Embed Size (px)
Citation preview
IMPORTANT: Please see the Notice on the back ofthe front cover of this plan material concerningstudent health insurance coverage.
Policy Number: 2013-202513-1
STUDENTINJURY AND SICKNESS
INSURANCE PLAN2013-2014

TABLE OF CONTENTS
Student Health Insurance Office Letter . . . . . . . . . . . . 1Non-Discrimination Policy . . . . . . . . . . . . . . . . . . . . . . 2Student Injury and Sickness Insurance Plan . . . . . . . . 2Eligibility . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2-3Coverage Dates and Costs . . . . . . . . . . . . . . . . . . . 3-4Enrollment Process . . . . . . . . . . . . . . . . . . . . . . . . . . . 4Dependent Coverage. . . . . . . . . . . . . . . . . . . . . . . . . . 5Late Enrollment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5Confirmation of Coverage for Particular Services . . . 6-7Summary of Benefits . . . . . . . . . . . . . . . . . . . . . . . . . . 8Policy Year Deductibles . . . . . . . . . . . . . . . . . . . . . . . . 8Out-of-Pocket Maximum . . . . . . . . . . . . . . . . . . . . . . . 8Prescription Drug Plan – Express Scripts . . . . . . . . 9-10Prescription Drug Plan – Health Center at Auraria. . . . 10Pre-Existing Conditions . . . . . . . . . . . . . . . . . . . . . . . 10Right of Reimbursement. . . . . . . . . . . . . . . . . . . . 10-11Maximum Benefit. . . . . . . . . . . . . . . . . . . . . . . . . . . . 11General Plan Provisions . . . . . . . . . . . . . . . . . . . . . . . 11Covered Medical Expenses. . . . . . . . . . . . 11-20, 25-27Schedule of Benefits . . . . . . . . . . . . . . . . . . . . . . . 21-24Exclusions and Limitations . . . . . . . . . . . . . . . . . . 28-31Pre-Existing Conditions. . . . . . . . . . . . . . . . . . . . . . . . 31Important Notice. . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31Creditable Coverage . . . . . . . . . . . . . . . . . . . . . . . . . . 32Extension of Benefits . . . . . . . . . . . . . . . . . . . . . . . . . 32Continuation of Coverage . . . . . . . . . . . . . . . . . . . . . . 32Coordination of Benefits . . . . . . . . . . . . . . . . . . . . . . . 33Definitions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33-36Claim Submissions Requirements/Proof of LossDeadlines . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 37
Notice of Appeal Rights. . . . . . . . . . . . . . . . . . . . . 37-40Privacy Policy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 40FrontierMEDEX: Global Emergency Service . . . . . . 41-42Accidental Death and Dismemberment Benefits . . . . . 42Claim Procedures . . . . . . . . . . . . . . . . . . . . . . . . . . . . 43Claims, Eligibility and Benefits Questions . . . . . . . . . . 43Participating Provider Organization . . . . . . . . . . . . . . . 43Health Care Management Program. . . . . . . . . . . . . . . 43Insurance Company . . . . . . . . . . . . . . . . . . . . . . . . . . 43
Notice Regarding Your Student HealthInsurance Coverage
Your student health insurance coverage,offered by UnitedHealthcare InsuranceCompany, may not meet the minimumstandards required by the health carereform law for restrictions on annualdollar limits. The annual dollar limitsensure that consumers have sufficientaccess to medical benefits throughout theannual term of the policy. Restrictions forannual dollar limits for group andindividual health insurance coverage are$1.25 million for policy years beforeSeptember 23, 2012; and $2 million forpolicy years beginning on or afterSeptember 23, 2012 but before January 1,2014. Restrictions on annual dollar limitsfor student health insurance coverage are$100,000 for policy years before September23, 2012 and $500,000 for policy yearsbeginning on or after September 23, 2012but before January 1, 2014. Your studenthealth insurance coverage puts a policyyear limit of $500,000 that applies to theessential benefits provided in the Scheduleof Benefits unless otherwise specified. Ifyou have any questions or concerns aboutthis notice, contact Customer Service at1-800-767-0700. Be advised that you maybe eligible for coverage under a grouphealth plan of a parent’s employer orunder a parent’s individual healthinsurance policy if you are under the ageof 26. Contact the plan administrator ofthe parent’s employer plan or the parent’sindividual health insurance issuer for moreinformation.

Page 2
Dear Student,
The University of Colorado Denver, Downtown Campus(DC) strongly encourages all students to have healthinsurance coverage. This will help insure success in theacademic community even in the event of an unexpectedmedical expense. The University highly recommends thatyou consider this health program to help protect yourselfagainst unexpected health emergencies which mightarise. Without adequate medical protection your ability tomaintain good health and meet education expensescould be seriously jeopardized. If you are not currentlycovered by other medical insurance at an adequate level,we urge you to take advantage of this opportunity topurchase medical protection at a very reasonable cost.The Student Injury and Sickness Insurance Plan isdesigned to coordinate with the Health Center at Aurariato assure the availability of quality health care at thelowest possible cost. The endorsed plan made availableby the University of Colorado Denver, DowntownCampus Student Injury and Sickness Insurance Plan isdescribed in this brochure. Be sure to read the Scheduleof Benefits as well as the Exclusions and Limitationssections of this brochure. Coverage is voluntary and youmust enroll in every coverage period that you wantcoverage (your coverage does not automatically renewafter the semester in which you were enrolled). It is veryimportant to know what the Policy does and does notcover. If you have any questions about this plan, pleasecontact AmeriBen at 855-539-8678. We look forward toassisting you in maintaining good health while youachieve your educational goals.
Sincerely,Student Insurance Office
Tivoli 127303-556-6273
Page 1
NON-DISCRIMINATION POLICY
The University of Colorado Denver, Downtown Campusdoes not discriminate on the basis of race, color, nationalorigin, sex, age, disability, creed, religion, sexualorientation, or veteran status in admission and access to,and treatment and employment in, its educationalprograms and activities.
The University of Colorado Denver, Downtown Campustakes action to increase ethnic, cultural, and genderdiversity, to employ qualified disabled individuals, and toprovide equal opportunity to all students and employees.
The University of Colorado Denver, Downtown Campuscomplies with all local, state, and federal laws andregulations related to education, employment andcontracting.
STUDENT INJURY AND SICKNESSINSURANCE PLAN
This brochure is designed to acquaint students and otherinterested parties with the medical services available, costof the plan and exclusions to the services offered. We askthat you read it carefully so that you will know the extentof medical services and insurance benefits you canexpect.
The insurance plan is entirely supported by studentpremiums, no tuition or State appropriations are used topay for these services.
The insurance becomes effective for a student asprovided in the Master Policy and explained in thisbooklet.
ELIGIBILITY
Domestic undergraduate students taking 6 or more credithours and graduate students enrolled in a degree-seekingprogram are eligible to enroll in this plan on a voluntarybasis. International students with a visa status other thanan F-1 or J-1 who are engaged in educational activitiesthrough the University provided he or she: 1) possesses acurrent valid visa; and 2) is temporarily located outside hisor her home country as a non-resident alien mayparticipate on a voluntary basis.
International students engaged in Practical Training (OPT)through the University are eligible to enroll for up to oneyear (or the length of the OPT term, whichever is thelesser) beyond their regular course of study, provided theywere enrolled in the separate University-sponsoredInternational Student Health Insurance Plan in the
COVERAGE DATES AND COSTS (CON’T)
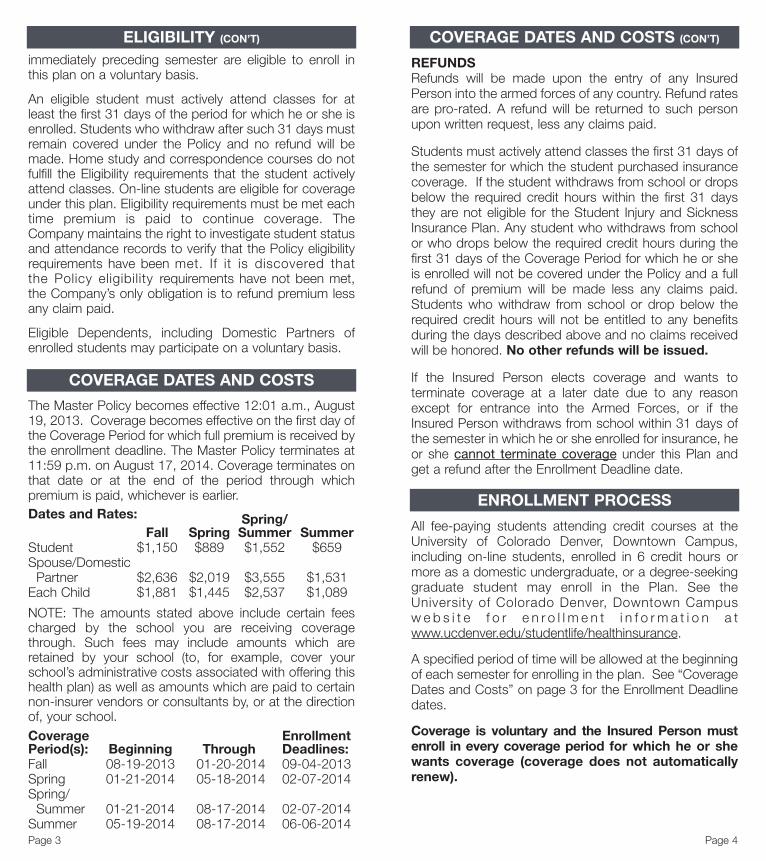
REFUNDSRefunds will be made upon the entry of any InsuredPerson into the armed forces of any country. Refund ratesare pro-rated. A refund will be returned to such personupon written request, less any claims paid.
Students must actively attend classes the first 31 days ofthe semester for which the student purchased insurancecoverage. If the student withdraws from school or dropsbelow the required credit hours within the first 31 daysthey are not eligible for the Student Injury and SicknessInsurance Plan. Any student who withdraws from schoolor who drops below the required credit hours during thefirst 31 days of the Coverage Period for which he or sheis enrolled will not be covered under the Policy and a fullrefund of premium will be made less any claims paid.Students who withdraw from school or drop below therequired credit hours will not be entitled to any benefitsduring the days described above and no claims receivedwill be honored. No other refunds will be issued.
If the Insured Person elects coverage and wants toterminate coverage at a later date due to any reasonexcept for entrance into the Armed Forces, or if theInsured Person withdraws from school within 31 days ofthe semester in which he or she enrolled for insurance, heor she cannot terminate coverage under this Plan andget a refund after the Enrollment Deadline date.
ENROLLMENT PROCESS
All fee-paying students attending credit courses at theUniversity of Colorado Denver, Downtown Campus,including on-line students, enrolled in 6 credit hours ormore as a domestic undergraduate, or a degree-seekinggraduate student may enroll in the Plan. See theUniversity of Colorado Denver, Downtown Campusw e b s i t e f o r e n r o l l m e n t i n f o r m a t i o n a twww.ucdenver.edu/studentlife/healthinsurance.
