Embed Size (px)
Citation preview

356
One in 7 patients suffers a major complication or death after coronary artery bypass graft surgery (CABG),1
and available cardiac surgery risk scores are often not able to identify these patients in advance. Identification of high-risk patients and subsequent tailoring of the revascularization strategy and postoperative management may be aided by an assessment of cardiac structure and function, such as by echocardiography. However, risk scores encompass very few echocardiographic parameters; the Society of Thoracic Surgeons (STS) risk score1 includes left ventricular ejection fraction (LVEF) and significant valvular regurgitation or
stenosis, whereas the EuroSCORE2 includes LVEF and pulmonary arterial hypertension.
Clinical Perspective on p 364
Professional society guidelines have limited comments on the practice of routine preoperative echocardiography; as a result, there is significant variability among practitioners and institutions. The 2011 American College of Cardiology (ACC)/American Heart Association (AHA) CABG Guidelines3 do not provide specific recommendations for preoperative echocar-diography, whereas the preceding 2004 Guidelines4 listed it as
Background—Although echocardiography is commonly performed before coronary artery bypass surgery, there has yet to be a study examining the incremental prognostic value of a complete echocardiogram.
Methods and Results—Patients undergoing isolated coronary artery bypass surgery at 2 hospitals were divided into derivation and validation cohorts. A panel of quantitative echocardiographic parameters was measured. Clinical variables were extracted from the Society of Thoracic Surgeons database. The primary outcome was in-hospital mortality or major morbidity, and the secondary outcome was long-term all-cause mortality. The derivation cohort consisted of 667 patients with a mean age of 67.2±11.1 years and 22.8% females. The following echocardiographic parameters were found to be optimal predictors of mortality or major morbidity: severe diastolic dysfunction, as evidenced by restrictive filling (odds ratio, 2.96; 95% confidence interval, 1.59-5.49), right ventricular dysfunction, as evidenced by fractional area change <35% (odds ratio, 3.03; 95% confidence interval, 1.28-7.20), or myocardial performance index >0.40 (odds ratio, 1.89; 95% confidence interval, 1.13-3.15). These results were confirmed in the validation cohort of 187 patients. When added to the Society of Thoracic Surgeons risk score, the echocardiographic parameters resulted in a net improvement in model discrimination and reclassification with a change in c-statistic from 0.68 to 0.73 and an integrated discrimination improvement of 5.9% (95% confidence interval, 2.8%-8.9%). In the Cox proportional hazards model, right ventricular dysfunction and pulmonary hypertension were independently predictive of mortality over 3.2 years of follow-up.
Conclusions—Preoperative echocardiography, in particular right ventricular dysfunction and restrictive left ventricular filling, provides incremental prognostic value in identifying patients at higher risk of mortality or major morbidity after coronary artery bypass surgery. (Circulation. 2013;127:356-364.)
Key Words: coronary artery bypass ■ echocardiography ■ outcome assessment (health care) ■ surgery ■ ventricular function, right
© 2012 American Heart Association, Inc.
Circulation is available at http://circ.ahajournals.org DOI: 10.1161/CIRCULATIONAHA.112.127639
Received June 28, 2012; accepted November 9, 2012.From the Cardiac Ultrasound Laboratory, Division of Cardiology (J.A., A.W.F., C.C., M.H.P.), the Division of Cardiac Surgery (A.K.A., D.M.S.), and
the Department of Surgery and Center for Quality and Safety (D.M.S.), Massachusetts General Hospital, Harvard University, Boston, MA; and the Cardiac Ultrasound Laboratory, Division of Cardiology (J.A., A.S., L.G.R.), and the Division of Cardiac Surgery (J.-F.M.), Jewish General Hospital, McGill University, Montreal, QC.
The online-only Data Supplement is available with this article at http://circ.ahajournals.org/lookup/suppl/doi:10.1161/CIRCULATIONAHA. 112.127639/-/DC1.
Correspondence to Jonathan Afilalo, MD, MSc, Massachusetts General Hospital, 55 Fruit Street, Yawkey 5E, Boston, MA 02114. E-mail [email protected]
Incremental Value of the Preoperative Echocardiogram to Predict Mortality and Major Morbidity in Coronary
Artery Bypass SurgeryJonathan Afilalo, MD, MSc; Aidan W. Flynn, MD, PhD; Avi Shimony, MD; Lawrence G. Rudski, MD; Arvind K. Agnihotri, MD; Jean-Francois Morin, MD; Cristina Castrillo, MD; David M. Shahian, MD;
Michael H. Picard, MD
7,31,36,100
Imaging
by guest on May 24, 2018
http://circ.ahajournals.org/D
ownloaded from
by guest on M
ay 24, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on May 24, 2018
http://circ.ahajournals.org/D
ownloaded from
by guest on M
ay 24, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on May 24, 2018
http://circ.ahajournals.org/D
ownloaded from
by guest on M
ay 24, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on May 24, 2018
http://circ.ahajournals.org/D
ownloaded from
by guest on M
ay 24, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on May 24, 2018
http://circ.ahajournals.org/D
ownloaded from

Afilalo et al Echocardiography Before Coronary Bypass Surgery 357
a level IIb recommendation (usefulness less well established) in a limited subset of patients with recent anterior myocar-dial infarction. Furthermore, the 2011 ACC/AHA/American Society of Echocardiography (ASE) Appropriateness Criteria5 provide recommendations for echocardiography before non-cardiac surgery but do not address echocardiography before CABG.
No previous studies thoroughly evaluated the prognostic information that can be gained from a comprehensive preop-erative echocardiogram. Such a study would demonstrate the independent value of each parameter, and the incremental value of the echocardiogram as a whole when added to traditional risk scores. With this new information, guideline committees would have a stronger evidence base on which to justify more definitive recommendations. Given this context, the objective of this study was to identify echocardiographic predictors of mortality and major morbidity in patients undergoing isolated CABG, and to determine the incremental prognostic value of the echocardiogram in addition to traditional risk scores.
MethodsStudy DesignA cohort of patients undergoing isolated CABG at 2 university hos-pitals in the United States and Canada between 2007 and 2011 was assembled. Preoperative echocardiograms were reviewed to test the hypothesis that echocardiographic parameters would add incre-mental value above traditional cardiac surgery risk scores to predict postoperative mortality or major morbidity. A comprehensive echo-cardiographic panel was measured in the derivation cohort to iden-tify optimal parameters, and subsequently verified in the validation cohort.
SettingThe derivation cohort consisted of consecutive patients who under-went isolated CABG at the Massachusetts General Hospital between January 1, 2007 and December 31, 2009. The validation cohort con-sisted of consecutive patients who underwent isolated CABG at the Jewish General Hospital between September 1, 2010 and July 11, 2011. Patients in both cohorts were followed from the time of their index admission to hospital discharge; additionally, patients in the derivation cohort were followed forward for vital status up to July 1, 2011.
ParticipantsThe inclusion criteria were as follows: (1) isolated CABG defined as coronary artery bypass surgery without concomitant repair or replacement of the heart valves or great vessels, and (2) preopera-tive transthoracic echocardiogram performed at the study center ≤30 days before surgery. Because echocardiographic images were reana-lyzed for the purpose of this study, patients were excluded if they only had echocardiographic reports from an outside center or if their digital echocardiographic images could not be retrieved for technical reasons.
Predictor VariablesA comprehensive list of quantitative parameters of left- and right-sided chamber size, geometry, systolic and diastolic function, and valvular function were measured from the preoperative echocardiogram. The echocardiographic protocol and normal reference limits adhered to the guidelines of the American Society of Echocardiography.6–10 Right and left atrial areas were measured at end-systole in the apical 4-cham-ber view; left atrial height was also measured to calculate left atrial volume using the single-plane area-length method. Right ventricular (RV) area was measured at end-diastole and end-systole in the apical
4-chamber view, and fractional area change (FAC) was calculated as follows: [RV end-diastolic area – RV end-systolic area] / [RV end-diastolic area]. Tricuspid valve closure to opening time was measured by continuous wave Doppler of the tricuspid regurgitation or pulsed Doppler of the tricuspid inflow. Pulmonic ejection time was measured by pulsed Doppler of the distal RV outflow tract. RV myocardial performance index (MPI), an index of RV efficiency reflecting both systolic and diastolic function, was calculated as follows: [Tricuspid valve closure opening time – Pulmonic ejection time] / [Pulmonic ejection time]. Pulmonary artery systolic pressure (PASP) was mea-sured by continuous wave Doppler of the tricuspid regurgitation with 10 mm Hg added for right atrial pressure. LVEF and volumes were measured using the biplane Simpson method. Left ventricular (LV) mass was measured using the Devereux method. LV diastolic func-tion was assessed using a multi-parametric approach including pulsed Doppler of the mitral and pulmonary vein inflow, tissue Doppler of the medial and lateral annulus, and left atrial volume. Valvular regur-gitation and stenosis were assessed using a multi-parametric approach as reported by the echocardiography reader, including mean and peak gradients, color Doppler jet appearance, vena contracta, and proximal isovelocity shell area (PISA) where applicable.
Measurements were performed in duplicate by 2 independent echo-cardiography readers (J.A., A.F., C.C., A.S.), and arbitrated by a third senior reader (M.H.P., L.G.R.). All readers were cardiologists trained in echocardiography. To ensure accuracy and consistency of measure-ment techniques, readers participated in focused training sessions and quality audits throughout the study. Readers were blinded to the clini-cal data and outcomes when interpreting the echocardiograms.
Outcome VariablesThe primary outcome was a composite of in-hospital mortality or major morbidity defined according to the STS data definitions as any 1 of the following: all-cause death, stroke, renal failure, prolonged ventilation, deep sternal wound infection, or need for reoperation.11 The secondary outcome was long-term all-cause mortality defined as death from any cause occurring from the time of cardiac surgery to the end of follow-up. There were no patients lost to follow-up for the primary or secondary outcomes.
Data SourcesEchocardiographic measurements were performed on the digital echo-cardiographic images stored on dedicated servers. Echocardiograms were performed with the Philips IE33, Sonos 7500, or GE Vivid 7 machines and analyzed on the Xcelera workstation (Philips Medical Systems, Andover, MA) at the derivation site, and with the GE Vivid 7 machine and EchoPAC workstation (GE, Milwaukee, WI) at the validation site. Clinical data, including in-hospital outcomes, were ex-tracted according to the STS Adult Cardiac Surgery Database. Vital status was extracted from the Social Security Death Index by way of the Research Patient Data Registry (Partners Healthcare, Boston, MA).
Study SizeAssuming a baseline incidence of mortality or major morbidity of 14.4%,1 430 patients were needed to demonstrate an odds ratio of at least 1.5 with a 2-sided alpha of 0.05 and a beta of 0.2 in our multivariable regression model. Moreover, because the multivariable model was prespecified to contain up to 11 covariables (10 echocardiographic parameters plus the STS-Predicted Risk of Mortality or Major Morbidity [STS-PROMM]), ≈110 events were required to maintain an appropriate covariable:event ratio to avoid overfitting.12
Statistical MethodsEchocardiography variables were preserved in their continuous form13 and standardized such that the resulting odds ratios represented the increase in odds per standard deviation in that variable. To test the ap-propriateness of entering a continuous variable in a logistic regression model, each echocardiographic variable (x axis) was plotted against
by guest on May 24, 2018
http://circ.ahajournals.org/D
ownloaded from

