Embed Size (px)
Citation preview
Dermal and Dermal and Subcutaneous Subcutaneous
Tumors – Part IITumors – Part II
Adam Wray, D.O.Adam Wray, D.O.
June 28, 2005June 28, 2005
Kaposi’s SarcomaKaposi’s SarcomaFive Presentations: Five Presentations:
1. Classic1. Classic– Middle aged, European menMiddle aged, European men– Red, violaceous nodules on toes or soles.Red, violaceous nodules on toes or soles.– Coalesce to form plaques. Brawny edemaCoalesce to form plaques. Brawny edema– Later more widespread involvement esp soft Later more widespread involvement esp soft
palate. Periods of remission/involution.palate. Periods of remission/involution.
2. African Cutaneous2. African Cutaneous– Nodular infiltrating vascular masses of extremitiesNodular infiltrating vascular masses of extremities– Men 20-50 yrs. Endemic to Africa.Men 20-50 yrs. Endemic to Africa.– Locally aggressive.Locally aggressive.– Massive edema of legs and bone involvement.Massive edema of legs and bone involvement.
Kaposi’s SarcomaKaposi’s Sarcoma3. African Lymphadenopathic3. African Lymphadenopathic
– Lymph nodes with/without skin in Lymph nodes with/without skin in children <10.children <10.
– Fatal in < 2years.Fatal in < 2years.
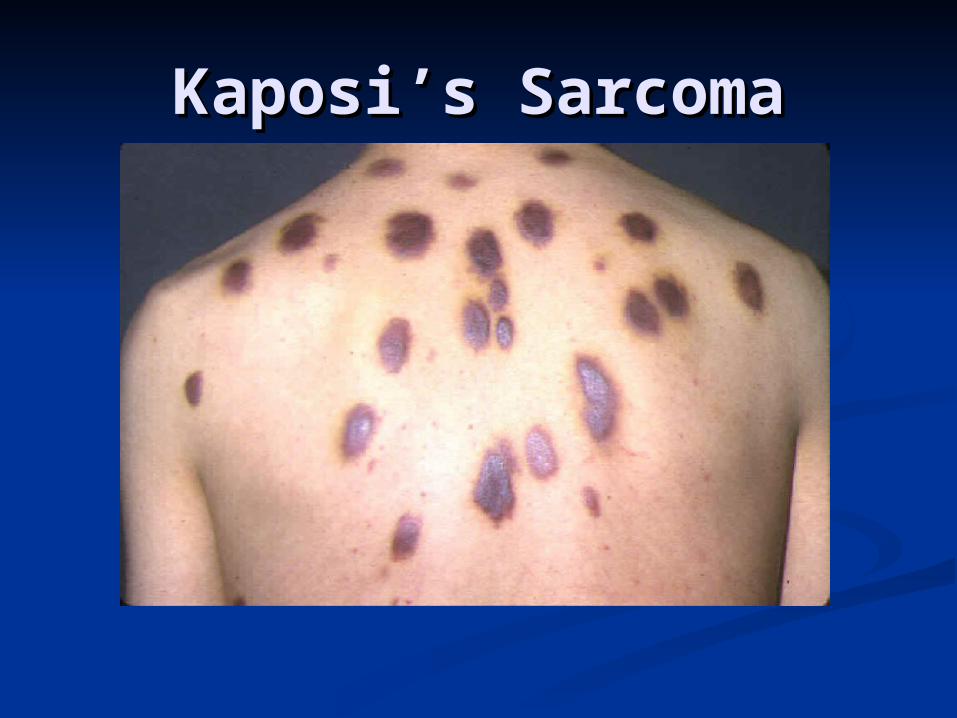
4. AIDS4. AIDS– Violaceous macules progress to Violaceous macules progress to
papules, nodules and plaques. papules, nodules and plaques. – Head, neck, trunk and mucous Head, neck, trunk and mucous
membranes.membranes.
5. Lymphoma / immunosuppressive 5. Lymphoma / immunosuppressive TX.TX.
Resembles classic but more variable Resembles classic but more variable presentation.presentation.

