Embed Size (px)
Citation preview
CV risk in the Elderly Dr David Milne
Helping to keep patients out of hospital: Prevention, early diagnosis and improved patient outcomes
Session 1 - 6th Nov 2016 PCCJ Conference
Declaration of Interests I have accepted remuneration for writing articles, chairing
meetings, giving presentations and sponsorship for attending medical meetings from Servier pharmaceuticals, MSD, Schering-Plough AstraZeneca, Sanofi-aventis and Bristol Myers Squibb. I have been on advisory boards for GE Healthcare and Schering-Plough.
This presentation is not promotional and is not intended to recommend any particular medications
Dr David Milne MA FRCP DRCOG
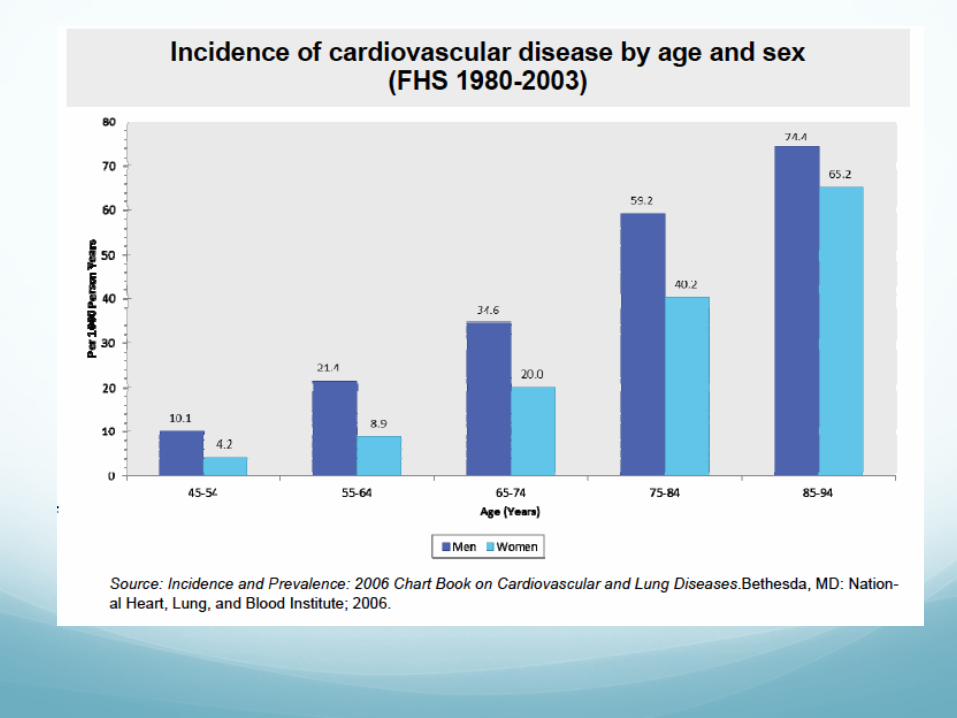
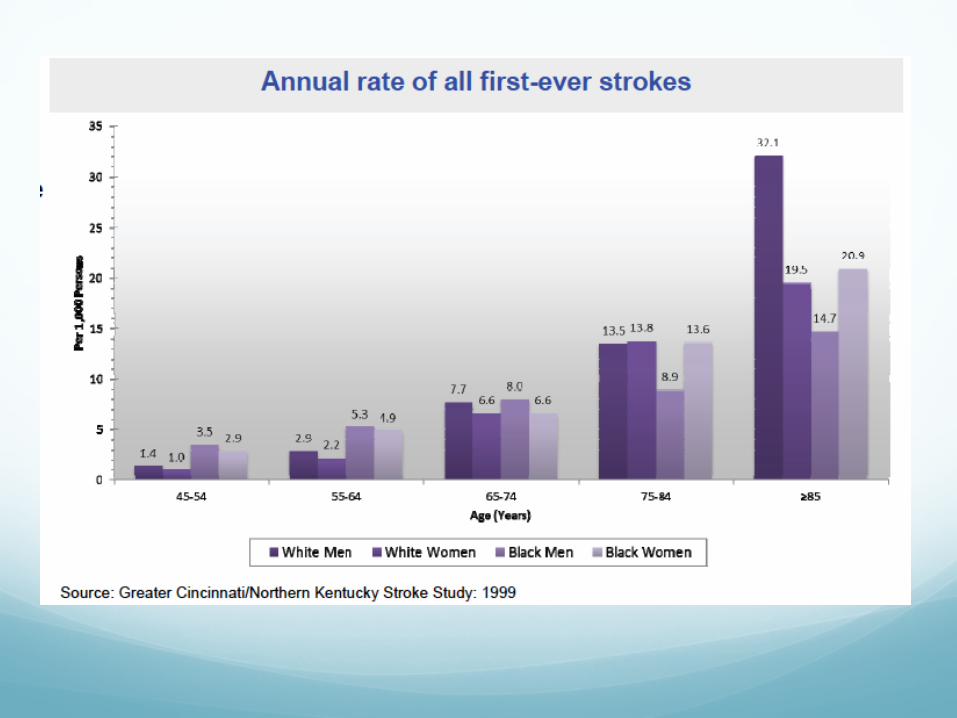
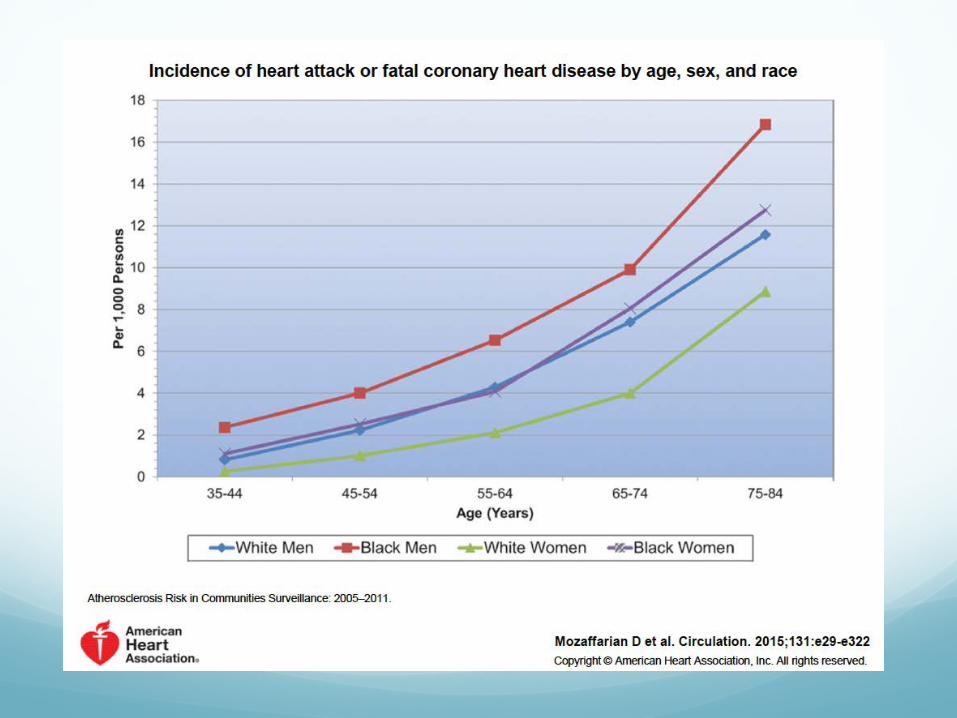
The Problem Cardiovascular diseases are degenerative in nature
Increased incidence and prevalence in older adults
Common cause of morbidity and mortality – and therefore of hospitalisation
Therapeutic nihilism in patient and clinician
Are we
“Saving a patient for Cancer”
Professor A Polak
Risk Factors for CV Disease Smoking
Hypertension
Cholesterol
AF
Diabetes
Obesity
Inactivity
Problems of advising elderly patients on evidence
Trial data often does not include elderly patients
