Embed Size (px)
Citation preview

Deep sedation in natural orifice transluminal endoscopic surgery(NOTES): a comparative study with dogs
Mohammad Al-Haddad • Daniel McKenna • Jeff Ko • Stuart Sherman •
Don J. Selzer • Samer G. Mattar • Thomas F. Imperiale • Douglas K. Rex •
Attila Nakeeb • Seong Mok Jeong • Cynthia S. Johnson • Lynetta J. Freeman
Received: 19 December 2011 / Accepted: 2 April 2012
� Springer Science+Business Media, LLC 2012
Abstract
Background Natural orifice transluminal endoscopic sur-
gery (NOTES) has been mostly performed with the animal
under general and inhalational anesthesia (IA-NOTES). To
date, NOTES using propofol sedation (PS-NOTES) has not
been investigated. This study aimed to assess the feasibility
and safety of PS-NOTES for transgastric oophorectomy
with carbon dioxide insufflation and to compare its success
rates with those of conventional IA-NOTES.
Methods In this prospective randomized study, NOTES
oophorectomy was performed for 19 female dogs random-
ized to two conditions: PS (study group) and IA (control
group). Sedation success rates (ability to visualize and resect
ovaries without converting to IA), operative success rates
(ability to resect and retrieve both ovaries in full using only
NOTES), and vital parameters including hemodynamic and
respiratory changes were documented.
Results In the PS-NOTES group (n = 9), the sedation
success rate was 100 %. The operative success rate was
67 % (6 of 9 animals) compared with 80 % (8 of 10 animals)
in the IA-NOTES group. No purposeful movement occurred
during surgical manipulation and no respiratory or cardio-
vascular complications in occured the PS group. Heart rate
(HR) and end-tidal carbon dioxide (ETCO2) were signifi-
cantly higher in the PS group than in the IA group. Blood
pressure (BP) was significantly higher in the PS group only
during the middle part of the procedure. Only mild respi-
ratory depression was noted in the PS group, as indicated by
elevated but acceptable ETCO2. Elevations in BP and HR
are thought to be related to elevated CO2 but did not appear
to have an adverse impact on the course of the procedure.
Recovery was uneventful for all the animals.
Conclusion The use of PS-NOTES appears to be feasible,
resulting in outcomes comparable with those for IA in
dogs. Further studies are needed to determine the appli-
cability of this concept in human NOTES.
Keywords Inhalational anesthesia � NOTES �Oophorectomy � Propofol sedation
Natural orifice transluminal endoscopic surgery (NOTES)
has emerged as an ‘‘incisionless’’ transvisceral approach to
the peritoneal cavity [1, 2]. The advantages that NOTES
has over conventional surgery include less postoperative
pain, fewer complications, decreased anesthesia require-
ments, accelerated patient recovery and return to normal
function, and elimination of the risk for incisional hernia-
tion. Despite the identification of barriers to human uses in
the first white paper [3], human NOTES applications
continue to expand rapidly under investigational settings at
a limited number of centers [4–15].
Presented as a poster at the Digestive Disease Week held in Chicago,
IL, USA between 7–10 May 2011.
M. Al-Haddad (&) � S. Sherman � T. F. Imperiale � D. K. Rex
Department of Medicine, Division of Gastroenterology, Indiana
University School of Medicine, 550 N University Boulevard,
UH 4100, Indianapolis, IN 46202, USA
e-mail: [email protected]
D. McKenna � D. J. Selzer � S. G. Mattar � A. Nakeeb
Department of Surgery, Indiana University School of Medicine,
Indianapolis, IN, USA
J. Ko � S. M. Jeong � L. J. Freeman
Purdue University School of Veterinary Medicine,
West Lafayette, IN, USA
C. S. Johnson
Division of Biostatistics, Indiana University School of Medicine,
Indianapolis, IN, USA
123
Surg Endosc
DOI 10.1007/s00464-012-2309-1
and Other Interventional Techniques

Similar to laparoscopy, to date, human NOTES has been
performed with the patient under general anesthesia for
hemodynamic and ventilating reasons. The increased
intraabdominal pressure from carbon dioxide (CO2)
insufflation during laparoscopy adversely affects the
hemodynamic stability of the patients by preventing
venous return and reducing cardiac output [16]. Further-
more, the increased abdominal pressure displaces the dia-
phragm cephalad, reducing lung’s vital capacity during
surgery and the early postoperative period [17–19]. Post-
operative pain after laparoscopic procedures also could be
at least partially attributed to insufflation of CO2.
A proposed benefit of NOTES is that it requires minimal
intraabdominal CO2 insufflation for visualization of struc-
tures and performance of procedures, and this combined with
less abdominal trauma could partly explain the reduced need
for postoperative analgesics in the clinical cases of NOTES
cholecystectomy performed recently [20]. Our group has
demonstrated that NOTES oophorectomy can be performed
easily with the subject under a CO2 insufflation pressure of 10
to 12 mmHg, which is lower than the 14 mmHg of pressure
required for the same procedure performed via laparoscopy
[21]. Reduced insufflation pressures with NOTES procedures
may preserve total lung capacity and maintain hemodynamic
stability of the anesthetized patient without the need for
assisted ventilation during the procedure [22].
We recently have demonstrated that NOTES oopho-
rectomy allows earlier recovery than open and laparoscopic
approaches [23, 24]. This has led to the assumption that
sedation rather than general anesthesia may be feasible for
NOTES due to the lower insufflation pressures compared
with laparoscopy.
Conscious sedation with or without local anesthesia has
been used successfully on a limited scale in gynecologic
and general surgical procedures [25–27]. A few NOTES
case reports have introduced this concept for a percutane-
ous endoscopic gastrostomy (PEG) rescue in one case [28]
and for peritoneoscopy in another case [29]. Propofol is a
short-acting hypnotic agent with the advantage of rapid
onset and offset of sedation as well as faster recovery of
neuropsychiatric function [30–33]. Its safety and effec-
tiveness for gastrointestinal (GI) procedures have been well
described in large studies and endorsed by the various GI
societies [30–32, 34–36]. Moreover, propofol use has
facilitated the performance of complex endoscopic inter-
ventions in which traditional conscious sedation could be
inadequate [37] and for high-risk patients [38].
Our hypothesis that NOTES can be performed with the
patient under deep sedation was derived from previous
observations of NOTES oophorectomy performed in dogs.
This study aimed to assess the feasibility and safety of
NOTES oophorectomy using propofol sedation (PS) com-
pared with general inhalational anesthesia (IA).
Methods
Animal model
The study was approved by Indiana University and Purdue
University Institutional Animal Care and Use Committees
(IACUC). A local animal shelter provided all the animals
for the study. The study used 20 healthy female dogs
weighing 11.6–26.4 kg. The animals were randomized into
blocks with procedures consecutively performed on all the
animals in the same group (PS or IA). One dog initially
assigned to the PS group was excluded when the preop-
erative exam showed a spaying scar. At completion of the
monitoring period, the dogs were returned to the same
shelter for adoption.