Kaposi’s SarcomaKaposi’s Sarcoma
Classic Variety.
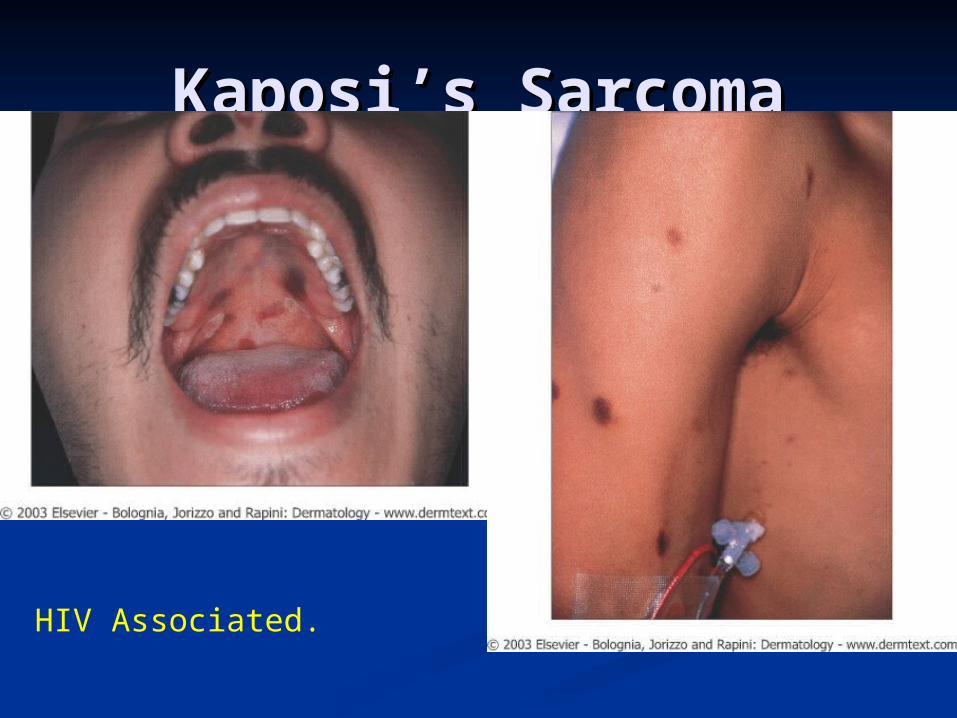
Kaposi’s SarcomaKaposi’s Sarcoma
HIV Associated.
Kaposi’s SarcomaKaposi’s Sarcoma
Kaposi’s SarcomaKaposi’s Sarcoma Internal InvolvementInternal Involvement
G.I. Tract is site of internal G.I. Tract is site of internal involvement esp the small involvement esp the small intestine.intestine.
Skeletal changes are diagnosticSkeletal changes are diagnostic Rarefaction, cyst, cortical erosionRarefaction, cyst, cortical erosion
In AIDS: In AIDS: 25% cutaneous alone, 25% cutaneous alone, 29% viscous alone. 29% viscous alone. Ultimately, 70% will have viscous Ultimately, 70% will have viscous
involvement of G.I. (50%), lungs involvement of G.I. (50%), lungs (37%) or Lymph nodes (50%)(37%) or Lymph nodes (50%)
Kaposi’s SarcomaKaposi’s Sarcoma EtiopathogenesisEtiopathogenesis Proliferation of abnormal vascular Proliferation of abnormal vascular
endothelial cells.endothelial cells. Muliticentric originMuliticentric origin HHV-8 is strongly assoc. and predictive of HHV-8 is strongly assoc. and predictive of
K.S. in HIV infected individuals.K.S. in HIV infected individuals. HistologyHistology
Large endothelial cells of capillaries Large endothelial cells of capillaries protrude into lumen like buds. protrude into lumen like buds.
Lesions with proliferation of capillaries and Lesions with proliferation of capillaries and fibrosarcoma like tissue in varying fibrosarcoma like tissue in varying proportions.proportions.
Late lesions: spindle cell proliferation with Late lesions: spindle cell proliferation with sarcoma like properties.sarcoma like properties.