A specified period of time will be allowed at the beginningof each semester for enrolling in the plan. See “CoverageDates and Costs” on page 3 for the Enrollment Deadlinedates.
Coverage is voluntary and the Insured Person mustenroll in every coverage period for which he or shewants coverage (coverage does not automaticallyrenew).
Page 4
immediately preceding semester are eligible to enroll inthis plan on a voluntary basis.
An eligible student must actively attend classes for atleast the first 31 days of the period for which he or she isenrolled. Students who withdraw after such 31 days mustremain covered under the Policy and no refund will bemade. Home study and correspondence courses do notfulfill the Eligibility requirements that the student activelyattend classes. On-line students are eligible for coverageunder this plan. Eligibility requirements must be met eachtime premium is paid to continue coverage. TheCompany maintains the right to investigate student statusand attendance records to verify that the Policy eligibilityrequirements have been met. If it is discovered thatthe Policy eligibility requirements have not been met,the Company’s only obligation is to refund premium lessany claim paid.
Eligible Dependents, including Domestic Partners ofenrolled students may participate on a voluntary basis.
COVERAGE DATES AND COSTS
The Master Policy becomes effective 12:01 a.m., August19, 2013. Coverage becomes effective on the first day ofthe Coverage Period for which full premium is received bythe enrollment deadline. The Master Policy terminates at11:59 p.m. on August 17, 2014. Coverage terminates onthat date or at the end of the period through whichpremium is paid, whichever is earlier.Dates and Rates: Spring/
Fall Spring Summer SummerStudent $1,150 $889 $1,552 $659Spouse/DomesticPartner $2,636 $2,019 $3,555 $1,531
Each Child $1,881 $1,445 $2,537 $1,089
NOTE: The amounts stated above include certain feescharged by the school you are receiving coveragethrough. Such fees may include amounts which areretained by your school (to, for example, cover yourschool’s administrative costs associated with offering thishealth plan) as well as amounts which are paid to certainnon-insurer vendors or consultants by, or at the directionof, your school.Coverage EnrollmentPeriod(s): Beginning Through Deadlines:Fall 08-19-2013 01-20-2014 09-04-2013Spring 01-21-2014 05-18-2014 02-07-2014Spring/Summer 01-21-2014 08-17-2014 02-07-2014
Summer 05-19-2014 08-17-2014 06-06-2014Page 3
ELIGIBILITY (CON’T)

Page 6
DEPENDENT COVERAGE(Including Newborn Enrollment and Eligibility)
Eligible students who do enroll may also insure theireligible dependents on a voluntary basis. Eligibledependents are the spouse or Domestic Partner anddependent children under age 26. Dependent/DomesticPartner eligibility expires concurrently with that of theInsured Student unless the dependent is covered throughthe Extension of Benefits provision after termination ofcoverage.
Newborn ChildrenIn the event of the birth of a child to an Insured Personwhile the student’s health plan is in force, that childautomatically becomes a Insured Person from themoment of birth. Coverage will continue for 31 days. If thestudent wants continuing coverage for the newborn after31 days, enrollment and payment of premium must bemade within the first 31 days, or the coverage willterminate for that child at the end of the 31-day period.While covered under the Policy, coverage is subject to allPolicy provisions, including the deductible. Benefitsmandated by the state of Colorado that apply to newborninfants are payable under the Policy for the first 31 days.
LATE ENROLLMENTStudents will not be allowed to enroll in the Plan after theapplicable enrollment deadline period unless proof isfurnished that the eligible student was dropped fromcoverage under another Creditable health plan during the30 days* immediately preceding the date of the requestfor late enrollment. In such cases, the cost of the periodwill be the same as it would have been at the beginningof that period but the effective date will be the date thestudent enrolls and makes the full payment. The premiumfor the period purchased will not be pro-rated unless theperiod purchased is 60 days or less. In such cases, a onemonth premium amount will apply to coverage periods ofup to 30 days and a two month premium amount willapply to Coverage Periods of 31 to 60 days.
*30 days means the enrollment form and full payment isdue at the Student Insurance Office within that 30 dayperiod.
Page 5
CONFIRMATION OF COVERAGEFOR PARTICULAR SERVICES
It is the student’s responsibility to confirm whether or nota particular service is covered under the plan. Thisconfirmation must be done with AmeriBen by calling themat 855-539-8678. Health Center staff, including medicalproviders, are not adequately trained to provideconfirmation of coverage for any services.
Health Center at Auraria: 303-556-2525Find out the availability of daily access, appointments andhours of the Health Center.
100% Reimbursement With NO Deductible orCoinsurance
(This applies to eligible services; this option is notalways available due to hours of operation andstaffing)
Prescriptions at the Health Center at Auraria:Are not subject to any copay up to a 30-day supply perprescription. Contraceptives are provided at the HealthCenter at Auraria for students only.
SPECIAL HEALTH CENTER BENEFITSThe deductible and pre-existing condition exclusion willbe waived and benefits will be paid at 100% forMedical Expenses incurred when treatment is renderedat the Health Center at Auraria. This includes limitedwell care, supplies, in-house testing and procedures.No claim forms will be required. Health Center atAuraria benefits are not always available due to hoursof operation and staffing.
SUMMARY OF BENEFITS
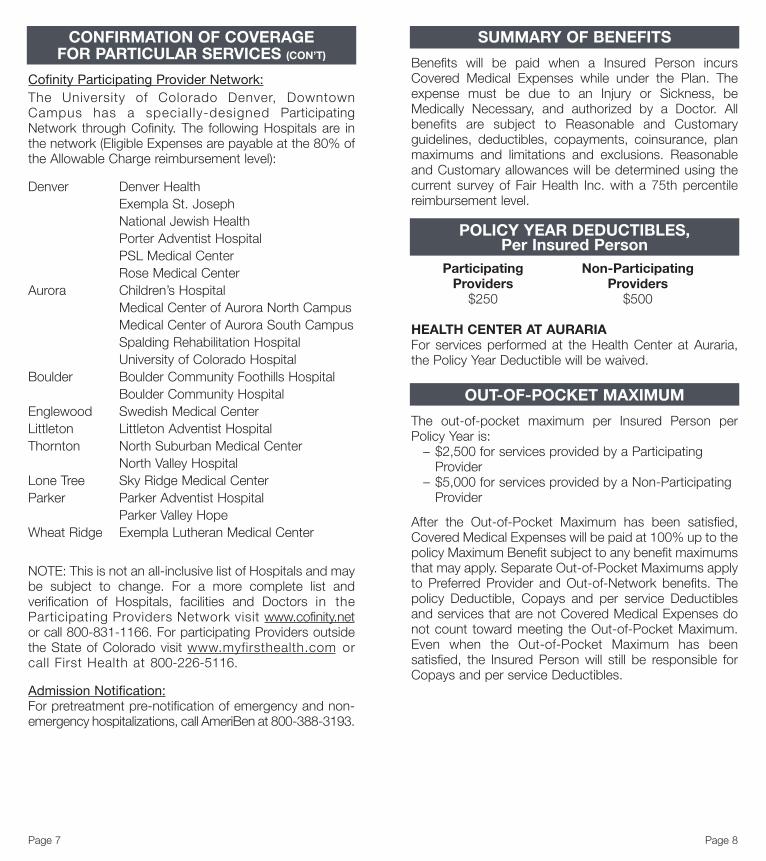
Benefits will be paid when a Insured Person incursCovered Medical Expenses while under the Plan. Theexpense must be due to an Injury or Sickness, beMedically Necessary, and authorized by a Doctor. Allbenefits are subject to Reasonable and Customaryguidelines, deductibles, copayments, coinsurance, planmaximums and limitations and exclusions. Reasonableand Customary allowances will be determined using thecurrent survey of Fair Health Inc. with a 75th percentilereimbursement level.
POLICY YEAR DEDUCTIBLES,Per Insured Person
Participating Non-ParticipatingProviders Providers
$250 $500
HEALTH CENTER AT AURARIAFor services performed at the Health Center at Auraria,the Policy Year Deductible will be waived.
OUT-OF-POCKET MAXIMUM
The out-of-pocket maximum per Insured Person perPolicy Year is:– $2,500 for services provided by a ParticipatingProvider
– $5,000 for services provided by a Non-ParticipatingProvider
After the Out-of-Pocket Maximum has been satisfied,Covered Medical Expenses will be paid at 100% up to thepolicy Maximum Benefit subject to any benefit maximumsthat may apply. Separate Out-of-Pocket Maximums applyto Preferred Provider and Out-of-Network benefits. Thepolicy Deductible, Copays and per service Deductiblesand services that are not Covered Medical Expenses donot count toward meeting the Out-of-Pocket Maximum.Even when the Out-of-Pocket Maximum has beensatisfied, the Insured Person will still be responsible forCopays and per service Deductibles.
Page 8
Cofinity Participating Provider Network:The University of Colorado Denver, DowntownCampus has a special ly-designed ParticipatingNetwork through Cofinity. The following Hospitals are inthe network (Eligible Expenses are payable at the 80% ofthe Allowable Charge reimbursement level):
Denver Denver HealthExempla St. JosephNational Jewish HealthPorter Adventist HospitalPSL Medical CenterRose Medical Center
Aurora Children’s HospitalMedical Center of Aurora North CampusMedical Center of Aurora South CampusSpalding Rehabilitation HospitalUniversity of Colorado Hospital
Boulder Boulder Community Foothills HospitalBoulder Community Hospital
Englewood Swedish Medical CenterLittleton Littleton Adventist HospitalThornton North Suburban Medical Center
North Valley HospitalLone Tree Sky Ridge Medical CenterParker Parker Adventist Hospital
Parker Valley HopeWheat Ridge Exempla Lutheran Medical Center
NOTE: This is not an all-inclusive list of Hospitals and maybe subject to change. For a more complete list andverification of Hospitals, facilities and Doctors in theParticipating Providers Network visit www.cofinity.netor call 800-831-1166. For participating Providers outsidethe State of Colorado visit www.myfirsthealth.com orcall First Health at 800-226-5116.
Admission Notification:For pretreatment pre-notification of emergency and non-emergency hospitalizations, call AmeriBen at 800-388-3193.
Page 7
CONFIRMATION OF COVERAGEFOR PARTICULAR SERVICES (CON’T)

for which the medication is dispensed. Commonconditions that involve treatment with one of the specialtydrugs include multiple sclerosis, hepatitis C andrheumatoid arthritis.
With a new Specialty Pharmacy prescription, a InsuredPerson may contact Member Services or access theinternet website address shown on the Insured Person’smedical identification card to identify the drugs containedon the Specialty Pharmacy list. A Insured Person mayalso contact Member Services or access the internetwebsite for assistance in locating the Specialty Pharmacythat can be used to obtain medication.
The Copay for Specialty drugs will mirror the RetailNetwork Pharmacy copays. Specialty Drugs can only befilled for 30 days. Members may fill a one-month supply ata local participating pharmacy before using the SpecialtyPharmacy Network (SPN).