Study definitions
Sedation success with PS-NOTES was defined as the
ability to visualize and complete ovarian resection without
respiratory or hemodynamic compromise necessitating
conversion to general IA for completion of the procedure.
Operative success was defined as complete resection and
retrieval of both ovaries and gastric closure using the
NOTES technique.
Sedation, anesthesia, and monitoring
All the animals were fasted for 24 h, and baseline values for
heart rate, respiratory rate, and temperature were obtained.
In the PS-NOTES group, a loading dose of propofol (3 mg/
kg) was administered intravenously (IV) followed by inter-
mittent boluses (*1 mg/kg given every 1–2 min) for
maintenance titered to a desired depth of sedation and vital
parameters. The trachea was not intubated in this group, and
a sampling catheter was placed in the proximal trachea to
obtain a sample of expired air for end-tidal CO2. Supple-
mental oxygen also was provided, and the animals breathed
spontaneously without ventilation. The a priori criteria for
conversion from PS to IA included any sustained hemody-
namic or respiratory compromise or excessive animal
movement impairing the progress of the procedure.
The dogs in the IA group were premedicated with ace-
promazine 0.02 mg/kg and hydromorphone 0.1 mg/kg
followed by propofol induction (6 mg/kg, IV), endotra-
cheal intubation, isoflurane anesthesia, and periodic man-
ual ventilation. Mechanical ventilation then was used, and
end-tidal CO2 was maintained between 35 and 40 mmHg.
Overall and segment-specific procedure durations were
tabulated, and vital signs including heart rate (HR), mean
blood pressure (BP), respiratory rate (RR), oxygen satu-
ration (SpO2) levels, and end-tidal partial pressure of CO2
(ETCO2) levels were recorded every 5 min in each group.
Surg Endosc
123
The animals were positioned in dorsal recumbency on a
circulating water blanket to prevent anesthesia-induced
hypothermia. Intravenous fluids were given during the
procedure. Perioperative antibiotics (cefazolin 22 mg/kg
IV every 2 h intraoperatively) were given, and aseptic
procedures for clipping, preparing, and draping of the
abdomen were followed. The endoscopes and other
equipment underwent high-level disinfection after every
use. An overtube (U.S. Endoscopy, Mentor, OH, USA) was
used to reduce oral contamination. Both groups received
carprofen (4 mg/kg, subcutaneously) preoperatively and
24 h postoperatively for analgesia. The dogs were given
hydromorphone 0.05 mg/kg intramuscularly (IM) at the
end of the surgical procedure for postoperative analgesia. A
second dose of hydromorphone 0.05 mg/kg IM was
administered 6 h after surgery.
Postoperatively, each animal was monitored in recovery
until its body temperature was higher than 37.2 �C. Post-
operatively, the heart rate, respiratory rate, temperature, and
indirect blood pressure were recorded every 6 h. The ani-
mals were monitored for 48 h for postoperative pain and
complications before they were returned to the local shelter.
NOTES procedure
Starting with the IA group, NOTES oophorectomy was
performed as we have previously described (Fig. 1) [24].
After a flexible therapeutic endoscope (Olympus GIF 2T-
160; Olympus America Inc., Center-Valley, PA, USA) had
been passed into the stomach, cefazolin (1 g in 200 ml of
normal saline) was instilled for 10 min and then aspirated.
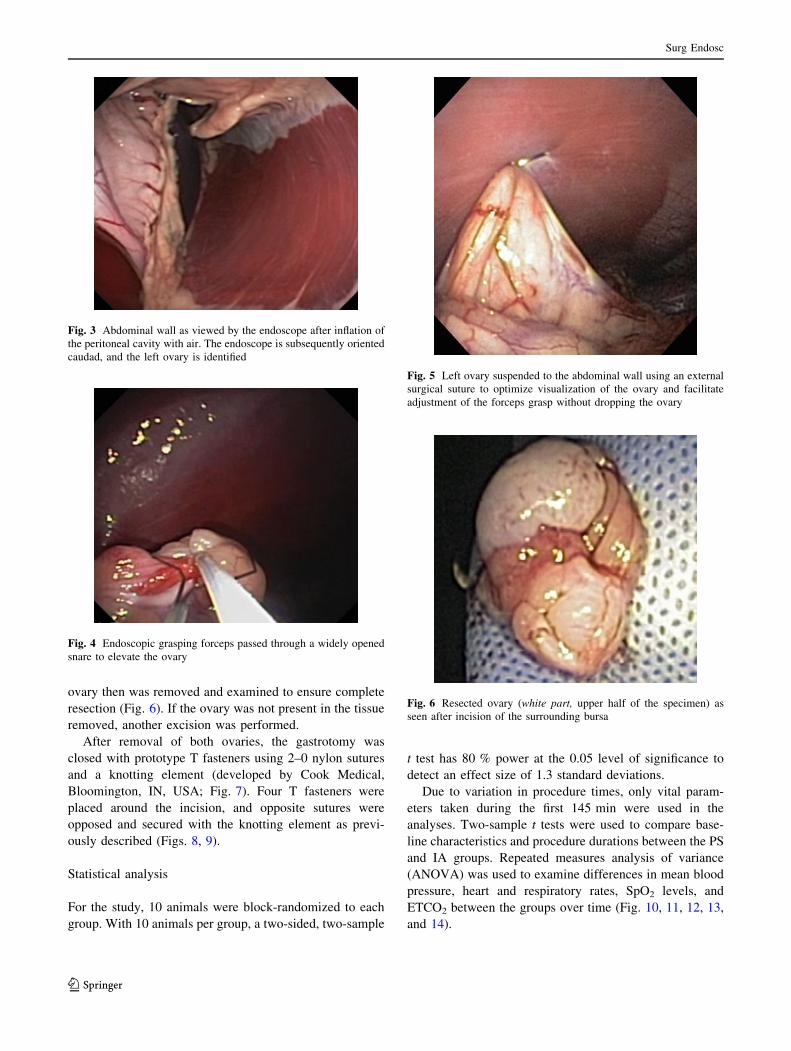
The gastrotomy was performed using an endoscopic bal-
loon dilator (CRE Esophageal/Colonic Wire-Guided Bal-
loon; Boston Scientific Corporation, Natick, MA, USA)
advanced over a percutaneously inserted guidewire to
create a 20 mm gastrotomy (Fig. 2) [24]. The endoscope
was passed into the abdominal cavity, and air insufflation
via the endoscope was provided (Fig. 3). Another 18-gauge
catheter was placed in the peritoneal cavity, and CO2
insufflation was provided by a standard laparoscopic
insufflator (Karl Storz Veterinary 183 Endoscopy America,
Goletta, CA, USA) with the pressure set to 10 mmHg in
addition to air from the endoscope. An alarm sounded
when the intraabdominal pressure exceeded 10 mmHg or
decreased to \8 mmHg.
