Embed Size (px)
Citation preview

Correction
MEDICAL SCIENCESCorrection for “Glucagon receptor antibody completely sup-presses type 1 diabetes phenotype without insulin by disrupting anovel diabetogenic pathway,” by May-YunWang, Hai Yan, ZhiqingShi, Matthew R. Evans, Xinxin Yu, Young Lee, Shiuhwei Chen,Annie Williams, Jacques Philippe, Michael G. Roth, and Roger H.Unger, which appeared in issue 8, February 24, 2015, of ProcNatl Acad Sci USA (112:2503–2508; first published February 9,2015; 10.1073/pnas.1424934112).The authors note that on page 2507, left column, after the
second full paragraph, the following paragraph should be added:“Treatment of Alloxan-Induced Diabetic Mice with REMD-477.
For the experiments shown in Fig. 2, 8-wk-old male FVB mice wereinjected IP with 100 mg/kg body weight of alloxan. Diabetic micewith blood glucose >300 mg/dL were then injected subcutaneouslywith buffer (control, n = 5) or buffer containing 5 mg/kg of REMD-477 monoclonal antibody to the glucagon receptor (n = 6), andblood glucose concentration was monitored daily for 8 d.”
www.pnas.org/cgi/doi/10.1073/pnas.1512209112
E4158 | PNAS | July 28, 2015 | vol. 112 | no. 30 www.pnas.org
Dow
nloa
ded
by g
uest
on
July
21,
202
1 D
ownl
oade
d by
gue
st o
n Ju
ly 2
1, 2
021
Dow
nloa
ded
by g
uest
on
July
21,
202
1 D
ownl
oade
d by
gue
st o
n Ju
ly 2
1, 2
021
Dow
nloa
ded
by g
uest
on
July
21,
202
1 D
ownl
oade
d by
gue
st o
n Ju
ly 2
1, 2
021
Dow
nloa
ded
by g
uest
on
July
21,
202
1 D
ownl
oade
d by
gue
st o
n Ju
ly 2
1, 2
021

Glucagon receptor antibody completely suppressestype 1 diabetes phenotype without insulin bydisrupting a novel diabetogenic pathwayMay-Yun Wanga, Hai Yanb,c, Zhiqing Shib,c, Matthew R. Evansd, Xinxin Yua, Young Leea, Shiuhwei Chene,Annie Williamsf, Jacques Philippeg, Michael G. Rothd,1, and Roger H. Ungera,h,1
aTouchstone Diabetes Center, Department of Internal Medicine, University of Texas Southwestern Medical Center, Dallas, TX 75390; bREMD Biotherapeutics,Inc., Camarillo, CA 93012; cBeijing Cosci-REMD Biotherapeutics Inc., Beijing 102206, China; dDepartment of Biochemistry and eDepartment of Cell Biology,University of Texas Southwestern Medical Center, Dallas, TX 75390; fUniversity of Notre Dame, Notre Dame, IN 46556; gUniversity of Geneva School ofMedicine, 1211 Geneva, Switzerland; and hDepartment of Medical Service, Veteran’s Administration North Texas Health Care System, Dallas, TX 75216
Contributed by Roger H. Unger, January 6, 2015 (sent for review November 20, 2014; reviewed by Christopher B. Newgard)
Insulin monotherapy can neither maintain normoglycemia in type1 diabetes (T1D) nor prevent the long-term damage indicated byelevated glycation products in blood, such as glycated hemoglobin(HbA1c). Here we find that hyperglycemia, when unaccompaniedby an acute increase in insulin, enhances itself by paradoxicallystimulating hyperglucagonemia. Raising glucose from 5 to 25 mMwithout insulin enhanced glucagon secretion ∼two- to fivefold inInR1-G9 α cells and ∼18-fold in perfused pancreata from insulin-deficient rats with T1D. Mice with T1D receiving insulin treatmentparadoxically exhibited threefold higher plasma glucagon duringhyperglycemic surges than during normoglycemic intervals. Block-ade of glucagon action with mAb Ac, a glucagon receptor (GCGR)antagonizing antibody, maintained glucose below 100 mg/dL andHbA1c levels below 4% in insulin-deficient mice with T1D. Inrodents with T1D, hyperglycemia stimulates glucagon secretion,up-regulating phosphoenolpyruvate carboxykinase and enhancinghyperglycemia. GCGR antagonism in mice with T1D normalizesglucose and HbA1c, even without insulin.
