Embed Size (px)
Citation preview

SALUD PREVENTIVA
DDA´S PARADIGM IN HCV TREATMENT
VIROLOGY EDUCATION SAN JUAN, PUERTO RICO
Dr. David KershenobichDirector General

Eradication: Incidence zero of HCV infection and decrease in cirrhosis and hepatocarcinoma. The concept of eradication is to eliminate HCV of the earth.
Andres Marco Rev Enf Emerg 2015
Control:Decrease the incidence of cirrhosisand hepatocarcinoma, as well as theincidence of HCV.
Elimination:Incidence zero in HCV infection and decrease of cirrhosis andhepatocarcinoma in a given area. The concept of elimination refersto the disappearance of the virus in an area, region, state orcountry

Worldwide prevalence of hepatitis C
3
71million
0.6%
The Polaris Observatory HCV Collaborators, Lancet Gastroenterol Hepatol 2017; 2: 161–76

Viral Hepatitis in the Americas
Data from GlobalBurden of Disease, 2016
Cooke et al. Lancet Gastroenterol Hepatol 2019; 4: 135–84

Prevalence of Anti-HCVin the Americas
Petruzziello et al. World J Gastroenterol 2016; 22(34): 7824-7840

BMC Med. 2014; 12: 145.
Liver Cirrhosis Mortality

• HCV is implicated in:
México
Cases of liver cirrhosis
Cases of hepatocarcinoma
Lozano R et al
Global Burden of Disease Study 2010
Lancet 2012;389:2095-128

¿Do we have an adequate drugto treat hepatitis C ?

Mangia A, et al. AASLD 2018; Poster #600
Genotype Fibrosis
1299/1319
RV
S12 (
%)
547/558
509/512
198/204
44/44
334/335
274/281
Efficacy of SOF/VEL for 12 weeksin real life

Efficacy of GLE/PIB for 8 o 12 weeksin real life
Wiegand J, et al. AASLD 2018; Poster #611
Genotype Fibrosis
592/609
RV
S1
2 (
%)
319/327
37/38
192/199
30/31
14/14
134/137
59/59
19/20

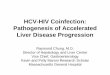
Pangenotypic Treatments for Hepatitis C
• SOF + DCV is licensed in the EU for the treatment of GT 1, 3 and 4, not GT 2, 5 and 6, chronic HCV infection. GLE/PIB for 16 weeks, not 12 weeks, is licensed in the EU for the treatment of GT 3 patients with prior PEG-IFN ± RBV ± SOF experience. Recommendations for people aged ≥18 years. aPeople with GT 3 infection who have received IFN and/or RBV in the past should be treated for 16 weeks; bSOF + DCV for 12 weeks may be considered in countries where genotype distribution is known and GT 3 prevalence is <5%; c12 weeks recommended for GT 3 patients with prior PEG-IFN ± RBV ± SOF experience; d12 weeks recommended for GT 3 patients with prior PEG-IFN ± RBV ± SOF experience; eIn GT 3 patients with cirrhosis where the Y93H RAS cannot be confirmed as absent, addition of RBV or treating with SOF/VEL/VOX recommended. DCV: daclatasvir; GLE: glecaprevir; GT: genotype; IFN: interferon; PEG-IFN: pegylated interferon; PIB: pibrentasvir; RAS: resistance associated substitution; RBV: ribavirin; SOF: sofosbuvir; VEL: velpatasvir; VOX: voxilaprevir
• WHO. Guidelines for the care and treatment of persons diagnosed with chronic hepatitis C virus infection. July 2018. Available at: http://apps.who.int/iris/bitstream/handle/10665/273174/9789241550345-eng.pdf?ua=1; EASL. J Hepatol 2018;69:461–511;
GLE/PIB SOF/VEL SOF + DCV
No cirrhosis Cirrhosis No cirrhosis Cirrhosis No cirrhosis Cirrhosis
8 weeks
16 weeks
12 weeks
16 weeks12 weeks 12 weeks
12 weeks
24 weeks
8 weeks
12 weeks
12 weeks
16 weeks12 weeks ± RBV — —

Requerimientos de los agentes antivirales de acción directa (AAD)
• Adapted from: Asselah T, et al. Liver Int 2018;38:7–13
ESSENTIAL FOR
EACH PATIENT
CRITICAL FOR
ELIMINATION
DELIVERY OF DAA`S
RVS >95%
Security
Tolerability
Pangenotypic
High resistance barrier
Short duration
Minimal pharmacological interactions
Less tablets
Treatment
High priority
Secondary
priorities

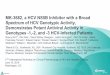
SVR
van der Meer AJ, et al. JAMA. 2012;308(24):2584-2593.
(%)
Hepatocellular carcinoma
Time in years
p<0.001
N=530 Without SVRl
With SVR
(%)Mortality related to the liver or liver transplantation
Time in years
p<0.001
N=530 Without SVR
With SVR

¿Do we have an adequate drugto treat hepatitis C?
yes

Searching for the missing patients
¿Are we prepared to carry out the diagnosis?
Only 14% of people with Hepatitis C in Latin America have been diagnosed and < 1% has received an adequate treatment

Point-of-care testing: Advantages
• Rapid testing.
• Allows testing and getting the result in the same visit.
• Can be done outside the clinical laboratories.
• Can be interpreted by non-specialists.
• Increases the number of patients tested andsimplifies the process of confirmation and referenceto treatment.