The animal’s position was adjusted to expose each
ovary. A 3.0 9 4.5 cm hexagonal snare (AcuSnare; Cook
Medical Inc., Bloomington, IN, USA) was passed through
one of the working channels of the endoscope, and endo-
scopic grasping forceps (Polygrab Tripod; Olympus
Endoscopy, Center-Valley, PA, USA) were passed into the
second channel. Together, these instruments were used to
elevate and loop the ovary (Fig. 4).
The ovary was suspended to the abdominal wall using a
surgical suture and inspected before initiation of cautery
(Fig. 5). If needed, the ovary was released and resuspended
to achieve the optimum resection level. The blood supply
then was coagulated and transected using monopolar
electrocautery at 20–40 W of blended current (Endostat II
electrosurgical generator; Boston Scientific Corp.). The site
was examined for hemorrhage. When encountered, hem-
orrhage was treated by attempted endoscopic cautery. Each
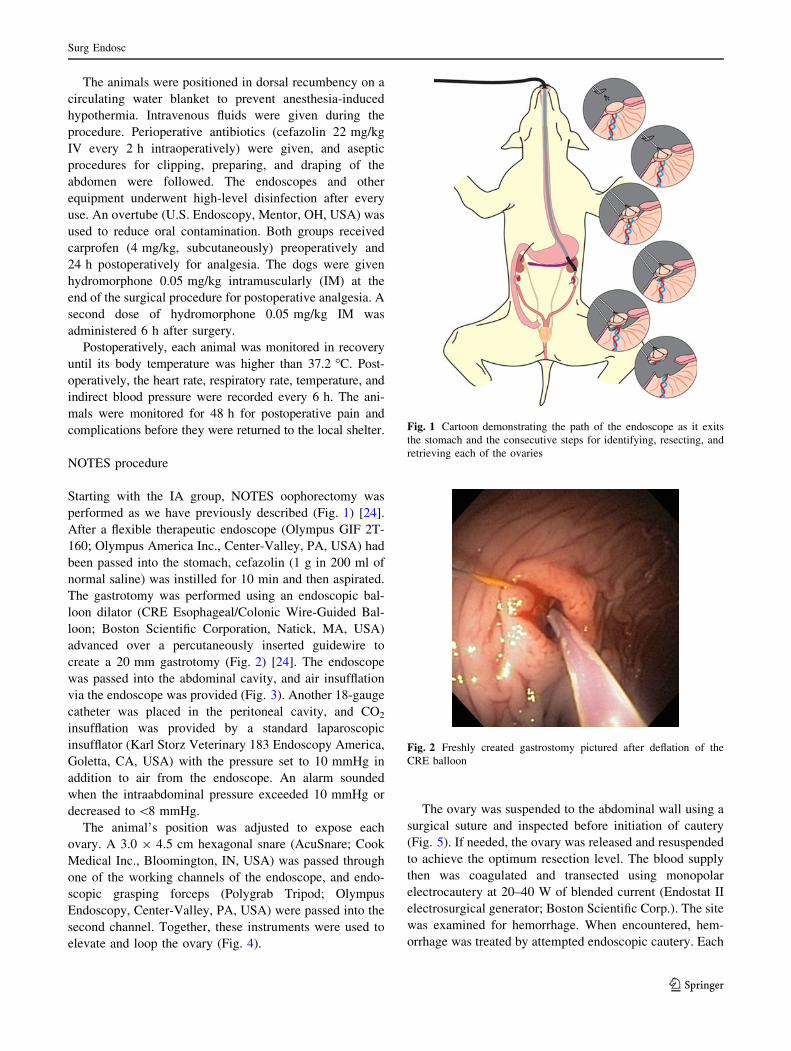
Fig. 1 Cartoon demonstrating the path of the endoscope as it exits
the stomach and the consecutive steps for identifying, resecting, and
retrieving each of the ovaries
Fig. 2 Freshly created gastrostomy pictured after deflation of the
CRE balloon
Surg Endosc
123
ovary then was removed and examined to ensure complete
resection (Fig. 6). If the ovary was not present in the tissue
removed, another excision was performed.
After removal of both ovaries, the gastrotomy was
closed with prototype T fasteners using 2–0 nylon sutures
and a knotting element (developed by Cook Medical,
Bloomington, IN, USA; Fig. 7). Four T fasteners were
placed around the incision, and opposite sutures were
opposed and secured with the knotting element as previ-
ously described (Figs. 8, 9).
Statistical analysis
For the study, 10 animals were block-randomized to each
group. With 10 animals per group, a two-sided, two-sample
t test has 80 % power at the 0.05 level of significance to
detect an effect size of 1.3 standard deviations.
Due to variation in procedure times, only vital param-
eters taken during the first 145 min were used in the
analyses. Two-sample t tests were used to compare base-
line characteristics and procedure durations between the PS
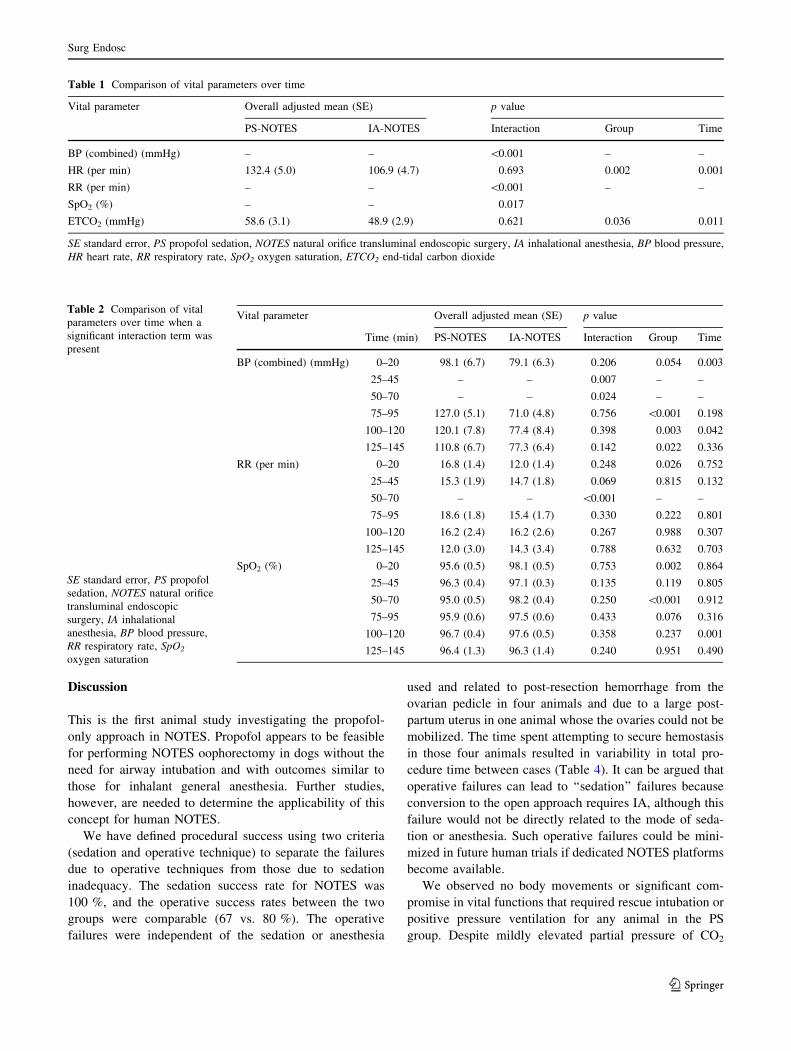
and IA groups. Repeated measures analysis of variance
(ANOVA) was used to examine differences in mean blood
pressure, heart and respiratory rates, SpO2 levels, and
ETCO2 between the groups over time (Fig. 10, 11, 12, 13,
and 14).
