Embed Size (px)
Citation preview

Int. 1. Radiation Oncology Bid. Phys.. Vol 9, pp. 911-915 03~3016/83/060911~5503.00/0 Printed in the U.S.A. All rights rcscrvcd. Copyright 0 1983 Pergamon Press Ltd.
??Brief Communication
CURATIVE SURGERY FOR ADENOCARCINOMA OF THE PANCREAS/AMPULLA OF VATER: THE ROLE OF ADJUVANT PRE OR
POSTOPERATIVE RADIATION THERAPY
GENE KOPELSON, M.D.
Assistant Professor, Dept. of Therapeutic Radiology, Tufts University School of Medicine and Tufts-New England Medical Center, Boston MA 02111
From 1972 to 1981, 7 patients received a&vast external beam radiation therapy before (5 patients) or after (2 patients) a curative Whipple operation for adenocarcinoma of the pancreas (5 patients) or ampulla of Vater (2 patients). Via supervoltage, 4000-4520 rad/20-25 fractions/4-5 l/2 weeks were delivered to the tumor ked and draining lymphatics. Two patients (of 4 at risk) are Syear survivors; 3 are alive-without-disease at 1-2 years follow-up. Distant metastases have developed to date in 3 patients. A marginal miss occurred at the edge of a radiation portal in 1 patient, and no true in-field failures have occurred. Complications occurred in 2 patients. Because of the high incidence of local-regional failures after curative surgery alone for adenocarcinoma of the pancreas or ampulla of Vater, the above results suggest that adjuvant radiation therapy should he considered as a modality to potentially improve treatment results.
INTRODUCTION
Even after potentially curative surgery (i.e., Whipple operation or total pancreatectomy), 5-year survival rates for patients who survive the operation with adenocarci- noma of the pancreas or ampulla of Vater range from 3-18s 1.6.11.16.17 and 6_39%,‘0.” respectively. There has been little attention in the literature to the sites of tumor recurrence after radical surgery alone. Yet several recent analyses from the Massachusetts General Hospital found a high incidence of post-operative local-regional recur- rences for adenocarcinomas of the pancreas’ and ampulla of Vater.* Radiation therapy is a' regional modality in which postoperative adjuvant irradiation used after cura- tive surgery has been able to sterilize subclinical disease in ~90% of cases for adenocarcinomas of the rectum- rectosigmoid,7*9 sigmoid colon,’ uterus,’ ovary,‘* breast,” and lung.*
Thus the analogy to pancreatic adenocarcinoma is clear, and the present review was undertaken to assess the efficacy of the Whipple procedure coupled with adjuvant radiation therapy in an attempt to decrease the high regional recurrence rate after surgery alone and perhaps to improve survival.
METHODS AND MATERIALS
From 1972 to 1981, 7 patients at the Department of Therapeutic Radiology of the Tufts-New England Medi- cal Center received adjuvant radiation therapy pre- or
post-operatively in conjunction with a Whipple operation for adenocarcinoma of the pancreas or ampulla of Vater. Patients with initially unresectable disease were excluded as were those patients who were given preoperative irra- diation in an attempt to convert the lesion to being resectable.14 Patients with gross residual or microscopic residual (i.e., positive margins) disease are excluded, as are patients with potentially-resectable lesions in whom medical contraindications precluded radical surgery and in whom radical irradiation was given.
There were 4 women and 3 men; their age at diagnosis ranged from 45-72 years (median 57). Each patient had an adenocarcinoma (cystadenocarcinomas were ex- cluded). A summary of the clinical courses appear in Tables 1 and 2.
Of the 5 patients irradiated preoperatively (Table l), initial exploration revealed small-to-moderate sized lesions of the pancreatic head or ampulla of Vater. There was no radiographic nor palpable evidence of vessel fixation or other evidence of surgical unresectability. The one initially un-explored patient had small adenocarci- noma of the ampulla of Vater diagnosed at endoscopic retrograde cholangio-pancreatography (although at final pathology the origin of the tumor was felt to be in the pancreatic head). Biliary-enteric anastamoses were accomplished, and the patients were then irradiated prior to definitive surgery.
Supervoltage (@‘Co-l patient, 45MV X rays-4
Reprint requests to: Dr. G. Kopelson, Dept: of Radiation Oncology, Salem Hospital, 81 Highland Ave., Salem, MA 01970. Acknowledgements-The author would like to thank Mindy
and Barry Printz-Kopelson for their help in the preparation of this manuscript.