358 Circulation January 22, 2013
the logit of the primary outcome (y axis) and the resulting graphical plot was inspected for linearity. Because clinicians often use cutoffs in day-to-day practice, echocardiography variables were also dichot-omized according to accepted normal reference limits and analyses were presented using both continuous and dichotomized predictors.
The multivariable echocardiographic model was a priori prespeci-fied to include 1 parameter from each of the following domains: right atrial size, RV size, RV systolic function, RV diastolic function or MPI, PASP, tricuspid regurgitation, left atrial size, LV size, LV sys-tolic function, LV diastolic function, LV mass, and mitral regurgita-tion. Indexed parameters were used and volumes/areas were favored over linear dimensions for cavity size. Right and left atrial size were removed from the model because they were found to be intermediate factors in the causal pathway between diastolic dysfunction and ad-verse outcomes, and also between tricuspid/mitral regurgitation and adverse outcomes (leading to model instability and overadjustment bias when entered).14
For the primary outcome, a multivariable logistic regression model was used to identify the optimal echocardiographic parameters to pre-dict in-hospital mortality or major morbidity. For the secondary out-come, a multivariable Cox proportional hazards model was used to identify the optimal echocardiographic parameters to predict all-cause mortality. The proportionality of hazards assumptions was tested based on Schoenfeld residuals. Of note, these echocardiographic models did not contain clinical variables or the STS-PROMM.
To test the incremental predictive value for mortality or major morbidity, the optimal echocardiographic parameters identified in the above model were then entered in a subsequent model that contained the STS-PROMM. Model performance statistics were calculated before and after addition of the echocardiographic pa-rameters to STS-PROMM. These statistics included the c-statistic for discrimination, Aikaikes Information Criterion (AIC) for global fit, Net Reclassification Improvement, and Integrated Discrimination Improvement (IDI) for reclassification.15 For the Net Reclassification Improvement, the Q1 and Q3 were used to define STS-PROMM cut-offs: low risk 0% to 10%, intermediate risk 10% to 25%, and high risk >25%. The AIC approach with forward selection was used to select the echocardiographic variables for the model, with the optimal model being that which minimized the AIC.
The model selected and coefficients identified in the derivation co-hort were applied to predict the risk of mortality or major morbidity in the external validation cohort. The c-statistic for these predicted probabilities in the validation cohort was calculated and compared with the c-statistic for the STS-PROMM alone.
Sensitivity analysis was performed in which the echocardiographic parameters were entered in a model containing individual clinical covariables rather than the composite STS-PROMM. The clinical covariables were chosen to be those with the highest coefficients in the STS-PROMM model (age, female, diabetes mellitus, chronic kidney disease, chronic lung disease, peripheral arterial disease, cerebrovascular disease, atrial fibrillation, previous cardiac surgery). Measurements were >90% to 95% complete for all echocardio-graphic parameters, with the exception of PASP (74% complete, not measurable when no tricuspid regurgitation). Therefore, a sensitivity analysis was performed in which multiple imputation was used to derive missing values for PASP. All analyses were performed with STATA 12 (College Station, TX).
ResultsDerivation CohortA total of 1150 patients underwent isolated CABG at the derivation site between 2007 and 2009, of which 667 had available echocardiograms performed at the study center ≤30 days before surgery (mean 5.6±5.8 days before surgery; Figure 1). Those who did not have available echocardio-grams at the study center were excluded; they had deter-mination of left ventricular function by angiocardiography (n=387), echocardiography at another center (n=49), nuclear
medicine (n=33), or other modality (n=14), and were less likely to present with myocardial infarction, have heart fail-ure, or require urgent surgery (Table I in the online-only Data Supplement).
Baseline clinical characteristics are shown in Table 1. The mean age was 67.2±11.1 years, with 10.0% octogenarians and 22.8% females. Patients were evenly distributed in low-risk (29% with STS-PROMM 0% to 9%), intermediate-risk (46% with STS-PROMM 10% to 25%), and high-risk (25% with STS-PROMM ≥25%) categories. One hundred four (15.6%) postoperative mortalities or major morbidities were observed during the index hospitalization.
The preoperative echocardiographic parameters are shown in Table 2. The optimal echocardiographic model to predict in-hospital mortality or major morbidity consisted of the fol-lowing (continuous predictors): restrictive LV diastolic filling (odds ratio [OR], 2.39; 95% confidence interval [CI], 1.26-4.55), RV fractional area change (OR, 0.73; 95% CI, 0.56-0.95), RV myocardial performance index (OR, 1.44; 95% CI, 1.10-1.90), and mitral regurgitation (OR, 1.44; 95% CI, 1.04-2.01), although mitral regurgitation did not reach statisti-cal significance when dichotomized at the moderate severity threshold (Table 3).
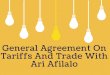
Addition of these echocardiographic parameters to the STS-PROMM resulted in a net improvement in model performance as evidenced by an increase in c-statistic from 0.68 to 0.73, a decrease in AIC from 543 to 470, an Net Reclassification Improvement of 27.5% (95% CI, 12.8-42.1%), and an IDI of 5.9% (95% CI, 2.8-8.9%) (Figure 2). After adjusting for STS-PROMM, restrictive LV diastolic filling (OR, 2.38; 95% CI, 1.21-4.70) and RV fractional area change (OR, 0.73; 95% CI, 0.55-0.98) remained independently predictive.
Seventy-three (10.9%) deaths were observed over a median follow-up of 3.2 years (Q1 2.5, Q3 3.9 years). In the Cox proportional hazards model, 2 echocardiographic parameters
Figure 1. Flow diagram for the main derivation cohort. Of 1150 patients who had isolated coronary artery bypass surgery (CABG) at the Massachusetts General Hospital in the study period, 667 met the inclusion criteria and were considered in the analyses.
by guest on May 24, 2018
http://circ.ahajournals.org/D
ownloaded from