Extrapolation from benefit in younger patients is not necessarily correct
Trial patients are often atypical Even if they are elderly they rarely have the multiple co-
morbidities typical in our patients No co- prescription of multiple medications
Trials are often funded by pharmaceutical companies and designed to show a particular benefit – possible systematic bias

Who is at risk? The Usual Suspects
Those known to the clinicians – on treatments and with “Previous”
The New Recruits
Healthy and with little previous contact with medical services
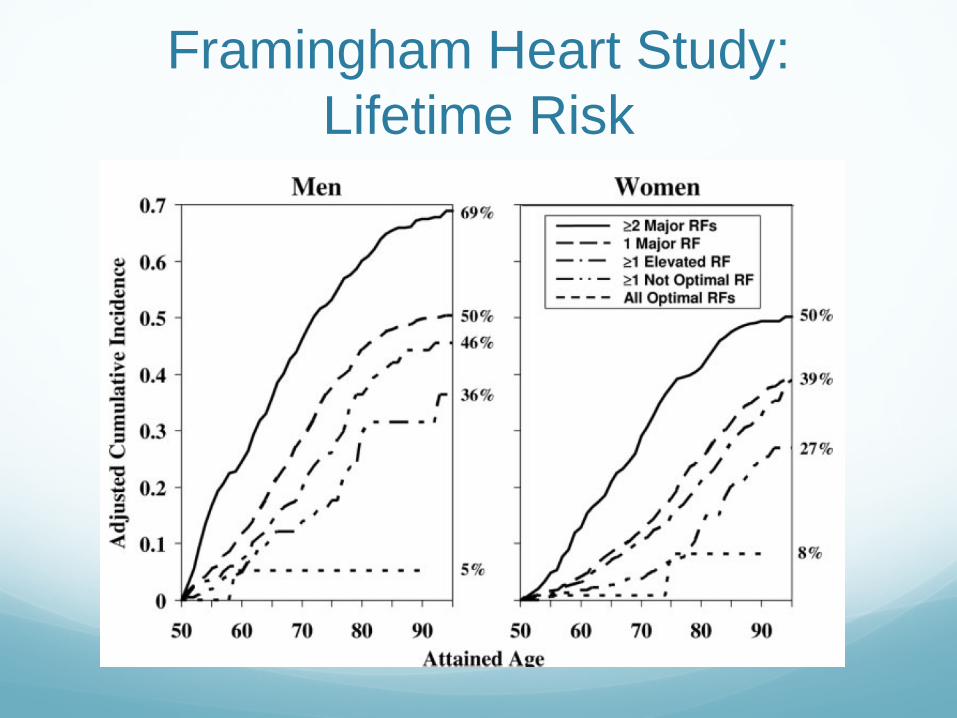
Framingham Heart Study: Lifetime Risk
At 50 years of age the absence of any major risk factors for CVD is associated with a very low lifetime risk and markedly longer survival
But - 2 or more major risk factors at 50 68.9% lifetime risk in men 50.2% lifetime risk in women
Lloyd-Jones et al. Circulation 2006, 113; 791 - 798
Framingham Heart Study: Lifetime Risk
Challenges Population ageing is unprecedented,
without parallel in the history of humanity. Increases in the proportions of older persons (60 years or older) are being accompanied by declines in the proportions of the young (under age 15) such that by 2050, the proportion of older persons will have risen from 15% today to 25%.