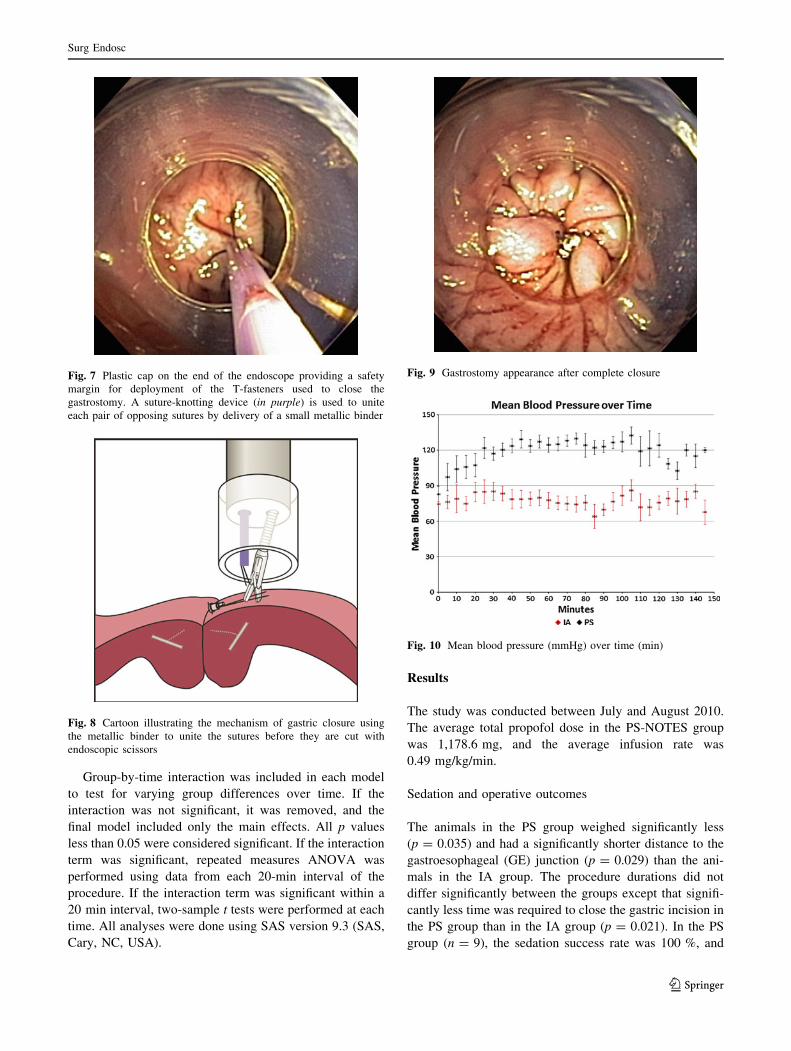
Fig. 3 Abdominal wall as viewed by the endoscope after inflation of
the peritoneal cavity with air. The endoscope is subsequently oriented
caudad, and the left ovary is identified
Fig. 4 Endoscopic grasping forceps passed through a widely opened
snare to elevate the ovary
Fig. 5 Left ovary suspended to the abdominal wall using an external
surgical suture to optimize visualization of the ovary and facilitate
adjustment of the forceps grasp without dropping the ovary
Fig. 6 Resected ovary (white part, upper half of the specimen) as
seen after incision of the surrounding bursa
Surg Endosc
123
Group-by-time interaction was included in each model
to test for varying group differences over time. If the
interaction was not significant, it was removed, and the
final model included only the main effects. All p values
less than 0.05 were considered significant. If the interaction
term was significant, repeated measures ANOVA was
performed using data from each 20-min interval of the
procedure. If the interaction term was significant within a
20 min interval, two-sample t tests were performed at each
time. All analyses were done using SAS version 9.3 (SAS,
Cary, NC, USA).
Results
The study was conducted between July and August 2010.
The average total propofol dose in the PS-NOTES group
was 1,178.6 mg, and the average infusion rate was
0.49 mg/kg/min.
Sedation and operative outcomes
The animals in the PS group weighed significantly less
(p = 0.035) and had a significantly shorter distance to the
gastroesophageal (GE) junction (p = 0.029) than the ani-
mals in the IA group. The procedure durations did not
differ significantly between the groups except that signifi-
cantly less time was required to close the gastric incision in
the PS group than in the IA group (p = 0.021). In the PS
group (n = 9), the sedation success rate was 100 %, and
Fig. 7 Plastic cap on the end of the endoscope providing a safety
margin for deployment of the T-fasteners used to close the
gastrostomy. A suture-knotting device (in purple) is used to unite
each pair of opposing sutures by delivery of a small metallic binder
Fig. 8 Cartoon illustrating the mechanism of gastric closure using
the metallic binder to unite the sutures before they are cut with
endoscopic scissors
Fig. 9 Gastrostomy appearance after complete closure
Fig. 10 Mean blood pressure (mmHg) over time (min)
Surg Endosc
123

the operative success rate was 67 % (6 of 9 animals)
compared with 80 % in the IA group (8 of 10 animals).
The five operative failures were related to inadequate
hemostasis of the ovarian pedicle in four animals (2 in each
group) and inability to mobilize the ovary due to uterine size in
one animal (PS group). These failures were resolved by con-
version to open laparotomy with the animal under general IA.
There was one episode of desaturation lasting less than
1 min that required removal and repositioning of the
esophageal overtube in the first PS-NOTES animal. There
was no purposeful movement during surgical manipulation,
and no respiratory or cardiovascular adverse events were
encountered in either group. Recovery was uneventful,
with no need for rescue analgesia or postoperative com-
plications in any animal.