Afilalo et al Echocardiography Before Coronary Bypass Surgery 359
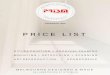
were found to be predictive of all-cause mortality: RV fractional area change (hazard ratio [HR], 0.73; 95% CI, 0.57-0.95) and PASP (HR, 1.03; 95% CI, 1.01–1.05) (Table 3). In particular, patients with a preoperative PASP ≥50 mm Hg had a 3-fold increase in mortality (HR, 3.54; 95% CI, 1.95, 6.42; Figure 3).
In sensitivity analyses, the same echocardiographic predic-tors were identified when individual clinical covariables were used instead of the composite STS-PROMM to adjust for baseline characteristics (Tables II and III in the online-only Data Supplement), and when multiple imputation was used to derive values for missing PASP (n=175 missing as a result of insufficient tricuspid regurgitation jet envelope).
Validation CohortA total of 236 patients underwent isolated CABG at the validation site, of which 187 had available preoperative echocardiograms
Table 1. Clinical Characteristics
Overall(n=667)
Mortality or Major Morbidity
Yes (n=104) No (n=563)
Age, y 67.2±11.1 70.5±11.2 66.6±11.0
Female 152 (22.8) 26 (25.0) 126 (22.4)
BMI, kg/m2 28.8±5.2 28.3±4.5 28.9±5.3
Diabetes mellitus 250 (37.5) 42 (40.4) 208 (36.9)
Chronic kidney disease 247 (37.0) 55 (52.9) 192 (34.1)
Chronic lung disease 85 (12.7) 16 (15.4) 69 (12.3)
Peripheral arterial disease 138 (20.7) 30 (28.8) 108 (19.2)
Cerebrovascular disease 119 (17.8) 23 (22.1) 96 (17.1)
Atrial fibrillation 70 (10.5) 21 (20.2) 49 (8.7)
Previous cardiac surgery 27 (4.0) 7 (6.7) 20 (3.6)
Cardiogenic shock 3 (0.4) 2 (1.9) 1 (0.2)
CHF within 2 wk 195 (29.2) 56 (53.8) 139 (24.7)
STS predicted mortality/morbidity
Mean 19.1±13.3 17.7±12.2 27.6±16.2
Low risk (0% to 10%) 194 (29.1) 13 (12.9) 179 (31.8)
Intermediate risk (10% to 25%)
309 (46.3) 48 (36.6) 327 (58.1)
High risk (>25%) 164 (24.6) 53 (50.5) 57 (10.1)
Cardiac presentation
No symptoms 37 (7.8) 7 (10.1) 30 (7.4)
Stable angina 81 (17.2) 12 (17.4) 69 (17.1)
Unstable angina 156 (33.1) 13 (18.8) 143 (35.5)
NSTEMI 151 (32.0) 24 (34.8) 127 (31.5)
STEMI 47 (10.0) 13 (18.8) 34 (8.4)
Operative status
Elective 67 (10.0) 7 (6.7) 60 (10.7)
Urgent 598 (89.7) 96 (92.3) 502 (89.2)
Emergent 2 (0.3) 1 (1.0) 1 (0.2)
Number of grafts 3.3±1.1 3.3±1.2 3.3±1.1
In-hospital outcomes
Mortality or major morbidity
104 (15.6)
Mortality 11 (1.6)
Stroke 11 (1.6)
Renal failure 23 (3.4)
Prolonged intubation 68 (10.2)
Deep sternal wound infection
4 (0.6)
Reoperation 44 (6.6)
BMI indicates body mass index; CHF, congestive heart failure; NSTEMI, non–ST-elevation myocardial infarction; STEMI, ST-elevation myocardial infarction; and STS-PROMM, Society of Thoracic Surgeons predicted risk of mortality or major morbidity.
Table 2. Preoperative Echocardiographic Parameters
Overall(n=667)
Mortality or Major Morbidity
Yes (n=104) No (n=563)
LA volume index, mL/m2 31.4±12.2 35.3±12.5 30.7±12.0
LA linear dimension (PLAX), cm
3.8±0.6 3.8±0.6 3.8±0.5
LV end-diastolic volume index, mL/m2
53.1±18.3 60.1±21.8 51.8±17.3
LV end-diastolic linear dimension, cm
4.7±0.7 4.7±0.8 4.6±0.7
LVEF, % 55.3±12.7 49.9±14.8 56.3±12.0
LVEF
<30% 38 (5.7) 15 (14.4) 23 (4.1)
30% to 49% 149 (22.3) 31 (29.8) 118 (21.0)
50% to 69% 427 (64.0) 48 (46.2) 379 (67.3)
≥70% 53 (8.0) 10 (9.6) 43 (7.6)
Diastolic filling
Normal 237 (35.5) 26 (25.0) 211 (37.5)
Impaired 225 (33.7) 28 (26.9) 197 (35.0)
Pseudonormal 103 (15.4) 18 (17.3) 85 (15.1)
Restrictive 67 (10.0) 25 (24.0) 42 (7.5)
N/A 35 (5.3) 7 (6.7) 28 (5.0)
LV mass index, g/m2 94.6±24.0 99.8±25.6 93.6±23.6
Mitral regurgitation
None-Trivial 392 (58.8) 45 (43.3) 347 (61.6)
Mild 222 (33.3) 41 (39.4) 181 (32.1)
Moderate 53 (7.9) 18 (17.3) 35 (6.2)
RA area index, cm/m2 7.3±2.1 7.9±2.0 7.2±2.0
RV end-diastolic area index, cm/m2
8.2±2.2 8.7±2.4 8.1±2.1
RV fractional area change, %
50.2±9.3 45.8±11.6 51.1±8.6
RV myocardial performance index
0.33±0.15 0.40±0.18 0.31±0.14
PASP, mm Hg 38.2±11.8 42.4±15.4 37.3±10.8
N/A 175 (26.2) 19 (18.3) 156 (27.7)
Tricuspid regurgitation
None-Trivial 482 (72.3) 65 (62.5) 417 (74.1)
Mild 156 (23.4) 28 (26.9) 128 (22.7)
Moderate 29 (4.3) 11 (10.6) 18 (3.2)
LA indicates left atrial; LV, left ventricular, LVEF, left ventricular ejection fraction; N/A, not available; PASP, pulmonary artery systolic pressure; PLAX, parasternal long-axis view; RA, right atrial; and RV, right ventricular.
by guest on May 24, 2018
http://circ.ahajournals.org/D
ownloaded from