glucagon receptor | antibody | type 1 diabetes | insulin
Ninety years of insulin treatment in patients with type 1 di-abetes (T1D) have made it clear that insulin alone cannot
normalize glucose homeostasis or glycated hemoglobin (HbA1c)levels. Even optimally controlled patients may exhibit post-prandial surges of glucose levels to three or four times normal (1,2), which may explain why HbA1c levels below 6% are so rare inpatients with T1D. Current thinking attributes these spikes inperipheral plasma glucose to insufficient uptake of incomingdietary glucose by peripheral target tissues as a result of a lack ofinsulin. As a consequence, they are often managed by a pre-prandial bolus of insulin and restriction of dietary carbohydrate.This strategy results in chronic iatrogenic hyperinsulinemia (3) inpatients with “well-controlled” T1D and is responsible for a highincidence of hypoglycemic events, which can be life-threatening.In nondiabetic subjects, a glucose load suppresses glucagon
levels by stimulating an acute transient rise in paracrine insulinfrom β-cells juxtaposed to the glucagon-producing α cells (4–6).This glucagon suppression converts the liver from an organ ofglucose production to an organ of glucose storage (7). In T1D,paracrine insulin is lacking and is replaced by peripherallyinjected insulin. The resulting intraislet insulin concentrationsare but a small fraction of the paracrine concentrations of un-diluted insulin that suppress glucagon in nondiabetic subjects (8,9). In 1974, it was reported that hyperglycemia paradoxicallystimulates glucagon secretion in dogs with chemically induceddiabetes (10). More recently, plasma glucagon concentrationswere reported to rise, with a tripling of hepatic glucose pro-duction, in normal rats continuously infused with glucose ata constant rate (11). Thus, there is evidence that in the absenceof adequate insulin, elevated glucose might stimulate glucagon
production, which in turn aggravates hyperglycemia. In this set-ting, the liver would not be reprogrammed to store incomingglucose but, rather, would continue to produce glucose as if itwere still in the unfed state (12). This may play a major role inpostprandial hyperglycemia (10).Here we find that in T1D, hyperglycemia stimulates, rather
than suppresses, glucagon secretion. This suggests that in T1D,a positive hormonal feedback loop enhances hyperglycemia byadding endogenously produced glucose to diet-derived glucose.If this is an important factor in the hyperglycemic surges thatplague patients with T1D, then suppressing glucagon secretionor blocking glucagon action should eliminate the surges of hy-perglycemia observed in T1D in mice.To measure the normal response of pancreatic islets to ele-
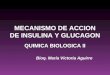
vated glucose, pancreata were isolated from normal mice andperfused with 5 or 25 mM glucose. Glucagon concentrationswere measured in the perfusate. Raising the glucose concentra-tion fivefold decreased glucagon concentration in the perfusateapproximately sixfold (Fig. 1A). To determine the effect of in-creased glucose concentration on glucagon secretion withoutparacrine insulin, we measured glucagon levels in the medium ofcultured InR1-G9 α cells in 5, 10, and 25 mM glucose. The risefrom 5 to 10 mM glucose caused an approximately threefoldincrease in glucagon secretion, and the rise from 10 to 25 mMcaused another twofold rise (Fig. 1B). Because cultured cells may
Significance
Subcutaneous injections of insulin sustain life in mammalsunable to produce insulin (type 1 diabetes) but do not preventhyperglycemic and hypoglycemic swings or decrease hemo-globin A1c levels to normal amounts. In mice treated with in-sulin alone, repeated episodes of transient elevated bloodglucose cause long-term damage. We show that in mice withtype 1 diabetes treated with insulin, the transient high bloodglucose levels require production of glucagon, a hormone thatwill cause the liver to produce more glucose. Blocking the ac-tion of glucagon with an antibody to the glucagon receptorcompletely normalizes blood glucose and hemoglobin A1c inthe complete absence of insulin therapy. Suppressing glucagonaction in combination with low-dose insulin would be a supe-rior treatment for type 1 diabetes.
Author contributions: H.Y., M.G.R., and R.H.U. designed research; M.-Y.W., Z.S., M.R.E., X.Y.,Y.L., S.C., and A.W. performed research; J.P. contributed new reagents/analytic tools;M.-Y.W., H.Y., M.R.E., X.Y., M.G.R., and R.H.U. analyzed data; and Z.S., M.G.R., and R.H.U.wrote the paper.
Reviewers: C.B.N., Duke University Medical Center.
The authors declare no conflict of interest.1To whom correspondence may be addressed. Email: [email protected] [email protected].
