Embed Size (px)
Citation preview

535Indian Journal of Clinical Practice, Vol. 25, No. 6, November 2014
INTERNAL MEDICINE
Cytodiagnosis of Microfilaria at Unusual SitesKALPANA CHANDRA*, PRAVEEN KUMAR†, MEGHA GARG‡
ABSTRACT
Filariasis is a major public health problem especially in tropical countries like India. It is routinely examined in night peripheral blood smears. Fine-needle aspiration cytology (FNAC) is not routinely used for its identification. It has always been detected incidentally, while doing FNACs for evaluation of other lesions. It has been found in lymph nodes, breast, thyroid, cystic lesions, etc. In few reported cases, it has been found even with primary/metastatic malignancy. We also found two cases of microfilaria incidentally. One on USG-guided FNAC of liver SOL (space-occupying lesion) reported as metastatic adenocarcinoma with microfilaria and other in a case of asymptomatic epitrochlear swelling reported as reactive hyperplasia of lymph node with microfilaria.
Keywords: Liver SOL, epitrochlear lymph node, microfilaria
Filariasis is a global problem. It is a major social and economic scourge in the tropics and subtropics of Africa, Asia, Western Pacific and
parts of the Americas, affecting over 83 countries. The disease is endemic all over India1 and is caused by two closely related nematode worms, Wuchereria bancrofti and Brugia malayi transmitted by the Culex mosquito. Despite high incidence, it is less frequent to find microfilaria in the peripheral smear. The disease mainly involves the lymph node and lymphatic system of the body.
In lymphatic filariasis, the commonly involved sites are lungs, bronchial aspirates, cervicovaginal smears, pleural and pericardial fluids.2 It is very unusual and quite incidental to find microfilaria on fine-needle aspiration cytology (FNAC) in liver SOL (space-occupying lesion) and in epitrochlear lymph node, which itself is very rarely involved by any diseases pathology.
*Associate Professor Dept. of Pathology†Associate ProfessorDept. of General Medicine‡Resident Dept. of PathologyShri Ram Murti Smark Institute of Medical Sciences, Bhojipura, Bareilly, Uttar PradeshAddress for correspondenceDr Kalpana Chandra A-1, Doctor’s ResidenceShri Ram Murti Smark Institute of Medical Sciences Bhojipura, Bareilly - 243 202, Uttar Pradesh E-mail: [email protected]
This case is reported only because of peculiarity of site where it was not clinically suspected and how careful and vigilant screening of smear led to its identification and helped in further management.
CASE REPORTS
Case 1
A 60-year-old male presented with breathlessness and pain in abdomen since 1 month. Patient was admitted in our hospital and investigated with routine hematological examination, ultrasonography (USG) abdomen and contrast-enhanced computed tomography (CECT) thorax. Findings were suggestive of lung mass with multiple liver metastases and advised USG-guided FNAC.
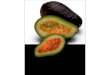
On USG-guided FNAC, hemorrhagic aspirate was obtained. Smears revealed moderately cellular aspirate and composed of neoplastic cells morphologically resembling adenocarcinoma cells. Background showed small clusters of benign hepatocytes, few chronic inflammatory cells and microfilarial parasites (Figs. 1 and 2). The diagnosis of metastatic epithelial malignancy of glandular origin with microfilaria was made.
Case 2
A 22-year-old male presented with a painless swelling of right arm, since 1 month with no other significant clinical symptom. On examination, a small subcutaneous swelling in right elbow of about 1.5 × 1 cm was noted. Swelling was firm, nontender and movable.

INTERNAL MEDICINE
536 Indian Journal of Clinical Practice, Vol. 25, No. 6, November 2014
FNAC was performed from the swelling, which yielded blood mixed aspirate. Smears revealed polymorphous cell population of small and large lymphoid cell along with numerous ensheathed coiled and slightly curved microfilaria (Figs. 3 and 4). A final diagnosis of reactive lymphoid hyperplasia with microfilaria was made. This patient took the treatment and remained asymptomatic after therapy.
DISCUSSION
Filariasis is a global health problem of huge magnitude. Adult worms are found in the lymphatic vessels and lymph nodes of human beings only, whereas larval forms (microfilaria) may circulate in the peripheral blood. Humans are exclusive and definitive host for W. bancrofti. The major vectors are Culex mosquitoes in most of the urban areas and Anopheles mosquitoes in rural areas. A significant number of infected individuals in endemic areas remain asymptomatic throughout their life.
Microfilaria displays nocturnal periodicity. That is why, three consecutive night blood samples are commonly used for its detection but considered less sensitive tools for its diagnosis. Other methods are circulating filarial antigen (CFA) detection test, which is now regarded as the gold standard and demonstration of organism in histopathological sections.3 FNAC are not applied for routine diagnosis of clinically suspected filariasis. Incidental detection on FNAC has been reported in cytological smears from almost any part of body and it is the most frequently diagnosed parasite and microfilaria is the most common form. The presence of microfilaria along with neoplasm is generally regarded as a chance association. In our case also, where there was a strong clinical suspicion of metastatic malignancy involving liver, microfilaria was a chance finding. This may be due to its transmigration along with metastatic emboli. It has also been suggested that such aberrant migration to these dead- end sites is probably determined by local factors such as lymphatic blockage by scars or tumors and damage to the vessel wall by inflammation, trauma
Figures 1 and 2. Clusters of neoplastic cells and microfilaria (MGG-40X).
Figures 3 and 4. Straight and curved microfilaria with lymphoid cells in the background (MGG-40X).