Accepted for publication 20 January 1983.
911
Tabl
e 1.
Pre
oper
ativ
e ad
juva
nt
radi
atio
n th
erap
y
Pt. n
o.
Site
Initi
al e
xplo
ratio
n R
adia
tion
deta
ils
Size
/Ext
ent
PKX
XdU
r~
Fiel
ds
Rad
/Fxn
/El
da
ys
Rad
iatio
n-&
post
Surg
ery
inte
rval
R
adia
tion
cour
se
Path
olog
y
Tum
or
Nod
es
Com
plic
atio
ns
Surv
ival
Fa
ilure
site
(s)
I P
3.5
x 4
cm;
inv
Ch-
J A
P-PA
44
00/2
2/30
4.
5 w
k.
“Tum
or s
hrun
k”
No
chan
ge (
mod
. diff
. N
eg.
Obs
truct
ed
Ch-
J: b
iliar
y-cc
- 8m
Pe
riton
eal
duod
enum
, C
BD
ad
encc
a)
Ioni
c fis
tula
se
edin
g 2
P 4x
5cm
C
h-J
AP-
PA
4500
/23/
39
3 w
k.
No
Cha
nge
Ung
rade
d ad
enoc
a.
Neg
. N
one
ly2m
Li
ver
3 P
4x6c
m
Chd
-J
4-fie
ld
4500
/25/
35
6.5
wk.
“M
arke
d 1”
N
o re
sidu
al t
umor
N
eg.
Non
e sly
3m
Non
e (p
rior
poor
ly d
iff.
aden
oca.
) 4
P’
“waln
ut”
Non
e*
AP-
PA
4ooo
/20/
26
4 w
k.
“Mar
ked
1”
Wel
l diff
. ade
noca
. N
eg.
Smal
l bo
wel
obs
truct
ion;
7y
3m
Mar
gina
l [C
hd-J
,G-J
] m
argi
nal
stom
ach
ulce
r re
curr
ence
5
AV
3c
m
Chd
-J,
G-J
A
P-PA
40
00/2
0/26
5
wk.
N
o C
hang
e M
od d
iff. a
deno
ca.
Neg
. N
one
sgy7
m
Non
e
P -
Panc
reas
; A
V -
A
mpu
lla o
f V
ater
; A
denc
ca.
- A
deno
carc
inom
a;
CL-
J -
Cho
lecy
stoj
ejun
osto
my;
C
hd-J
-
Cho
ledo
choj
ejun
osto
my;
H
pJ
- H
epat
iwje
juno
stom
y;
G-J
-
Gas
troje
jum
stom
y;
AP-
PA
_ A
nter
ior-
Post
erio
r pa
ralle
l-opp
c6ed
; >
- pa
tient
stil
l aliv
e.
*Dia
gnos
is m
ade
endo
scop
ical
ly;
tum
or f
elt t
o ar
ise
in p
ancr
eas
at f
inal
pat
holo
gy
(see
text
).
Tabl
e 2.
Pos
tope
rativ
e ad
juva
nt
radi
atio
n th
erap
y
Initi
al s
urge
ry
Rad
iatio
n de
tails
Su
rger
y-to
-radi
atio
n Pt
. no.
Si
te
Proc
edur
es
Size
/Ext
ent
Nod
es
Gra
de
inte
rval
Fi
elds
R
ad/F
sn/E
l da
ys
Com
plic
atio
ns
Surv
ival
Fa
ilure
site
s
6 P
HpJ
G
-J
2 cm
/inv.
pe
ripan
crea
tic
fat,
116
Pas.
Wel
l dilT
. 2.
5 m
o.
AP-
PA
4500
/25/
40
Non
e =-
2Y
Non
e du
oden
um a
nd p
ylor
ic
aden
oca.
sp
hinc
ter
7 A
V
Chd
-J G
-J
Inv.
hea
d pa
ncre
as a
nd
Neg
. M
od. d
itT.
2 m
o.
AP-
PA
4520
/24/
36
Non
e >l
Y
Non
e du
oden
um
adcn
oca.
Sam
e ab
brev
iatio
ns a
s in
Tab
le I
.