360 Circulation January 22, 2013
performed within 30 days at the study center. Compared with the derivation cohort, the validation cohort demonstrated slightly lower mean age (65.8±10.3 versus 67.2±11.1), lower proportion of females (17.6% versus 22.8%), and lower mean STS-PROMM (13.8±12.1% versus 19.1±13.3%; Table IV in the online-only Data Supplement). Thirty-three (17.6%) postoperative mortalities or major morbidities were observed
during the index hospitalization. When the echocardiographic parameters tested in the derivation cohort were re-entered, the AIC model selection procedure identified restrictive LV diastolic filling (OR, 4.73; 95% CI, 1.11-20.06), abnormal RV myocardial performance index (OR, 2.54; 95% CI, 1.04-6.22), and mitral regurgitation (OR, 1.65; 95% CI, 0.99-2.76) as the optimal predictors of mortality or major morbidity. Abnormal RV fractional area change was a strong predictor in univariate analysis (OR, 8.93; 95% CI, 2.02-39.50), but it was not statistically significant in multivariable analysis, partly because of its lower prevalence in the validation cohort (6.1% versus 10.0%). The model coefficients fit in the derivation set were applied to the validation set and used to calculate the c-statistic for the STS-PROMM alone versus the STS-PROMM plus the echocardiographic parameters. Addition of the echocardiographic parameters resulted in a similar net improvement in model performance as evidenced by an increase in c-statistic from 0.73 to 0.76.
DiscussionOur study has demonstrated the prognostic impact of a com-prehensive echocardiogram in patients undergoing CABG.
Table 3. Optimal Echocardiographic Predictors in Multivariable Analysis
OR (95% CI)Continuous Predictors*
OR (95% CI)Dichotomous Predictors**
In-hospital mortality or major morbidity (104 events)
Severe LV diastolic dysfunction (restrictive filling pattern)
2.39 (1.26, 4.55; P=0.008)
2.96 (1.59, 5.49; P=0.001)
RV systolic dysfunction (fractional area change)
0.73 (0.56, 0.95; P=0.02)
3.03 (1.28, 7.20; P=0.01)
RV inefficiency (myocardial performance index)
1.44 (1.10, 1.90; P=0.009)
1.89 (1.13, 3.15; P=0.02)
Mitral regurgitation (grade 0–4) 1.44 (1.04, 2.01; P=0.03)
1.96 (0.96, 4.02; P=0.07)
All-cause mortality at a medium of 3.2 yrs (73 events)
RV systolic dysfunction (fractional area change)
0.73 (0.57, 0.95; P=0.01)
2.03 (0.95, 4.33; P=0.07)
Pulmonary artery systolic pressure (mm Hg)
1.03 (1.01, 1.05; P=0.001)
3.54 (1.95, 6.42; P<0.001)
*Continuous predictors denotes entry of continuous echocardiographic variables in their continuous form (RV fractional area change and RV myocardial performance index were standardized such that the OR and HR are per SD change).
**Dichotomous predictors denotes entry of continuous echocardiographic variables in a transformed dichotomous form according to ASE guidelines and normal reference limits (RV fractional area change <35%, RV myocardial performance index >0.4, Mitral regurgitation severity ≥moderate, Pulmonary artery systolic pressure ≥50 mm Hg).
CI indicates confidence interval; HR, hazard ratio; LV, left ventricular; OR, odds ratio; and RV, right ventricular.
Figure 2. Incremental value of echocardiography when added to the STS-PROMM risk score. The Receiver Operating Char-acteristic curve is shown for the STS-PROMM alone and the STS-PROMM plus the echocardiographic parameters to predict mortality or major morbidity. AUC indicates Area Under Curve; STS-PROMM indicates Society of Thoracic Surgeons Predicted Risk of Mortality or Major Morbidity.
Figure 3. Kaplan–Meier survival curves for the echocardio-graphic predictors of mortality over the 3.2-year follow-up period. Top, Right ventricular fractional area change (RV FAC). Bottom, Pulmonary artery systolic pressure (PASP). CABG indicates coro-nary artery bypass surgery. PASP denotes patients in whom the tricuspid regurgitation Doppler jet envelope was insufficient to measure PASP (n=175).
by guest on May 24, 2018
http://circ.ahajournals.org/D
ownloaded from

Afilalo et al Echocardiography Before Coronary Bypass Surgery 361
Preoperative RV dysfunction and restrictive LV filling emerged as powerful predictors of mortality or major mor-bidity after CABG, whereas RV dysfunction and pulmonary hypertension predicted long-term mortality over 3.2 years. Importantly, addition of these echocardiographic parameters to the STS risk score resulted in a net improvement in model performance, signifying that echocardiography yielded incre-mental value.
The incremental value provided by the echocardiogram above traditional risk scores was found to be substantive. The increase in c-statistic of 0.03 to 0.05 and IDI of 5.9% com-pare favorably with other commonly used prognostic tests, such as coronary artery calcium testing (increase in c-statistic +0.04, IDI 1.5%) or high-sensitivity c-reactive protein testing (increase in c-statistic +0.01, IDI 0.2%) above traditional risk factors to predict incident cardiovascular events.16 The modest baseline c-statistic of 0.68 to predict major morbidity in this study is consistent with previous reports (c-statistic 0.65–0.70 to predict morbidity versus 0.75–0.80 to predict mortality)17 and confirms the limitations in predicting who will suffer a postoperative complication.
Inclusion of RV dysfunction and restrictive LV filling in risk scores would lead to refined estimates of operative risk, which have historically been less accurate in certain patients, particularly the elderly.17 Using echocardiography to improve risk prediction would allow clinicians and patients to be bet-ter informed in their shared decision-making and planning. Because higher-risk patients are often those who derive greater benefits from revascularization, the main clinical util-ity of echocardiography in identifying higher-risk patients would not be to withhold CABG from such patients but rather to tailor the revascularization strategy to the individual patient. For example, a patient found to have preoperative RV dys-function or restrictive LV filling may potentially benefit from a less invasive revascularization strategy (minimally inva-sive CABG, off-pump CABG, multivessel PCI). Carefully designed prospective studies are needed to test and validate this hypothesis.
Intraoperative transesophageal echocardiography (TEE), now commonly performed in many centers, provides valu-able guidance for intraoperative management during CABG. However, the mandate and focus of the intraoperative TEE is clearly different from that of the preoperative transthoracic examination. The preoperative transthoracic examination offers a comprehensive assessment of the severity and extent of disease, and in doing so, exerts a direct influence on patient selection and revascularization strategy. The intraoperative TEE is performed at a time when the revascularization strat-egy has in large part already been determined and would be impractical to change. Thus, the preoperative transthoracic examination and the intraoperative TEE serve complimentary (as opposed to redundant) roles.
Beyond guiding the overall revascularization strategy, specific interventions aimed at a given echocardiographic abnormality could be used. For the severely dysfunctional RV (abnormal RV FAC), right ventricular assist devices have been successfully used as adjuncts to CABG.18,19 For the mildly dysfunctional RV, ischemic preconditioning by transient aor-tic cross-clamping and reperfusion showed positive results,
although these have yet to be applied in clinical practice.20 Revascularization of intermediate right coronary artery ste-noses does not seem to be a predictor of RV recovery after CABG.21,22 For patients with pulmonary hypertension, pulmo-nary vasodilators have been shown to improve outcomes.23,24 For the restrictive LV, milrinone has had mixed results25,26 whereas close monitoring and optimization of volume status and filling pressures remains the mainstay.
Preoperative RV dysfunction was a strong predictor of short- and long-term outcomes after CABG. Previously, the clinical impact of preoperative RV dysfunction was unclear. One series of 74 patients showed that tricuspid annular plane systolic excursion was not predictive of death or readmis-sion after CABG,27 whereas another series of 41 patients with severe LV dysfunction showed that RV FAC assessed by intraoperative TEE was predictive of ventilator hours and inotrope requirements in the early postoperative period.28 The latter study was difficult to extrapolate because RV FAC had been measured under anesthetized conditions, in a highly selected patient population, with a small sample size under-powered to detect differences in clinical endpoints (only 7 patients had an abnormal RV FAC). Our series of 667 diverse patients has shown more definitively that RV FAC assessed by resting preoperative TTE was predictive of major clinical endpoints.
In addition to RV FAC as a measure of RV systolic dysfunc-tion, our echocardiographic protocol included RV MPI as a measure of global RV efficiency. These two measures proved to be complementary—RV FAC identified a small group of patients (5%) with overt RV hypokinesis who were at extreme risk (50% observed mortality or major morbidity), whereas RV MPI identified a larger group (24%) with subclinical RV impairment which may not otherwise be detected by visual assessment of the RV that were at high risk (26% observed mortality or major morbidity). We opted not to include mea-sures of longitudinal RV function (tricuspid annular plane systolic excursion or tricuspid annular tissue Doppler veloc-ity) for 2 reasons: first, these have been shown to inaccu-rately correlate with postoperative RV ejection fraction29 or functional capacity30 after cardiac surgery, and second, these require dedicated M-Mode and tissue Doppler acquisitions, which are not always available. RV FAC and MPI have the distinct advantage of being measurable offline from routinely acquired images within <5 minutes. These 2 parameters are recommended for routine clinical use by the Guidelines for the Echocardiographic Assessment of the Right Heart from the American Society of Echocardiography,6 because their reli-ability and prognostic value have been extensively validated.
Restrictive LV filling, the echocardiographic hallmark of severe diastolic dysfunction, was the other independent pre-dictor of mortality or major morbidity in our cohort. This finding is consistent with previous studies, which have con-sistently shown that severe but not mild or moderate diastolic dysfunction is associated with mortality and complications after CABG.31–34 The prevalence of restrictive LV filling was 6% to 10% in our 2 cohorts, in line with previous studies. This prevalence may vary depending on the patient population studied (3% in elective low-risk patients34 up to 48% in high-risk patients with severe LV systolic dysfunction).33
by guest on May 24, 2018
http://circ.ahajournals.org/D
ownloaded from