www.pnas.org/cgi/doi/10.1073/pnas.1424934112 PNAS | February 24, 2015 | vol. 112 | no. 8 | 2503–2508
MED
ICALSC
IENCE
S

not reflect the behavior of native α cells in situ in T1D, we iso-lated pancreata from streptozotocin-induced insulin-deficientT1D rats and perfused them with 5, 10, and 25 mM glucoseconcentrations. When the perfusate glucose was increased from5 to 10 mM, glucagon secretion increased fourfold (Fig. 1C). Anincrease in glucose from 10 to 25 mM increased glucagon se-cretion another fourfold. Insulin concentrations in all of theseperfusates were below the detection limit of a radioimmune as-say (RIA) (EMD Millipore). Previously, we reported that thestreptozotocin treatment protocol we used resulted in the de-struction of 93.4% of β cells (13).The fact that elevations of glucose stimulated glucagon se-
cretion in the absence of an acute paracrine insulin releasesuggested that in animals with T1D, any rise in glucose wouldstimulate glucagon secretion and give rise to a cycle of self-enhancinghyperglycemia (3, 14). To investigate the possibility of such a
diabetogenic pathway, we compared plasma glucagon levels ininsulin-treated NOD/ShiLtJ T1D mice during and between hy-perglycemic surges (Fig. 1D). The mice were treated with 0.1 ULevemir twice daily, and blood glucose was measured in themorning 17 h after an insulin injection (high blood glucose) and inthe afternoon 7 h after an insulin injection (low blood glucose)(Fig. 1E). In mice receiving this insulin regimen, glucagon averaged138 ± 41 pg/mL and insulin 3.9 ± 1.1 ng/mL in samples in whichglucose averaged 500 ± 37 mg/dL This glucagon concentration wassignificantly higher (P < 0.05) than the mean glucagon level of 55 ±35 pg/mL, measured in samples from the same mice when theirglucose levels averaged 130 ± 71 mg/dL and insulin averaged14.3 ± 4.5 ng/mL These findings are consistent with a glucagon-mediated contribution to the surges of hyperglycemia.To assess directly the effect on the liver of the hyper-
glucagonemia accompanying hyperglycemia in the absence of
A B
C D
E
Fig. 1. In the absence of paracrine insulin, glucagon secretion increases in response to increases in glucose. (A) An increase from 5 to 25 mM in the glucoseperfused into the isolated pancreata of nondiabetic mice causes profound suppression of glucagon secretion. n = 3. (B) In the absence of insulin, increasingglucose concentration progressively increases glucagon secretion by cultured InR1G9 α cells. n = 4. (C) Perfusing increasing glucose concentrations intopancreata of rats with streptozotocin-induced destruction of β cells causes progressive rise in glucagon secretion. n = 6. (D) Glucagon was measured in plasmacollected twice daily (10:00 AM and 5:00 PM) from insulin-treated (0.1 U bid) mice with T1D. The average glucagon concentration, when blood glucose levelsaveraged 500 mg/dL (black bar) and when glucose levels averaged 130 mg/dL (white bar), are shown. The results are from 112 specimens collected from eightdifferent mice. (E) The mean glucose measurements taken each day that were used to classify samples as high glucose or low glucose for D are presented.Error bars are SDs.
2504 | www.pnas.org/cgi/doi/10.1073/pnas.1424934112 Wang et al.

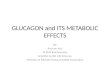
endogenous insulin, we compared activation of key markers ofglucagon action in liver. The phosphorylation of cAMP responseelement binding protein (CREB), a transducer of the glucagonsignal, and the expression of a gluconeogenic glucagon target,phosphoenolpyruvate carboxykinase (PEPCK), were measuredin T1D and nondiabetic mice. Compared with nondiabetic liver,there was a 3.5-fold elevation in phosphorylated CREB and a2.5-fold increase in PEPCK expression in T1D livers (Fig. 2 A–C).To demonstrate that these differences were glucagon-mediated, wetreated T1D mice with a single injection of 5 mg/kg mAb B (15),a fully human, antiglucagon receptor (GCGR) antibody drug can-didate under development by REMD Biotherapeutics, Inc. (15–17).In mice treated with the monoclonal antibody mAb B, daily 10:00AM blood glucose measurements averaged 85 ± 5 mg/dL andremained normoglycemic for 8 d (Fig. 2D), at which time liverswere harvested. In the mAb B-treated T1D livers, phosphorylatedCREB protein was reduced to nondiabetic levels and PEPCKprotein expression was reduced below that of nondiabetic mice (Fig.2 A–C). Thus, the activation of hepatic gluconeogenesis in T1Dmice was a result of their hyperglucagonemia and disappearedwhen glucagon actions were blocked.If self-enhancing action of hyperglycemia is mediated by
glucose-stimulated increase in glucagon in T1D, it follows thatsuppressing glucagon secretion should eliminate or reduce theproblem. To test this, we placed T1D mice on a low dose ofinsulin (0.01 U twice daily) and then began continuous s.c.infusions of four peptides known to suppress glucagon directlyor indirectly (18–22). A fifth, nonpeptidic suppressor (23),GABA, was given mixed in the chow. Each of the five reagentslowered glucagon levels, and in each case, this was accompa-nied by reduction of hyperglycemia from >600 mg/dL to 160 ±75 mg/dL (P < 0.001; Fig. 3A). The average insulin concen-trations in these samples were not correlated with either glu-cagon or glucose concentrations. With the exception of leptin,which reduced food intake by 50% compared with diabeticanimals receiving insulin monotherapy, none of these glucagonsuppressors caused a significant reduction in food intake.If the glucose-lowering effects of glucagon suppressors re-
sulted entirely from reduced glucagon secretion, rather thanfrom off-target actions, therapy with a GCGR antibody shouldcause as dramatic an improvement as the glucagon-suppressingagents. Mice with chemically (streptozotocin)-induced T1Dand a starting hyperglycemia of ∼325 ± 72 mg/dL were injectedi.p. once each week with 7.5 mg/kg anti-GCGR antibody mAbAc (15) (Fig. 3B), and blood glucose was measured weekly for12 wk. Blood glucose concentrations returned to normal (∼90mg/dL) in the mice treated with the antibody 1 wk after a singledose (first time point), and this normalization continued for theduration of treatment. Body weight did not change significantlybetween the control and antibody-treated groups of mice fromthe start to finish of the experiment. In the vehicle-treatedcontrol mice, blood glucose levels rose to 540 ± 70 mg/dLduring the 12-wk study. At the end of this treatment, HbA1cwas measured as an indication of chronic hyperglycemia. In themice treated with mAb Ac, HbA1c levels were normal (4 ±1%), whereas in the control mice, HbA1c averaged 11 ± 1%(Fig. 3C). GLP-1 averaged 3.64 ± 0.9 pmol/L in the controlmice and 3.63 ± 0.52 pmol/L in the mice treated with antibody.By immunohistochemistry, the ratio of insulin-positive cells toglucagon-positive cells in islets observed in sections of pancreastaken from five control mice at the end of the study was 0.15, andusing cells from five antibody treated mice, the ratio was 0.16.Because the ratio of β cells to α cells in wild-type mice is ∼6.0(24), the ratios observed are those expected for severe ablation ofβ cells by streptozotocin. The fact that the ratio did not changebetween the two groups of animals indicates that the antibodytreatment did not induce α-cell hyperplasia in this experiment.