Surgery for adenocarcinoma of pancreas/ampulla of vater 0 G. KOPELSON 913
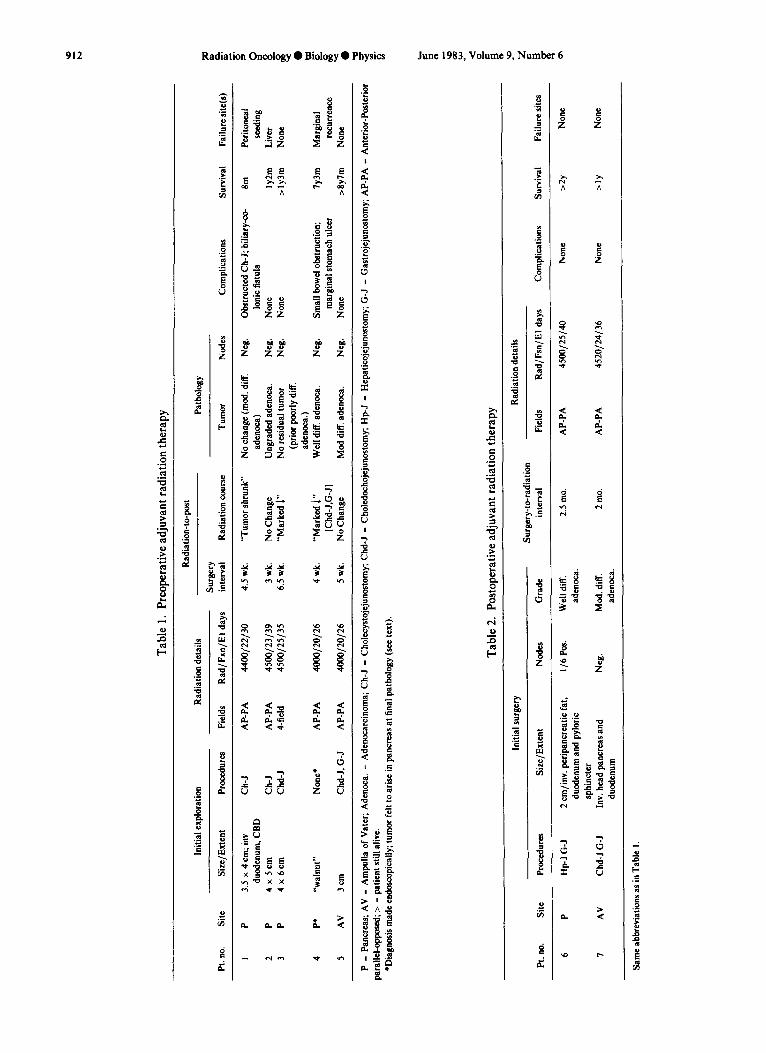
patients) was used to irradiate the primary tumor (in the ampulla, or in the pancreati’c head), areas of probable microscopic involvement such as pancreatic body and draining pancreaticoduodenal, celiac axis, and porta hepatis lymph nodes. The pancreatic tail, splenic hilum, and the lateral suprapancreatic nodes were not included because of efforts to maximize sparing of left renal parenchyma. Irradiation dose-time factors appear in Table 1. At the subsequent Whipple procedure (Table l), there was marked tumor shrinkage noted in 3/5 patients. Fibrosis causing a lengthy operation was found in one patient in whom there was a 6.5 week interval between the end of irradiation and surgery. All patients irradiated preoperatively had negative lymph nodes at final patholo- gY*
For the 2 patients irradiated postoperatively (Table 2), similar field sizes and doses were used as described above and in Table 1.
No patient received adjuvant chemotherapy. Survival was calculated from date of surgery.
RESULTS
Of 4 patients at risk, 2 were 5-year survivors. The 3 other patients are alive without disease at l-2 years follow-up. Distant disease developed in Patients No. 1, 2, and 4. There were no true in-field post-irradiation recur- rences, although a marginal miss occurred in Patient No. 4 (Fig. 1). One of 4 patients irradiated preoperatively for carcinoma of the pancreas (No. 3) showed no residual tumor.
Two patients to date have experienced complications. In Patient No. 1, the cholecystojejunostomy became obstructed postoperatively necessitating revision; unfor- tunately shortly thereafter a biliary-colonic fistula devel- oped and the patient died. No patient died of complica- tions resulting from the initial surgical procedures. In Patient No. 4, subsequent small bowel obstruction neces- sitated lysis of adhesions, and a marginal stomach ulcer was managed successfully conservatively. Thus the known complication rate to date is 2 of 7.