362 Circulation January 22, 2013
The rationale for RV dysfunction and restrictive LV dia-stolic filling as determinants of postoperative mortality or major morbidity can be appreciated by reviewing the usual physiological changes after CABG. Two of the predominant disturbances are (1) altered RV contraction and relaxation observed at the time of pericardial opening,35 and (2) increased LV stiffness attributable to myocardial edema and extrinsic compressive forces.36–38 Thus, given the expected decline in RV performance and LV stiffness after CABG, patients with preoperative findings of abnormal RV performance or LV stiffness (severe diastolic dysfunction) are at a clear disad-vantage. Conversely, CABG is associated with improved LV relaxation attributable in part to relief of ischemia,39 which may explain why patients with preoperative findings of abnor-mal LV relaxation (mild-to-moderate diastolic dysfunction) do not face an increase in adverse events. Additionally, severe diastolic dysfunction as measured by a mitral inflow decelera-tion time <150 ms has been shown to be a surrogate marker for viability (or lack thereof) validated against dobutamine echocardiography and myocardial scintigraphy33; this may explain, in part, why patients with restrictive LV filling tend to deteriorate rather than improve after CABG.
By analyzing the comprehensive echocardiogram rather than individual parameters of interest, our study was able to adjust for confounding between echocardiographic param-eters. Previous studies have been limited by partial adjustment for confounding, often adjusting for basic clinical variables but no other echocardiographic variables, leading to incon-sistent results. For example, the effect of low LVEF on post-operative mortality has been reported to be highly significant when adjusted for basic clinical variables40–42 but nonsignifi-cant when adjusted for LV size and diastolic function.31,43 Our data reflect this, with the effect of low LVEF being highly significant in univariate analysis (OR, 5.2; P<0.001) but non-significant when diastolic dysfunction and RV dysfunction were entered in the multivariable model (OR, 1.8; P=NS). Irrespective of these potential confounders, it is not surpris-ing that LVEF was nonsignificant in our contemporary cohorts because the prognostic impact of LVEF has been steadily declining in parallel with improvements in surgical techniques and postoperative care.44,45
A number of limitations should be acknowledged. First, the STS composite end point used as our primary outcome is intended to capture representative major morbidities after car-diac surgery, including deep sternal wound infection, which is of questionable relevance to preoperative echocardiography. However, deep sternal wound infection contributed very few events (n=4) to the composite end point and a sensitivity anal-ysis excluding it was unchanged. Second, follow-up echocar-diography is not routinely performed after CABG, precluding the assessment of functional recovery as an outcome mea-sure. Third, approximately one third of patients undergoing CABG in the derivation cohort and one fifth in the validation cohort did not have a recent preoperative echocardiogram; these tended to be lower risk patients. Although this nonran-dom subset could have affected the generalizability of our findings, the derivation and validation cohorts still included a large number of low-risk patients who were ultimately found to derive a similar if not greater incremental value from the
echocardiogram. Fourth, although a formal cost-effectiveness analysis was not performed, it is encouraging to note that the cost savings of preventing 1 postoperative major morbidity (average additive cost $40,704-62,77346) would offset the cost of performing >200 preoperative echocardiograms (global cost $233 as per the 2011 ASE Coding and Reimbursement Newsletter). Fifth, because the STS-PROMM was not designed nor validated to predict long-term mortality, the incremental value of echocardiographic predictors over such a clinical risk score was not assessed for this outcome mea-sure. Lastly, the effect of significant MR was equivocal (it was identified by the model selection procedure as 1 of 4 important predictors, yet it did not reach statistical significance), and the study was not designed to address how significant MR should be managed at the time of CABG. This remains a controver-sial question, which will be most appropriately answered by ongoing randomized clinical trials.
The strengths of this study include a multi-center design with derivation and validation cohorts, and a comprehensive echocardiographic protocol including right heart parameters, which had previously been less thoroughly evaluated. Our findings serve as an impetus to begin to integrate measures of RV dysfunction and severe LV diastolic dysfunction in the preoperative assessment of risk before CABG.
AcknowledgmentsWe thank Marcia Leavitt, David Crowell, and Karen Lynch for their invaluable help in obtaining clinical and echocardiographic data for this study. We also thank all of the cardiac sonographers at the Massachusetts General Hospital and Jewish General Hospital for their excellence in acquiring the echocardiographic images that made this study possible.
We thank Dr Murray Mittleman for his expertise and guidance. This work was con ducted with support from Harvard Catalyst | The Harvard Clinical and Translational Science Center (National Institutes of Health award #UL1 RR 025758 and financial contribu-tions from Harvard University and its affiliated academic health care centers). The con tent is solely the responsibility of the authors and does not necessarily represent the official views of Harvard Catalyst, Harvard University and its affiliated academic health care centers, the National Center for Research Resources, or the National Institutes of Health.
Sources of FundingDr Afilalo was supported by the FRSQ (Fonds de Recherché Santé du Québec) Research Fellowship Award.
DisclosuresDr Afilalo had full access to all the data in the study and takes re-sponsibility for the integrity of the data and the accuracy of the data analysis. The authors report no conflicts.
References 1. Shahian DM, O’Brien SM, Filardo G, Ferraris VA, Haan CK, Rich JB,
Normand SL, DeLong ER, Shewan CM, Dokholyan RS, Peterson ED, Ed-wards FH, Anderson RP; Society of Thoracic Surgeons Quality Measure-ment Task Force. The Society of Thoracic Surgeons 2008 cardiac surgery risk models: part 1–coronary artery bypass grafting surgery. Ann Thorac Surg. 2009;88(1 Suppl):S2–22.
2. Nashef SA, Roques F, Michel P, Gauducheau E, Lemeshow S, Salamon R. European system for cardiac operative risk evaluation (EuroSCORE). Eur J Cardiothorac Surg. 1999;16:9–13.
3. Hillis LD, Smith PK, Anderson JL, Bittl JA, Bridges CR, Byrne JG, Cigar-roa JE, Disesa VJ, Hiratzka LF, Hutter AM Jr, Jessen ME, Keeley EC,
by guest on May 24, 2018
http://circ.ahajournals.org/D
ownloaded from

