population is low. The New England programme is based on the detection of toxoplasma-specific IgM in neonatal blood samples obtained by heel-prick and stored on filter paper. The sensitivity and specificity of this approach has not been established, but the system would not be expected to identify asymptomatic cases of congenital toxoplasmosis which lack a detectable IgM response and which may constitute the majority of cases of congenital toxoplasma infection. An alternative system of postnatal screening has been established in Denmark. Here, first trimester maternal blood and neonatal Guthrie card samples are compared for toxoplasma IgG status in order to select instances of seroconversion.27 Children resulting from ‘at risk’ pregnancies are then investigated during the first year of life (Table III).
A major defect of all screening models for congenital toxoplasmosis has been the failure to achieve satisfactory case compliance. In a UK study only 50% of self-selected, motivated women, found to be at high risk of congenital transmission, completed an investigation procedure leading to a final diagnosis of the status of the child.28 Indeed, in the absence of enhanced specialist intervention, this figure fell to 25%. In France, 133

Congenital toxoplasmosis
Table III. Screening procedures for toxoplasmosis associated with pregnancy
Reference Method Advantages Disadvantages number
185
21
3 25 41
27
26
Pre-conception IgG High sensitivity and Poor compliance with specificity due to pre-conception testing
IgG status during precision of IgG tests pregnancy Costs of multiple tests
Early intervention for during pregnancy Confirmation of ‘at risk’ pregnancies seroconversion by IgM measurement
IgG + IgM status in Improved early pregnancy compliance
IgG and/or IgM assessment during pregnancy
Early intervention for ‘at risk’ pregnancies
IgG status in early pregnancy
IgG status on cord blood
IgM testing of cord blood
High sensitivity and Does not allow specificity due to intervention prior to precision of IgG tests delivery
Improved compliance
Reduced costs
Much reduced costs
Full compliance
Poor specificity of IgM as a measure of recent infection
Costs of multiple tests during pregnancy
Poor sensitivity as IgM-negative infected babies are not identified
Does not allow intervention prior to delivery
(41%) of 326 infants with suspected congenital toxoplasmosis were not followed up for more than six weeks.29
Treatment
Management of toxoplasmosis associated with pregnancy can be directed toward the mother, the fetus and the baby (Figure 2). Once infection is established no treatment is curative because none of the currently available anti-toxoplasma drugs have reliable activity against the cyst form of the parasite.30 Consequently, treatment of the mother aims to prevent fetal infection while treatment of the fetus and infant aims to limit physical damage due to infection.
When a pregnancy is found to be at risk due to acute toxoplasma infection
186 R. E. Holliman
many women will opt for termination even though the majority of babies in such cases are not infected and an even smaller number would be affected by toxoplasmosis. Detailed counselling is required prior to screening to ensure such decisions are based on an informed opinion. Women who elect to continue the pregnancy should be offered spiramycin therapy in the first instance. Spiramycin is a macrolide drug, similar to erythromycin, which concentrates in the placenta and reduces the incidence of maternal-fetal transmission of toxoplasmosis.31 It is without serious side-effect in preg- nancy but the efficacy of the drug has not been assessed in a double-blind placebo controlled tria1.l’ Many health workers are of the opinion that such a trial would now be unethical due to the established reduction in placental infection after spiramycin therapy.32 Prospective studies suggest that ma- ternal spiramycin treatment results in a 60% reduction in congenital toxo- plasmosis.’ When radiology or fetal serology indicates congenital infection has been established, a late termination of pregnancy can be considered. Otherwise a sulphonamide, such as sulphadiazine, plus pyrimethamine with folinic acid supplementation may be given in short courses alternating with courses of spiramycin until delivery. One study found that the placenta was infected in 77% of women given spiramycin against 42% of women who received combination therapy, suggesting improved efficacy as a pro- phylactic measure.33 Due to the toxicity of the combined therapy and the teratogenic potential of pyrimethamine, many authorities reserve combined treatment for cases where there is substantive evidence of fetal infection.22 This approach may result in fewer cases of clinical disease after congenital infection.33’34
Postnatal treatment of infants born after acute maternal toxoplasmosis depends on the clinical, radiological and serological status of the child. If the child is asymptomatic with normal radiology of the skull, no detectable specific IgM or IgA and a failure to isolate the parasite from the placenta or neonatal blood, management consists of periodic serological assessment to monitor the removal of passively-acquired IgG of maternal origin. No specific therapy is indicated. When the child has clinical, serological or parasite isolation evidence of congenital infection, specific therapy comprises alternating courses of spiramycin followed by a combination of sulphonamide with pyrimethamine plus folinic acid.22,33 Some paediatricians also give systemic steroids if neurological damage is severe. Treatment is continued through the first 12 months of life in an attempt to limit tissue damage until the child’s immune system matures sufficiently to control the infection.30 Comparison of the outcome of treated infants with those of historical controls suggests postnatal therapy may reduce the incidence of sensorineural hearing 10~s.~’ Active exacerbation of ocular toxoplasmosis in later life subsequent to congenital infection requires short-course antiparasite and anti-inflammatory ther- apy.30