PRESCRIPTION DRUG PLANHEALTH CENTER AT AURARIA
Maintenance medications filled at the Health Center atAuraria may be filled up to a 90 day supply. No copays ordeductibles apply at the Health Center at Auraria forprescription drugs.
For Maintenance medications filled near the end of thesemester, only a 30 day supply can be filled 30 days orless to the end of the semester for which premium hasbeen paid; and only a 60 day supply can be filled 60 to 30days to the end of the semester for which premium hasbeen paid. If it is over 60 days to the end of the semesterfor which premium has been paid a 90 day supply can befilled.
Contraceptives provided at the Health Center at Aurariaare provided with no copay.
PRE-EXISTING CONDITIONS
Covered Medical Expenses are subject to Exclusions andLimitations for Pre-Existing Conditions on page 31 andCreditable Coverage on page 32.
RIGHT OF REIMBURSEMENT
The Company shall have a lien against any recoveryreceived by an Insured Person as compensation for anInjury or Sickness to the extent that the Insured Personreceived benefits for such Injury or Sickness under thecoverage of the Policy. The Company’s lien will apply to
Page 10
PRESCRIPTION DRUG PLAN
Benefits are provided through Express Scripts, apoint-of-service provider. Please call 800-206-4005for questions regarding benefits or participatingpharmacies. If a Insured Person incurs Rx claimswithin the first 6 weeks of enrollment, the InsuredPerson must pay for the Rx and submit a claim toExpress Scripts after the 6th week at:
Express Scripts, Inc.P.O. Box 66583St. Louis, MO 63166-6583Attn: STD AccntsGroup # AM2A
After 6 weeks, the Insured Person may go to anyparticipating pharmacy. A $10 Copay will apply pergeneric prescription. A Copay of $30 will apply perbrand name prescription. A Copay of $50 will applyper non-formulary prescription.
Copays are for allowable drugs, for up to a 31 daysupply per prescription or refill. Mail Order is notavailable for prescriptions. Generic oral contraceptivesare covered with no copay. Brand and non-formularycopays will apply unless there is medical necessity. Ifyou have medical necessity for Brand and non-formulary contraceptive drugs your provider must fillout a Prior Authorization form and it must be approvedby Express Scripts. All contraceptives at the HealthCenter at Auraria are covered with no copays.
When a generic drug is available and the InsuredPerson chooses to purchase a brand name drug, evenwhen the Doctor writes “dispense as written” or “maynot substitute,” the Insured Person must pay the costdifference between the brand name prescription andthe generic prescription, in addition to the Copay. Forprescriptions filled at non-network participatingpharmacies the Insured Person will be reimbursed thedifference between the retail amount the InsuredPerson paid at the pharmacy and the networknegotiated rate less the applicable Copay.
Specialty Drug Program – The Specialty Drug Programcovers certain drugs commonly referred to as high-costspecialty drugs. To receive the network discount forthese medications, and lower out-of-pocket costs, thesedrugs must be obtained by mail through a select group ofpharmacies. These pharmacies comprise the SpecialtyPharmacy Network (SPN). The SPN specializes indispensing and delivering drugs that require specialhandling. Specialty Pharmacies provide additional helpfulservices, including free courier delivery, MedicallyNecessary ancillary supplies such as syringes and alcoholswabs, and education programs focused on the disease
Page 9
PRESCRIPTION DRUG PLAN (CON’T)

“Autism Spectrum Disorders” include the followingneurobiological disorders: autistic disorder,asperger’s disorder, and atypical autism as adiagnosis within pervasive developmental disordernot otherwise specified, as defined in the most recentedition of the Diagnostic and Statistical Manual ofMental Disorders at the time of diagnosis.
“Treatment for Autism Spectrum Disorders” shallbe for treatments that are Medically Necessary,appropriate, effective, or efficient. Treatment forAutism Spectrum Disorders shall include:
a. Evaluation and assessment services;b. Behavior training and behavior management
and applied behavior analysis, including but notlimited to, consultations, direct care, supervision,or treatment, or any combination thereof, providedby autism services providers;
c. Habilitative or rehabilitative care, including but notlimited to, occupational therapy, physical therapy,or speech therapy, or any combination of thosetherapies;
d. Psychiatric care;e. Psychological care, including family counseling;f. Therapeutic care; andg. Pharmacy care and medication if provided for in
the policy.
Benefits shall be subject to all Deductible,Copayment, Coinsurance, limitations, or any otherprovisions of the policy.
2. Biologically Based Mental Illness: Benefits will bepaid the same as any other Sickness for the treatmentof Biologically Based Mental Illness and MentalDisorders as defined below. The benefit providedwill not duplicate any other benefits provided in thispolicy.
“Biological ly Based Mental I l lness” meansschizophrenia, schizoaffective disorder, bipolaraffective disorder, major depressive disorder, specificobsessive-compulsive disorder, and panic disorder.
“Mental Disorder” means posttraumatic stressdisorder, drug and alcohol disorders, dysthymia,cyclothymia, social phobia, agoraphobia with panicdisorder, and general anxiety disorder. MentalDisorder also includes anorexia nervosa and bulimianervosa to the extent those diagnoses are treated onan out-patient, day treatment, and in-patient basis,exclusive of residential treatment.
Benefits shall be subject to all Deductible,Copayment, Coinsurance, limitations, or any otherprovisions of the policy.
Page 12
such recovery made by the Insured Person from anyperson, or entity that was responsible for causing suchInjury or Sickness or their insurers. The Insured Personwill not be required to return to the Company more thanthe amount which was recovered for such Injury orSickness.
The Insured Person (or a parent or a guardian if theInsured Person is not able to execute such papers) willexecute and deliver such papers as may be required bythe Company. Also, the Insured Person will do whateverelse is needed to help the Company in its attempts torecover the benefits it paid under the Policy to the InsuredPerson or the Insured Person’s assignee.
MAXIMUM BENEFIT
The maximum benefit is $500,000 per Insured Person perPolicy Year.
GENERAL PLAN PROVISIONS
Coverage will be in effect 24 hours a day for emergencytreatment. An Insured Person will be insured at home,school or when traveling outside the United States whileinsurance is in force.
COVERED MEDICAL EXPENSES
Benefits are payable for Covered Medical Expenses (see"Definitions") less any Deductible incurred by or for anInsured Person for loss due to Injury or Sickness subjectto: a) the Maximum Benefit for all services; b) themaximum amount for specific services; both as set forthin the Schedule of Benefits; and c) any Coinsuranceamount set forth in the Schedule of Benefits or anyendorsement hereto.
Covered Medical Expenses include:
State Mandated Covered Medical Expenses
1. Treatment of Autism Spectrum Disorders: Benefitswill be paid the same as any other Sickness forCovered Medical Expenses related to theassessment, diagnosis and treatment, includingApplied Behavior Analysis, of Autism SpectrumDisorders. Treatment for Autism Spectrum Disordersmust be prescribed or ordered by a licensedPhysician or license psychologist.
“Applied behavior analysis” means the use ofbehavior analytic methods and research findings tochange socially important behaviors in meaningfulways.
Page 11
COVERED MEDICAL EXPENSES (CON’T)RIGHT OF REIMBURSEMENT (CON’T)
feeding appliances; Medically Necessary orthodonticand prosthodontic treatment; habilitative speechtherapy, otolaryngology treatment; and audiologicalassessments and treatment.
Benefits shall be subject to all Deductible,Copayment, Coinsurance, limitations, or any otherprovisions of the policy.
6. Therapies for Congenital Defects and BirthAbnormalities: Benefits will be paid the same as anyother Sickness for physical, occupational and speechtherapy for congenital defects and birthabnormalities for covered Dependent childrenbeginning after the first 31 days of life to five years ofage.
Benefits will be paid for the greater of the number ofsuch visits provided under the policy or twenty visitsper year for each therapy. Benefits will be providedwithout regard to whether the condition is acute orchronic and without regard to whether the purpose ofthe therapy is to maintain or to improve functionalcapacity.
Benefits shall be subject to all Deductible,Copayment, Coinsurance, limitations, or any otherprovisions of the policy.
7. Diabetes: Benefits will be paid for the Usual andCustomary Charges for all medically appropriate andnecessary equipment, supplies, and outpatientdiabetes self-management training and educationalservices including nutritional therapy if prescribed bya Physician.
Diabetes outpatient self-management training andeducation shall be provided by a Physician withexpertise in diabetes.
Benefits shall be subject to all Deductible,Copayment, Coinsurance, limitations, or any otherprovisions of the policy.
8. Hearing Aids for Minor Children: Benefits will bepaid for Covered Medical Expenses for Hearing Aidsfor a Minor Child who has a hearing loss that hasbeen verified by a licensed Physician and a licensedAudiologist. The Hearing Aid shall be medicallyappropriate to meet the needs of the Minor Childaccording to accepted professional standards.
Benefits shall include the purchase of the following:
a. Initial Hearing Aids and replacement Hearing Aidsnot more frequently than every five years;
b. A new Hearing Aid when alterations to the existingHearing Aid cannot adequately meet the needs ofthe Minor Child; and
Page 14
3. Cervical Cancer Vaccines: Benefits are payable forthe cost of cervical cancer vaccinations for all femaleInsured Persons for whom a vaccination isrecommended by the Advisory Committee onImmunization practices of the United StatesDepartment of Health and Human Services.
4. Child Health Supervision Services: Benefits will bepaid for the Usual and Customary Charges for ChildHealth Supervision Services from birth up to the ageof 13. Benefits are payable on a per visit basis to onehealth care provider per visit.
Child Health Supervision Services rendered during aperiodic review are covered only to the extent suchservices are provided during the course of one visitby, or under the supervision of a single Physician,Physician’s assistant or Registered Nurse.
Child Health Supervision Services means theperiodic review of a child’s physical and emotionalstatus by a Physician or other provider as above. Areview shall include but not be limited to a history,complete physical examination, developmentalassessment, anticipatory guidance, appropriateimmunizations, preventative services, andlaboratory tests in keeping with prevailing medicalstandards.
Immunizations are based on the recommendedchildhood immunization schedule and therecommended immunization schedule for childrenwho start late or who are more than 1 month behindpublished by the CDC. Recommended schedulesare available from:
Advisory Committee on Immunization Practices,www.cdc.aov/nip/acip;
American Academy of Pediatrics, www.aap.org;
American Academy of Family Physicians,www.aafp.org.
The policy Deductible and dollar limits will not beapplied to this benefit.
Benefits shall be subject to all Copayment,Coinsurance, limitations, or any other provisions ofthe policy.
5. Cleft Lip or Cleft Palate: Benefits will be paid thesame as any other Sickness for treatment of newbornchildren born with cleft lip or cleft palate or both.Benefits shall include the Medically Necessary careand treatment including oral and facial surgery;surgical management; the Medically Necessarycare by a plastic or oral surgeon; prosthetictreatment such as obturators, speech appliances,
Page 13
COVERED MEDICAL EXPENSES (CON’T) COVERED MEDICAL EXPENSES (CON’T)
written, oral or electronic prescription. Benefits will notbe provided for alternative medicine.