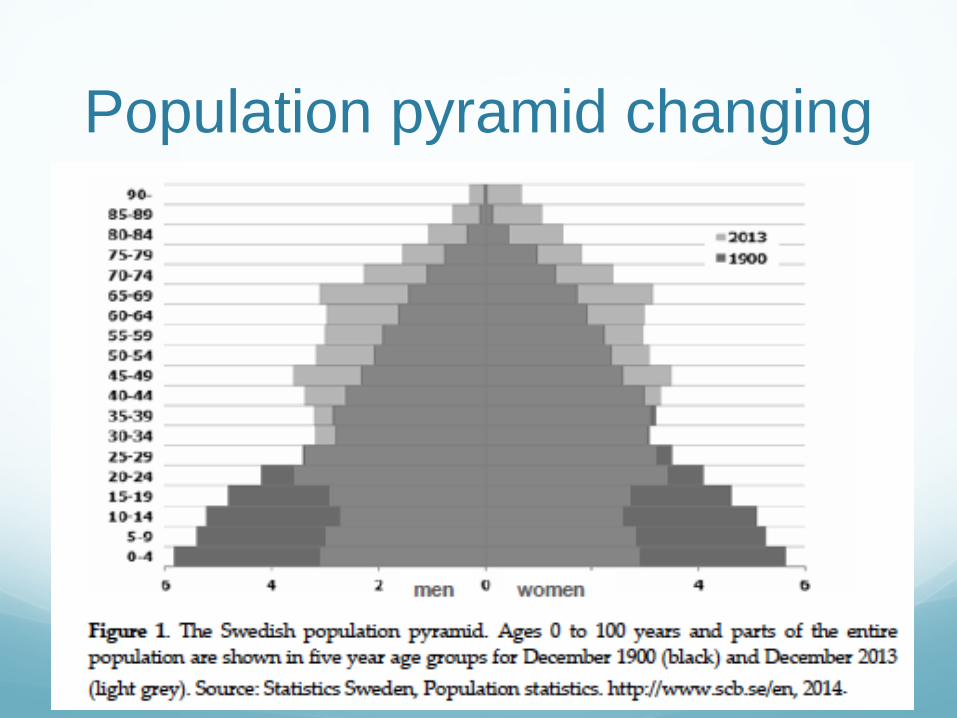
Population pyramid changing
CV Risks
Smoking More than 1 in every 10
cardiovascular deaths in the world in the year 2000 were attributable to smoking, demonstrating that it is an important preventable cause of cardiovascular mortality
The tobacco epidemic is one of the biggest public health threats the world has ever faced, killing around 6 million people a year
Ezzati M, Henley SJ, Thun MJ, Lopez AD: Role of smoking in global and regional cardiovascular mortality. Circulation 2005, 112(4):489-497.
THE WHO –Tobacco Fact sheet N°339Updated July 2015

Getting them to stop? Ask Bev!
Why do some smokers live a long life?
It’s in their genes
A Genetic Network Associated With Stress Resistance, Longevity, and Cancer in Humans ME Levine & EM Crimmins J Gerontol A Biol Sci Med Sci (2015) doi: 10.1093/gerona/glv141 First published online: September 9, 2015
• Using long-lived smokers as a phenotype a genome-wide association study comparing them to smokers at ages 52–69.
• Results were used to identify single nucleotide polymorphisms that collectively related to smokers’ longevity.
• Identified a set of 215 single nucleotide polymorphisms that were located within genes making-up a functional interaction network.
• Found to be significantly associated with a 22% increase in the likelihood of being aged 90–99 (n = 253) and an over threefold increase in the likelihood of being a centenarian
Hypertension Older people have
Increased arterial stiffness with decreased blood vessel distensibility,