Afilalo et al Echocardiography Before Coronary Bypass Surgery 363
Lahey SJ, Lange RA, London MJ, Mack MJ, Patel MR, Puskas JD, Sabik JF, Selnes O, Shahian DM, Trost JC, Winniford MD; American College of Cardiology Foundation; American Heart Association Task Force on Practice Guidelines; American Association for Thoracic Surgery; Society of Cardiovascular Anesthesiologists; Society of Thoracic Surgeons. 2011 ACCF/AHA Guideline for Coronary Artery Bypass Graft Surgery. A re-port of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Developed in collabora-tion with the American Association for Thoracic Surgery, Society of Car-diovascular Anesthesiologists, and Society of Thoracic Surgeons. J Am Coll Cardiol. 2011;58:e123–e210.
4. Eagle KA, Guyton RA, Davidoff R, Edwards FH, Ewy GA, Gardner TJ, Hart JC, Herrmann HC, Hillis LD, Hutter AM Jr, Lytle BW, Marlow RA, Nugent WC, Orszulak TA; American College of Cardiology; American Heart Association. ACC/AHA 2004 guideline update for coronary artery bypass graft surgery: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Com-mittee to Update the 1999 Guidelines for Coronary Artery Bypass Graft Surgery). Circulation. 2004;110:e340–e437.
5. Douglas PS, Garcia MJ, Haines DE, Lai WW, Manning WJ, Patel AR, Picard MH, Polk DM, Ragosta M, Parker Ward R, Weiner RB. ACCF/ASE/AHA/ASNC/HFSA/HRS/SCAI/SCCM/SCCT/SCMR 2011 Appropriate use cri-teria for echocardiography. J Am Soc Echocardiogr. 2011;24:229–267.
6. Rudski LG, Lai WW, Afilalo J, Hua L, Handschumacher MD, Chan-drasekaran K, Solomon SD, Louie EK, Schiller NB. Guidelines for the echocardiographic assessment of the right heart in adults: a report from the American Society of Echocardiography endorsed by the European Asso-ciation of Echocardiography, a registered branch of the European Society of Cardiology, and the Canadian Society of Echocardiography. J Am Soc Echocardiogr. 2010;23:685–713; quiz 786.
7. Lang RM, Bierig M, Devereux RB, Flachskampf FA, Foster E, Pellikka PA, Picard MH, Roman MJ, Seward J, Shanewise JS, Solomon SD, Spen-cer KT, Sutton MS, Stewart WJ; Chamber Quantification Writing Group; American Society of Echocardiography’s Guidelines and Standards Com-mittee; European Association of Echocardiography. Recommendations for chamber quantification: a report from the American Society of Echo-cardiography’s Guidelines and Standards Committee and the Chamber Quantification Writing Group, developed in conjunction with the Euro-pean Association of Echocardiography, a branch of the European Society of Cardiology. J Am Soc Echocardiogr. 2005;18:1440–1463.
8. Nagueh SF, Appleton CP, Gillebert TC, Marino PN, Oh JK, Smiseth OA, Waggoner AD, Flachskampf FA, Pellikka PA, Evangelista A. Recommen-dations for the evaluation of left ventricular diastolic function by echocar-diography. J Am Soc Echocardiogr. 2009;22:107–133.
9. Baumgartner H, Hung J, Bermejo J, Chambers JB, Evangelista A, Griffin BP, Iung B, Otto CM, Pellikka PA, Quiñones M. Echocardiographic as-sessment of valve stenosis: EAE/ASE recommendations for clinical prac-tice. J Am Soc Echocardiogr. 2009;22:1–23; quiz 101–2.
10. Zoghbi WA, Enriquez-Sarano M, Foster E, Grayburn PA, Kraft CD, Levine RA, Nihoyannopoulos P, Otto CM, Quinones MA, Rakowski H, Stewart WJ, Waggoner A, Weissman NJ; American Society of Echocar-diography. Recommendations for evaluation of the severity of native val-vular regurgitation with two-dimensional and Doppler echocardiography. J Am Soc Echocardiogr. 2003;16:777–802.
11. Shahian DM, Edwards FH, Ferraris VA, Haan CK, Rich JB, Normand SL, DeLong ER, O’Brien SM, Shewan CM, Dokholyan RS, Peterson ED; Society of Thoracic Surgeons Quality Measurement Task Force. Quality measurement in adult cardiac surgery: part 1–Conceptual framework and measure selection. Ann Thorac Surg. 2007;83(4 Suppl):S3–12.
12. Peduzzi P, Concato J, Kemper E, Holford TR, Feinstein AR. A simulation study of the number of events per variable in logistic regression analysis. J Clin Epidemiol. 1996;49:1373–1379.
13. Sauerbrei W, Royston P, Binder H. Selection of important variables and determination of functional form for continuous predictors in multivari-able model building. Stat Med. 2007;26:5512–5528.
14. Schisterman EF, Cole SR, Platt RW. Overadjustment bias and unnecessary adjustment in epidemiologic studies. Epidemiology. 2009;20:488–495.
15. Pencina MJ, D’Agostino RB Sr, D’Agostino RB Jr, Vasan RS. Evaluating the added predictive ability of a new marker: from area under the ROC curve to reclassification and beyond. Stat Med. 2008;27:157–72; discussion 207.
16. Möhlenkamp S, Lehmann N, Moebus S, Schmermund A, Dragano N, Stang A, Siegrist J, Mann K, Jöckel KH, Erbel R; Heinz Nixdorf Recall Study Investigators. Quantification of coronary atherosclerosis and in-flammation to predict coronary events and all-cause mortality. J Am Coll Cardiol. 2011;57:1455–1464.
17. Dupuis JY. Predicting outcomes in cardiac surgery: risk stratification mat-ters? Curr Opin Cardiol. 2008;23:560–567.
18. Hughes P, Hasenkam JM, Severinsen IK, Steinbrüchel DA. Right heart as-sist for beating heart coronary artery bypass grafting. Eur J Cardiothorac Surg. 2003;24:762–769.
19. Sommer SP, Gorski A, Aleksic I, Yildirim C, Schimmer C, Beissert M, Weininger M, Leyh RG. Heartmate II implantation with right coronary bypass grafting in ischemic cardiomyopathy with “fixed” pulmonary hy-pertension: treatment strategy to protect right ventricular function. J Card Surg. 2010;25:116–119.
20. Wu ZK, Pehkonen E, Laurikka J, Kaukinen L, Honkonen EL, Kaukinen S, Laippala P, Tarkka MR. The protective effects of preconditioning decline in aged patients undergoing coronary artery bypass grafting. J Thorac Cardiovasc Surg. 2001;122:972–978.
21. Schirmer U, Calzia E, Lindner KH, Hemmer W, Georgieff M. Right ven-tricular function after coronary artery bypass grafting in patients with and without revascularization of the right coronary artery. J Cardiothorac Vasc Anesth. 1995;9:659–664.
22. Roshanali F, Yousefnia MA, Mandegar MH, Rayatzadeh H, Alinejad S. Decreased right ventricular function after coronary artery bypass grafting. Tex Heart Inst J. 2008;35:250–255.
23. Haché M, Denault A, Bélisle S, Robitaille D, Couture P, Sheridan P, Pel-lerin M, Babin D, Noël N, Guertin MC, Martineau R, Dupuis J. Inhaled epoprostenol (prostacyclin) and pulmonary hypertension before cardiac surgery. J Thorac Cardiovasc Surg. 2003;125:642–649.
24. Winterhalter M, Simon A, Fischer S, Rahe-Meyer N, Chamtzidou N, Hecker H, Zuk J, Piepenbrock S, Strüber M. Comparison of inhaled il-oprost and nitric oxide in patients with pulmonary hypertension during weaning from cardiopulmonary bypass in cardiac surgery: a prospective randomized trial. J Cardiothorac Vasc Anesth. 2008;22:406–413.
25. Axelsson B, Arbeus M, Magnuson A, Hultman J. Milrinone improves dia-stolic function in coronary artery bypass surgery as assessed by acoustic quantification and peak filling rate: a prospective randomized study. J Car-diothorac Vasc Anesth. 2010;24:244–249.
26. Couture P, Denault AY, Pellerin M, Tardif JC. Milrinone enhances systolic, but not diastolic function during coronary artery bypass grafting surgery. Can J Anaesth. 2007;54:509–522.
27. Bajraktari G, Duncan A, Pepper J, Henein M. Prolonged total isovolumic time predicts cardiac events following coronary artery bypass surgery. Eur J Echocardiogr. 2008;9:779–783.
28. Maslow AD, Regan MM, Panzica P, Heindel S, Mashikian J, Comunale ME. Precardiopulmonary bypass right ventricular function is associated with poor outcome after coronary artery bypass grafting in patients with severe left ventricular systolic dysfunction. Anesth Analg. 2002;95:1507–18, table of contents.
29. Tamborini G, Muratori M, Brusoni D, Celeste F, Maffessanti F, Caiani EG, Alamanni F, Pepi M. Is right ventricular systolic function reduced after cardiac surgery? A two- and three-dimensional echocardiographic study. Eur J Echocardiogr. 2009;10:630–634.
30. Hedman A, Alam M, Zuber E, Nordlander R, Samad BA. Decreased right ventricular function after coronary artery bypass grafting and its relation to exercise capacity: a tricuspid annular motion-based study. J Am Soc Echocardiogr. 2004;17:126–131.
31. Merello L, Riesle E, Alburquerque J, Torres H, Aránguiz-Santander E, Pedemonte O, Westerberg B. Risk scores do not predict high mortality after coronary artery bypass surgery in the presence of diastolic dysfunc-tion. Ann Thorac Surg. 2008;85:1247–1255.
32. Vaskelyte J, Stoskute N, Kinduris S, Ereminiene E. Coronary artery bypass grafting in patients with severe left ventricular dysfunction: pre-dictive significance of left ventricular diastolic filling pattern. Eur J Echo-cardiogr. 2001;2:62–67.
33. Yong Y, Nagueh SF, Shimoni S, Shan K, He ZX, Reardon MJ, Letsou GV, Howell JF, Verani MS, Quiñones MA, Zoghbi WA. Deceleration time in ischemic cardiomyopathy: relation to echocardiographic and scintigraphic indices of myocardial viability and functional recovery after revascular-ization. Circulation. 2001;103:1232–1237.
34. Youn YN, Shim CY, Yang H, Hong S, Chung N, Yoo KJ. Effect of diastolic dysfunction on early outcomes during elective off-pump coronary artery bypass grafting: a prospective observational study. Ann Thorac Surg. 2011;92:587–593.
35. Unsworth B, Casula RP, Kyriacou AA, Yadav H, Chukwuemeka A, Che-rian A, Stanbridge Rde L, Athanasiou T, Mayet J, Francis DP. The right ventricular annular velocity reduction caused by coronary artery bypass graft surgery occurs at the moment of pericardial incision. Am Heart J. 2010;159:314–322.
by guest on May 24, 2018
http://circ.ahajournals.org/D
ownloaded from