DiscussionThe present report provides the first evidence to our knowledgethat acquired ablation, similar to congenital ablation of glucagonaction, completely prevents the hyperglycemia and elevatedHbA1c of T1D. Our work further supports the essential role of
Fig. 2. Glucagon action is chronically high in the livers of diabetic animals.(A) Hepatic markers of glucagon signaling (P-CREB) and of glucagon action(PEPCK) were measured by immunoblotting liver samples from nondiabeticand diabetic mice. (B) The ratio of activated P-CREB to total CREB proteinwas measured by densitometry of immunoblots of livers from nondiabeticmice (n = 2), untreated T1D mice (n = 3), and T1D mice (n = 4) treated with5 mg antiglucagon receptor antibody mAb B. (C) Similar measurements weremade of PEPCK protein in these specimens. (D) Blood glucose levels areplotted for T1D mice treated with buffer (n = 5) or 5 mg/kg anti-GCGRantibody mAb B (n = 6) for the time shown. Error bars in B–D are SDs.
Wang et al. PNAS | February 24, 2015 | vol. 112 | no. 8 | 2505
MED
ICALSC
IENCE
S

glucagon in the pathophysiology of diabetes, as was first proposedin 1975 (25). Subsequently, it was supported by demonstrationsthat diabetes was ameliorated by every glucagon suppressor usedin every species tested. This included human T1D (26). Similarly,glucagon receptor antibodies have been shown to lower hyper-glycemia in T2D (15), but this is the first demonstration, to ourknowledge, of normalization of glycemia and HbA1c in complete
insulin deficiency, a result that, to our knowledge, has never beenachieved with existing therapies. Previous neutralization of glu-cagon itself reduced, but did not normalize, blood glucose levels(27–29). Synthetic glucagon receptor antagonists (30–33) simi-larly improved the diabetes but did not normalize it.Despite the abundance of scientific support for glucagon’s
central role in the disease, plus the calculation by Cahill thatwithout glucagon the liver was incapable of producing hypergly-cemia, the idea has persisted that insufficient insulin action,rather than excess glucagon action, causes diabetes. However,during the 9 decades of insulin therapy, it has become evidentthat correcting the deficit in insulin action cannot restore glucosehomeostasis or HbA1c levels to normal, despite the hyper-insulinemia it induces. Incontrovertible evidence of glucagon es-sentiality to diabetes was recently reported in congenital glucagonreceptor-null mice in which total insulin deficiency failed to raiseblood glucose or glucose tolerance above normal (13). Now, inthe present study, we show in genetically normal rodents thatacquired loss of glucagon action caused by glucagon receptorimmunoneutralization also prevents and reverses T1 diabetes.This study also proposes a novel self-enhancing pathophysio-
logic pathway to severe hyperglycemia. In 1971, it was reportedthat without glucagon action, the liver cannot produce enoughglucose to sustain hyperglycemia in insulin-deficient T1D mice.Here we present evidence for progressive enhancement of hy-perglycemia by glucose-stimulated glucagon secretion that occurswhen a blood glucose rise is unaccompanied by a physiologic risein paracrine insulin. The anti-GCGR mAb Ac maintained nor-moglycemia and normalized HbA1c in severely insulin-deficientmice with impending diabetic ketoacidosis. Most remarkably,A1c normalization was achieved without inducing iatrogenichyperinsulinemia (3), which may result in excess cardiovascularmortality (34). The antibody without any concomitant insulinadministration completely prevented the T1D phenotype.Thus, the metabolic phenotype of T1D can be eradicated by
blocking glucagon action on the liver. The fact that the foregoingresults were obtained in rodents raises the question of speciesdifferences from humans. Earlier work from our laboratory showedin human T1D that suppression of glucagon secretion with so-matostatin eliminated postprandial hyperglycemic surges (26). Thisis evidence that the concept of antagonizing glucagon action as aneffective therapy for diabetes will apply to humans. In any event,the approach of antagonizing the glucagon receptor for therapy indiabetes will need to be validated in human clinical studies.Taken together, this suggests that insulin replacement therapy
alone, without glucagon suppression by an agent other thaninsulin, is an incomplete strategy for regulating T1D. A morerational approach would be to first lower the unphysiologicallyhigh insulin doses now in common use (3) to doses that do notproduce peripheral hyperinsulinemia and hypoglycemia. Thislowering of insulin would increase glucagon and blood glucoselevels, but both could be reduced by a glucagon-suppressing agentor by an anti-GCGR antibody, such as mAb B and mAb Ac.