Coverage includes but is not limited to the followingdiagnosed conditions: phenylketonuria; maternalphenylketonuria; maple syrup urine disease;tyrosinemia; homocystinuria; histidinemia; urea cycledisorders; hyperlysinemia; glutaric acidemias;methylmalonic acidemia; and propionic acidemia.Benefits do not apply to cystic fibrosis patientsor lactose- or soy-intolerant patients.
There is no age limit on the benefits provided forinherited enzymatic disorders except forphenylketonuria. The maximum age to receivebenefits for phenylketonuria is twenty-one years ofage; except that the maximum age to receive benefitsfor phenylketonuria for women who are of child-bearing age is thirty-five years of age.
Medical foods means prescription metabolicformulas and their modular counterparts, obtainedthrough a pharmacy that are specifically designedand manufactured for the treatment of inheritedenzymatic disorders caused by single gene defectsinvolved in the metabolism of amino, organic, andfatty acids and for which medically standard methodsof diagnosis, treatment, and monitoring exist. Suchformulas are specifically processed or formulated tobe deficient in one or more nutrients and are to beconsumed or administered enterally either via tube ororal route under the direction of a Physician.
Benefits shall be subject to all Deductible,Copayment, Coinsurance, limitations, or any otherprovisions of the policy.
11. Oral Anticancer Medication: If the policy providesbenefits for cancer chemotherapy treatment, thenbenefits will be provided for prescribed, orallyadministered anticancer medication that has beenapproved by the Federal Food and DrugAdministration and is used to kill or slow the growth ofcancerous cells.
The orally administered medication shall be providedat a cost to the Insured not to exceed theCoinsurance percentage or the Copayment amountas is applied to an intravenously administered or aninjected cancer medication prescribed for the samepurpose.
The medication provided pursuant to this benefitshall:
a. only be prescribed upon a finding that it isMedically Necessary by the treating Physician for
Page 16
c. Services and supplies including, but not limited to,the initial assessment, fitting, adjustments, andauditory training that is provided according toprofessional standards.
“Hearing Aid” means amplification technology thatoptimizes audibility and listening skills in theenvironments commonly experienced by the patient,including a wearable instrument or device designed toaid or compensate for impaired human hearing.“Hearing Aid” shall include any parts or ear molds.
“Minor Child” means an Insured Person under the ageof eighteen.
Benefits shall be subject to all Deductible,Copayment, Coinsurance, limitations, or any otherprovisions of the policy.
9. Hospitalization and General Anesthesia forDental Procedures for Dependent Children:Benefits will be paid the same as any other Sicknessfor general anesthesia, when rendered in a Hospital,outpatient surgical facility, or other facility licensedpursuant to Colorado Statute Section 25-3-101, andfor associated Hospital or facility charges for dentalcare provided to a Dependent child. Such Dependentchild shall, in the treating Physician’s opinion, meetone or more of the following criteria:
a. The child has a physical, mental, or medicallycompromising condition;
b. The child has dental needs for which localanesthesia is ineffective because of acuteinfection, anatomic variations, or allergy;
c. The child is an extremely uncooperative,unmanageable, anxious, or uncommunicativechild or adolescent with dental needs deemedsufficiently important that dental care cannot bedeferred; or
d. The child has sustained extensive orofacial anddental trauma.
Benefits shall be subject to all Deductible,Copayment, Coinsurance, limitations, or any otherprovisions of the policy.
10.Medical Foods: Benefits are payable for MedicalFoods needed to treat inherited enzymaticdisorders caused by single gene defects involved inthe metabolism of amino, organic, and fatty acids asspecified below.
If the policy provides benefits for Prescription Drugs,benefits will be paid the same as any other Sicknessfor Medical Foods, to the extent Medically Necessary,for home use for which a Physician has issued a
Page 15
COVERED MEDICAL EXPENSES (CON’T) COVERED MEDICAL EXPENSES (CON’T)

who has a family medical history of colorectalcancer; a prior occurrence of cancer or precursorneoplastic polyps; a prior occurrence of achronic digestive disease condition such asinflammatory bowel disease, Crohn’s disease, orulcerative colitis; or other predisposing factors asdetermined by a Physician;
f. Childhood immunizations pursuant to theschedule established by the ACIP;
g. Influenza vaccinations pursuant to the scheduleestablished by the ACIP;
h. Pneumococcal vaccinations pursuant to theschedule established by the ACIP; and
i. Tobacco use screening of adults and tobaccocessation interventions by the Insured Person’sPhysician.
For the purposes of this mandate:
“ACIP” means the advisory committee onimmunization practices to the centers for diseasecontrol and prevention in the federal Department ofHealth and Human Services, or any successor entity.
“A Recommendation” means a recommendationadopted by the task force that strongly recommendsthat clinicians provide a preventive health care servicebecause the task force found there is a high certaintythat the net benefit of the preventive health careservice is substantial.
“B Recommendation” means a recommendationadopted by the task force that recommends thatclinicians provide a preventive health care servicebecause the task force found there is a high certaintythat the net benefit is moderate or there is moderatecertainty that the net benefit is moderate tosubstantial.
“Task force” means the U.S. preventive services taskforce, or any successor organization, sponsored bythe agency for healthcare research and quality, thehealth services research arm of the federalDepartment of Health and Human Services.
The policy Deductible and Coinsurance will not beapplied to this benefit.
Benefits shall be subject to all Copayments,limitations or any other provisions of the policy.
13. Prostate Cancer Screening: Benefits will be paidfor actual charges incurred for an annual screening bya Physician for the early detection of prostate cancer.Benefits will be payable for one screening per year forany male Insured 50 years of age or older. Onescreening per year shall be covered for any male
Page 18
the purpose of killing or slowing the growth ofcancerous cells in a manner that is inaccordance with nationally accepted standardsof medical practice;
b. be clinically appropriate in terms of type,frequency, extent site, and duration; and
c. not be primarily for the convenience of the Insuredor Physician.
This benefit does not require the use of orallyadministered medications as a replacement for othercancer medications, nor does it prohibit the Companyfrom applying an appropriate formulary or otherclinical management to any medication described inthis benefit.
Benefits shall be subject to all Deductible,Copayment, Coinsurance, limitations, or any otherprovisions of the policy.
12. Preventive Health Care: Benefits will be providedfor the cost of the following Preventive Health Careservices, in accordance with the A or Brecommendations of the Task Force for theparticular Preventive Health Care service:
a. Alcohol misuse screening and behavioralcounseling interventions for adults by theirPhysician;
b. Cervical Cancer Screening;c. Breast Cancer Screening with Mammography:
1) Benefits shall be determined on a Policy Yearbasis and shall in no way diminish or limitdiagnostic benefits otherwise allowable underthe policy;
2) If an Insured Person who is eligible for apreventive mammography screening has notutilized the benefit during the Policy Year, thenthe coverage shall apply to one diagnosticscreening for that same Policy Year. Any otherdiagnostic screenings shall be subject to allapplicable policy provisions;
3) Benefits shall also be provided for an annualbreast cancer screening with mammographyfor an Insured Person possessing at leastone risk factor including, but not limited to, afamily history of breast cancer, being fortyyears of age or older, or a geneticpredisposition to breast cancer;
d. Cholesterol screening for lipid disorders;e. Colorectal cancer screening coverage for tests for
the early detection of colorectal cancer andadenomatous polyps. Benefits shall also beprovided to an Insured Person who is at a high riskfor colorectal cancer, including an Insured Person
Page 17
COVERED MEDICAL EXPENSES (CON’T) COVERED MEDICAL EXPENSES (CON’T)
All Other Covered Medical Expenses
16. Accidental Death and Dismemberment: thebenefits and the maximum amounts are specified inthe Schedule of Benefits.
17. Ambulance Services18. Anesthetist Services (Inpatient): professional serv-
ices administered in connection with Inpatient surgery.19. Anesthetist Services (Outpatient): professional
services administered in connection with outpatientsurgery.
20. Assistant Surgeon Fees: in connection withinpatient and outpatient surgery.
21. Chemotherapy (Outpatient)22. Complications of Pregnancy: Same as any other
Sickness.23. Consultant Physician Fees: when requested and
approved by the attending Physician.24. Day Surgery Miscellaneous (Outpatient): in
connection with outpatient day surgery; excludingnon-scheduled surgery; and surgery performed in aHospital emergency room; trauma center; Physician'soffice; or clinic. Benefits will be paid for services andsupplies such as: the cost of the operating room;laboratory tests and X-ray examinations, includingprofessional fees; anesthesia; drugs or medicines;therapeutic services; and supplies.
25. Dental Treatment: 1) performed by a Physician; and,2) made necessary by Injury to Sound, Natural Teeth.Breaking a tooth while eating is not covered. Routinedental care and treatment to the gums are notcovered.
26. Diabetes Services: See Benefits for Diabetes.27. Diagnostic X-ray Services (Outpatient):
Diagnostic X-rays are only those procedures identifiedin Physicians' Current Procedural Terminology (CPT)as codes 70000 - 79999 inclusive. X-ray services forpreventive care are provided as specified underPreventive Care Services.
28. Durable Medical Equipment: 1) when prescribedby a Physician; and 2) a written prescriptionaccompanies the claim when submitted. Durablemedical equipment includes equipment that: 1) isprimarily and customarily used to serve a medicalpurpose; 2) can withstand repeated use; and 3)generally is not useful to a person in the absence ofInjury or Sickness. Benefits for durable medicalequipment are limited to the initial purchase or onereplacement purchase per Policy Year. No benefits willbe paid for rental charges in excess of purchase price.See also Benefits for Prosthetic Devices on page 18.
29. Hospital Miscellaneous Expenses: 1) whenconfined as an Inpatient; or 2) as a precondition forbeing confined as an Inpatient. Benefits will be paidfor services and supplies such as: the cost of the
Page 20
Insured 40 to 50 years of age who is at risk ofdeveloping prostate cancer as determined by theInsured’s Physician. The screening shall consist of thefollowing tests:
a. A prostate-specific antigen (PSA) blood test; andb. Digital rectal examination.
The policy Deductible will not be applied to thisbenefit and this benefit will not reduce any diagnosticbenefits otherwise allowable under the policy.
Benefits shall be subject to all Copayment,Coinsurance, limitations, or any other provisions ofthe policy.
14. Prosthetic Devices: Benefits will be paid for theUsual and Customary Charges for the purchase ofProsthetic Devices.
Prosthetic device means an artificial device to replace,in whole or in part, an arm or leg. Benefits are limitedto the most appropriate model that adequately meetsthe medical needs of the Insured as determined by aPhysician. Repairs and replacements of ProstheticDevices are also covered unless necessitated bymisuse or loss.
Benefits shall be subject to all Deductible,Copayment, Coinsurance, limitations, or any otherprovisions of the policy.