Congenital toxoplasmosis
Table IV. Principles of weening
187
Disease: The disease should be an important health problem with a well-described natural history and identifiable early stage
Test: There should be a suitable diagnostic test, acceptable to the target population
Treatment: Treatment at the early stage of the disease should be of greater benefit than delayed treatment
Administration: There should be adequate facilities for diagnosis and effective treatment of cases identified
Harm:benefit ratio: Screened individuals should have a lower risk of physical or psychological harm than the chance of benefit
Harm --benefit assessment
The evaluation of a systematic programme of prevention, screening and treatment of toxoplasmosis associated with pregnancy must apply certain criteria.36 It is necessary to establish basic facts about the disease itself, the diagnostic tests to be used, the treatment of the condition and the administrative structure of the programme. Overall the benefits of the programme must outweigh the associated harm (Table IV). In the context of congenital toxoplasmosis, a number of problems exist when evaluating intervention programmes. The size of the problem remains uncertain in most countries.* Most importantly the degree of handicap due to congenital toxoplasmosis has not been defined and calculations based on disease presentation prior to the development of modern medical management may be inappropriate.6 The precision of toxoplasma serology tests may not be adequate when applied to a large population with a low incidence of infection2j so that excessive numbers of false-positive and false-negative findings may occur. Patient acceptance of diagnostic and management for toxoplasma in pregnancy has been assumed despite a number of studies indicating that compliance is, in reality, relatively low.“,37 In many countries there are insufficient resources for the patient counselling, detailed laborat- ory testing and fetal blood sampling required in a screening programme. The efficacy of drug therapy of acute toxoplasmosis in pregnancy, fetal infection and during the postnatal period has not been subjected to vigorous, controlled trials. These limitations indicate that any calculation of the harm: benefit ratio is speculative at best.
Benefits of screening for congenital toxoplasmosis include: a reduction in the numbers of babies born with overt disease and of those who develop ocular problems in later life; a reduction in the severity of damage in some infected individuals; the provision of reassurance to pregnant women found to be immune to the infection; and the satisfaction of parental demand for

188 R. E. Holliman
the screening process itself.” Harm associated with screening includes: wastage of uninfected or infected but undamaged fetuses;6 psychological damage to the parents when the programme fails and a child with congenital toxoplasmosis is born; maternal concern generated by the necessary delays and decision-making involved during testing;38 and the complications of drug therapy and termination of pregnancy.39 Calculations of the financial costs of screening and the savings in health expenditure resulting from the prevention of handicap are complex and imprecise. Some studies have concluded that UK costs would outweigh savings4’ while others found the reverse situation in Scotland.41 Global consideration of the harm:benefit ratio have led some authorities to promote screening in the US,’ France4’ and the UK.4X20 Others have considered the same data and concluded that screening should not be introduced in the UK43 and questioned its continuation in France.17 As a result, ad hoc testing on demand takes place in the absence of organized screening programmes in most countries while Austria and France remain committed to prenatal screening despite suboptimal evaluation of this approach.‘j
Future prospects
Given the present unsatisfactory position, which is the way forward? Firstly, a clear understanding that the pregnant woman with an illness compatible with toxoplasmosis should be investigated. In the UK the well but worried woman should be given careful counselling as to the benefits and potential harm that could be generated by screening and only selected individuals should proceed to testing. Routine screening of a pregnant population is not indicated outside of ethically approved, properly funded, scientific studies.43 All pregnant women should be given simple health education concentrating on the value of good hygiene. Those interested in the subject must recognize that the onus of proof lies with those who believe routine screening should be introduced. Any programme must be regarded as experimental research until the value and safety of that approach has been confirmed.# Directed research is required into the incidence of toxoplasmosis in pregnancy and of congenital infection, the frequency of physical or mental handicap due to congenital toxoplasmosis,43 development of screening tests for the infection with enhanced precision and the in- troduction of efficacious, safe treatment, particularly drugs which eradicate the cyst form of the parasite.