Increased thickness of the intima media and endothelial dysfunction
But also
Baroreceptors become insensitive and requires a large blood pressure change to compensatory raise the heart frequency and thus an increased risk for hypotension and decreased cerebral perfusion
The HYpertension in the
Very Elderly Trial N. Beckett, R. Peters, A. Fletcher, C. Bulpitt
on behalf of the HYVET committees and investigators
ClinicalTrials.gov: NCT00122811
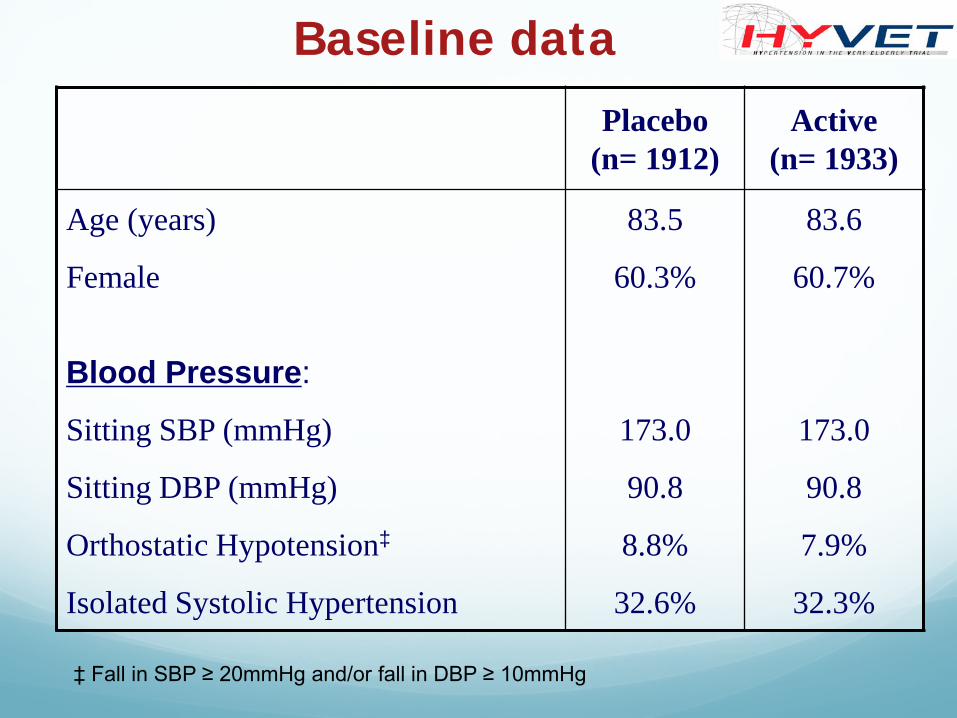
Placebo (n= 1912)
Active (n= 1933)
Age (years) 83.5 83.6
Female 60.3% 60.7%
Blood Pressure:
Sitting SBP (mmHg) 173.0 173.0
Sitting DBP (mmHg) 90.8 90.8
Orthostatic Hypotension‡ 8.8% 7.9%
Isolated Systolic Hypertension 32.6% 32.3%
Baseline data
‡ Fall in SBP ≥ 20mmHg and/or fall in DBP ≥ 10mmHg
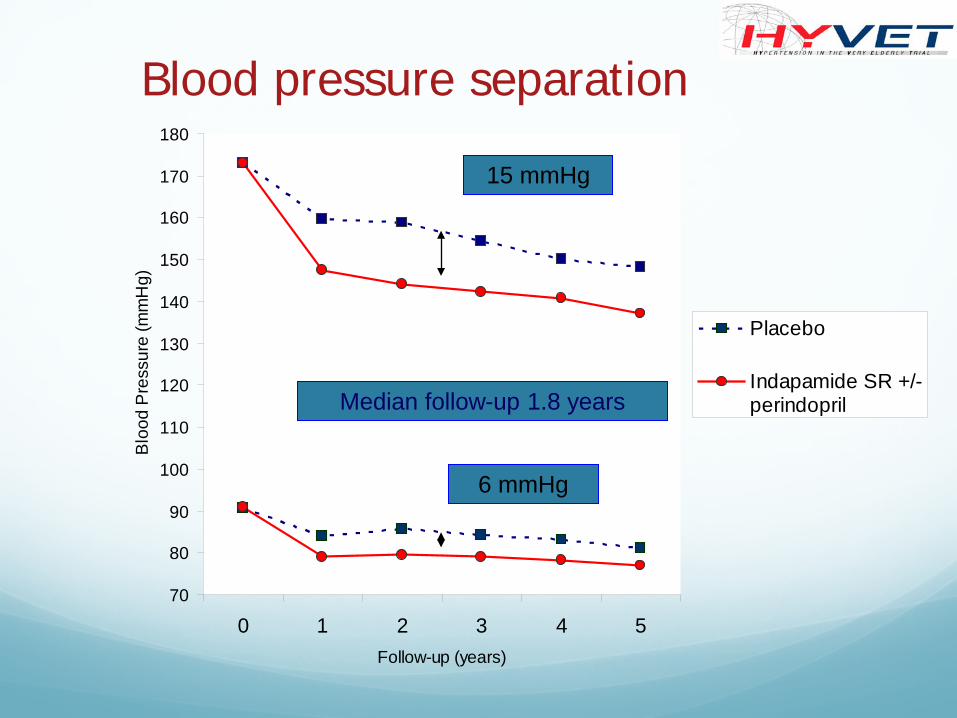
Blood pressure separation
70
80
90
100
110
120
130
140
150
160
170
180
0 1 2 3 4 5Follow-up (years)
Blo
od P
ress
ure
(mm
Hg)
Placebo
Indapamide SR +/-perindoprilIMedian follow-up 1.8 years
15 mmHg
6 mmHg
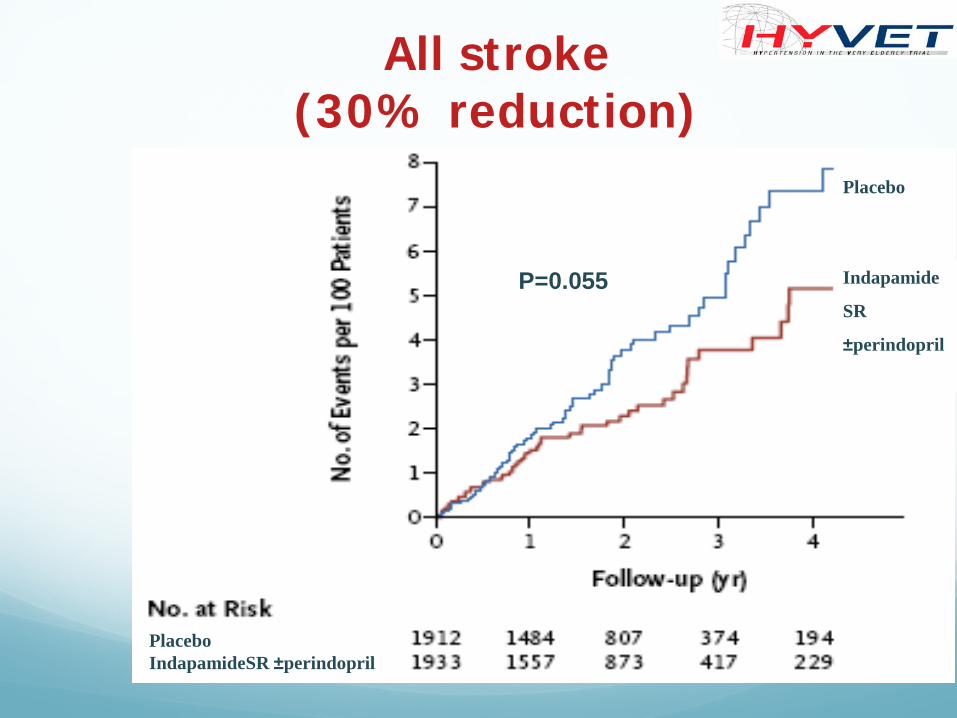
All stroke (30% reduction)
Placebo IndapamideSR ±perindopril
Indapamide
SR
±perindopril
Placebo
P=0.055
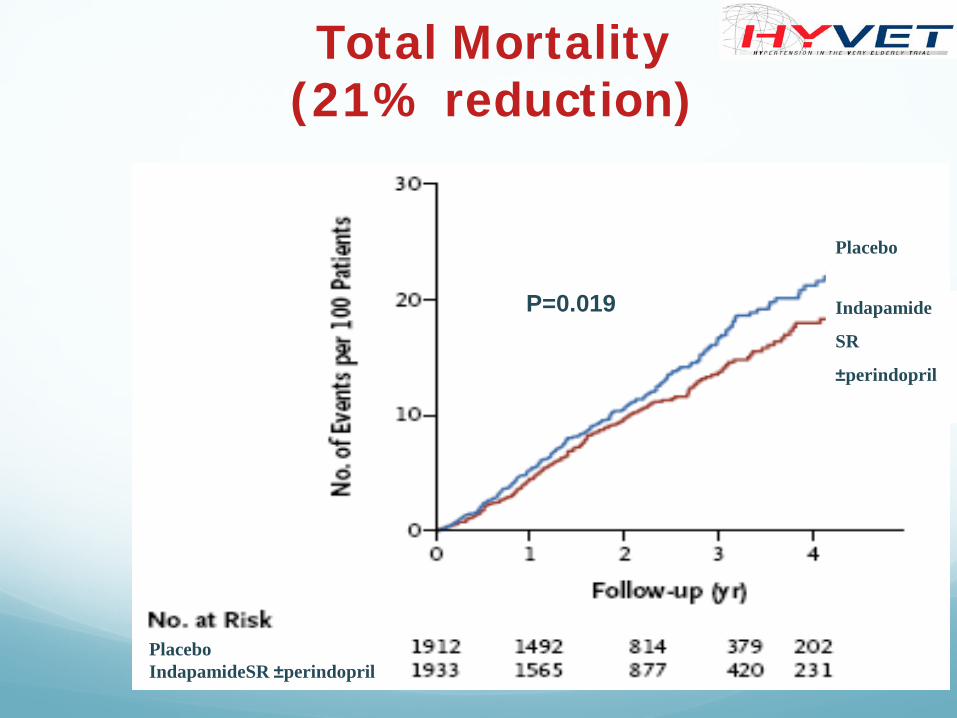
Total Mortality (21% reduction)
Placebo
Indapamide
SR
±perindopril
P=0.019
Placebo IndapamideSR ±perindopril
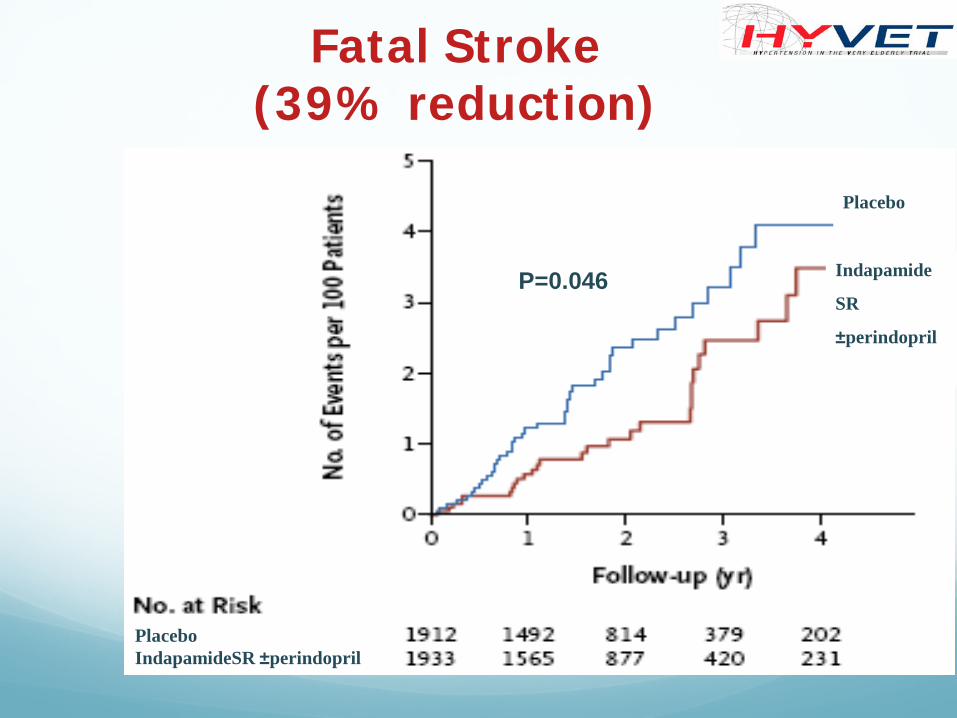
Fatal Stroke (39% reduction)
Indapamide
SR
±perindopril
Placebo
P=0.046
Placebo IndapamideSR ±perindopril
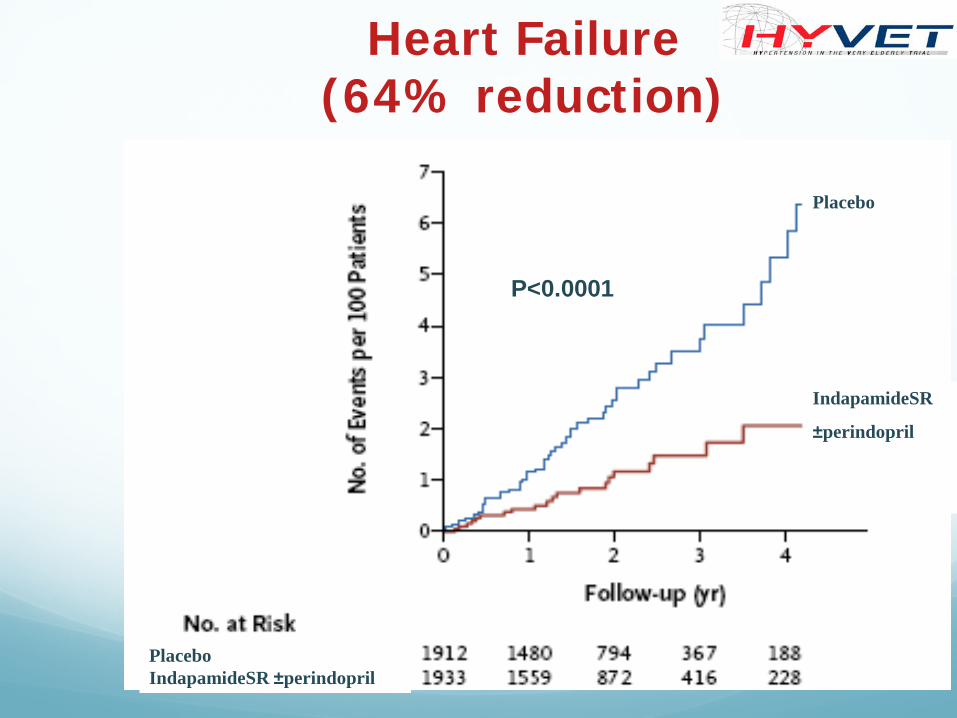
Heart Failure (64% reduction)