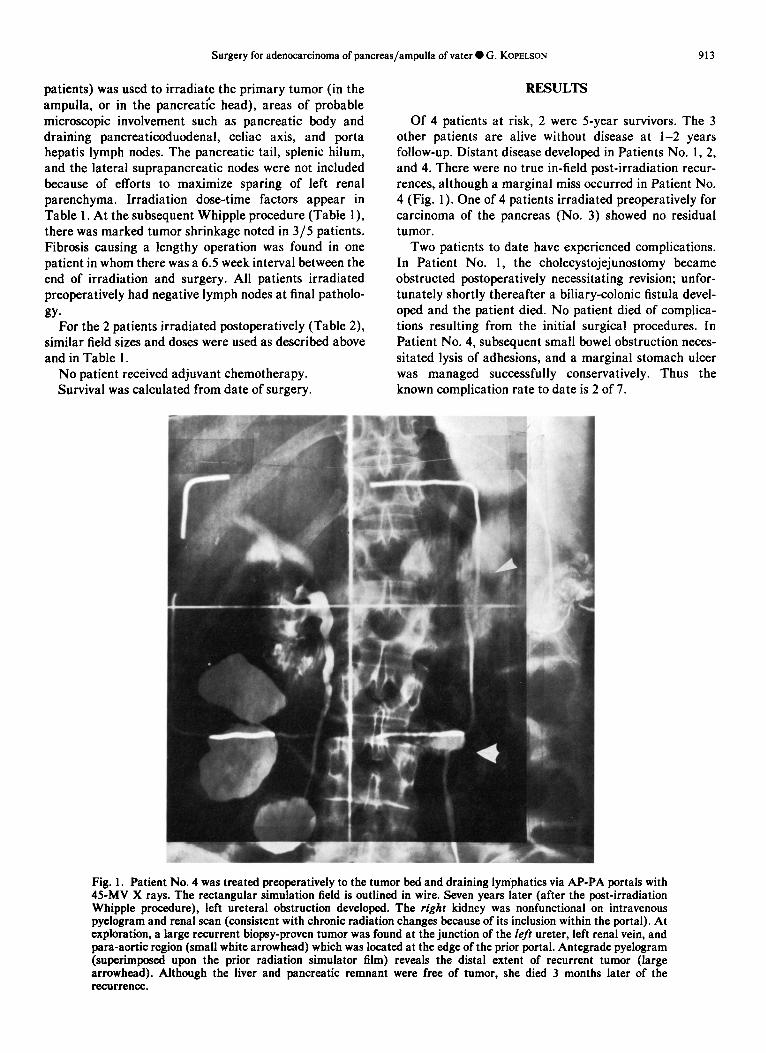
Fig. 1. Patient No. 4 was treated preoperatively to the tumor bed and draining lymphatics via AP-PA portals with 45MV X rays. The rectangular simulation field is outlined in wire. Seven years later (after the post-irradiation Whipple procedure), left ureteral obstruction developed. The right kidney was nonfunctional on intravenous pyelogram and renal scan (consistent with chronic radiation changes because of its inclusion within the portal). At exploration, a large recurrent biopsy-proven tumor was found at the junction of the left ureter, left renal vein, and para-aortic region (small white arrowhead) which was located at the edge of the prior portal. Antegrade pyelogram (superimposed upon the prior radiation simulator film) reveals the distal extent of recurrent tumor (large arrowhead). Although the liver and pancreatic remnant were free of tumor, she died 3 months later of the recurrence.

914 Radiation Oncology 0 Biology ??Physics June 1983, Volume 9, Number 6
DISCUSSION Although there has been much discussion in the litera-
ture as to the intent of surgery (i.e., curative vs palliative) and the choice of operation (i.e., Whipple procedure vs total pancreatectomy vs bypass alone) for patients with apparently localized carcinoma of the pancreas/periam- pullary region,‘*6~“*‘6~‘7 overall survival remains extremely poor as noted in the Introduction.