15. Telemedicine Services: Benefits will be paid forCovered Medical Expenses on the same basis asservices provided through a face-to-face consultationfor services provided through Telemedicine for anInsured residing in a county with one hundred fiftythousand or fewer residents. “Telemedicine” meansthe use of interactive audio, video, or other electronicmedia to deliver health care. The term includes theuse of electronic media for diagnosis, consultation,treatment, transfer of medical data and medicaleducation. The term does not include servicesperformed using a telephone or facsimile machine.
Nothing in this provision shall require the use ofTelemedicine when in-person care by a participatingprovider is available to an Insured Person within theCompany’s network and within the Insured’sgeographic area.
Benefits shall be subject to all Deductible,Copayment, Coinsurance, limitations, or any otherprovisions of the policy.
Page 19
COVERED MEDICAL EXPENSES (CON’T) COVERED MEDICAL EXPENSES (CON’T)

Page 21
SCHEDULE OF BENEFITSMaximum Benefit: $500,000 (per Insured Person per Policy Year)Deductible: $250 PPO Network (per Insured Person per Policy Year)
$500 OON (per Insured Person per Policy Year)Co-Insurance 80% PPO Providers (except as noted below)
60% OON (except as noted below)Out-of-Pocket $2,500 PPO (excluding deductible, copay and non-covered expenses) and (per insured person per policy year)
$5,000 OON (excluding deductible, copay and non-covered expenses) and (per insured person per policy year)
The PPO Network is Cofinity (in the State of Colorado) and FIRST HEALTH (outside the State of Colorado). The Deductible and Pre-Existing Conditionexclusion will be waived and benefits will be paid at 100% for Medical Expenses incurred when treatment is rendered at the Health Center at Auraria.Pregnancy is not subject to the pre-existing condition limitations of the Plan.
PA = Preferred Allowance for PPO providers. U&C = Usual & Customary of Fair Health Index for non-network (OON) providers.The Fair Health Index for this Plan is 75%.
BENEFIT HEALTH CENTER PREFERRED OUT-OF-NETWORK ADDITIONAL LIMITATIONSDESCRIPTIONS AT AURARIA PROVIDER PROVIDER AND EXPLANATIONSINPATIENTAnesthetist: N/A 80% of PA 60% of U&CAssistant Surgeon: N/A 25% of surgery allowance 25% of surgery allowanceHospital Miscellaneous: N/A 80% of PA 60% of U&CPhysician's Visits: N/A 80% of PA 60% of U&CPhysiotherapy: N/A 80% of PA 60% of U&CPre-admission Testing: N/A 80% of PA 60% of U&CRegistered Nurse's Services: N/A 80% of PA 60% of U&CRoom & Board: N/A 80% of PA 60% of U&CRoutine Newborn Care: N/A Paid as any Paid as any
other Sickness other SicknessSurgery: N/A 80% of PA 60% of U&COUTPATIENTAnesthetist: 100% 80% of PA 60% of U&CAssistant Surgeon: 100% 25% of surgery allowance 25% of surgery allowanceChemotherapy: N/A 80% of PA 60% of U&CDay Surgery Miscellaneous: 100% 80% of PA 60% of U&CInjections: 100% 80% of PA 60% of U&CLaboratory: 100% 80% of PA 60% of U&CMedical Emergency: 100% $150 copay per visit $150 copay per visit,
80% of PA 80% of U&CPhysician's Visits: 100% $20 copay per visit 60% of U&C
100% of PAPhysiotherapy: N/A 80% of PA 60% of U&CPrescription Drugs: 100% $10 copay generic No Benefits Prescriptions filled at Express Scripts
$30 copay brand pharmacies.$50 copay non-formulary Coverage for Maintenance Drugs throughUp to a 31-day supply Express Scripts for up to 90 days for 3x theper Rx. copay and up to 60 days for 2x the copay.
Radiation Therapy: N/A 80% of PA 60% of U&CSurgery: 100% 80% of PA 60% of U&C
Page 22

Page 23
SCHEDULE OF BENEFITS (CON’T)
BENEFIT HEALTH CENTER PREFERRED OUT-OF-NETWORK ADDITIONAL LIMITATIONSDESCRIPTIONS AT AURARIA PROVIDER PROVIDER AND EXPLANATIONSTests & Procedures: 100% 80% of PA 60% of U&CX-rays: 100% 80% of PA 60% of U&COTHERAmbulance: N/A 80% of PA 80% of U&CComplications of Pregnancy: N/A Paid as any Paid as any
other Sickness other SicknessConsultant: 100% $20 copay per visit 60% of U&C
100% of PADental: 80% of PA 80% of U&C $5,000 maximum Per Policy Year
Benefits paid on Injury to Sound, Natural Teethonly. Benefits are not subject to the$500,000 Maximum Benefit.
Diabetes Services: N/A See Benefits for See Benefits forDiabetes Diabetes
Durable Medical Equipment: 100% 80% of PA 60% of U&C Exception: See Benefits for Prosthetic Devices.$5,000 maximum Per Policy Year.Durable Medical Equipment benefits payableunder the $5,000 maximum Per Policy Yearare not included in the $500,000 MaximumBenefit. Prosthetic Appliances/Orthotic Devicesare not subject to the DME $5,000 maximumPer Policy Year.
Elective Abortion: N/A No Benefits No BenefitsInfertility Testing: N/A 80% of PA 60% of U&C $1,000 maximum Per Policy Year.
Infertility testing benefits are not subject to the$500,000 Maximum Benefit.
Maternity: N/A Paid as any Paid as anyother Sickness other Sickness
Medical Evacuation: N/A Benefits provided by Benefits provided byFrontierMEDEX FrontierMEDEX
Mental Illness Treatment : N/A Paid as any Paid as any See also Benefits for Biologically Basedother Sickness other Sickness Mental Illness on page 12.
Nutrition Programs: N/A 80% of PA 60% of U&C Benefits are not subject to the $500,000Maximum Benefit.
Preventive Care Services: 100% 100% of PA No Benefits No Deductible, copay or coinsurance willbe applied to Preventive Care Services whenthe services are received from a PreferredProvider. Benefits include routine immunizationtiters. See also Benefits for Preventive HealthCare on page 17.
Reconstructive Breast Surgery N/A Paid as any Paid as anyFollowing Mastectomy: other Sickness other Sickness
Repatriation: N/A Benefits provided by Benefits provided byFrontierMEDEX FrontierMEDEX
Substance Use Disorder: 100% Paid as any Paid as any See also Benefits for Biologically Basedother Sickness other Sickness Mental Illness on page 12.
Page 24
Physician’s Visits for preventive care are provided asspecified under Preventive Care Services.
38. Physiotherapy (Inpatient): See Schedule of Benefits.39. Physiotherapy (Outpatient): Physiotherapy includes
but is not limited to the following: 1) physical therapy;2) occupational therapy; 3) cardiac rehabilitationtherapy; 4) manipulative treatment; and 5) speechtherapy, unless excluded in the policy. Review ofMedical Necessity will be performed after 12 visits perInjury or Sickness.
40. Pre-admission Testing: limited to routine tests suchas: complete blood count; urinalysis; and chest X-rays. If otherwise payable under the policy, majordiagnostic procedures such as: cat-scans; NMR's;and blood chemistries will be paid under the "HospitalMiscellaneous" benefit. This benefit is payable within3 working days prior to admission.
41. Prescription Drugs (Outpatient)42. Preventive Care Services: medical services that
have been demonstrated by clinical evidence to besafe and effective in either the early detection ofdisease or in the prevention of disease, have beenproven to have a beneficial effect on health outcomesand are limited to the following as required underapplicable law: 1) Evidence-based items or servicesthat have in effect a rating of “A” or “B” in the currentrecommendations of the United States PreventiveServices Task Force; 2) immunizations that have ineffect a recommendation from the AdvisoryCommittee on Immunization Practices of the Centersfor Disease Control and Prevention; 3) with respect toinfants, children, and adolescents, evidence-informedpreventive care and screenings provided for in thecomprehensive guidelines supported by the HealthResources and Services Administration; and 4) withrespect to women, such additional preventive careand screenings provided for in comprehensiveguidelines supported by the Health Resources andServices Administration. See also Benefits forPreventive Health Care on page 17.
43. Radiation Therapy (Outpatient)44. Reconstructive Breast Surgery Following
Mastectomy: same as any other Sickness and inconnection with a covered mastectomy. Benefitsinclude: 1) all stages of reconstruction of the breast onwhich the mastectomy has been performed; 2) sur-gery and reconstruction of the other breast toproduce a symmetrical appearance; and 3) pros-theses and physical complications of mastectomy,including lymphedemas.
45. Registered Nurse’s Services: 1) private dutynursing care only; 2) while an Inpatient; 3) ordered bya licensed Physician; and 4) a Medical Necessity.General nursing care provided by the Hospital is notcovered under this benefit.
Page 26
operating room; laboratory tests; X-ray examinations;anesthesia; drugs (excluding take home drugs) ormedicines; therapeutic services; and supplies. Incomputing the number of days payable under thisbenefit, the date of admission will be counted, but notthe date of discharge.
30. Injections (Outpatient): 1) when administered in thePhysician's office; and 2) charged on the Physician'sstatement. Immunizations for preventive care areprovided as specified under Preventive Care Services.
31. Laboratory Procedures (Outpatient): LaboratoryProcedures are only those procedures identified inPhysicians' Current Procedural Terminology (CPT) ascodes 80000 - 89999 inclusive. Laboratory proce-dures for preventive care are provided as specifiedunder Preventive Care Services.
32.Maternity: Same as any other Sickness. Benefits willbe paid for an inpatient stay of at least: 1) 48 hoursfollowing a vaginal delivery; or 2) 96 hours following acesarean section delivery. If the mother agrees, theattending Physician may discharge the mother earlierthan these minimum time frames.
33.Medical Emergency Expenses (Outpatient): onlyin connection with a Medical Emergency as defined.Benefits will be paid for the facility charge for use ofthe emergency room and supplies. Treatment mustbe rendered within 72 hours from time of Injury or firstonset of Sickness.
34.Medical Evacuation: 1) when Hospital Confined forat least five consecutive days; and 2) whenrecommended and approved by the attendingPhysician. Benefits will be paid for the evacuation ofthe Insured to his home country. This benefit is limitedto the maximum benefit specified in the Schedule ofBenefits. No additional benefits will be paid underBasic or Major Medical coverage.
35.Mental Illness Treatment: the benefits are specifiedin the Schedule of Benefits. Benefits will be paid forservices received: 1) on an Inpatient basis whileconfined to a Hospital including partialhospitalization/day treatment received at a Hospital;and 2) on an outpatient basis including intensiveoutpatient treatment. See also Benefits for BiologicallyBased Mental Illness on page 12.
36. Physician's Visits (Inpatient): non-surgical serviceswhen confined as an Inpatient. Benefits do not applywhen related to surgery. Covered Medical Expenseswill be paid under the Inpatient benefit or under theoutpatient benefit for Physician's Visits, but not bothon the same day.