P<0.0001
Placebo
IndapamideSR
±perindopril
Placebo IndapamideSR ±perindopril
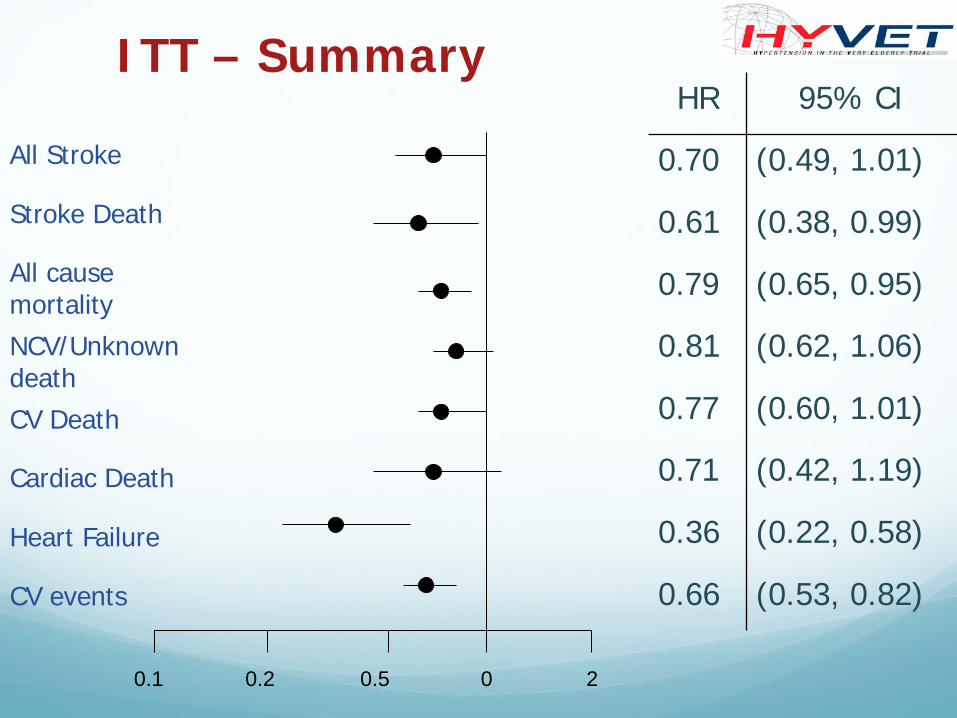
0 2 0.5 0.2 0.1
HR 95% CI
0.70 (0.49, 1.01)
0.61 (0.38, 0.99)
0.79 (0.65, 0.95)
0.81 (0.62, 1.06)
0.77 (0.60, 1.01)
0.71 (0.42, 1.19)
0.36 (0.22, 0.58)
0.66 (0.53, 0.82)
All Stroke
Stroke Death
All cause mortality NCV/Unknown death CV Death
Cardiac Death
Heart Failure
CV events
ITT – Summary
HYVET extension Very elderly patients with hypertension may gain
immediate benefit from treatment. Sustained differences in reductions of total mortality and cardiovascular mortality reinforce the benefits and support the need for early and long term treatment.
Immediate and late benefits of treating very elderly people with hypertension: results from active treatment extension to Hypertension in the Very Elderly randomised controlled trial – Beckett et al BMJ 2012;344:d7541 doi: 10.1136/bmj.d7541
Cholesterol NICE Guideline CG 181 Sept 2014
The UK population is ageing and atherosclerosis is an age-associated process. Few trials assessing cardiovascular outcomes have recruited many people older than 80 years yet the important effect of age on CVD risk suggests that all people in this group should be offered statin therapy. However, there is no evidence to validate the CVD benefits and side effects of statin therapy such as effect on muscle and renal function in this age group.
Cholesterol Secondary prevention
Statins are most beneficial for preventing cardiovascular events in patients who already have CHD.