INTERNAL MEDICINE
537Indian Journal of Clinical Practice, Vol. 25, No. 6, November 2014
or stasis. Rich blood supply in the tumors could be a reason for concentration of parasites at these sites.3 Gupta has emphasized that microfilariae wander in tissue fluid and may get entrapped in needle during aspiration.4
Microfilariae have been reported in association with malignant lesions as well as benign lesions. Some malignant lesions where microfilariae have been detected are Ewing’s sarcoma of the bone, non-Hodgkin’s lymphoma, squamous cell carcinoma of the maxillary antrum, craniopharyngioma of the third ventricle, transitional cell carcinoma of the bladder, follicular carcinoma of the thyroid, seminoma of undescended testis, etc.3 Benign lesion sites are breast, testis, epididymis, thyroid, lung, lymph nodes, skin, etc.4,5 Kumar et al6 reported a case of microfilaria in the supraclavicular lymph node in the background of malignant cells where the primary was in the stomach.In our case, the chance detection of microfilariae from liver in a case of metastatic malignancy and from isolated swelling in the epitrochlear region, which is an infrequent site for lymphadenopathy signifies the value of FNAC and careful screening of the smears in the detection of asymptomatic and clinically unsuspected cases of filariasis.
AcknowledgmentI take this opportunity to extend my gratitude and sincere thanks to all those who helped me to complete this study.
I am highly thankful to Dept. of Pathology, Medicine, Microbiology and Radiology department for providing me adequate facility, which helped me to carry out this study. I owe great sense of indebtedness to Dean (SRMS-IMS), Bhojipura, Bareilly for permitting me to carry out this study.
REFERENCES
1. Park K. Lymphatic filariasis, epidemiology of communicable diseases. In: Textbook of Preventive and Social Medicine. 22nd edition, Banarasidas Bhanot Publishers: Jabalpur; pg.245.
2. R Veena Kumar, R Sridhar Reddy. Adult filarial worms in tissue sections of a painless breast mass. J Cont Med A Dent 2014;2(1):48-50.
3. Katti TV, Athanikar VS, Ananthrao AS, Rathod CV. Cytodiagnosis of microfilarial lymphadenitis coexistent with metastatic squamous cell carcinoma in a left cervical lymph node: An unusual presentation. Ann Nigerian Med 2012;6:47-9.
4. Gupta S, Gupta R, Bansal B, Singh S, Gupta K, Kudesia M. Significance of incidental detection of filariasis on aspiration smears: a case series. Diagn Cytopathol 2010;38(7):517-20.
5. Garg PK, Jain BK, Rathi V, Singh N, Mohanty D. Mid-arm and epitrochlear lymphadenopathy: a clinico-radiological surprise. J Infect Dev Ctries 2011;5(11):820-4.
6. Kumar R. Microfilariae in lymph node aspirate associated with metastatic gastric carcinoma: a case report. Acta Cytol 2010;54(3):319-20.
■ ■ ■ ■
Atrial Fibrillation Doubles Risk for Silent Stroke
Atrial fibrillation (AF) is associated with a more than two-fold increase in the odds for silent cerebral infarction (SCI), or a stroke that has no outward signs or symptoms, according to a review being published in Annals of Internal Medicine. AF is the most common arrhythmia in the elderly, affecting more than 2.7 million Americans. Patients with AF have up to five times greater risk for stroke and poorer post-stroke outcomes than those without AF. Research indicates that AF is associated with a 40% increase in the risk for cognitive impairment, independent of a history of symptomatic stroke and comorbid conditions, suggesting another underlying cause, such as SCI.
Bleeding Risks in Patients with Atrial Fibrillation
Two new studies have provided more data on the bleeding risks among patients with atrial fibrillation (AF) treated with dabigatran, with one showing that the oral anticoagulant carries a significantly higher risk of major bleeding, as well as gastrointestinal bleeding, when compared with warfarin. The first report is published in JAMA: Internal Medicine while the second one is published in Circulation. In the second report, there was no increased risk of major bleeding with dabigatran, but there was a 28% greater risk of gastrointestinal hemorrhage.