Health care workers and lay groups must accept full responsibility for the sequelae of their actions. The general practitioner, obstetrician or midwife who orders toxoplasma serology testing of a pregnant woman must appreciate that this action may result in a child being subjected to repeated investigations in early life. Patient help groups who promote routine screening and claim credit for a beneficial outcome should share the responsibility when harm results. Most importantly perhaps, those for and

Congenital toxoplasmosis 189
against screening should cooperate towards the common goal of improved health care. The two sides have been portrayed as the ‘evangelists’ marching towards the holy grail of universal screening and the ‘snails’ studiously considering the problems along the route.6z45 The enthusiasm of one group should be combined with the logic of the other to secure progress through good research.
I am grateful to Mrs Ivy Crossman for her expert secretarial assistance.
1.
2.
3.
4. 5.
6. 7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
References
Remington JS, Desmonts G. Toxoplasmosis. In: Remington JS, Klein JO, Eds. Infectious Diseases of Foetus and Newborn Infant, 3rd edn. Philadelphia: WB Saunders 1990, 89-195. Thulliez P. Screening programme for congenital toxoplasmosis in France. Stand J Infect Dis 1992; S84: 43-45. Aspock H, Pollak A. Prevention of prenatal toxoplasmosis by serological screening of pregnant women in Austria. Stand J Infect Dis 1993; S84: 32-38. Joynson DH, Payne R. Screening for toxoplasma in pregnancy. Lancet 1988; ii: 795-796. McCabe R, Remington JS. Toxoplasmosis: the time has come. N Eng J Med 1988; 318: 313-31s. Hall SM. Congenital toxoplasmosis. BMJ 1992; 305: 291-297. Desmonts G, Couvreur J. Toxoplasmosis in pregnancy and its transmission to the foetus. Bul N Y Acad Med 1974; 50: 146-159. Holliman RE. Clinical sequelae of chronic maternal toxoplasmosis. Rev Med Microbial 1994; 5: 47-55. Joynson DH. Epidemiology of toxoplasmosis in the UK. ScandJ Infect Dis 1992; S84: 65-69. Walker J, Nokes DJ, Jennings R. Longitudinal study of toxoplasma seroprevalence in South Yorkshire. Epidemiol Infect 1992; 108: 99-106. Peckham CS, Logan S. Screening for toxoplasmosis during pregnancy. Arch Dis Child 1993; 68: 3-5. Koppe JG, Lower-Sieger DH, de Roever-Bonnet H. Results of 20 year follow-up of congenital toxoplasmosis. Lancet 1986; i: 254-256. Koppe JG, Rothova A. Congenital toxoplasmosis. A long-term follow-up of 20 years. Int Ophthalmol 1989; 13: 387-390. Wilson CB, Remington JS, Stagno S, Reynolds DW. Development of adverse sequelae in children born with subclinical congenital toxoplasma infection. Pediatrics 1980; 66: 767-774. Hermentin K, Aspiick H. Efforts towards a vaccine against Toxoplasma gondii: a review. Zbl Bakt Hyg 1988; 269: 423-426. Buxton D, Thomson K, Maley S, Wright S, Bos HJ. Vaccination of sheep with a live, incomplete strain (S48) of Toxoplasma gondii and their immunity to challenge when pregnant. IAt Ret 1991; 129: 89-93. Jeanne1 D, Costagliola D, Niel G, Hubert B, Danis M. What is known about the prevention of congenital toxoplasmosis? Lancet 1990; 336: 359-361. Frenkel JK. Breaking the transmission chain of toxoplasma: a program for the prevention of human toxoplasmosis. Bull N Y Acad Med 1974; 50: 228-235. Carter AO, Gelmon SB, Wells GA, Toepell AP. The effectiveness of a prenatal education programme for the prevention of congenital toxoplasmosis. Epidemiol Infect 1989; 103: 539-545. Ho-Yen DO, Chatterton JM. Congenital toxoplasmosis-why and how to screen. Rev Med Microbial 1990; 1: 229-235. Lelong M. Prophylaxie des toxoplasmoses du nouveau n& et de la femme enceinte. Rev Hyg Med Sot 1959; 7: 531. Daffos F, Forestier F, Capella-Paulousky M et al. Prenatal management of 746 preg- nancies at risk for congenital toxoplasmosis. N Eng r Med 1988; 318: 271-275.

