Embed Size (px)
DESCRIPTION
g
Citation preview

7/15/2019 Death Due to Neurogenic Shock Following Gastric
http://slidepdf.com/reader/full/death-due-to-neurogenic-shock-following-gastric 1/6
Death due to neurogenic shock following gastricrupture in an anorexia nervosa patient
I. Sinicina*, H. Pankratz, A. Buttner, G. Mall
Institute of Legal Medicine, Ludwig-Maximilians-University, Frauenlobstraße 7a, D-80337 Munich, Germany
Received 26 March 2004; accepted 26 October 2004
Available online 13 December 2004
Abstract
We report a case of fatal gastric rupture discovered after death, which developed due to a bulimic attack of a 19-year-old
woman suffering from anorexia nervosa. An autopsy revealed an acute gastric dilatation and rupture without commonly
observed ischemic damage of gastric wall structures. However, it may be difficult to determine the cause of death despite the
marked findings. The death as a consequence of neurogenic shock accounts for all the results of gross examination and histologic
analysis. This case is the first reported case of fatal gastric rupture of an anorectic patient discovered after death.
# 2004 Elsevier Ireland Ltd. All rights reserved.
Keywords: Gastric rupture; Anorexia; Binge eating; Fatal
1. Introduction
Anorexia nervosa is a common psychiatric condition of
adolescence in which, apart from the striking psychopathol-
ogy, somatic complications are frequently observed. The
disease has one of the highest death rates of any psychiatric
disorder. The documented crude mortality rates of anorexia
nervosa range from 3.3% in an 8-year follow-up study [1] to
18% in a 33-year outcome study [2]. Causes of death
reported for anorexia nervosa patients include complications
of the eating disorder such as inanition, electrolyte imbal-
ance, dehydration [3], suicide [1], and less commonly,
alcoholism [4]. There are two cases of fatal gastric rupturein anorectic patients reported by Lebriquir et al. [5] and Saul
et al. [6]. The young women treated by the authors died from
septic shock in consequence of surgical treatment. However,
acute gastric dilatation can often be observed in cases of
anorectic patients experiencing episodes of binge eating [7].
Yet only a few case reports exist concerning gastric necrosis
and consequent rupture following acute gastric dilatation
after binge eating [6,8–11].
The patients described in the literature attended a hospi-
tal with a chief complaint of increasing severe abdominal
pain. All patients were surgically treated and all but two
survived. In this paper, we report on a case of a young
anorectic woman who died suddenly and unexpectedly
following an episode of binge eating and we review previous
reports on the subject as well.
2. Case report
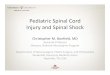
A 19-year-old woman was found dead kneeling at
the water-closet in the bathroom of her apartment. Her
left arm loosely hang into the closet, her head bent forward.
On external examination postmortal lividity was present
on the back of the thighs, on the legs below the knees, on
the face and on the forearms of the deceased (Fig. 1). Fully
established postmortem rigidity was observed in all parts
www.elsevier.com/locate/forsciint
Forensic Science International 155 (2005) 7–12
* Corresponding author. Tel.: +49 89 51605111;
fax: +49 89 51605144.
E-mail address: [email protected]
(I. Sinicina).
0379-0738/$ – see front matter # 2004 Elsevier Ireland Ltd. All rights reserved.
doi:10.1016/j.forsciint.2004.10.021

7/15/2019 Death Due to Neurogenic Shock Following Gastric
http://slidepdf.com/reader/full/death-due-to-neurogenic-shock-following-gastric 2/6
of the body. A faint green discoloration of the skin was
noted at the right abdominal wall. The cornea was slightly
clouded and the pupils showed a circular shape. No petechia
was observed in the palpebral conjunctiva. There were
no signs of any injury to the thoracic or abdominal walls.
The abdomen was remarkably distended. A slight edema
and strong hypostasis of the vaginal and anal entrances were
present, even resembling ‘‘fresh bruises’’. Signs of hema-temesis or vomit around the body or in the closet could not
be found.
The deceased had last been seen the previous evening.