364 Circulation January 22, 2013
36. Tulner SAF, Klautz RJM, van Rijk-Zwikker GL, Engbers FHM, Bax JJ, Baan J, van der Wall EE, Dion RA, Steendijk P. Perioperative assessment of left ventricular function by pressure-volume loops using the conduc-tance catheter method. Anesth Analg. 2003;97:950–957.
37. de Waal EE, De Boeck BW, Kruitwagen CL, Cramer MJ, Buhre WF. Ef-fects of on-pump and off-pump coronary artery bypass grafting on left ventricular relaxation and compliance: a comprehensive perioperative echocardiography study. Eur J Echocardiogr. 2010;11:732–737.
38. Ekery DL, Davidoff R, Orlandi QG, Apstein CS, Hesselvik JF, Shemin RJ, Shapira OM. Imaging and diagnostic testing: diastolic dysfunction after coronary artery bypass grafting: a frequent finding of clinical significance not influenced by intravenous calcium. Am Heart J. 2003;145:896–902.
39. Hedman A, Samad BA, Larsson T, Zuber E, Nordlander R, Alam M. Im-provement in diastolic left ventricular function after coronary artery by-pass grafting as assessed by recordings of mitral annular velocity using Doppler tissue imaging. Eur J Echocardiogr. 2005;6:202–209.
40. Ahmed WA, Tully PJ, Baker RA, Knight JL. Survival after isolated coro-nary artery bypass grafting in patients with severe left ventricular dysfunc-tion. Ann Thorac Surg. 2009;87:1106–1112.
41. Hamad MAS, van Straten AHM, Schönberger JPAM, Woorst ter JF, de Wolf AM, Martens EJ, van Zundert AAJ. Preoperative ejection fraction as
a predictor of survival after coronary artery bypass grafting: comparison with a matched general population. J Cardiothorac Surg. 2010;5:29.
42. Topkara VK, Cheema FH, Kesavaramanujam S, Mercando ML, Cheema AF, Namerow PB, Argenziano M, Naka Y, Oz MC, Esrig BC. Coronary artery bypass grafting in patients with low ejection fraction. Circulation. 2005;112(9 Suppl):I344–I350.
43. Liu J, Tanaka N, Murata K, Ueda K, Wada Y, Oyama R, Matsuzaki M. Prognostic value of pseudonormal and restrictive filling patterns on left ventricular remodeling and cardiac events after coronary artery bypass grafting. Am J Cardiol. 2003;91:550–554.
44. Davierwala PM, Maganti M, Yau TM. Decreasing significance of left ven-tricular dysfunction and reoperative surgery in predicting coronary artery bypass grafting-associated mortality: a twelve-year study. J Thorac Car-diovasc Surg. 2003;126:1335–1344.
45. Appoo J, Norris C, Merali S, Graham MM, Koshal A, Knudtson ML, Gha-li WA. Long-term outcome of isolated coronary artery bypass surgery in patients with severe left ventricular dysfunction. Circulation. 2004;110(11 Suppl 1):II13–II17.
46. Speir AM, Kasirajan V, Barnett SD, Fonner E Jr. Additive costs of postop-erative complications for isolated coronary artery bypass grafting patients in Virginia. Ann Thorac Surg. 2009;88:40–5; discussion 45.
CLINICAL PERSPECTIVEEchocardiography is commonly performed before coronary artery bypass surgery to assess left ventricular systolic function and concomitant valvular lesions. Beyond these basic parameters, this study of 854 patients has shown that left ventricular diastolic function and right ventricular function merit careful consideration because they carry meaningful information about the patient’s risk for postoperative mortality and major morbidity. A derivation cohort at the Massachusetts General Hospital was used to identify optimal echocardiographic predictors, which were subsequently confirmed in a validation cohort at the Jewish General Hospital. Specifically, the presence of restrictive diastolic filling and abnormal right ventricular function (as measured by fractional area change or myocardial performance index) were each associated with a 2- to 3-fold increase in in-hospital mortality or major morbidity. These echocardiographic parameters demonstrated an incremental value above clinical covariables and the Society of Thoracic Surgeons Risk Score, resulting in improved discrimination and reclassification of risk. The prognostic value of the preoperative echocardiogram extended past the in-hospital timeframe, with right ventricular function and pulmonary arterial systolic pressure emerging as independent predictors of all-cause mortality after a median of 3.2 years of follow-up. Although previous studies had evaluated selected echocardiographic parameters, the independent value of each parameter within the context of a comprehensive echocardiogram remained unclear. With the help of this study, clinicians will be in a better position to integrate echocardiographic findings in their evaluation of operative risk and ultimately make more informed treatment decisions for their patients.
by guest on May 24, 2018
http://circ.ahajournals.org/D
ownloaded from

Jean-Francois Morin, Cristina Castrillo, David M. Shahian and Michael H. PicardJonathan Afilalo, Aidan W. Flynn, Avi Shimony, Lawrence G. Rudski, Arvind K. Agnihotri,
Morbidity in Coronary Artery Bypass SurgeryIncremental Value of the Preoperative Echocardiogram to Predict Mortality and Major
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 2012 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/CIRCULATIONAHA.112.127639
2013;127:356-364; originally published online December 12, 2012;Circulation.
http://circ.ahajournals.org/content/127/3/356World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circ.ahajournals.org/content/suppl/2012/12/12/CIRCULATIONAHA.112.127639.DC1Data Supplement (unedited) at:
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer this process is available in the
click Request Permissions in the middle column of the Web page under Services. Further information aboutOffice. Once the online version of the published article for which permission is being requested is located,
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the EditorialCirculationin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on May 24, 2018
http://circ.ahajournals.org/D
ownloaded from

1
Incremental Value of the Preoperative Echocardiogram to Predict Mortality and
Major Morbidity in Coronary Artery Bypass Surgery
SUPPLEMENTAL MATERIAL

2
Supplementary Table 1: Characteristics of Included vs. Excluded Patients
Included (N=667)
Excluded (N=483)
Age, years 67.2 ± 11.1 67.8 ± 9.7 Female 152 (22.8) 67 (13.9) BMI, kg/m2 28.8 ± 5.2 29.0 ± 5.1 Diabetes 250 (37.5) 159 (32.9) Chronic kidney disease 247 (37.0) 109 (22.7) Chronic lung disease 85 (12.7) 44 (9.1) Peripheral arterial disease 138 (20.7) 68 (14.1) Cerebrovascular disease 119 (17.8) 69 (14.3) Atrial fibrillation 70 (10.5) 30 (6.2) Prior cardiac surgery 27 (4.0) 29 (6.0) Cardiogenic shock 3 (0.4) 4 (0.8) CHF within 2 weeks 195 (29.2) 32 (6.6) * Cardiac presentation No symptoms 37 (7.8) 48 (15.5) Stable angina 81 (17.2) 129 (41.8) Unstable angina 156 (33.1) 99 (32.0) NSTEMI 151 (32.0) 25 (8.1) * STEMI 47 (10.0) 8 (2.6) * Operative status Elective 67 (10.0) 267 (55.3) Urgent 598 (89.7) 208 (43.1) * Emergent 2 (0.3) 8 (1.7) LVEF (clinically reported value) 57.4 ± 14.5 60.0 ± 13.5 STS-‐PROMM 19.1 ± 13.3 12.2 ± 9.2 In-‐hospital outcomes Mortality or major morbidity 104 (15.6) 47 (9.7) Mortality 11 (1.6) 2 (0.4) Stroke 11 (1.6) 3 (0.6) Renal failure 23 (3.4) 9 (1.9) Prolonged intubation 68 (10.2) 21 (4.3) Deep sternal wound infection 4 (0.6) 1 (0.2) Reoperation 44 (6.6) 21 (4.3) Abbreviations: BMI, body mass index; CHF, congestive heart failure; STEMI, ST-‐elevation myocardial infarction; NSTEMI, non-‐STEMI; LVEF, left ventricular ejection fraction; STS-‐PROMM, Society of Thoracic Surgeons predicted risk of mortality or major morbidity.