For carcinomas of the pancreas, at the Massachusetts General Hospital Tepper et ~1.‘~ found a minimum local regional failure rate of 50% after curative surgery, which was unrelated to tumor size or nodal involvement. In a series from Memorial Hospital, approximately ‘/3 of patients had positive regional nodes (microscopically) beyond the resected area (e.g., peripancreatic nodes around the pancreatic body), which were potentially encompassable within a regional irradiation fie1d.3 Simi- larly, investigators from the Peter Bent Brigham Hospital found similar microscopic involvement of the common duct or body or tail of the pancreas.” In the Memorial series, lesions of the pancreatic head (locations which are usually considered for a Whipple procedure) did not appear to involve peripancreatic nodes located at the pancreatic tail.
of the Whipple procedure. Indeed, the one anastamotic complication (Patient No. 1) [a similar incidence to surgery-alone series ‘*6*‘o*“~‘6*‘7] suggests that biliary- enteric or enteroenteric or gastro-enteric anastamoses may be constructed successfully after preoperative irra- diation and may tolerate postoperative irradiation to 4500 rad. The extensive fibrosis which was found at surgery (performed 6.5 weeks after preoperative irradiation) in Patient No. 3 suggest that a 4-5 week interval might be preferred.
Although survival results are better for lesions of the ampulla of Vater after curvative surgery,“,” at the Mas- sachusetts Genera1 Hospital, Kopelson et al.” found a 57% local-regional failure rate at that institution after curative surgery alone, and an even higher rate of 80% from 4 other series in the literature that had reported sites of postoperative recurrences.
The present series suggests that by the inclusion in a radiation portal of the tumor bed and draining unresected lymphatic regions (porta hepatis, celiac axis, peripan- creatic, some pancreaticoduodenal), that no in-field regional recurrences have occurred to date compared to a much higher incidence that would have been anticipated from the above surgery-alone series.‘0*‘6 The 5-year sur- vival of 2 of 4 patients at risk is encouraging. However, the occurrence of one marginal miss (Fig. 1) suggests that a more generous infero-lateral border to encompass more of the pancreatic body/tail (while maximizing left renal sparing) might be done in the future, possibly with shaped multiple fields as described by Shipley et al.” and Gun- derson.’
The relative advantages and disadvantages of preoper- ative vs postoperative adjuvant irradiation in this setting are discussed by Tepper et ~1.‘~ Practically, to avoid a second exploration, postoperative irradiation would be the most commonly used sequence. There is very sparse data on such adjuvant irradiation in pancreas/peri-ampullary carcinomas. In a follow-up series from the Massachusetts Genera1 Hospital, Shipley et al.” reported on 10 patients who had a Whipple procedure, 9 of whom survived the operation. Of this latter group of 9, 6 did not have adjuvant postoperative irradiation and 4/6 developed local-regional failure (confirming the prior report from the same hospital by Tepper et a1.16). Of the 3 postopera- tive survivors who received postoperative adjuvant irra- diation, ‘/J failed local-regionally, although the authors did not state whether this was a marginal recurrence or in-field failure. Nguyen et ~1.‘~ reported a small series of patients with carcinoma of the pancreas or ampulla of Vater who were irradiated primarily (9 patients) or adjuvantly after a Whipple procedure (9 patients). Although the median survival for the latter postoperative patients was 13 months for lesions of the head of the pancreas and was 17 months for lesions of the ampulla, unfortunately, detailed results of sites of failure and complications were not described for those patients irra- diated adjuvantly postoperatively (i.e. after the Whipple operation).
The relatively low complication rate and 0% peri- operative mortality rate (Patient No. 1 died after a second operation) are certainly comparable to surgery-alone series,‘*6*‘0v”*‘6*‘7 which have spanned this time period. In fact the data in Tables l-2 suggest that 4500 rad/ 180-200 rad fractions to the upper abdomen can be potentially well-tolerated, even when added to the rigors
It should be emphasized that the present study is a small, nonrandomized, retrospective analysis. The con- tinuing occurrence of distant failures suggests that adju- vant chemotherapy may be another alternative modality to improve results of surgery-alone series, or that com- bined adjuvant chemotherapy-radiation therapy be con- sidered. The point of the present paper is to suggest no increased patient morbidity/mortality when adjuvant external beam irradiation is added to a Whipple opera- tion, and that improved regional disease control rates and survival may occur also. These findings deserve consider- ation for a prospective randomized study; the Gastroin- testinal Tumor Study Group did such a study although results have not been published to date.