She had been known to suffer from anorexia nervosa for 5
years. Her weight and her height were presently 43 kg and
155 cm, respectively.
Due to the nature of the case any sexual interference
could not be excluded. Photographs were taken and an
autopsy was carried out.
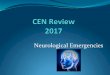
The postmortem examination revealed a massively dila-
tated stomach, extending from the xyphoid to the pubis, that
almost filled the entire abdominal cavity. A single 15 cm
perforation of the anterior wall of the gastric body was
detected (Fig. 2). Fresh hemorrhages surrounded the margin
of the rupture. The gastric wall was extremely thin, with a
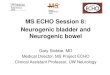
flattened mucosa. The external anterior surface of the sto-
mach was of a patchy reddish colour. About 5600 ml of
yellowish and brownish thick fluid were detected in the
abdominal cavity and in the stomach (Fig. 3). The gross
examination of the serous surface showed no fibrin forma-tion due to inflammation, except a slight injection of the
small subserous vessels. The small and large bowel were
both hypostatic. The right lung weighed 180 g, the left lung
155 g. The lungs showed a dry cut surface. The heart
weighed 165 g only, with a small amount of blood within
its cavities. The urinary bladder was empty.
The examination of the brain showed the signs of a slight
cerebral edema with a general flattening of the gyri, a filling
of the sulci and a discrete herniation of the cerebellar tonsils
through the foramen magnum.
The histological examination showed autolysis of the
gastric mucosa. Nevertheless, fresh intramural hemorrhages
I. Sinicina et al. / Forensic Science International 155 (2005) 7–128
Fig. 1. The position of the deceased.

7/15/2019 Death Due to Neurogenic Shock Following Gastric
http://slidepdf.com/reader/full/death-due-to-neurogenic-shock-following-gastric 3/6
I. Sinicina et al. / Forensic Science International 155 (2005) 7–12 9
Fig. 2. Gastric wall with fresh rupture.
Fig. 3. Gastric content recovered from the stomach and the abdominal cavitiy.

7/15/2019 Death Due to Neurogenic Shock Following Gastric
http://slidepdf.com/reader/full/death-due-to-neurogenic-shock-following-gastric 4/6
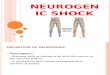
were found at the margins of the rupture without necrotic
areas or inflammatory infiltration. Some fresh ruptures of
intramural blood vessels were observed as well. A markedfibrous thickening of the entire gastric submucosa was
present (Fig. 4).
The myocardial cells were atrophic and narrow, the
collections of lipofuscin granules were present at the poles
of the nuclei. Areas with atrophic epicardial adipose tissue
were detected.
Occasionally strong granulocytic infiltration of the bron-
chial walls was seen. In some small areas of the lungs the
alveoli were contained some granulocytes and fibrin.
Toxicologic analysis failed to detect anydrugs, alcohol or
unusual substances.Death was attributed to neurogenic
shock in consequence of a gastric rupture.
3. Discussion
Anorexia nervosa is an eating disorder that may beaccompanied by episodes of binge eating. The food intake
during a bulimic attack can be enormous. Under physiologic
conditions the stomach contains up to 3 l fluid and/or food.
During binge eating attacks the stomach may harbour up to
12 l [8]. Gastric emptying and oesophageal motility are
impaired in patients with bulimic episodes. Thus, a bulimic
binge can become life-threatening if the stomach does not
empty spontaneously. The patients who developed an acute
gastric dilatation have a history of progressive abdominal
pain. Other symptoms such as an absent femoral pulses due
to markedly increased intraabdominal pressure can be pre-
sent. Vomiting may cause an acute increase in intragastric
I. Sinicina et al. / Forensic Science International 155 (2005) 7–1210
Fig. 4. Gastric wall with thickened gastric submucosa and freshly ruptured blood vessels (EvG, Â100).