A meta-analysis of patients with existing disease (aged 65–82 years) found that all-cause mortality was significantly lower with statins than with placebo (15.6% vs 18.7%) over five years. This equates to a number needed to treat of 28 over five years to save one life. Approximately 25% of patients in the trials were female. Frail older patients may have been excluded because of
comorbidity or organ dysfunction.
Statins for secondary prevention in elderly patients: a hierarchical bayesian meta-analysis. Afilalo J1, Duque G, Steele R, Jukema JW, de Craen AJ, Eisenberg MJ. J Am Coll Cardiol. 2008 Jan 1;51(1):37-45.

Cholesterol
The role of statins in primary prevention of cardiovascular disease in older people is less clear. Their effects seem to increase over five years, with only minimal benefits over placebo seen in the first year. It is therefore important to consider the patient's probable lifespan when deciding whether to start or continue a statin.
Studies of secondary prevention in patients with cerebrovascular disease suggest that statins are associated with a decrease in recurrent ischaemic stroke but an increase in haemorrhagic stroke.
Baigent C, Keech A, Kearney PM, Blackwell L, Buck G, Pollicino C, et al. Efficacy and safety of cholesterol-lowering treatment: prospective meta-analysis of data from 90,056 participants in 14 randomised trials of statins. Lancet 2005;366:1267-78.
Cholesterol Epidemiological studies suggest that the relative risk for coronary heart
disease associated with high cholesterol decreases with age.