Vital parameters
Heart rate and ETCO2 were significantly higher in the PS
group (p = 0.002) than in the IA group (p = 0.036). There
were significant group-by-time interactions for mean blood
pressure (p \ 0.001), respiratory rate (p \ 0.001), and
SpO2 (p = 0.017) (Table 1). The mean blood pressure did
not differ significantly between the groups during the first
20 min of the procedure or after 70 min (Table 2). The
animals in the PS group had a significantly higher mean
blood pressure than the animals receiving IA for
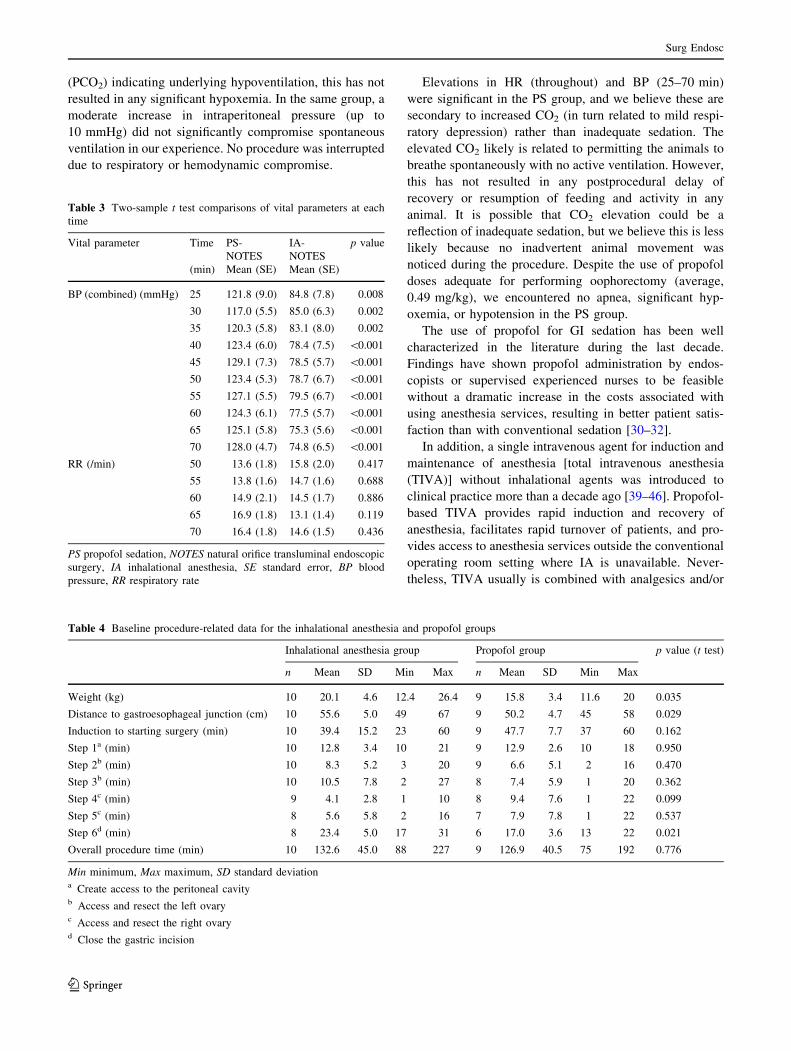
25–70 min (Table 3). The animals receiving PS had a
significantly higher respiratory rate than the animals
receiving IA during the first 20 min of the procedure
(Table 1), but the respiratory rates did not differ signifi-
cantly between the groups after 20 min (Tables 2, 3).
During the first 20 min, and again between 50 and 70 min,
the animals receiving PS had a significantly greater SpO2
than the animals receiving IA. At other times during the
procedure, the SpO2 did not differ significantly between the
groups
Fig. 11 Mean heart rate over time (min)
Fig. 12 Mean respiratory rate over time (min)
Fig. 13 Mean oxygen saturation (SpO2) (mmHg) over time (min)
Fig. 14 Mean end-tidal carbon dioxide (CO2) (mmHg) over time
(min)
Surg Endosc
123
Discussion
This is the first animal study investigating the propofol-
only approach in NOTES. Propofol appears to be feasible
for performing NOTES oophorectomy in dogs without the
need for airway intubation and with outcomes similar to
those for inhalant general anesthesia. Further studies,
however, are needed to determine the applicability of this
concept for human NOTES.
We have defined procedural success using two criteria
(sedation and operative technique) to separate the failures
due to operative techniques from those due to sedation
inadequacy. The sedation success rate for NOTES was
100 %, and the operative success rates between the two
groups were comparable (67 vs. 80 %). The operative
failures were independent of the sedation or anesthesia
used and related to post-resection hemorrhage from the
ovarian pedicle in four animals and due to a large post-
partum uterus in one animal whose the ovaries could not be
mobilized. The time spent attempting to secure hemostasis
in those four animals resulted in variability in total pro-
cedure time between cases (Table 4). It can be argued that
operative failures can lead to ‘‘sedation’’ failures because
conversion to the open approach requires IA, although this
failure would not be directly related to the mode of seda-
tion or anesthesia. Such operative failures could be mini-
mized in future human trials if dedicated NOTES platforms
become available.
We observed no body movements or significant com-
promise in vital functions that required rescue intubation or
positive pressure ventilation for any animal in the PS
group. Despite mildly elevated partial pressure of CO2
Table 1 Comparison of vital parameters over time
Vital parameter Overall adjusted mean (SE) p value
PS-NOTES IA-NOTES Interaction Group Time
BP (combined) (mmHg) – – \0.001 – –
HR (per min) 132.4 (5.0) 106.9 (4.7) 0.693 0.002 0.001
RR (per min) – – \0.001 – –
SpO2 (%) – – 0.017
ETCO2 (mmHg) 58.6 (3.1) 48.9 (2.9) 0.621 0.036 0.011
SE standard error, PS propofol sedation, NOTES natural orifice transluminal endoscopic surgery, IA inhalational anesthesia, BP blood pressure,
HR heart rate, RR respiratory rate, SpO2 oxygen saturation, ETCO2 end-tidal carbon dioxide
Table 2 Comparison of vital
parameters over time when a
significant interaction term was
present
SE standard error, PS propofol
sedation, NOTES natural orifice
transluminal endoscopic
surgery, IA inhalational
anesthesia, BP blood pressure,
RR respiratory rate, SpO2
oxygen saturation
Vital parameter Overall adjusted mean (SE) p value
Time (min) PS-NOTES IA-NOTES Interaction Group Time
BP (combined) (mmHg) 0–20 98.1 (6.7) 79.1 (6.3) 0.206 0.054 0.003
25–45 – – 0.007 – –
50–70 – – 0.024 – –
75–95 127.0 (5.1) 71.0 (4.8) 0.756 \0.001 0.198
100–120 120.1 (7.8) 77.4 (8.4) 0.398 0.003 0.042
125–145 110.8 (6.7) 77.3 (6.4) 0.142 0.022 0.336
RR (per min) 0–20 16.8 (1.4) 12.0 (1.4) 0.248 0.026 0.752
25–45 15.3 (1.9) 14.7 (1.8) 0.069 0.815 0.132
50–70 – – \0.001 – –
75–95 18.6 (1.8) 15.4 (1.7) 0.330 0.222 0.801
100–120 16.2 (2.4) 16.2 (2.6) 0.267 0.988 0.307
125–145 12.0 (3.0) 14.3 (3.4) 0.788 0.632 0.703
SpO2 (%) 0–20 95.6 (0.5) 98.1 (0.5) 0.753 0.002 0.864
25–45 96.3 (0.4) 97.1 (0.3) 0.135 0.119 0.805
50–70 95.0 (0.5) 98.2 (0.4) 0.250 \0.001 0.912
75–95 95.9 (0.6) 97.5 (0.6) 0.433 0.076 0.316
100–120 96.7 (0.4) 97.6 (0.5) 0.358 0.237 0.001
125–145 96.4 (1.3) 96.3 (1.4) 0.240 0.951 0.490
Surg Endosc
123
(PCO2) indicating underlying hypoventilation, this has not
resulted in any significant hypoxemia. In the same group, a
moderate increase in intraperitoneal pressure (up to
10 mmHg) did not significantly compromise spontaneous
ventilation in our experience. No procedure was interrupted
due to respiratory or hemodynamic compromise.