3
* CHF, NSTEMI/STEMI presentation, and urgent operative status were associated with having a preoperative echocardiogram in multivariable analysis. ‡ 132 patients in the excluded group did not have any assessment of valvular function (compared to 0 patients in the included group).

4
Supplementary Table 2: Logistic Model with Echocardiographic and Clinical Covariables to Predict In-‐Hospital Mortality or Major Morbidity OR (95% CI) Age, per year 1.00 (0.97, 1.03) Female 1.42 (0.76, 2.67) Chronic lung disease 0.94 (0.45, 1.95) Chronic kidney disease 1.34 (0.72, 2.49) Peripheral arterial disease 1.14 (0.62, 2.08) Cerebrovascular disease 1.23 (0.66, 2.30) Diabetes mellitus 0.87 (0.51, 1.48) Atrial fibrillation 2.18 (1.10, 4.33) Redo surgery 2.01 (0.70, 5.82) LV end-‐diastolic volume index, per mL/m2 1.02 (1.00, 1.03) LV ejection fraction <30% 1.40 (0.50, 3.89) 30-‐49% 1.15 (0.59, 2.23) 50-‐69% Referent >=70% 2.17 (0.95, 4.92) LV restrictive diastolic filling 2.33 (1.15, 4.71) LV mass index, per g/m2 0.99 (0.98, 1.01) Mitral regurgitation, per grade 1.20 (0.82, 1.75) RV area index, per cm2/m2 1.04 (0.92, 1.17) RV fractional area change, per % 0.74 (0.55, 0.99) RV myocardial performance index, per unit 1.37 (1.01, 1.87) Pulmonary artery systolic pressure >=50 mmHg 0.85 (0.39, 1.88) Tricuspid regurgitation, per grade 0.98 (0.63, 1.51) The AIC model selection procedure identified the following optimal model: OR (95% CI) LV restrictive diastolic filling 1.59 (0.97, 2.61) RV fractional area change, per % 1.01 (1.00, 1.03) RV myocardial performance index, per unit 1.55 (0.85, 2.82) LV end-‐diastolic volume index, per mL/m2 2.18 (1.15, 4.14) Female 2.38 (1.24, 4.57) Chronic kidney disease 1.36 (1.02, 1.80) Atrial fibrillation 0.71 (0.54, 0.94)

5
Supplementary Table 3: Cox Proportional Hazards Model with Echocardiographic and Clinical Covariables to Predict Long-‐Term Mortality OR (95% CI) Age, per year 0.99 (0.96, 1.02) Female 0.91 (0.46, 1.77) Chronic lung disease 1.58 (0.85, 2.96) Chronic kidney disease 2.22 (1.14, 4.33) Peripheral arterial disease 1.69 (0.96, 3.01) Cerebrovascular disease 2.39 (1.32, 4.33) Diabetes mellitus 2.44 (1.38, 4.31) Atrial fibrillation 1.36 (0.64, 2.88) Redo surgery 0.99 (0.29, 3.37) LV end-‐diastolic volume index, per mL/m2 1.00 (0.98, 1.02) LV ejection fraction <30% 0.55 (0.16, 1.82) 30-‐49% 1.66 (0.87, 3.20) 50-‐69% Referent >=70% 1.45 (0.58, 3.65) LV restrictive diastolic filling 0.60 (0.27, 1.35) LV mass index, per g/m2 1.00 (0.99, 1.01) Mitral regurgitation, per grade 1.09 (0.73, 1.63) RV area index, per cm2/m2 0.99 (0.87, 1.12) RV fractional area change, per % 0.71 (0.52, 0.97) RV myocardial performance index, per unit 1.22 (0.89, 1.68) Pulmonary artery systolic pressure >=50 mmHg 1.62 (0.79, 3.32) Tricuspid regurgitation, per grade 1.08 (0.70, 1.65) The AIC model selection procedure identified the following optimal model: OR (95% CI) Pulmonary artery systolic pressure >=50 mmHg 1.93 (1.05, 3.57) RV fractional area change, per % 0.77 (0.61, 0.99) LV ejection fraction 30-‐49% 1.82 (1.05, 3.14) Chronic kidney disease 2.34 (1.32, 4.15) Diabetes 2.22 (1.29, 3.84) Cerebrovascular disease 2.39 (1.37, 4.18) Peripheral arterial disease 1.72 (1.01, 2.92)

6
Supplementary Table 4: Clinical and Echocardiographic Characteristics of Patients in the Validation Cohort
N=187 CLINICAL Age, years 65.8 ± 10.3 Female 33 (17.6) BMI, kg/m2 27.7 ± 4.4 Diabetes 76 (40.6) Chronic kidney disease 48 (25.7) Chronic lung disease 14 (7.5) Peripheral arterial disease 26 (13.9) Cerebrovascular disease 21 (11.2) Atrial fibrillation 16 (8.6) Prior cardiac surgery 1 (0.5) Cardiogenic shock 4 (2.1) CHF within 2 weeks 37 (21.3) Cardiac presentation No symptoms 3 (1.6) Stable angina 39 (20.9) Unstable angina 66 (35.3) NSTEMI 67 (35.8) STEMI 12 (6.4) Operative status Elective 53 (28.3) Urgent 128 (68.4) Emergent 6 (3.2) STS-‐PROMM 13.8 ± 12.1 In-‐hospital outcomes Mortality or major morbidity 33 (17.6) Mortality 3 (1.6) Stroke 2 (1.1) Renal failure 5 (2.7) Prolonged intubation 19 (10.2) Deep sternal wound infection 2 (1.1) Reoperation 15 (8.0) ECHOCARDIOGRAPHIC LA volume index, mL/m2 24.1 ± 10.1 LV end-‐diastolic volume index, mL/m2 41.6 ±18.9
LV end-‐diastolic linear dimension, cm 4.8 ± 0.6 LVEF, % 54.8 ± 14.3

7
LVEF <30% 13 (7.1) 30-‐49% 39 (21.2) 50-‐69% 105 (57.1) ≥70% 27 (14.7) Diastolic filling Normal 72 (39.8) Impaired 54 (29.8) Pseudonormal 27 (14.9) Restrictive 11 (6.1) N/A 17 (9.4) LV mass index, g/m2 84.2 ±23.6 Mitral regurgitation None-‐Trivial 119 (63.6) Mild 59 (31.6) Moderate 9 (4.8) RA area index, cm/m2 7.5 ±1.8 RV end-‐diastolic area index, cm/m2 7.4 ±1.8 RV fractional area change, % 49.3 ±9.0 RV myocardial performance index 0.36 ±0.17 PASP, mmHg 34.2 ±10.5 N/A 62 (33.2) Tricuspid regurgitation None-‐Trivial 137 (73.2) Mild 49 (26.2) Moderate 1 (0.5) Abbreviations: BMI, body mass index; CHF, congestive heart failure; STEMI, ST-‐elevation myocardial infarction; NSTEMI, non-‐STEMI; LVEF, left ventricular ejection fraction; STS-‐PROMM, Society of Thoracic Surgeons predicted risk of mortality or major morbidity.