Kaposi’s SarcomaKaposi’s Sarcoma
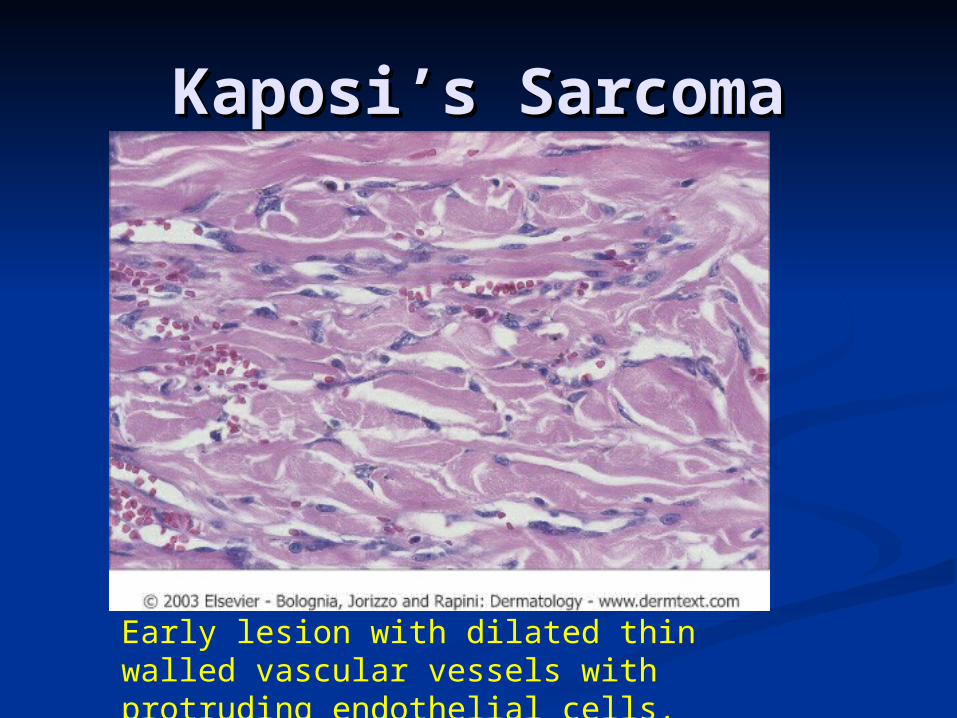
Early lesion with dilated thin walled vascular vessels with protruding endothelial cells.
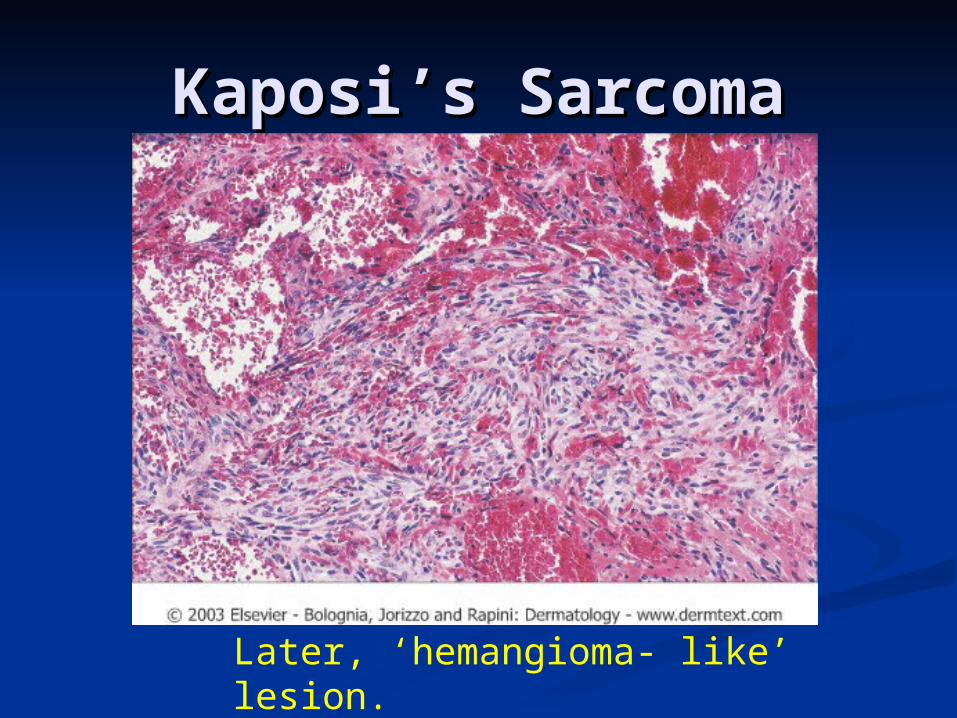
Kaposi’s SarcomaKaposi’s Sarcoma
Later, ‘hemangioma- like’ lesion.