Elevations in HR (throughout) and BP (25–70 min)
were significant in the PS group, and we believe these are
secondary to increased CO2 (in turn related to mild respi-
ratory depression) rather than inadequate sedation. The
elevated CO2 likely is related to permitting the animals to
breathe spontaneously with no active ventilation. However,
this has not resulted in any postprocedural delay of
recovery or resumption of feeding and activity in any
animal. It is possible that CO2 elevation could be a
reflection of inadequate sedation, but we believe this is less
likely because no inadvertent animal movement was
noticed during the procedure. Despite the use of propofol
doses adequate for performing oophorectomy (average,
0.49 mg/kg), we encountered no apnea, significant hyp-
oxemia, or hypotension in the PS group.
The use of propofol for GI sedation has been well
characterized in the literature during the last decade.
Findings have shown propofol administration by endos-
copists or supervised experienced nurses to be feasible
without a dramatic increase in the costs associated with
using anesthesia services, resulting in better patient satis-
faction than with conventional sedation [30–32].
In addition, a single intravenous agent for induction and
maintenance of anesthesia [total intravenous anesthesia
(TIVA)] without inhalational agents was introduced to
clinical practice more than a decade ago [39–46]. Propofol-
based TIVA provides rapid induction and recovery of
anesthesia, facilitates rapid turnover of patients, and pro-
vides access to anesthesia services outside the conventional
operating room setting where IA is unavailable. Never-
theless, TIVA usually is combined with analgesics and/or
Table 3 Two-sample t test comparisons of vital parameters at each
time
Vital parameter Time PS-
NOTES
IA-
NOTES
p value
(min) Mean (SE) Mean (SE)
BP (combined) (mmHg) 25 121.8 (9.0) 84.8 (7.8) 0.008
30 117.0 (5.5) 85.0 (6.3) 0.002
35 120.3 (5.8) 83.1 (8.0) 0.002
40 123.4 (6.0) 78.4 (7.5) \0.001
45 129.1 (7.3) 78.5 (5.7) \0.001
50 123.4 (5.3) 78.7 (6.7) \0.001
55 127.1 (5.5) 79.5 (6.7) \0.001
60 124.3 (6.1) 77.5 (5.7) \0.001
65 125.1 (5.8) 75.3 (5.6) \0.001
70 128.0 (4.7) 74.8 (6.5) \0.001
RR (/min) 50 13.6 (1.8) 15.8 (2.0) 0.417
55 13.8 (1.6) 14.7 (1.6) 0.688
60 14.9 (2.1) 14.5 (1.7) 0.886
65 16.9 (1.8) 13.1 (1.4) 0.119
70 16.4 (1.8) 14.6 (1.5) 0.436
PS propofol sedation, NOTES natural orifice transluminal endoscopic
surgery, IA inhalational anesthesia, SE standard error, BP blood
pressure, RR respiratory rate
Table 4 Baseline procedure-related data for the inhalational anesthesia and propofol groups
Inhalational anesthesia group Propofol group p value (t test)
n Mean SD Min Max n Mean SD Min Max
Weight (kg) 10 20.1 4.6 12.4 26.4 9 15.8 3.4 11.6 20 0.035
Distance to gastroesophageal junction (cm) 10 55.6 5.0 49 67 9 50.2 4.7 45 58 0.029
Induction to starting surgery (min) 10 39.4 15.2 23 60 9 47.7 7.7 37 60 0.162
Step 1a (min) 10 12.8 3.4 10 21 9 12.9 2.6 10 18 0.950
Step 2b (min) 10 8.3 5.2 3 20 9 6.6 5.1 2 16 0.470
Step 3b (min) 10 10.5 7.8 2 27 8 7.4 5.9 1 20 0.362
Step 4c (min) 9 4.1 2.8 1 10 8 9.4 7.6 1 22 0.099
Step 5c (min) 8 5.6 5.8 2 16 7 7.9 7.8 1 22 0.537
Step 6d (min) 8 23.4 5.0 17 31 6 17.0 3.6 13 22 0.021
Overall procedure time (min) 10 132.6 45.0 88 227 9 126.9 40.5 75 192 0.776
Min minimum, Max maximum, SD standard deviationa Create access to the peritoneal cavityb Access and resect the left ovaryc Access and resect the right ovaryd Close the gastric incision
Surg Endosc
123

benzodiazepines and muscle relaxants and typically
requires endotracheal intubation with positive ventilation
due to the risk of apnea associated with higher doses of
anesthetics.
None of these adjunct agents were used in the current
study, so we labeled the intervention as ‘‘sedation’’ rather
than anesthesia. Our data suggest that visceral resection can
be performed with the subject under deep sedation alone,
without the need for airway control, or combined with sys-
temic analgesics or muscle relaxants. In our opinion, the lack
of abdominal wall trauma (compared with open surgery) and
reduced intraperitoneal pressure (compared with laparos-
copy) is behind this observation in NOTES. Additionally,
there is evidence that propofol-based anesthesia is associated
with less increase in catecholamines, adrenocorticotropic
hormone, and cortisol intra- and postoperatively than inha-
lational agents [47, 48] which could have reduced the car-
diovascular burden of anesthesia in our study.
The study had some limitations. First, the limited
number of animals in each group may not have powered
the study sufficiently for comparison of the particular
outcomes we reported between the two groups, but we
believe that such results would hold true in a larger sample
due to the strength of the statistical significance.
Second, the study used block randomization of 10 ani-
mals each, starting with the IA group. The impact of the
timing in this case probably was minimal because our team
achieved the ‘‘plateau’’ of the learning curve earlier, as we
have demonstrated in a previous study [49]. For this study to
be applicable to humans, we are assuming that abdominal
wall compliance in humans and canines is similar. Never-
theless, few data exist to support this assumption. Moreover,
factors that could potentially alter abdominal wall compli-
ance in the dogs, such as previous pregnancy or weight loss,
were largely unknown for the animals selected for this study.
Additionally, we discovered after completion of the
study that the two groups were not well matched by weight
and that the animals in the IA group were significantly
heavier. Because all the animals were provided by the local
shelter, the investigators had limited control over the breed
or the weight of the animals sent for oophorectomy.