Point-of-care testing for hepatitis C
• Sensibility 95-99%
• Specificity 99-100%
• Results available in 5-10 minutes
• Easy to interpretJ Virol Methods 2018


FROM A TREATMENT STRATEGY TO THE ELIMINATION OF HEPATITIS C

Global Elimination of Hepatitis C
Lazarus J, et al. J Hepatol 2017;67:665–6
20
Industry
Direct antiviral
agents
Health
professionals
WHO
Legislators
Civil Society
Researchers

Elimination of HCV
Grebely J. EASL monothematic conference 2018; Oral #205020; Courtesy of the Kirby Institute, Sydney, Australia.
21
¿HOW?
¿With what?
Pangenotypic
simple therapy
¿Who?
Expand number of
treating physicians
¿Where?
Increase number of
treating centers
¿Regulations?
Simplification

Elimination of HCV by 2030
Global Health Sector Strategy on Viral Hepatitis, 2016 - 2021
22
Diagnosis of HCV
Treatment of VHC
20 400 60 80 100
(%)
2015 Basal
2030 Goals
90%
80%

Care Cascade for Hepatitis C patients
Yehia BR, et al. PLoS One 2014;9:e101554; WHO. Global health sector strategy on viral Hepatitis 2016–2021. Available at: http://apps.who.int/iris/bitstream/10665/246177/1/WHO-HIV-2016.06-eng.pdf?ua=1 (accessed March 2018)
23
100
0
20
40
60
80P
erc
en
tag
e
HC
V-P
AT
IEN
TS
Dia
gn
ose
d
Access
to
ca
re
TX SVR

Epidemiology of Hepatitis C in Latinamerica
Polaris Cascate 2017: Brazil, Mexico, Chile, Colombia and Argentina
1.905.300
442.000
27.200 80.000
Prevalence Diagnosed patients Treated patients in 2015 Patients treated by 2017
24

Yehia BR, et al. PLoS One 2014;9:e101554; WHO. Global health sector strategy on viral Hepatitis 2016–2021. Available at: http://apps.who.int/iris/bitstream/10665/246177/1/WHO-HIV-2016.06-eng.pdf?ua=1 (accessed March 2018)
25
HCV continuum of care
100
0
20
40
60
80H
CV
PA
TIE
NT
S
Dia
gn
ose
d
Acce
sto
cre
TXSVR
90 % reduction of new infections
90 % of diagnosed patients
80% elegible for treatment
Dia
gn
ose
d
Care Cascade for Hepatitis C patients
Pe
rce
nta
ge

Micro-elimination Strategies
• Lazarus J, et al. J Hepatol 2017;67:665–6
• More realistic objectives and goals. • Can be achived in a shorter period of time. • Tailored strategies. • Costs can be predicted. • Prevention of re-infections.

Models of Micro-Elimination in high riskpopulations
• Drug users
HIV/HCV co-infection
Migrants
Hospitals
Prisoners
Hemophilia
Men having sex with men
Transplanted patients
Cities
Dialysis
Chronic liver disease

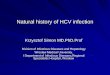
Number of tablets (excluding RBV)
• Gilead Sciences Europe Ltd. VOSEVI® (sofosbuvir/velpatasvir/voxilaprevir) SmPC, December 2018; Gilead Sciences Europe Ltd. EPCLUSA ® (sofosbuvir/velpatasvir) SmPC, December 2018; Merck Sharp & Dohme Ltd. ZEPATIER ® (grazoprevir/elbasvir) SmPC, June 2018; Gilead Sciences Europe Ltd. HARVONI ® (ledipasvir/sofosbuvir) SmPC, December 2018; Bristol-Myers Squibb Pharma EEIG. DAKLINZA ® (daclatasvir) SmPC, July 2018; AbbVie Ltd. MAVIRET ® (glecaprevir/pibrentasvir) SmPC, July 2018; AbbVie Ltd. EXVIERA ® (dasabuvir) SmPC, October 2018; AbbVie Ltd. VIEKIRAX ® (ombitasvir/paritaprevir/ritonavir) SmPC, September 2018.
• This comparison is for illustrative purposes only. Minimum and maximum number of pills have been calculated based on treatment durations recommended on the posologytable in the respective SmPCs. DAA-naïve patients without or with compensated cirrhosis.
• DCV: daclatasvir; DSV: dasabuvir; EBR: elbasvir; GRZ: grazoprevir; LDV: ledipasvir; OBV: ombitasvir; PTV; paritaprevir; r: ritonavir; RBV: ribavirin
5684 84
56
168 168 168
84 84112
168
336 336
672
0
175
350
525
700
SOF/VEL/VOX SOF/VEL EBR/GRZ LDV/SOF SOF + DCV GLE/PIB OBV/PTV/r ± DSV
Min Max
With
foodWith
food
With or
without
food
With or
without
food
With or
without
food
With or
without
food
With
food

Road to Simplicity
PATIENT
PHYSICIAN
ONE TABLET A DAY FOR 12 WEEKS
12 WEEKS DURATION OF TREATMENT FOR
ALL CASES
Treatment easy to explain and prescribe

Hepatitis C
Think globally
Act locallySimplify Transform

FROM A TREATMENT STRATEGY TO THE ELIMINATION OF HEPATITIS C

CONCLUSIONS
PARADIGM 1: It is possible to go from a treatment strategy to an elimination strategy of Hepatitis C.
PARADIGM 2: Think globally and act locally.
PARADIGM 3: The model of care of Hepatitis C most be transformed and simplified.
PARADIGM 4: We need an integral model of care for Hepatitis C.

FROM CURE TO ELIMINATIONOF HEPATITIS C