37. Physician's Visits (Outpatient): Benefits do notapply when related to surgery or Physiotherapy.Covered Medical Expenses will be paid under theoutpatient benefit or under the Inpatient benefit forPhysician's Visits, but not both on the same day.
Page 25
COVERED MEDICAL EXPENSES (CON’T) COVERED MEDICAL EXPENSES (CON’T)

No benefits will be paid for: a) loss or expense caused by,contributed to, or resulting from; or b) treatment, servicesor supplies for, at, or related to any of the following:1. Acupuncture;2. Nicotine addiction, except as specifically provided in
the policy;3. Milieu therapy, learning disabilities, behavioral
problems, parent-child problems, conceptualhandicap, developmental delay or disorder or mentalretardation;
4. Cosmetic procedures, except cosmetic surgeryrequired to correct an Injury for which benefits areotherwise payable under this policy or for newborn oradopted children;
5. Custodial Care; care provided in: rest homes, healthresorts, homes for the aged, halfway houses, collegeinfirmaries or places mainly for domiciliary orCustodial Care; extended care in treatment orsubstance abuse facilities for domiciliary or CustodialCare;
6. Dental treatment, except for accidental Injury toSound, Natural Teeth
7. Elective Surgery or Elective Treatment;8. Elective abortion;9. Eye examinations, eye refractions, eyeglasses,
contact lenses, prescriptions or fitting of eyeglassesor contact lenses, vision correction surgery, or othertreatment for visual defects and problems; exceptwhen due to a covered Injury or disease process;
10. Health spa or similar facilities; strengtheningprograms;
11. Hearing examinations; hearing aids, except asspecifically provided in the policy; or other treatmentfor hearing defects and problems, except as a resultof an infection or trauma. "Hearing defects" meansany physical defect of the ear which does or canimpair normal hearing, apart from the diseaseprocess;
12. Hirsutism; alopecia;13. Hypnosis;14. Immunizations, except as specifically provided in
the policy; preventive medicines or vaccines, exceptwhere required for treatment of a covered Injury or asspecifically provided in the policy;
15. Injury or Sickness for which benefits are paid orpayable under any Workers' Compensation orOccupational Disease Law or Act, or similarlegislation;
16. Injury sustained by reason of a motor vehicleaccident to the extent that benefits are paid orpayable by any other valid and collectible insurance;
17. Injury sustained while (a) participating in anyintercollegiate, or professional sport, contest or
Page 28
46. Repatriation: if the Insured dies while insured underthe policy; benefits will be paid for: 1) preparing; and2) transporting the remains of the deceased's body tohis home country. This benefit is limited to themaximum benefit specified in the Schedule ofBenefits. No additional benefits will be paid underBasic or Major Medical coverage.
47. Room and Board Expense: 1) daily semi-privateroom rate when confined as an Inpatient; and 2)general nursing care provided and charged by theHospital.
48. Routine Newborn Care: 1) while Hospital Confined;and 2) routine nursery care provided immediately afterbirth. Benefits will be paid for an inpatient stay of atleast: 1) 48 hours following a vaginal delivery; or 2) 96hours following a cesarean section delivery. If themother agrees, the attending Physician maydischarge the newborn earlier than these minimumtime frames.
49. Substance Use Disorder Treatment: the benefitsare specified in the Schedule of Benefits. Benefits willbe paid for services received: 1) on an Inpatient basiswhile confined to a Hospital including partialhospitalization/day treatment received at a Hospital;2) on an outpatient basis including intensiveoutpatient treatment. See also Benefits for BiologicallyBased Mental Illness on page 12.
50. Surgery (Inpatient): Physician's fees for Inpatientsurgery. If two or more procedures are performedthrough the same incision or in immediate successionat the same operative session, the maximum amountpaid will not exceed 50% of the second procedureand 50% of all subsequent procedures.
51. Surgery (Outpatient): Physician's fees for outpatientsurgery. If two or more procedures are performedthrough the same incision or in immediate successionat the same operative session, the maximum amountpaid will not exceed 50%of the second procedureand 50% of all subsequent procedures.
52. Tests and Procedures (Outpatient): 1) diagnosticservices and medical procedures; 2) performedby a Physician; 3) excluding Physician's Visits;Physiotherapy; X-Rays; and Laboratory Procedures.The following therapies will be paid under the Testsand Procedures (Outpatient) benefit: inhalationtherapy; infusion therapy; pulmonary therapy;andrespiratory therapy. Tests and Procedures forpreventive care are provided as specified underPreventive Care Services.
Page 27
COVERED MEDICAL EXPENSES (CON’T) EXCLUSIONS AND LIMITATIONS

Page 30
24. Research or examinations relating to researchstudies, or any treatment for which the patient or thepatient’s representative must sign an informedconsent document identifying the treatment in whichthe patient is to participate as a research study orclinical research study;
25. Residential treatment of eating disorders, such asanorexia or bulimia;
26. Routine Newborn Infant Care, well-baby nurseryand related Physician charges except as specificallyprovided in the policy;
27. Preventive care services; routine physicalexaminations and routine testing; preventive testingor treatment; screening exams or testing in theabsence of Injury or Sickness; except as specificallyprovided in the policy;
28. Services provided normally without charge by theHealth Service of the Policyholder; or servicescovered or provided by the student health fee;
29. Skeletal irregularities of one or both jaws, includingorthognathia and mandibular retrognathia; deviatednasal septum, including submucous resection and/orother surgical correction thereof; nasal and sinussurgery, except for treatment of a covered Injury ortreatment of chronic purulent sinusitis;
30. Skydiving, parachuting, hang gliding, glider flying,parasailing, sail planing, bungee jumping, or flight inany kind of aircraft, except while riding as a passengeron a regularly scheduled flight of a commercial airline;
31. Speech therapy, except as specifically provided inthe policy;
32. Supplies, except as specifically provided in thepolicy;
33. Surgical breast reduction, breast augmentation,breast implants or breast prosthetic devices, orgynecomastia; except as specifically provided in thepolicy;
34. Treatment in a Government hospital, unless there isa legal obligation for the Insured Person to pay forsuch treatment;
35.War or any act of war, declared or undeclared; orwhile in the armed forces of any country other thanthe United States (a pro-rata premium will berefunded upon request for such period not covered);and
36.Weight management, service and supplies relatedto weight reduction programs, weight managementprograms, and treatment for obesity, (except surgeryfor morbid obesity), (treatment for Morbid Obesity iscovered. Morbid Obesity is defined as follows: MorbidObesity associated with serious and life threateningdisorders such as diabetes mellitus and hypertension.Morbid Obesity means a body weight of two times the
competition; (b) traveling to or from such sport,contest or competition as a participant; or (c) whileparticipating in any practice or conditioning programfor such sport, contest or competition;
18. Investigational services;19. Lipectomy;20. Participation in a riot or civil disorder; commission of
or attempt to commit a felony;21. Pre-existing Conditions in excess of $1,000 for a
period of 6 months, except for individuals who havebeen continuously insured for at least 6 consecutivemonths under the school’s student insurance policy;The Pre-existing Condition exclusionary period will bereduced by the total number of months that theInsured provides documentation of continuouscoverage under prior Creditable Coverage if suchCreditable Coverage was continuous to a date notmore than 90 days prior to the Insured’s EffectiveDate under this policy; This exclusion will not beapplied to an Insured Person who is under age 19;
22. Prescription Drugs, services or supplies as follows:a) Therapeutic devices or appliances, including:
hypodermic needles, syringes, support garmentsand other nonmedical substances, regardless ofintended use, except as specifically provided inthe policy;
b) Immunization agents, except as specificallyprovided in the policy, biological sera, blood orblood products administered on an outpatientbasis;
c) Drugs labeled, “Caution - limited by federal law toinvestigational use” or experimental drugs;
d) Products used for cosmetic purposes;e) Drugs used to treat or cure baldness; anabolic
steroids used for body building;f) Anorectics - drugs used for the purpose of weight
control;g) Fertility agents or sexual enhancement drugs,
such as Parlodel, Pergonal, Clomid, Profasi,Metrodin, Serophene, or Viagra;
h) Growth hormones; ori) Refills in excess of the number specified or
dispensed after one (1) year of date of theprescription.
23. Reproductive/Infertility services including but notlimited to: family planning; infertility (male or female),including any services or supplies rendered for thepurpose or with the intent of inducing conception;premarital examinations; impotence, organic orotherwise; female sterilization procedures, except asspecifically provided in the policy; vasectomy; sexualreassignment surgery; reversal of sterilizationprocedures;
Page 29
EXCLUSIONS AND LIMITATIONS (CON’T)EXCLUSIONS AND LIMITATIONS (CON’T)
Page 32
normal weight or greater, or 100 pounds in excess ofnormal body weight based on normal body weightusing generally accepted height and weight tables fora person of the same age, sex, height and frame.Benefits will be provided only upon written request fortreatment with a treatment plan written by aPhysician, and services or treatment must meet theCompany's medical criteria.) and surgery for removalof excess skin or fat.
PRE-EXISTING CONDITIONS
Expenses Incurred by an Insured Person over $1,000 asa result of a Pre-existing Condition will not be considered.
This limitation will not apply if, during the periodimmediately preceding the Insured Person’s effective dateof coverage under the current Policy, the Insured Personwas covered under prior Creditable Coverage for 6consecutive months. Prior Creditable Coverage of lessthan 6 months will be credited toward satisfying the Pre-existing Condition limitation. This waiver of Pre-existingCondition limitation will apply only if the Insured Personbecomes eligible and enrolls for coverage within 90 daysof termination of his or her prior coverage.
Pre-existing Conditions do not apply to:a. a newborn dependent child; orb. pregnancy or complications of pregnancy; orc. an Insured Person who is under age 19.
IMPORTANT NOTICEFederal regulations now permit the time you are on theUniversity of Colorado Denver, Downtown CampusStudent Injury and Sickness Insurance Plan to becounted as a credit toward satisfying pre-existingclauses in future health insurance plans you mayparticipate in after you leave the University.
These regulations provide that, when your coverageunder the University sponsored plan terminates (forexample, your academic studies at University ofColorado Denver, Downtown Campus are completedor your eligibility under this Plan ends), you are eligibleto receive a certificate showing the amount of time youwere covered.
Please call AmeriBen at 855-539-8678 to obtain acertificate.
Page 31
EXCLUSIONS AND LIMITATIONS (CON’T) CREDITABLE COVERAGEAn Insured Person whose coverage under priorCreditable Coverage ended no more than 90 days beforethe Insured Person’s effective date under the current Planwill have any applicable Pre-Existing Condition limitationreduced by the total number of days the Insured Personwas covered under such coverage. If there is a break inCreditable Coverage of more than 90 days, the Companywill credit only the days of such coverage under the break.
Creditable Coverage means benefits or coverageprovided under: 1) Medicare or Medicaid; 2) An employeewelfare benefit plan or group health insurance or healthbenefit plan; 3) An individual health benefit plan; 4) A statehealth benefits risk pool (including but not limited toCoverColorado); or 5) Chapter 55 of title 10 of the UnitedStates code, a medical care program of the federal Indianhealth service or tribal organization, a health plan offeredunder chapter 89 of title 5, United States code, a publichealth plan, or a health benefit plan under section 5(e) ofthe federal “Peace Corps Act”(U.S.C. sec. 2504(e)).