Finally, we did not closely track the recovery time in the
IA group to allow comparison with the PS group because
this study was designed mainly to assess sedation and
outcomes. We have previously reported on earlier post-
operative recovery and resumption of bowel function in
NOTES oophorectomy [21].
If further studies demonstrate the feasibility of the
described approach for humans, several advantages can be
achieved. The PS-NOTES approach could provide a way to
perform intraabdominal surgical interventions on an out-
patient basis or in an environment such as a battlefield,
in which a fully equipped hospital is not immediately
available. Additionally, this approach will provide further
advantages by circumventing the need for bulky IA
equipment, reducing costs due to a shorter hospital stay and
facilitating outpatient procedures.
Acknowledgments This study was funded by the NOSCAR (2010)
and the Glen A. Lehman Endowed Chair Fund in Gastroenterology.
Disclosures Mohammad Al-Haddad, Daniel McKenna, Jeff Ko,
Stuart Sherman, Don J Selzer, Samer G. Mattar, Thomas F. Imperiale,
Douglas K. Rex, Attila Nakeeb, Seong Mok Jeong, Cynthia S.
Johnson, and Lynetta J Freeman have no conflicts of interest or
financial ties to disclose.
References
1. Flora ED, Wilson TG, Martin IJ, O’Rourke NA, Maddern GJ
(2008) A review of natural orifice translumenal endoscopic sur-
gery (NOTES) for intra-abdominal surgery: experimental models,
techniques, and applicability to the clinical setting. Ann Surg
247:583–602
2. McGee MF, Rosen MJ, Marks J, Onders RP, Chak A, Faulx A
et al (2006) A primer on natural orifice transluminal endoscopic
surgery: building a new paradigm. Surg Innov 13:86–93
3. Rattner D, Kalloo A (2006) ASGE/SAGES Working Group on
Natural Orifice Translumenal Endoscopic Surgery, October 2005.
Surg Endosc 20:329–333
4. Horgan S, Thompson K, Talamini M, Ferreres A, Jacobsen G,
Spaun G et al. Clinical experience with a multifunctional, flexible
surgery system for endolumenal, single-port, and NOTES pro-
cedures. Surg Endosc 25:586–592
5. Inoue H, Minami H, Kobayashi Y, Sato Y, Kaga M, Suzuki M
et al. Peroral endoscopic myotomy (POEM) for esophageal
achalasia. Endoscopy 42:265–271
6. Lehmann KS, Ritz JP, Wibmer A, Gellert K, Zornig C, Burghardt
J et al. The German registry for natural orifice translumenal
endoscopic surgery: report of the first 551 patients. Ann Surg
252:263–270
7. Nau P, Anderson J, Yuh B, Muscarella P Jr., Christopher Ellison
E, Happel L et al. Diagnostic transgastric endoscopic periton-
eoscopy: extension of the initial human trial for staging of pan-
creatic head masses. Surg Endosc 24:1440–1446
8. Nikfarjam M, McGee MF, Trunzo JA, Onders RP, Pearl JP,
Poulose BK et al. Transgastric natural-orifice transluminal
endoscopic surgery peritoneoscopy in humans: a pilot study in
efficacy and gastrotomy site selection by using a hybrid tech-
nique. Gastrointest Endosc 72:279–283
9. Park PO, Bergstrom M. Transgastric peritoneoscopy and appen-
dectomy: thoughts on our first experience in humans. Endoscopy
42:81–84
10. Park PO, Bergstrom M, Rothstein R, Swain P, Ahmed I, Gomez
G et al. Endoscopic sutured closure of a gastric natural orifice
transluminal endoscopic surgery access gastrotomy compared
with open surgical closure in a porcine model: a randomized,
multicenter controlled trial. Endoscopy 42:311–317
11. Saad S, Schmischke D, Martin C, Schieren T. Hybrid laparo-
scopic colectomy with transluminal colonoscopic specimen
extraction: a step toward natural orifice surgery. Endoscopy
42(Suppl 2):E346–E347
12. Salinas G, Saavedra L, Agurto H, Quispe R, Ramirez E, Grande J
et al. Early experience in human hybrid transgastric and trans-
vaginal endoscopic cholecystectomy. Surg Endosc 24:1092–1098
Surg Endosc
123

13. Sylla P, Rattner DW, Delgado S, Lacy AM. NOTES transanal
rectal cancer resection using transanal endoscopic microsurgery
and laparoscopic assistance. Surg Endosc 24:1205–1210
14. Zornig C, Siemssen L, Emmermann A, Alm M, von Waldenfels
HA, Felixmuller C et al. NOTES cholecystectomy: matched-pair
analysis comparing the transvaginal hybrid and conventional
laparoscopic techniques in a series of 216 patients. Surg Endosc.
Epub 25 December 2010
15. Zorron R, Palanivelu C, Galvao Neto MP, Ramos A, Salinas G,
Burghardt J et al. International multicenter trial on clinical natural
orifice surgery–NOTES IMTN study: preliminary results of 362
patients. Surg Innov 17:142–158
16. Galizia G, Prizio G, Lieto E, Castellano P, Pelosio L, Imperatore
V et al (2001) Hemodynamic and pulmonary changes during
open, carbon dioxide pneumoperitoneum, and abdominal wall-
lifting cholecystectomy: a prospective, randomized study. Surg
Endosc 15:477–483
17. Chumillas MS, Ponce JL, Delgado F, Viciano V (1998) Pul-
monary function and complications after laparoscopic cholecys-
tectomy. Eur J Surg 164:433–437
18. Wallace DH, Serpell MG, Baxter JN, O’Dwyer PJ (1997) Ran-
domized trial of different insufflation pressures for laparoscopic
cholecystectomy. Br J Surg 84:455–458
19. Bures E, Fusciardi J, Lanquetot H, Dhoste K, Richer JP, Lacoste
L (1996) Ventilatory effects of laparoscopic cholecystectomy.