190 R. E. Holliman
23. 24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
38. 39.
40.
41.
42. 43.
44. 45.
Fisk N, Bower S. Fetal blood sampling in retreat. BMJ 1993; 307: 143-144. Holliman RE, Johnson JD, Constantine G, Bissenden JG, Nicholaides K, Savva D. Difficulties in the diagnosis of congenital toxoplasmosis by cordocentesis. Case report. BrJ Obstet Gynaecol 1991; 98: 832-836. Aedes AE. Evaluating the sensitivity and predictive value of tests of recent infection: toxoplasmosis in pregnancy. Epidemiol Infect 1991; 107: 527-535. Hsu HW, Grady GF, Maguire JH, Weiblen BJ, Hoff R. Newborn screening for congenital toxoplasmosis infection: Five years experience in Massachusetts, USA. Stand J Infect Dis 1992; S84: 59-64. Lebech M, Petersen E. Neonatal screening for congenital toxoplasmosis in Denmark: Presentation of the design of a prospective study. Stand J Infect Dis 1992; S84: 75-79. Hartup C, Johnson JD, Holliman RE. Medical audit of the investigation of toxoplasmosis associated with pregnancy. Lancet 1992; 340: 118. Pujol M, Malbruny B, Morel C, Exmelin L. Rappel de l’importance du suivi serologique des enfants suspects de toxoplasmose congenitale. Pathol Biol 1992; 40: 238-241. Holliman RE. Uncommon infections: 4. Toxoplasmosis, toxocariasis and crypto- sporidiosis. Prescribers J 1992; 32: 127-l 32. Stryay-Pedersen B. Treatment of toxoplasmosis in the pregnant mother and newborn child. Stand J Infect Dis 1992; S84: 23-31. Couvreur J, Desmonts G, Thulliez P. Prophylaxis of congenital toxoplasmosis. Effects of spiramycin on placental infection. J Antimicrob Chemother 1988; 22: Bl93-200. Couvreur J, Thulliez P, Daffos F, Aufrant C, Bompard Y, Gesguiere A, Desmonts G. Foetopathie toxoplasmique. Traitment in utero par l’association pyrimethamine-sulfa- mides. Arch Fr Pediatr 1991; 48: 397-403. Hohlfeld P, Daffos F, Thulliez P A, et al. Fetal toxoplasmosis: Outcome of pregnancy and infant follow up after in utero treatment. J Pediatr 1989; 115: 765-769. McGee T, Wolters C, Stein L et al. Absence of sensorineural hearing loss in treated infants and children with congenital toxoplasmosis. Otolaryngol Head Neck Surg 1992; 106: 75-80. Wilson JMG, Junger G. Principles and Practice of Screening For Disease. Public Health Papers No. 34. WHO: Geneva 1968. Conyn-van Spaendonck MA. Prevention of Congenital Toxoplasmosis in the Netherlands. Bilthoven: National Institute of Public Health and Environmental Protection 1991. Marteau TM. Psychological costs of screening. BMJ 1989; 299: 527. Peckham CS, Logan S. Screening for toxoplasmosis during pregnancy. Arch Dis Child 1993; 68: 3-5. Henderson JB, Beattie CP, Hale EG, Wright T. The evaluation of new services: Possibilities for preventing congenital toxoplasmosis. Int J Epidemiol 1984; 13: 65-72. Joss AW, Chatterton JM, Ho-Yen DO. Congenital toxoplasmosis: to screen or not to screen? Public Health 1990; 104: 9-20. Desmonts G. Preventing congenital toxoplasmosis. Lancet 1990; 336: 1017-I 018. Multidisciplinary working group. Prenatal Screening for Toxoplasmosis in the UK. Royal College of Obstetricians and Gynaecologists 1992. Edwards PJ, Hall DM. Screening, ethics and the law. BMJ 1992; 305: 267-268. Sackett DL, Holland WW. Controversy in the detection of disease. Lancet 1975; ii: 357-359.




![Countermeasures against Congenital Toxoplasmosis and ... South/Monday...When the Japanese government (or specifically, the Ministry of Health, Labor and Welfare [MHLW]) tries to change](https://img.pdfslide.net/doc/110x75/5ea4f3f2fec58d28874feb7d/countermeasures-against-congenital-toxoplasmosis-and-southmondaywhen-the.jpg)