Kaposi’s SarcomaKaposi’s Sarcoma Treatment: Treatment:
Radiation. (all types are responsive) Radiation. (all types are responsive) For individual lesions: cryotherapy, For individual lesions: cryotherapy,
vincristine, excision, laser ablation. vincristine, excision, laser ablation. Alitretinoin applied 2-4 times daily.Alitretinoin applied 2-4 times daily.
Systemic chemotherapy if >10 lesions / Systemic chemotherapy if >10 lesions / month or symptomatic visceral month or symptomatic visceral involvement.involvement.
Resistance to single chemo agents over Resistance to single chemo agents over time so combo with other modalities.time so combo with other modalities.
Course: Usually progresses slowly Course: Usually progresses slowly and is rarely the cause of death. and is rarely the cause of death. (except African cutaneous variety. (except African cutaneous variety.
Epithelioid HemangioendotheliomaEpithelioid Hemangioendothelioma
Solitary, slow growing papule on the Solitary, slow growing papule on the extremities. Intermediate between extremities. Intermediate between angiosarcoma and hemangioma.angiosarcoma and hemangioma.
M>F. Frequently before age of 25 years.M>F. Frequently before age of 25 years. Rare.Rare. Histology: Dilated vascular channels, Histology: Dilated vascular channels,
spindle cells; cords and nests of spindle cells; cords and nests of epithelioid endothelial cells in a myxoid or epithelioid endothelial cells in a myxoid or hyalinized backgroundhyalinized background
30% mets to regional nodes, lung, liver, or 30% mets to regional nodes, lung, liver, or bonebone
TX: Wide excision with evaluation of TX: Wide excision with evaluation of regional nodes. 20-30% 2 year mortality.regional nodes. 20-30% 2 year mortality.
Spindle cell HemangioendotheliomaSpindle cell Hemangioendothelioma AKA spindle cell hemangiomaAKA spindle cell hemangioma Child or young adult with Multifocal Child or young adult with Multifocal
occurance of firm, blue nodules on extremityoccurance of firm, blue nodules on extremity Rare.Rare. May recur when excised. May recur when excised.
Retiform HemangioendotheliomaRetiform Hemangioendothelioma Low grade angiosarcoma. Slow growing Low grade angiosarcoma. Slow growing
exophytic mass sub-Q nodule or even a exophytic mass sub-Q nodule or even a plaque.plaque.
RareRare Extremities of young adultsExtremities of young adults Wide excision. Nodes may be affected locally Wide excision. Nodes may be affected locally
but no deaths reported due to Mets.but no deaths reported due to Mets.