REFERENCES 1. Brooks, J.R.: Operative approach to pancreatic carcinoma.
Semin. Oncol. 6: 357-367,1978. 2. Choi, N.C.H., Grille, H.C., Scannell, J.G., Wilkins, E.W.,
Jr.: Basis for new strategies in postoperative radiotherapy of bronchogenic carcinoma. Znt. J. Radiat. Oncol. Biol. Phys. 6: 3l-35,198O.
Surgery for adenocarcinoma of pancreas/ampulla of vater 0 G. KOPELSON 915
3.
4.
5.
6.
7.
8.
9.
10.
Cubilla, A.L., Fortner, J.G., Fitzgerald, P.J.: Lymph node involvement in carcinoma of the head of the pancreas. Cancer 41: 880-887,1978. Goodman, R., Hellman, S.: The role of postoperative irra- diation in carcinoma of the endometrium. Gynecol. Oncol. 2: 354-361,1974. Gunderson, L.L.: Radiation oncology. In Alimentary Tract Radiology, Vol. III, Margolis, A.R., Burhenne, H.J. (Eds.). St. Louis, CV Mosby. 1979, pp. 593-619. Hermann, R.E., Cooperman, A.M.: Current concepts in cancer-Cancer of the pancreas. N. Engl. J. Med. 301: 482485, 1979. Hoskins, B., Gunderson, L.L., Dosoretz, D., Galdabini, J.: Adjuvant postoperative radiotherapy for cancer of the rectum and rectosigmoid (Abstr.). Int. J. Radiat. Oncol. Biol. Phys. 6: 1380, 1980. Kopelson, G.: Adjuvant postoperative radiation therapy for colorectal carcinoma above the peritoneal reflection: I. Sigmoid colon. Cancer (In press). Kopelson, G.: Long-term survivors after adjuvant pelvic irradiation in rectal and sigmoid carcinoma: An assessment of late results. J. Surg. Oncol. (In press). Kopelson, G., Galdabini, J., Warshaw, A.L., Gunderson, L.L.: Patterns of failure after curative surgery for extra- hepatic biliary tract carcinoma: Implications for adjuvant
11.
12.
13.
14.
15.
16.
17.
18.
therapy. Int. J. Radiat. Oncol. Biol. Phys. 7: 413-417, 1981. Longmire, W.P., Jr., Traverso, L.W.: The Whipple proce- dure and other standard operative approaches to pancreatic cancer. Cancer 47: 1706-l 7 11,198 1. Mauch, P.M., Ehrman, R.L., Griffiths, C.T., Marck, A., Knapp, R.C., Leverne, M.B.: Radiation therapy in Stage II ovarian carcinoma. Cancer 45: 1344-l 35 1, 1980. Nguyen, T.D., Bugat, R., Combes, P.F.: Postoperative irradiation of carcinoma of the head of the pancreas area. Cancer 50: 53-56,1982. Pilepich, M.V., Miller, H.H.: Pre-operative irradiation in carcinoma of the pancreas. Cancer 46: 1945-l 949, 1980. Shipley, W.U., Nardi, G.L., Cohen, A.M., Ling, CC.: Iodine-125 implant and external beam irradiation in patients with localized pancreatic carcinoma. Cancer 45: 709-714,198O. Tepper, J.E., Nardi, G.L., Suit, H.D.: Carcinoma of the pancreas: Review of MGH experience from 1963-1973. Cancer37: 1519-1524, 1975. Tryka, A.F., Brooks, J.R.: Histopathology in the evaluation of total pancreatectomy for ductal carcinoma. Ann. Surg. 190: 373-381,1979. Weichselbaum, R.R., Marck, A., Hellman, S.: The role of postoperative irradiation in carcinoma of the breast. Cancer 37: 2682-2690,1976.



![Indikationen für die Abrechnung der Pauschalen für ... · 8 Bösartige Neubildungen der Verdauungsorgane2_15 C24.1 Bösartige Neubildung: Ampulla hepatopancreatica [Ampulla Vateri]](https://img.pdfslide.net/doc/110x75/5e04fd523baf0e25b840bc29/indikationen-fr-die-abrechnung-der-pauschalen-fr-8-bsartige-neubildungen.jpg)

