MethodsEffect of Glucose on Glucagon Secretion by InR1-G9 Cells. For the experimentsshown in Fig. 1, InR1-G9 (35, 36) cells, obtained from J.P., were cultured at37 °C in a humidified 5% (vol/vol) CO2 incubator in DMEM (high glucose) media,containing 10% (vol/vol) FBS, 50 U/mL penicillin, 50 mg/mL streptomycin,and 1 mmol/L sodium pyruvate, without insulin. Cells harvested from cul-tures lower than passage 25 were used. Cells were seeded into a 384-wellculture plate at a density of 10,000 cells per well in a volume of 30 μL. Aftera 2 h incubation to allow the cells to attach to the plate, the medium wasreplaced with the desired concentration (5, 10, or 25 mmol/L) of glucose,and the cells were grown for 20 h at 37 °C. Five μL of a 1:1,000 dilution (inPBS) of a rabbit antiglucagon antibody was added to each well and in-cubated for 30 min. Next, 5 μL of 20 μg/mL (2 μg/mL final concentration) ofAlphaLisa protein A conjugated acceptor beads (PerkinElmer) was added toeach well and allowed to incubate for an additional 30 min. After incubation,
A
B
C
Fig. 3. Agents that suppress glucagon secretion or antagonize GCGR nor-malize glucagon action in liver and plasma glucose in diabetic mice. (A)Plasma glucose and glucagon levels in diabetic NOD mice (n= 3–10) treatedwith the agents shown. (B) Blood glucose levels are plotted for chemicallyinduced T1D mice treated with buffer (n = 10) or 7.5 mg/kg mAb Ac anti-GCGR antibody (n = 10) for the time shown. P < 0.01 comparing antibody tovehicle for all measurements from weeks 1–12. (C) HbA1c was measured,with a Toshiba TBA-40FR automated biochemical analyzer, in blood from theanimals shown in B after 12 wk; average values are graphed. P < 0.01comparing antibody to vehicle. Error bars are SDs.
2506 | www.pnas.org/cgi/doi/10.1073/pnas.1424934112 Wang et al.

a 1 nmol/L final concentration of biotinylated-glucagon (Anaspec; catalognumber 60274-1) was added to each well and incubated for 60 min. Last,streptavidin-conjugated AlphaLisa donor beads were added to a final con-centration of 8 μg beads/mL to give a final sample volume of 50 μL. Themixture was incubated at room temperature for 2 h. All additions andincubations were made in subdued lighting conditions according to themanufacturer’s instructions. The assay was measured on an Envision platereader (PerkinElmer), and triplicate values were averaged.
Perfusion of Pancreata. To determine the effects of high glucose on glucagonsecretion by intact α cells in islets of rodents with T1D, six lean wild-typeZucker rats were treated twice with 100 mg streptozotocin 1 wk apart toinduce severe T1D. Insulin in blood collected from animals treated with twodoses of streptozotocin was undetectable by RIA. Seven days after the sec-ond dose of streptozotocin, they were fasted for 17 h and then anesthetizedwith 60 mg/kg body weight of sodium pentobarbital administered in-traperitoneally. The pancreas was isolated and perfused in situ at 37 °C. Theperfusate contained 1× KRB buffer (129 mmol/L NaCl, 4.8 mmol/L KCl,0.2 mmol/L CaCl2, 1 mmol/L KH2PO4, 1 mmol/L MgSO4, 5 mmol/L NaHCO3)plus D-glucose at 5, 10, or 25 mmol/L concentration. Perfusates were sup-plemented with 0.5% (wt/vol) bovine albumin fraction V and gassed for30 min with 95% (vol/vol) O2 and 5% (vol/vol) CO2 at 37 °C. Perfusate flowrate was maintained at 4 mL/min. After a 10-min equilibration period with5 mmol/L D-glucose, glucose was increased to 10 mmol/L for 10 min and to25 mmol/L for another 10 min. The temperature was kept constant at 37 °C.The effluent samples were collected from the portal vein, without recycling,into prechilled tubes containing 25 mmol/L EDTA and aprotinin, and frozenat −20 °C for later use. The concentrations of glucagon and insulin weremeasured by RIA (catalog numbers GL-32K and RI-13K; EMD Millipore),according to the manufacturer’s instructions. For measurements on normalrodents, pancreata from C57BL/6N mice from Charles River Laboratories In-ternational were perfused by the protocol described here for rats.