EXTENSION OF BENEFITSThe coverage provided under this policy ceases on theTermination Date. However, if an Insured is HospitalConfined on the Termination Date from a covered Injury orSickness for which benefits were paid before theTermination Date, Covered Medical Expenses for suchInjury or Sickness will continue to be paid as long as thecondition continues but not to exceed 90 days after theTermination Date. The total payments made in respect ofthe Insured for such condition both before and after theTermination Date will never exceed the Maximum Benefit.After this "Extension of Benefits" provision has beenexhausted, all benefits cease to exist, and under nocircumstances will further payments be made.
CONTINUATION OF COVERAGEAll Insured Persons who have been continuously insuredunder the school's regular student policy for at least 3consecutive months and who are no longer an EligiblePerson under the Policy, he or she has the right toexercise the option to continue coverage up to 3 monthsbeginning on the date coverage would otherwiseterminate. When an Insured Person chooses to exercisethis right, his or her written request and the appropriatepremium must be received by the Company (orauthorized representative) within 31 days following thedate coverage under the Policy terminates. In no eventwill this option to continue coverage be extended beyondthe number of months initially requested. Continuation ofCoverage will be subject to the terms and conditions ofthe Policy in effect on the date the Insured Personbecomes eligible under this option.
Covered Medical Expenses before payment of any benefitis made. The Deductible will apply as specified in theSchedule of Benefits.
Domestic Partner means a person who is neithermarried nor related by blood or marriage to the NamedInsured but who is: 1) the Named Insured’s sole spousalequivalent; 2) lives together with the Named Insured in thesame residence and intends to do so indefinitely; and 3)is responsible with the Named Insured for each other’swelfare; and 4) is the same sex as the Named Insured. Adomestic partner relationship may be demonstrated byany three of the following types of documentation: 1) ajoint mortgage or lease; 2) designation of the domesticpartner as beneficiary for life insurance; 3) designation ofthe domestic partner as primary beneficiary in the NamedInsured’s will; 4) domestic partnership agreement;5) powers of attorney for property and/or health care; and6) joint ownership of either a motor vehicle, checkingaccount or credit account.
Elective Surgery or Elective Treatment means thosehealth care services or supplies that do not meet thehealth care need for a Sickness or Injury. Elective Surgeryor Elective Treatment includes any service, treatment orsupplies that: 1) are deemed by the Company to beresearch or experimental; or 2) are not recognized andgenerally accepted medical practices in the UnitedStates.
Injury means bodily Injury which is all of the following: 1)directly and independently caused by specific accidentalcontact with another body or object; 2) unrelated to anypathological, functional, or structural disorder; 3) a sourceof loss; 4) treated by a Physician within 30 days after thedate of accident; and 5) sustained while the InsuredPerson is covered under this policy. All injuries sustainedin one accident, including all related conditions andrecurrent symptoms of these injuries will be consideredone Injury. Injury does not include loss which resultswholly or in part, directly or indirectly, from disease orother bodily infirmity. Covered Medical Expenses incurredas a result of an Injury that occurred prior to this policy’sEffective Date will be considered a Sickness under thispolicy.
Medical Emergency means the occurrence of asudden, serious and unexpected Sickness of Injury. In theabsence of immediate medical attention, a reasonableperson could believe the condition would result in any ofthe following: 1) Death; 2) Placement of the Insured’shealth in jeopardy; 3) Serious impairment of bodilyfunctions; 4) Serious dysfunction of any body organ or
Page 34
DEFINITIONS (CON’T)
The purpose of this medical insurance policy is to assistin the payment of medical bills. It is not intended that anInsured Person receive benefits greater than his/her totalallowable expenses. This plan will coordinate benefitswith any other valid and collectible insurance.
Benefits paid by the Master Policy will not exceed: 1) anyapplicable Policy maximums; and, 2) 100% of thecompensable expenses incurred when combined withbenefits paid by any Other Valid and CollectibleInsurance.
Medicare or MedicaidIf an Insured Person is eligible for Medicare or Medicaidbenefits, this plan may (or may not) be primary toMedicare or Medicaid. This is determined by Medicare orMedicaid regulations, as applicable. NOTE: THEHEALTH CENTER AT AURARIA IS NOT AMEDICARE OR MEDICAID PROVIDER.
DEFINITIONS
Coinsurance means a provision of the insurance bywhich the Insured Person and the insurance carrier sharein a specified ratio (e.g. 80% / 20%, 100% / 0%) for thepayment of hospital or medical expenses resulting from aSickness or Injury.
Copayment means a charge for Covered MedicalExpense which must be paid by the Insured Person.
Covered Medical Expenses means reasonable chargeswhich are: 1) not in excess of Usual and Customarycharges; 2) not in excess of the Preferred Allowancewhen the policy includes Preferred Provider benefits andthe charges are received from a Preferred Provider; 3) notin excess of the maximum benefit amount payable perservice as specified in the Schedule of benefits; 4) madefor services and supplies not excluded under the policy;
5) made for services and supplies which are a MedicalNecessity; 6) made for services included in the Scheduleof Benefits; and 7) in excess of the amount stated as aDeductible, if any.
Covered Medical Expenses will be deemed “incurred”only: 1) when the covered services are provided; and 2)when a charge is made to the Insured Person for suchservices.
Deductible means if an amount is stated in the Scheduleof Benefits or any endorsement to this policy as aDeductible, it shall mean an amount to be subtractedfrom the amount or an amount otherwise payable as
Page 33
COORDINATION OF BENEFITS

provide specific medical care at negotiated prices.Preferred Providers in your local school area arephysicians and hospitals who are participating membersof Cofinity.
The availability of specific providers is subject to changewithout notice. You should always confirm that aPreferred Provider is participating at the time services arerequired by calling Cofinity, for services in Colorado, at800-831-1166 toll-free or by checking the network’swebsite: www.cofinity.net and/or by asking the providerwhen you make an appointment for services. For servicesoutside the State of Colorado call First Health at 800-226-5116 toll-free or by checking the network’s website:www.myfirsthealth.com.
“Preferred Allowance” means the amount a PreferredProvider will accept as payment in full for CoveredMedical Expenses. “Out of Network” providers have notagreed to any prearranged fee schedules. You may incursignificant out-of-pocket expenses with these providers.Charges in excess of the insurance payment are yourresponsibility. Regardless of the provider, you areresponsible for the payment of your Deductible. You mustsatisfy your Deductible before benefits are paid. We willpay according to the benefit limits in the Schedule ofMedical Expense Benefits.
Sickness means sickness or disease of the InsuredPerson which causes loss, and originates while theInsured Person is covered under this policy. All relatedconditions and recurrent symptoms of the same or asimilar condition will be considered one sickness.Covered Medical Expenses incurred as a result of anInjury that occurred prior to this policy’s Effective Date willbe considered a sickness under this policy.
Usual and Customary Chargesmeans the lesser of theactual charge or a reasonable charge which is: 1) usualand customary when compared with the charges madefor similar services and supplies; and 2) made to personshaving similar medical conditions in the locality of thePolicyholder. The Company uses data from FAIR Health,Inc. to determine Usual and Customary Charges. Nopayment will be made under this policy for any expensesincurred which in the judgment of the Company are inexcess of Usual and Customary Charges.
Page 36
part; or 5) In the case of a pregnant woman, seriousjeopardy to the health of the fetus. Expenses incurred for“Medical Emergency” will be paid only for Sickness orInjury which fulfills the above conditions. These expenseswill not be paid for minor Injuries or minor Sicknesses.
Medical Necessity means those services or suppliesprovided or prescribed by a Hospital or Physician whichare all of the following: 1) Essential for the symptoms anddiagnosis or treatment of the Sickness or Injury; 2)Provided for the diagnosis, or the direct care andtreatment of the Sickness or Injury; 3) In accordance withthe standards of good medical practice; 4) Not primarilyfor the convenience of the Insured, or the Insured’sPhysician; and, 5) The most appropriate supply or level ofservice which can safely be provided to the Insured.
The Medical Necessity of being confined as an Inpatientmeans that both: 1) the Insured requires acute care as abed patient; and, 2) the Insured cannot receive safe andadequate care as an outpatient. This policy only providespayment for services, procedures and supplies which area Medical Necessity. No benefits will be paid for expenseswhich are determined not to be a Medical Necessity,including any or all days of Inpatient confinement.
Mental Illness means a Sickness that is a mental,emotional or behavioral disorder listed in the mentalhealth or psychiatric diagnostic categories in the currentDiagnostic and Statistical Manual of the AmericanPsychiatric Association. Mental Illness does not mean aBiologically Based Mental Illness or a Mental Disorder asdefined in the Benefits for Biologically Based MentalIllness. The fact that a disorder is listed in the Diagnosticand Statistical Manual of the American PsychiatricAssociation does not mean that treatment of the disorderis a Covered Medical Expense. If not excluded or definedelsewhere in the policy, all mental health or psychiatricdiagnoses are considered one Sickness.
Policy Year means a twelve (12) month period beginningeach Fall semester and specifically defined by theUniversity as the academic year.
Pre-existing Condition means any condition for whichan Insured Person: 1) incurred charges; 2) receivedmedical treatment; 3) consulted a health careprofessional; or 4) took Prescription Drugs within the 6months immediately prior to the Insured's Effective Dateunder this policy. “Pre-existing Condition” does notinclude pregnancy.
“Preferred Providers” are the Physicians Hospitals andother health care providers who have contracted to
Page 35
DEFINITIONS (CON’T)DEFINITIONS (CON’T)
3. The date(s) of service;4. The Provider’s name;5. The reason the claim should be reconsidered; and6. Any written comments, documents, records, or other
material relevant to the claim.
Please contact AmeriBen at 1-855-539-8678 with anyquestions regarding the Internal Appeal process. Thewritten request for an Internal Appeal should be sent to:AmeriBen, PO Box 7887, Boise, ID 83707.
Expedited Internal AppealFor Urgent Care Requests, an Insured Person or aDesignated Representative may submit a request, eitherorally or in writing, for an Expedited Internal Appeal of anAdverse Determination:
1. involving Urgent Care Requests; and2. related to a concurrent review Urgent Care Request
involving an admission, availability of care, continuedstay or health care service for an Insured Person whohas received emergency services, but has not beendischarged from a facility.
All necessary information, including the Company’sdecision, shall be transmitted to the Insured Person or aDesignated Representative via telephone, facsimile or themost expeditious method available. The Insured Personor the Designated Representative shall be notified of theEIR decision no more than seventy-two (72) hours afterthe Company’s receipt of the EIR request.
If the EIR request is related to a concurrent review UrgentCare Request, benefits for the service will continue untilthe Insured Person has been notified of the finaldetermination.