Acta Anaesthesiol Scand 40:566–573
20. Zorron R, Filgueiras M, Maggioni LC, Pombo L, Lopes Carvalho
G, Lacerda Oliveira A (2007) NOTES transvaginal cholecystec-
tomy: report of the first case. Surg Innov 14:279–283
21. Freeman LJ, Rahmani EY, Al-Haddad M, Sherman S, Chiorean
MV, Selzer DJ et al. Comparison of pain and postoperative stress
in dogs undergoing natural orifice transluminal endoscopic sur-
gery, laparoscopic, and open oophorectomy. Gastrointest Endosc
72:373–380
22. McGee MF, Rosen MJ, Marks J, Chak A, Onders R, Faulx A et al
(2007) A reliable method for monitoring intraabdominal pressure
during natural orifice translumenal endoscopic surgery. Surg
Endosc 21:672–676
23. Freeman L, Rahmani EY, Burgess RC, Al-Haddad M, Selzer DJ,
Sherman S, Constable P (2011) Evaluation of the learning curve
for natural orifice transluminal endoscopic surgery: bilateral
ovariectomy in dogs. Vet Surg 40(2):140–150
24. Freeman LJ, Rahmani EY, Sherman S, Chiorean MV, Selzer DJ,
Constable PD et al (2009) Oophorectomy by natural orifice
transluminal endoscopic surgery: feasibility study in dogs. Gas-
trointest Endosc 69:1321–1332
25. Pellicano M, Zullo F, Cappiello F, Di Carlo C, Cirillo D, Nappi C
(2000) Minilaparoscopic ovarian biopsy performed under con-
scious sedation in women with premature ovarian failure. J Re-
prod Med 45:817–822
26. Pellicano M, Zullo F, Fiorentino A, Tommaselli GA, Palomba S,
Nappi C (2001) Conscious sedation versus general anaesthesia
for minilaparoscopic gamete intra-Fallopian transfer: a prospec-
tive randomized study. Hum Reprod 16:2295–2297
27. Tytherleigh MG, Fell R, Gordon A (2004) Diagnostic conscious
pain mapping using laparoscopy under local anaesthetic and
sedation in general surgical patients. Surgeon 2:157–160
28. Marks JM, Ponsky JL, Pearl JP, McGee MF (2007) PEG ‘‘res-
cue’’: a practical NOTES technique. Surg Endosc 21:816–819
29. Lee CK, Lee SH, Chung IK, Lee TH, Kim HS, Park SH et al.
Human diagnostic transgastric peritoneoscopy with the submu-
cosal tunnel technique performed with the patient under con-
scious sedation (with video). Gastrointest Endosc 72:889–891
30. Rex DK (2006) Review article: moderate sedation for endoscopy:
sedation regimens for nonanaesthesiologists. Aliment Pharmacol
Ther 24:163–171
31. Rex DK, Heuss LT, Walker JA, Qi R (2005) Trained registered
nurses/endoscopy teams can administer propofol safely for
endoscopy. Gastroenterology 129:1384–1391
32. VanNatta ME, Rex DK (2006) Propofol alone titrated to deep
sedation versus propofol in combination with opioids and/or
benzodiazepines and titrated to moderate sedation for colonos-
copy. Am J Gastroenterol 101:2209–2217
33. Lichtenstein DR, Jagannath S, Baron TH, Anderson MA,
Banerjee S, Dominitz JA et al (2008) Sedation and anesthesia in
GI endoscopy. Gastrointest Endosc 68:815–826
34. Rex DK, Deenadayalu VP, Eid E, Imperiale TF, Walker JA,
Sandhu K et al (2009) Endoscopist-directed administration of
propofol: a worldwide safety experience. Gastroenterology
137:1229–1237 quiz 518–519
35. Dumonceau JM, Riphaus A, Aparicio JR, Beilenhoff U, Knape
JT, Ortmann M et al. European Society of Gastrointestinal
Endoscopy, European Society of Gastroenterology and Endos-
copy Nurses and Associates, and the European Society of Ana-
esthesiology Guideline: Nonanesthesiologist administration of
propofol for GI endoscopy. Endoscopy 42:960–974
36. Vargo JJ, Cohen LB, Rex DK, Kwo PY (2009) Position state-
ment: nonanesthesiologist administration of propofol for GI
endoscopy. Gastrointest Endosc 70:1053–1059
37. Imagawa A, Fujiki S, Kawahara Y, Matsushita H, Ota S, To-
moda T et al (2008) Satisfaction with bispectral index moni-
toring of propofol-mediated sedation during endoscopic
submucosal dissection: a prospective, randomized study. Endos
copy 40:905–909
38. Riphaus A, Stergiou N, Wehrmann T (2005) Sedation with pro-
pofol for routine ERCP in high-risk octogenarians: a randomized,
controlled study. Am J Gastroenterol 100:1957–1963
39. Collins SJ, Robinson AL, Holland HF (1996) A comparison
between total intravenous anaesthesia using a propofol/alfentanil
mixture and an inhalational technique for laparoscopic gynae-
cological sterilization. Eur J Anaesthesiol 13:33–37
40. Hogue CW Jr, Bowdle TA, O’Leary C, Duncalf D, Miguel R,
Pitts M et al (1996) A multicenter evaluation of total intravenous
anesthesia with remifentanil and propofol for elective inpatient
surgery. Anesth Analg 83:279–285
41. Matsumoto H, Shingu K, Numata K, Ogura S, Hanaoka K, Ito H
et al (1998) Total intravenous anesthesia with propofol is
advantageous than thiopental-sevoflurane anesthesia in the
recovery phase. Masui 47:1046–1058
42. Trinder TJ, Johnston JR, Lowry KG, Phillips AS, Cosgrove J
(1998) Propofol and alfentanil total intravenous anaesthesia: a
comparison of techniques for major thoracic surgery. Acta Ana-
esthesiol Scand 42:452–459
43. Juckenhofel S, Feisel C, Schmitt HJ, Biedler A (1999) TIVA mit
propofol/remifentanil oder balancierte anasthesie mit sevofluran/
fentanyl bei laparoskopischen operationen. Hamodynamik, au-
fwachverhalten und nebenwirkungen [TIVA with propofol-rem-
ifentanil or balanced anesthesia with sevoflurane-fentanyl in
laparoscopic operations: hemodynamics, awakening and adverse
effects]. Anaesthesist 48(11):807–812
44. Visser K, Hassink EA, Bonsel GJ, Moen J, Kalkman CJ (2001)
Randomized controlled trial of total intravenous anesthesia with
propofol versus inhalation anesthesia with isoflurane-nitrous
oxide: postoperative nausea with vomiting and economic analy-
sis. Anesthesiology 95:616–626
45. Rohm KD, Piper SN, Suttner S, Schuler S, Boldt J (2006) Early
recovery, cognitive function, and costs of a desflurane inhala-
tional vs a total intravenous anaesthesia regimen in long-term
surgery. Acta Anaesthesiol Scand 50:14–18
46. Lerman J, Johr M (2009) Inhalational anesthesia vs total intra-
venous anesthesia (TIVA) for pediatric anesthesia. Paediatr
Anaesth 19:521–534
Surg Endosc
123

47. Ledowski T, Bein B, Hanss R, Paris A, Fudickar W, Scholz J et al
(2005) Neuroendocrine stress response and heart rate variability:
a comparison of total intravenous versus balanced anesthesia.
Anesth Analg 101:1700–1705
48. Satani M, Hamada T, Nakada K, Umemoto Y, Fujii T, Takaki O
(2005) Comparison of total intravenous anesthesia and inhalation
anesthesia regarding hormonal responses during lung lobectomy.
Masui 54:1109–1115
49. Freeman L, Rahmani EY, Burgess RC, Al-Haddad M, Selzer DJ,
Sherman S et al. Evaluation of the learning curve for natural
orifice transluminal endoscopic surgery: bilateral ovariectomy in
dogs. Vet Surg 40:140–150
Surg Endosc
123





