Glucagon Suppression in Vivo in Mice with T1D. Eight-week-old NOD (NOD/ShiLtJ) female mice from the Jackson Laboratory that had developed di-abetes were assigned to one of three groups: insulin monotherapy (0.1 Utwice daily at 10:00 AM and 5:00 PM), reduced insulin monotherapy (0.01 Utwice daily at 10:00 AM and 5:00 PM), and reduced insulin therapy plusa glucagon suppressor. Miniosmotic pumps (ALZET model 2001; ALZET Os-motic Pumps) were implanted between the scapulae under ketamine/xylazine anesthesia (0.1 mL per 20–30 g body weight). The pumps deliveredagents at a rate of 1 μL/h during a 7-d period and were replaced every 7 d.They were loaded with various known or suspected glucagon suppressors,including recombinant leptin at 20 mg/mL (Amylin Pharmaceuticals, Inc.),pramlintide acetate at 1 g/mL (Amylin Pharmaceuticals, Inc.), 6 mg/mLliraglutide (Novo Nordisk A/S), 250 mg/mL exenatide (Amylin Pharmaceuticals,Inc.). An untreated control group received PBS delivered by Alzet pump,plus twice daily s.c. injections of 0.01 U of the long-acting insulin analog(Levemir U-100; Novo Nordisk) administered at 10:00 AM and 5:00 PM. Anadditional group of mice received 0.01 U Levemir injected twice daily plusthe orally effective (23) glucagon suppressor GABA (catalog numberA-2129; Sigma) mixed with the powdered food [4% (wt/wt) fat]. Food in-take, body weight, and blood glucose were monitored daily. Blood sampleswere obtained at 10:00 AM, 1:00 PM, and 5:00 PM. Insulin was administeredtwice daily at 10:00 AM and 5:00 PM, after obtaining the blood glucosespecimen. For all animal experiments, principles of laboratory animal care(NIH publication no. 85–23, revised 1985) were followed according to pro-tocols reviewed and approved by the University of Texas SouthwesternMedical Center Institutional Animal Care and Use Committee.
Treatment of NOD Mice with Monoclonal Antiglucagon Receptor Antibodies.The two monoclonal antibodies used differ by only one amino acid not in-volved in glucagon binding and have equivalent affinities for glucagon (15).Diabetic NOD mice were injected s.c. with buffer (control, n = 5) or buffercontaining 5 mg/kg mAb B monoclonal antibody to the GCGR (n = 6), andblood glucose concentration was monitored daily for 8 d. Male Balb/C miceat 8–10 wk of age were injected IP with 60 mg/kg streptozotocin daily for 5consecutive days, and after 14 d, were injected with vehicle (control = 10) or7.5 mg/kg mAb Ac (n = 10) weekly for 12 wk. Fasting blood glucose levelswere measured weekly. After 12 wk, blood HgA1c was measured in freshwhole blood with a Toshiba TBA-40FR auto-analyzer.
Plasma Measurements. Blood samples (100 μL) were collected in tubes con-taining 0.15 TIU/mL aprotinin and 10 mmol/L EDTA. Samples were centri-fuged, and aliquots of plasma were frozen at −20 °C. Plasma glucagon wasmeasured using a rodent glucagon RIA kit (Linco Research). Mouse plasmainsulin was measured by an ELISA kit (Crystal Chem, Inc.).
Immunoblotting Analysis. Total protein extracts prepared from liver tissues ofNOD mice with or without the treatment of glucagon suppressors wereresolved by SDS/PAGE and transferred to a nitrocellulose membrane (Bio-RadLaboratories). The blotted membrane was blocked in 1× Tris-buffered saline(TBS) containing 0.1% Tween and 5% (wt/vol) nonfat dry milk (TBST-MLK)for 1 h at room temperature with gentle, constant agitation. After in-cubation with primary antibodies anti-phospho-CREB, anti-CREB, or anti-PEPCK (Cell Signaling Technologies), or anti-γ-tubulin (Sigma) in freshlyprepared TBST-MLK at 4 °C overnight with agitation, the membrane waswashed two times with TBST buffer. This was followed by incubating withsecondary anti-rabbit or mouse horseradish peroxidase-conjugated Ig anti-bodies in TBST-MLK for 1 h at room temperature with agitation. Themembrane was then washed three times with TBST buffer, and the proteinsof interest on immunoblots were detected by an ECL plus Western blottingdetection system (GE Healthcare Life Sciences). The corresponding bandswere quantified using NIH Image software (version 1.6; available at rsb.info.nih.gov/nih-image).