At the same time an Insured Person or a DesignatedRepresentative files an EIR request, the Insured Person orthe Designated Representative may file:
1. An Expedited External Review (EER) request if theInsured Person has a medical condition where thetimeframe for completion of an EIR would seriouslyjeopardize the life or health of the Insured Person orwould jeopardize the Insured Person’s ability to regainmaximum function; or
2. An Expedited Experimental or Investigational TreatmentExternal Review (EEIER) request if the AdverseDetermination involves a denial of coverage based onthe a determination that the recommended orrequested service or treatment is experimental orinvestigational and the Insured Person’s treating
Page 38Page 37
NOTICE OF APPEAL RIGHTS (CON’T)CLAIM SUBMISSIONSREQUIREMENTS/PROOF OF LOSS
DEADLINESYou have 90 days after the date of loss to furnish proof ofloss to AmeriBen. If you do not furnish notice of proofwithin the time allotted, your claim will still be consideredif you show that it was not reasonably possible to furnishthe notice of proof and that the notice of proof wasfurnished as soon as reasonably possible. Except forabsence of legal capacity, no claim for benefit will beaccepted after one year from date treatment wascompleted. AmeriBen and University of Colorado Denverreserve the right and opportunity to examine the personwhose Injury or Sickness is the basis of a claim as oftenas it may reasonably require during continuance of theclaim. No action at law or in equity shall be brought torecover on the Policy prior to the expiration of 60 daysafter proof of loss has been filed. Nor shall action bebrought at all unless brought within three years from theexpiration of the time within which proof of loss is requiredby the Policy. If any time limitation of the Policy withrespect to giving notice, filing proof of loss orcommencing an action at law or in equity is less thanpermitted by the law of the state in which you reside atthe time the Policy is issued, the limitation is herebyextended to agree with the minimum period permitted bysuch law.
NOTICE OF APPEAL RIGHTS
Right to Internal Appeal
Standard Internal AppealThe Insured Person has the right to request an InternalAppeal if the Insured Person disagrees with theCompany’s denial, in whole or in part, of a claim orrequest for benefits. The Insured Person, or the InsuredPerson’s Designated Representative, must submit awritten request for an Internal Appeal within 180 days ofreceiving a notice of the Company’s AdverseDetermination. In order to secure an Internal Review afterthe receipt of the notification of a benefit denied due to acontractual exclusion, the Insured Person must be able toprovide evidence from a medical professional that there isa reasonable medical basis that the policy exclusion doesnot apply to the denied benefit.
The written Internal Appeal request should include:
1. A statement specifically requesting an Internal Appealof the decision;
2. The Insured Person’s Name and ID number (from the IDcard);
Insured Person’s ability to regain maximum function;or
b. The Final Adverse Determination involves anadmission, availability of care, continued stay, orhealth care service for which the Insured Personreceived emergency services, but has not beendischarged from a facility.
The Insured Person or Insured Person’s DesignatedRepresentative’s request for an Expedited ExternalReview must include a Physician’s Certification that theInsured Person’s medical condition meets the above criteria.
An EER may not be provided for retrospective AdverseDeterminations or Final Adverse Determinations.
Where to Send External Review RequestsAll types of External Review requests shall be submittedto the Company at the following address:
Claims AppealsAmeriBenPO Box 7887Boise, ID 83707855-539-8678
Questions Regarding Appeal RightsContact AmeriBen at 855-539-8678 with questionsregarding the Insured Person’s rights to an Internal Appealand External Review.
PRIVACY POLICY
We know that your privacy is important to you and westrive to protect the confidentiality of your non-publicpersonal information. We do not disclose any nonpublicpersonal information about our customers or formercustomers to anyone, except as permitted or required bylaw. We believe we maintain appropriate physical,electronic and procedural safeguards to ensure thesecurity of your nonpublic personal information. You mayobtain a copy of UnitedHealthcare Insurance Company’sprivacy practices by calling them toll-free at 800-767-0700or visiting them at www.uhcsr.com.
Page 40
Physician certifies in writing that the recommended orrequested service or treatment would be significantlyless effective if not promptly initiated.
To request an Expedited Internal Appeal, please contactAmeriBen at 1-855-539-8678. The written request for anExpedited Internal Appeal should be sent to:ClaimsAppeals, AmeriBen, PO Box 7887, Boise, ID 83707.
Right to External Independent Review
After exhausting the Company’s Internal Appeal process,the Insured Person, or the Insured Person’s DesignatedRepresentative, has the right to request an ExternalIndependent Review when the service or treatment inquestion:
1. Is a Covered Medical Expense under the Policy; and2. Is not covered because it does not meet the
Company’s requirements for Medical Necessity,appropriateness, health care setting, level or care, oreffectiveness, or the treatment is determined to beexperimental or investigational.
Standard External ReviewA Standard External Review request must be submitted inwriting within 4 months of receiving a notice of theCompany’s Adverse Determination or Final AdverseDetermination.Expedited External ReviewAn Expedited External Review request may be submittedeither orally or in writing when:
1. The Insured Person or the Insured Person’s DesignatedRepresentative has received an Adverse Determination,anda. The Insured Person, or the Insured Person’s
Designated Representative, has submitted a requestfor an Expedited Internal Appeal; and
b. Adverse Determination involves a medical conditionfor which the time frame for completing anExpedited Internal Review would seriouslyjeopardize the life or health of the Insured Person orjeopardize the Insured Person’s ability to regainmaximum function; or
2. The Insured Person or the Insured Person’s DesignatedRepresentative has received a Final AdverseDetermination, anda. The Insured Person has a medical condition for
which the time frame for completing a StandardExternal Review would seriously jeopardize the life orhealth of the Insured Person or jeopardize the
Page 39
NOTICE OF APPEAL RIGHTS (CON’T) NOTICE OF APPEAL RIGHTS (CON’T)

Serv ices are a lso access ib le v ia e-mai l a [email protected] calling the FrontierMEDEX Operations Center,please be prepared to provide:1. Caller's name, telephone and (if possible) fax number,
and relationship to the patient;2. Patient's name, age, sex, and FrontierMEDEX ID
Number as listed on your Medical ID Card;3. Description of the patient's condition;4. Name, location, and telephone number of hospital, if
applicable;5. Name and telephone number of the attending
physician; and6. Information of where the physician can be immediately
reachedFrontierMEDEX is not travel or medical insurance but aservice provider for emergency medical assistanceservices. All medical costs incurred should be submittedto your health plan and are subject to the policy limits ofyour health coverage. All assistance services must bearranged and provided by FrontierMEDEX. Claims forreimbursement of services not provided byFrontierMEDEX will not be accepted. Please refer to theFrontierMEDEX information in MyAccount atwww.uhcsr.com/frontiermedex for additional information,including limitations and exclusions.
ACCIDENTAL DEATH ANDDISMEMBERMENT BENEFITS
Loss of Life, Limb or SightIf such Injury shall independently of all other causes andwithin 180 days from the date of Injury solely result in anyone of the following specific losses, the Insured Person orbeneficiary may request the Company to pay theapplicable amount below in addition to payment underthe Medical Expense Benefits.
For Loss Of:Life $5,000Two or More Members $5,000One Member $2,500Thumb or Index Finger $1,250
Member means hand, arm, foot, leg, or eye. Loss shallmean with regard to hands or arms and feet or legs,dismemberment by severance at or above the wrist orankle joint; with regard to eyes, entire and irrecoverableloss of sight. Only one specific loss (the greater) resultingfrom any one Injury will be paid.
Page 42Page 41
FRONTIERMEDEX: GLOBAL EMERGENCYSERVICES
FRONTIERMEDEX: GLOBAL EMERGENCYSERVICES (CON’T)
If you are a student insured with this insurance plan, youand your insured Spouse/Domestic Partner and minorchild(ren) are eligible for FrontierMEDEX. Therequirements to receive these services are as follows:International Students, insured Spouse/Domestic Partnerand insured minor child(ren): You are eligible to receiveFrontierMEDEX services worldwide, except in your homecountry.Domestic Students, insured Spouse/Domestic Partnerand insured minor child(ren): You are eligible forFrontierMEDEX services when 100 miles or more awayfrom your campus address and 100 miles or more awayfrom your permanent home address or while participatingin a Study Abroad program.FrontierMEDEX includes Emergency Medical Evacuationand Return of Mortal Remains that meet the US StateDepartment requirements. The Emergency MedicalEvacuation services are not meant to be used in lieu of orreplace local emergency services such as an ambulancerequested through emergency 911 telephone assistance.All services must be arranged and provided byFrontierMEDEX; any services not arranged byFrontierMEDEX will not be considered for payment.Key Services include:• Transfer of Insurance Information to Medical Providers• Monitoring of Treatment• Medication, Vaccine and Blood Transfers• Transfer of Medical Records• Dispatch of Doctors/Specialists• Worldwide Medical and Dental Referrals• Facilitation of Hospital Admission Payments• Emergency Medical Evacuation• Transportation After Stabilization• Transportation to Join a Hospitalized Participant• Emergency Travel Arrangements• Continuous Updates to Family and Home Physician• Replacement of Corrective Lenses and Medical Devices• Replacement of Lost or Stolen Travel Documents• Hotel Arrangements for Convalescence• Return of Dependent Children• Repatriation of Mortal Remains• Legal Referrals• Transfer of Funds• Message Transmittals• Translation ServicesPlease visit www.uhcsr.com/frontiermedex for theFrontierMEDEX brochure which includes servicedescriptions and program exclusions and limitations.To access services please call:(800) 527-0218 Toll-free within the United States(410) 453-6330 Collect outside the United States

Page 43
CLAIMS PROCEDURES
Written notice of any event that may lead to a claim underthe Policy must be given to the Company or its authorizedadministrator within 60 days after the event. Written proofof loss must be furnished to the Company within 90 daysafter the date of loss. Proper positive written notice andproof of loss must be given before the Company will beliable for any loss.
Send Medical Send Prescriptionclaims to: claims to:AmeriBen Express Scripts, Inc.PO Box 7887 P.O. Box 66583Boise, ID 83707 St. Louis, MO 63166-6583Group #0812014 Attn: Claims Department
800-206-4005
CLAIMS, ELIGIBILITY ANDBENEFIT QUESTIONS
AmeriBen855-539-8678
Website:http://ucdenver.ameriben.com
E-Mail inquiries at:[email protected]
PARTICIPATING PROVIDERORGANIZATIONS
COFINITY (Inside Colorado)Toll-Free Number for PPO Information 800-831-1166
www.cofinity.net
FIRST HEALTH NETWORK (Outside Colorado)Toll-Free Number for PPO Information 800-226-5116
www.myfirsthealth.com
HEALTH CARE MANAGEMENT PROGRAM
AmeriBen Compass Medical Management, Inc.For Pre-Admission Notification
800-388-3193
INSURANCE COMPANY
UnitedHealthcare Insurance CompanyForm Number: 12-BR-CO
Policy Number: 2013-202513-1






