Significant benefits have been demonstrated from lipid lowering to reduce cardiovascular morbidity and mortality.
Lowering serum cholesterol by
1 mmol/l reduces risk of coronary
heart disease mortality by 50% in
people aged 40-49 years,
risk reduction is 33% in those aged
50-69 years and 15% in those aged 70-89 years.
Corti MC, Guralnik JM, Salive ME, et al. Clarifying the direct relation between total cholesterol levels and death from coronary heart disease in older persons. Ann Intern Med 1997; 126: 753-60.
Dosing In older adults, exposure to higher doses of statins or
higher potency statins does not increase their effectiveness, but does increase the risk of adverse effects such as myopathy and cognitive impairment, and concordance!!
With ageing, there is a decrease in body size, particularly in muscle mass and in hepatic and renal function, so the same dose will result in a greater degree of exposure in older people.
Statin therapy in older people
Statins are most beneficial for preventing cardiovascular events in people who already have coronary heart disease and reduce vascular events and mortality.
Statins are associated with a decrease in recurrent ischaemic stroke but an increase in haemorrhagic stroke in secondary prevention in people with cerebrovascular disease.
Their efficacy in primary prevention of CVD in older people is unclear with one study suggesting an increase in effect over 5 years, with only minimal benefits over placebo in the first year.
Hilmer S, Gnjidic D. Statins in older adults. Aust Prescr 2013; 36: 79-82. Afilalo J, Duque G, Steele R, et al. Statins for secondary prevention in elderly patients: a hierarchical Bayesian meta-analysis. J Am Coll Cardiol 2008; 51: 37-45. Baigent C, Keech A, Kearney PM, et al. Efficacy and safety of cholesterol lowering treatment: prospective meta-analysis of data from 90,056 participants in 14 randomised trials of statins. Lancet 2005; 366: 1267-78.
When to stop Statins should be discontinued when the potential benefits
are no longer clinically relevant.
People with severe physical or cognitive impairments, or those in their last year of life, therapeutic aims often change from preventative to palliative and reducing the risk of vascular events or mortality may not be relevant.
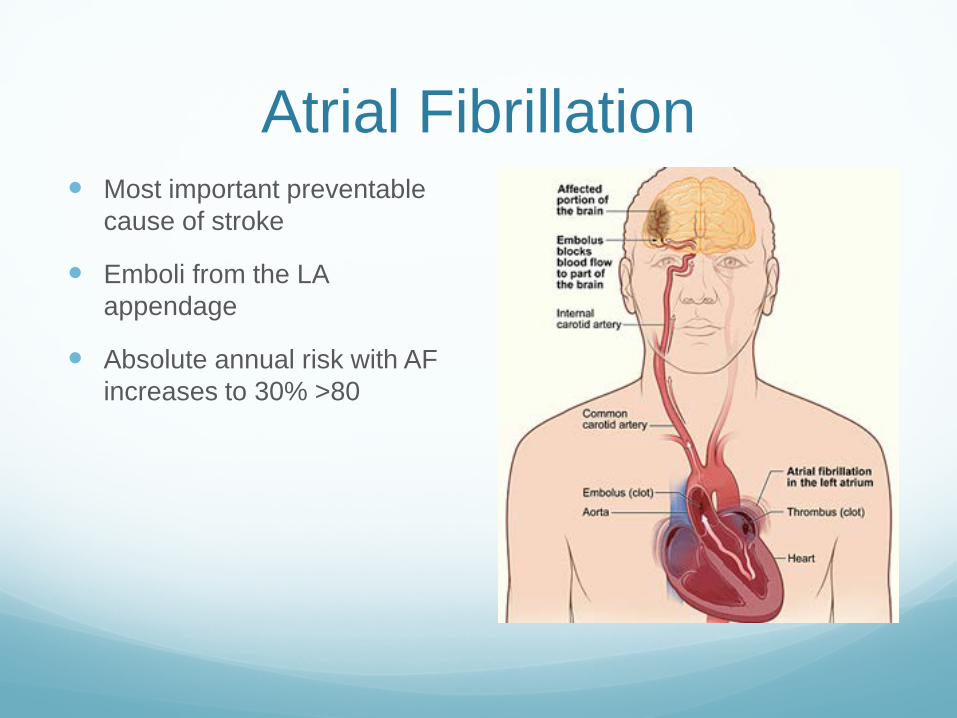
Atrial Fibrillation Most important preventable
cause of stroke
Emboli from the LA appendage
Absolute annual risk with AF increases to 30% >80
Header ATRIAL FIBRILLATION Predisposing Factors
Hypertension Coronary heart disease Pulmonary disease Excess alcohol intake Surgery Rheumatic heart disease (esp mitral stenosis) Dilated or hypertrophic cardiomyopathy Mitral valve prolapse Hyperthyroidism
80%
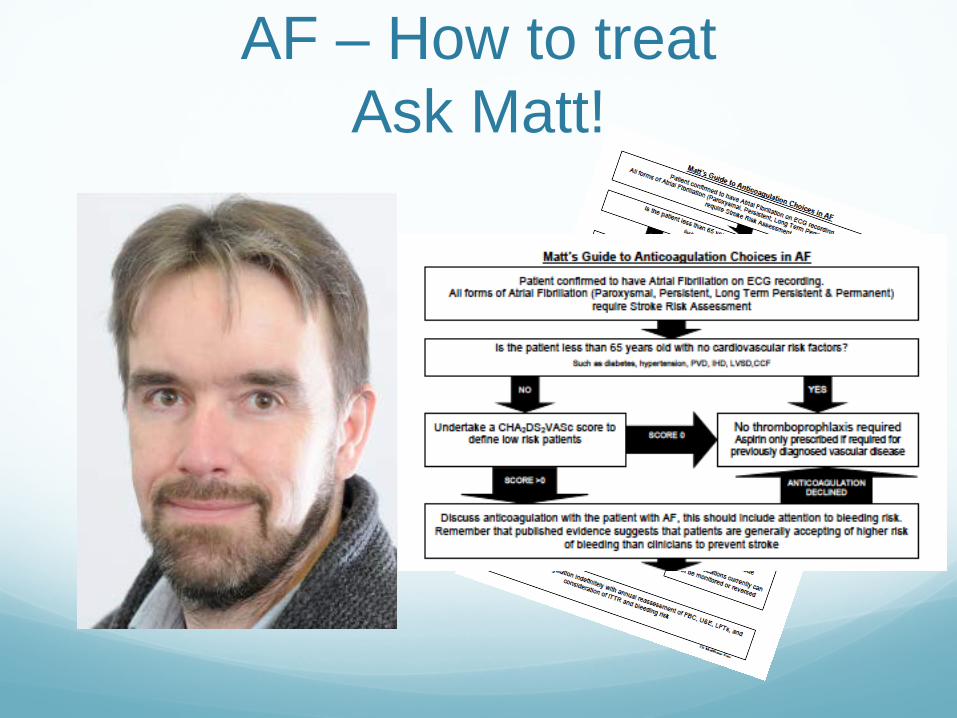
AF – How to treat Ask Matt!