Table 1
Reported cases of gastric rupture due to bulimic attack in anorexia nervosa
Number Author Year Gastric wall Surgical treatment Outcome
1 Evans [9] 1968 Necrosis Yes Recovery
2 Lebriquir et al. [5] 1978 Necrosis Yes Death (septic shock)
3 Saul et al. [6] 1981 Necrosis Yes Death (septic shock)
4 Abdu et al. [8] 1987 Necrosis Yes Recovery
5 Petrin et al. [10] 1990 Necrosis Yes Recovery
6 Willeke et al. [16] 1996 Necrosis Yes Recovery
7 Nakao et al. [17] 2000 Necrosis Yes Recovery
8 Present case 2003 No No Death (neurogenic shock)

7/15/2019 Death Due to Neurogenic Shock Following Gastric
http://slidepdf.com/reader/full/death-due-to-neurogenic-shock-following-gastric 5/6
pressure resulting in rupture, an extreme and relatively rare
complication of anorexia.
We found only six cases of acute gastric dilatation and
rupture (including our case) due to bulimic binging in
anorexia nervosa patients (Table 1). Rupture may be caused
by gastric wall necrosis secondary to ischemia, when the
wall tension exceeds the venous pressure. According to
Wolloch and Dinstman [12] gastric dilatation causes direct
mucosal necrosis. All case reports in Table 1, documented
gastric infarction and rupture and suggested that the obstruc-
tion of the venous outflow causes infarction and perforation
in acute gastric dilatation. In our case, no acute ischemic
damage of the mucosa was established by means of histo-
logical examination.
According to Ishikawa et al. [13], gastric ruptures are
usually located in the lesser curvature of stomach. In our
case, the rupture was located in the anterior wall of
the gastric body. An organic stenosis was found neither in
cardia nor in pylorus. In the English literature, the first deathfrom gastric perforation in a temporarily well-nourished
woman suffering from anorexia was reported by Saul
et al. [6].
In all described cases the patients were admitted to
the hospital with the symptoms of an acute abdomen. All
but two reported patients recovered after a surgical treat-
ment.
In our case, the autopsy revealed marked signs of sudden
death but no hemorrhage, no fibrin or abscess formation nor
peritoneal adhesions, indicating that the gastric rupture was
fatal within an extremely short period of time. Recently,
sudden and unexpected death of a 49-year-old, previouslyhealthy man due to the rupture of the stomach was reported
by Ishikawa et al. [13]. At the autopsy no convincing
morphological explanation of the cause of his death could
be found: no signs of hemorrhage or peritonitis were present.
The cause of death was determined as death from shock
caused by gastric rupture due to overeating. But what type of
shock should be considered?
Extreme gastric distension alone may cause a vaso-vagal
syncope. In our case, the young woman had obviously tried
to induce vomiting. The marked fibrous thickening of gastric
submucosa in our case is consistent with chronic ischemic
damage of the gastric wall. Thus, the deceased was used to
repeatedly occurring gastric distension following binge eat-ing.
Gastric rupture followed by release of approximately
5.6 l of stomach content into the peritoneal cavity leads
to the widespread peritoneal irritation and consequently to
the strong vagal activation. This activation induces general-
ized extensive peripheral vasodilatation and a decrease in
blood pressure along with bradycardia. Characteristically,
the resulting reduction in blood pressure is severe, sympa-
thetic activity is inhibited, plasma norepinephrine levels do
not increase, and the heart rate decreases. Transient sinus
arrest often follows. The defect is not a failure of the heart to
respond effectively to neurogenic or humoral excitatory
drive. Rather, it is a paradoxical interruption of sympathetic
excitation associated with parasympathetic excitation,
which causes profound vasodilatation and bradycardia.
Altogether these reactions result in neurogenic shock, a
distributive shock due to imbalance of sympathetic and
parasympathetic regulation of vascular smooth muscles
and heart rate.
Similar mechanisms are discussed in lethal outcomes
following striking on epigastrium [14,15]. Apart from the
acute gastric rupture, cardiac atrophy and focal pneumonia
were found in our case. A known laxative abuse and
repeatedly induced vomiting suggest at least temporary
hypovolaemia.
The combination of all the above factors with neurogenic
shock likely influenced the fatal outcome of gastric rupture
in our case.