Histochemistry. The pancreas was removed from five control and five testanimals at the end of the experiment shown in Fig. 3B and fixed in 4% (vol/vol)formaldehyde overnight, then embedded in paraffin, and each entirepancreas was sectioned. Paraffin was removed from the sections with xy-lene, and the sections were rehydrated through a graded series of alcohol inwater. Sections were treated with 3% (vol/vol) H2O2 for 10 min to blockendogenous peroxidase activity, and in 10% (vol/vol) goat serum for 30 minto block nonspecific antibody binding. Sections were then incubated se-quentially with rabbit anti-glucagon antibody (Abcam, ab18461) and bio-tinylated goat anti-rabbit IgG (Abcam, ab97049) and detected with ABC-HRPKit (Vector Laboratories, pk-4100) and DAB peroxidase substrate kit (VectorLaboratories, sk-4100), according to the manufacturer’s instructions. Sec-tions were then incubated with guinea pig antiinsulin antibody (Abcam,ab7842) and biotinylated goat anti-guinea pig IgG (Abcam, ab6907), and theantibody was detected with ABC-AP Kit (Vector Laboratories, ak-5000) andRed Alkaline Phosphatase Substrate Kit III (Vector Laboratories, sk-5100).Sections were counterstained with hematoxylin for 15 s, rinsed in water, anddehydrated through graded solutions from 70% (vol/vol) to 100% ethanoland then into 100% xylene. Sections were mounted in Permount (Fisher,SP15-100), dried, and observed by microscopy. Pancreatic islets in pancreassections were captured at a magnification of 200×, and the positive labeledcells in all islets were evaluated. The total area containing insulin-positiveand glucagon-positive cells (islet) was measured, as was the area of in-dividual cells stained with each marker within each islet. Dividing the area ofpositive cells for insulin or glucagon by the total area per islet ×100% givesthe percentage of each cell type in each islet.
Statistical Analysis. Results are presented as mean ± SEM and were evaluatedby Student’s t test for two groups or by ANOVA. For histochemistry, one-wayANOVA testing (SPSS 17.0) was applied among the groups; P < 0.05 wasaccepted as significant.
ACKNOWLEDGMENTS. We acknowledge the help of Dr. Jaime Davison andMs. Kay McCorkle with these studies. We also appreciate the support ofREMD Biotherapeutics, Inc., which provided a research grant and the fullyhuman anti-GCGR antibodies mAb Ac and mAb B, under a Sponsored Re-search Agreement in June 2014 between REMD Biotherapeutics, Inc., andthe University of Texas Southwestern Medical Center. This research was alsofunded in part by the Veterans Affairs North Texas Health Care System,Dallas, Texas, by a grant from Bristol-Myer Squibb (to R.H.U.), and by theDiane and Hal Brierley Chair in Biomedical Research (M.G.R.). R.H.U. andM.G.R. are founding partners of SynAlpha Therapeutics, LLC. Part of thework was conducted in a facility supported by Grant C06-RR15437 fromthe National Center for Research Resources (to M.G.R.). The streptozotocin-diabetic mouse study was conducted by Pharmaron in Beijing under a servicecontract with REMD Biotherapeutics, Inc.
1. Derr R, Garrett E, Stacy GA, Saudek CD (2003) Is HbA(1c) affected by glycemic in-
stability? Diabetes Care 26(10):2728–2733.
2. Kozawa J, et al. (2013) Early postprandial glucagon surge affects postprandial glucose
levels in obese and non-obese patients with type 2 diabetes. Endocr J 60(6):813–818.
Wang et al. PNAS | February 24, 2015 | vol. 112 | no. 8 | 2507
MED
ICALSC
IENCE
S

3. Wang M-Y, et al. (2013) Iatrogenic hyperinsulinemia in type 1 diabetes: Its effect onatherogenic risk markers. J Diabetes Complications 27(1):70–74.
4. Maruyama H, Hisatomi A, Orci L, Grodsky GM, Unger RH (1984) Insulin within islets isa physiologic glucagon release inhibitor. J Clin Invest 74(6):2296–2299.
5. Müller WA, Faloona GR, Unger RH (1971) The effect of experimental insulin deficiencyon glucagon secretion. J Clin Invest 50(9):1992–1999.
6. Unger RH, Orci L (2010) Paracrinology of islets and the paracrinopathy of diabetes.Proc Natl Acad Sci USA 107(37):16009–16012.
7. Moore MC, Coate KC, Winnick JJ, An Z, Cherrington AD (2012) Regulation of hepaticglucose uptake and storage in vivo. Adv Nutr 3(3):286–294.
8. Unger RH, Cherrington AD (2012) Glucagonocentric restructuring of diabetes: Apathophysiologic and therapeutic makeover. J Clin Invest 122(1):4–12.
9. Unger RH, Roth MG (2015) A New Biology of Diabetes Revealed by Leptin. Cell Metab21(1):15–20.
10. Braaten JT, Faloona GR, Unger RH (1974) The effect of insulin on the alpha-cell re-sponse to hyperglycemia in long-standing alloxan diabetes. J Clin Invest 53(4):1017–1021.
11. Jamison RA, et al. (2011) Hyperglucagonemia precedes a decline in insulin secretionand causes hyperglycemia in chronically glucose-infused rats. Am J Physiol EndocrinolMetab 301(6):E1174–E1183.