Diabetes Prevalence of type 2 diabetes of 10-20% in those
aged 60-79 years
But diabetes in ageing populations is characterized by:
Complexity of illness
Increased risk of medical comorbidities
Early development of functional decline and risk of frailty.
Risk Assessment Assessment of cardiovascular risk in older people with
diabetes is difficult as most risk assessment tools do not extrapolate beyond age 65 yrs.
The Framingham risk score has been validated for people up to 75 yrs but unreliable in older persons.
This, coupled with the fact that the combined presence of diabetes and older age automatically place these people at high cardiovascular risk
Therefore risk assessment using predictive tools is not necessary.
de Ruijter W, Westendorp RGJ, Assendelft WJJ. Use of Framingham risk score and new biomarkers to predict cardiovascular mortality in older people: population based observational cohort study. BMJ 2009; 338: a3083.
The evidence base and bottom line recommendations for the treatment of glucose, blood pressure, and lipids in older people with
diabetes.
The evidence is increasing that blood pressure and lipid reduction have specific benefits in older people with diabetes > 70 years
The evidence for tight glucose control is not available and may be counterproductive!
Recent studies are suggesting that a higher target HbA1c range may be more appropriate and safer.
Hypertension Hypertension is a common comorbidity in
people with diabetes being 1.5 to three times more common than in those without diabetes.
Most (60-80%) people with type 2 diabetes die of cardiovascular complications
75% of specific cardiovascular complications have been attributed to hypertension
Hypertensive people with diabetes are also at increased risk for diabetes-specific complications including nephropathy and retinopathy.
Sowers JR, Epstein M. Diabetes mellitus and associated hypertension, vascular disease, and nephropathy. An update. Hypertension 1995; 26: 869-79. Schall P, Wehling M. Treatment of arterial hypertension in the very elderly: a meta-analysis of clinical trials. Arzneimittelforschung 2011; 61: 221-8.
BP Target 140/90 In the absence of randomized clinical trials data, the
generally recommended target blood pressure target for older people with diabetes is less than 140/90 mmHg.
ACCORD trial people > 65 years of age found no additional benefit of a target systolic pressure less than 120 mmHg compared with a target of 140 mmHg
Potential harm associated with low on-treatment blood pressure as suggested by the ACCORD
Observational data from an extended follow-up of the predominantly elderly INVEST Study diabetes cohort suggest an increase in mortality when on-treatment SBP is less than 115 mmHg or DBP is less than 65 mmHg.
Beckett NS, Peters R, Fletcher AE, et al. Treatment of hypertension in patients 80 years of age or older. N Engl J Med 2008; 358: 188798. 142. Bulpitt CJ, Beckett NS, Cooke J, et al. Results of the pilot study for the Hypertension in the Very Elderly Trial. J Hypertens 2003; 21: 2409-17. 143. Beckett N, Peters R, Tuomilehto J, et al. Immediate and late benefits of treating very elderly people with hypertension: results from active treatment extension to Hypertension in the Very Elderly randomised controlled trial. BMJ; 344: d7541.
Stroke Patients with diabetes have:
1.5 - 3 fold increase in risk of stroke and it doubles the risk of stroke recurrence (ischaemic more than haemorrhagic)
Worse stroke outcomes, functional and neurologic
More neurologic and functional disability
Diabetic people with metabolic syndrome have an inflated risk of stroke
Canadian Stroke Network and the Heart and Stroke Foundation of Canada. Canadian best practice recommendations for stroke care. CMAJ 2008;179:E1-E93.Lehto et al (1996
Prescribing in older people Requires additional knowledge of age-associated changes in
pathophysiology, pharmacokinetics, and pharmacodynamics, use of multiple medicines, and drug to drug interactions and this adds to the challenges of managing diabetes in this older population.
Drug metabolism is affected by:
decline in renal and hepatic functions
lower lean body mass
pharmacodynamic changes = increased sensitivity to medicines.
Identification of risk factors for hypoglycaemia is important in view of the high vulnerability of older people to this complication of therapy, particularly those with frailty, under-nutrition, or dementia
Turnheim K. Drug therapy in the elderly. Exp Gerontol 2004; 39: 1731-8.
Prescribing in older people The altered pharmacokinetics and pharmacodynamics
associated with ageing require:
starting at lower doses and avoiding maximum doses of therapeutic agents.
The relative contribution of postprandial glucose is higher compared with fasting glucose in older people
agents which preferentially lower post prandial hyperglycaemia glucose may be more effective in achieving glycaemic goals without increasing the risk of fasting hypoglycaemia.
Conclusions The elderly and the very elderly are an increasing
proportion of the population
CVD are an age related group of conditions
Interventions around traditional risk factors have benefits – some immediate, some delayed
Benefits may be less marked, side effects more common
Start investing in your arteries now!