Although fatal neurogenic shock is extremely rare and
very difficult to prove, forensic pathologists should be aware
of such a potential condition.
References
[1] G.C. Patton, Mortality in eating disorders, Psychol. Med. 18
(1988) 947–951.
[2] S. Theander, Chronicity in anorexia nervosa: results from the
Swedish long-term study, in: W. Herzog, H. Deter, Vander-
eyken (Eds.), The Course of Eating Disorders, Springer, New
York, 1992, pp. 217–227.
[3] W. Herzog, H.C. Deter, W. Fiehn, E. Petzold, Medical findings
and predictors of long-term physical outcome in anorexia
nervosa: a prospective 12-year follow-up study, Psychol.Med. 27 (1997) 269–279.
[4] C.E. Norring, S.S. Sohlberg, Outcome, recovery, relapse and
mortality across six years in patients with clinical eating
disorders, Acta Psychiatr. Scand. 87 (1993) 437–444.
[5] M. Lebriquir, E. Moirot, J.M. Droy, J.P. Rogez, J. Leroy, Acute
gastric dilatation and anorexia nervosa. Apropos of 2 cases, 1
with gastric rupture, Sem. Hop. 54 (1978) 1175–1176.
[6] S.H. Saul, A. Dekker, C.G. Watson, Acute gastric dilatation
with infarction and perforation. Report of fatal outcome
in patient with anorexia nervosa, Gut 22 (1981) 978–
983.
[7] G.E. Trott, T. Elliger, P. Kerscher, G. Nissen, Acute abdomen
in anorexia nervosa. A case report, Fortschr. Med. 108 (1990)
525–526.
[8] R.A. Abdu, D. Garritano, O. Culver, Acute gastric necrosis in
anorexia nervosa and bulimia. Two case reports, Arch. Surg.
122 (1987) 830–832.
[9] D.S. Evans, Acute dilatation and spontaneous rupture of the
stomach, Br. J. Surg. 55 (1968) 940–942.
[10] C. Petrin, G. Tacchetti, G. Preciso, F. Gallo, S. Bernardi, M.
Mion, Acute distension followed by gastric rupture after an
episode of bulimia, J. Chir. 127 (1990) 213–215.
[11] G.S. Roseborough, W.A. Felix, Disseminated intravascular
coagulation complicating gastric perforation in a bulimic
woman, Can. J. Surg. 37 (1994) 55–58.
[12] Y. Wolloch, M. Dintsman, Spontaneous rupture of the stomach,
Isr. J. Med. Sci. 9 (1973) 1574–1577.
I. Sinicina et al. / Forensic Science International 155 (2005) 7–12 11

7/15/2019 Death Due to Neurogenic Shock Following Gastric
http://slidepdf.com/reader/full/death-due-to-neurogenic-shock-following-gastric 6/6
[13] T. Ishikawa, S. Miyaishi, Y. Yamamoto, K. Yoshitome, S.
Inagaki, H. Ishizu, Sudden unexpected death due to rupture
of the stomach, Leg Med. 5 (2003) 60–64.
[14] Y. Furuya, K. Shintaku, T. Kita, Neurogenic shock caused by
striking on epigastrium, Igaku Kenkyu 49 (1979) 371.
[15] M. Ogata, K. Ago, M. Ago, O. Tsuganezawa, A case of death
due to neurogenic shock, Nippon Hoigaku Zasshi 46 (1992)152–158.
[16] F. Willeke, S. Riedl, A. von Herbay, H. Schmidt, V. Hoffmann,
J. Stern, Decompensated acute gastric dilatation caused by a
bulimic attack in anorexia nervosa, Dtsch. Med. Wochenschr.
121 (1996) 1220–1225.
[17] A. Nakao, H. Isozaki, H. Iwagaki, T. Kanagawa, N. Takakura,
N. Tanaka, Gastric perforation caused by a bulimic attack in an
anorexia nervosa patient: report of a case, Surg. Today 30(2000) 435–437.
I. Sinicina et al. / Forensic Science International 155 (2005) 7–1212