12. Cherrington AD, Lacy WW, Chiasson JL (1978) Effect of glucagon on glucose pro-duction during insulin deficiency in the dog. J Clin Invest 62(3):664–677.
13. Lee Y, Wang MY, Du XQ, Charron MJ, Unger RH (2011) Glucagon receptor knockoutprevents insulin-deficient type 1 diabetes in mice. Diabetes 60(2):391–397.
14. Wang MY, et al. (2010) Leptin therapy in insulin-deficient type I diabetes. Proc NatlAcad Sci USA 107(11):4813–4819.
15. Yan H, et al. (2009) Fully human monoclonal antibodies antagonizing the glucagonreceptor improve glucose homeostasis in mice and monkeys. J Pharmacol Exp Ther329(1):102–111.
16. Gu W, et al. (2010) Glucagon receptor antagonist-mediated improvements in glyce-mic control are dependent on functional pancreatic GLP-1 receptor. Am J PhysiolEndocrinol Metab 299(4):E624–E632.
17. Gu W, et al. (2009) Long-term inhibition of the glucagon receptor with a monoclonalantibody in mice causes sustained improvement in glycemic control, with reversiblealpha-cell hyperplasia and hyperglucagonemia. J Pharmacol Exp Ther 331(3):871–881.
18. Fineman MS, et al. (2002) The human amylin analog, pramlintide, corrects postprandialhyperglucagonemia in patients with type 1 diabetes. Metabolism 51(5):636–641.
19. Nielsen LL, Young AA, Parkes DG (2004) Pharmacology of exenatide (synthetic ex-endin-4): A potential therapeutic for improved glycemic control of type 2 diabetes.Regul Pept 117(2):77–88.
20. Nauck MA, Meier JJ (2005) Glucagon-like peptide 1 and its derivatives in the treat-
ment of diabetes. Regul Pept 128(2):135–148.21. Berglund ED, et al. (2009) Fibroblast growth factor 21 controls glycemia via regulation
of hepatic glucose flux and insulin sensitivity. Endocrinology 150(9):4084–4093.22. Kharitonenkov A, et al. (2007) The metabolic state of diabetic monkeys is regulated
by fibroblast growth factor-21. Endocrinology 148(2):774–781.23. Xu E, et al. (2006) Intra-islet insulin suppresses glucagon release via GABA-GABAA
receptor system. Cell Metab 3(1):47–58.24. Kim A, et al. (2009) Islet architecture: A comparative study. Islets 1(2):129–136.25. Unger RH, Orci L (1975) The essential role of glucagon in the pathogenesis of diabetes
mellitus. Lancet 1(7897):14–16.26. Raskin P, Unger RH (1978) Hyperglucagonemia and its suppression. Importance in the
metabolic control of diabetes. N Engl J Med 299(9):433–436.27. Brand CL, et al. (1994) Immunoneutralization of endogenous glucagon with mono-
clonal glucagon antibody normalizes hyperglycaemia in moderately streptozotocin-
diabetic rats. Diabetologia 37(10):985–993.28. Sørensen H, et al. (2006) Immunoneutralization of endogenous glucagon reduces
hepatic glucose output and improves long-term glycemic control in diabetic ob/ob
mice. Diabetes 55(10):2843–2848.29. Vater A, et al. (2013) A mixed mirror-image DNA/RNA aptamer inhibits glucagon and
acutely improves glucose tolerance in models of type 1 and type 2 diabetes. J Biol
Chem 288(29):21136–21147.30. Mu J, et al. (2011) Chronic treatment with a glucagon receptor antagonist lowers
glucose and moderately raises circulating glucagon and glucagon-like peptide 1
without severe alpha cell hypertrophy in diet-induced obese mice. Diabetologia 54(9):
2381–2391.31. Mu J, et al. (2012) Anti-diabetic efficacy and impact on amino acid metabolism of
GRA1, a novel small-molecule glucagon receptor antagonist. PLoS ONE 7(11):e49572.32. Shen DM, et al. (2005) Discovery of novel, potent, and orally active spiro-urea human
glucagon receptor antagonists. Bioorg Med Chem Lett 15(20):4564–4569.33. Winzell MS, et al. (2007) Glucagon receptor antagonism improves islet function in
mice with insulin resistance induced by a high-fat diet. Diabetologia 50(7):1453–1462.34. Lind M, et al. (2014) Glycemic control and excess mortality in type 1 diabetes. N Engl J
Med 371(21):1972–1982.35. Takaki R, et al. (1986) Isolation of glucagon-secreting cell lines by cloning insulinoma
cells. In Vitro Cell Dev Biol 22(3 Pt 1):120–126.36. Drucker DJ, Philippe J, Mojsov S (1988) Proglucagon gene expression and post-
translational processing in a hamster islet cell line. Endocrinology 123(4):1861–1867.
2508 | www.pnas.org/cgi/doi/10.1073/pnas.1424934112 Wang et al.