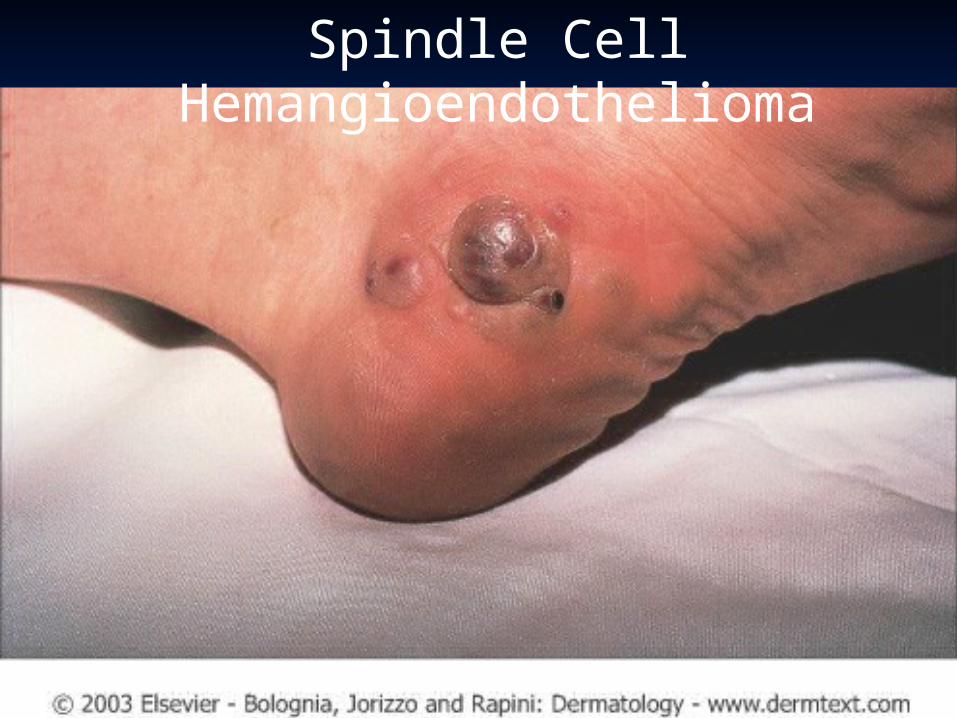
Spindle Cell Hemangioendothelioma
AngiosarcomaAngiosarcoma4 Clinical settings:4 Clinical settings:
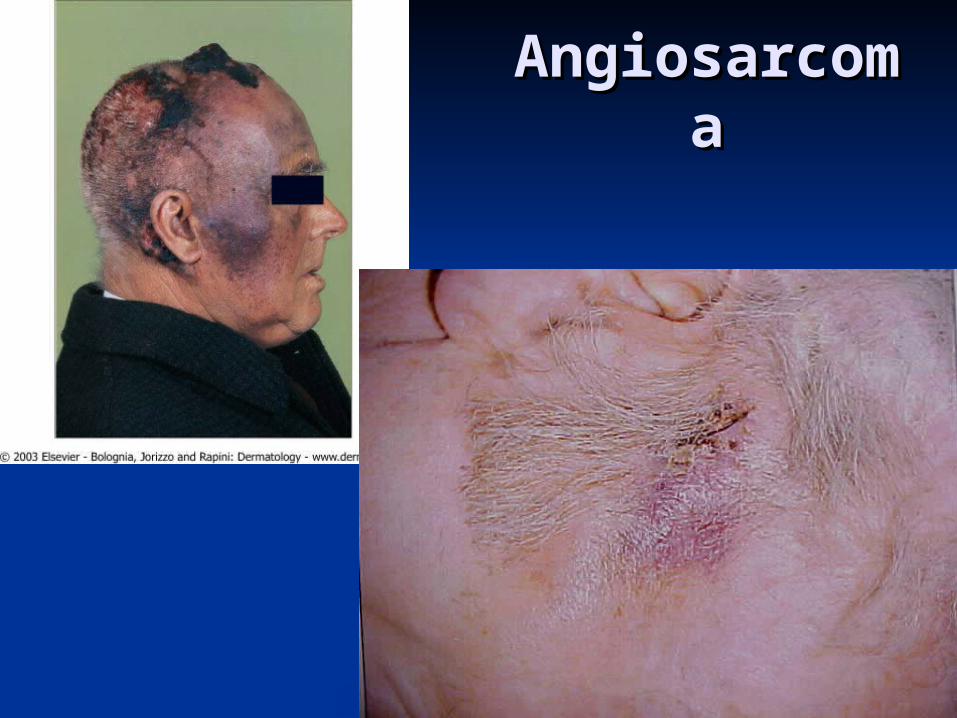
1.) Head and neck tumor of elderly1.) Head and neck tumor of elderly Most common clinical settingMost common clinical setting M:F = ratio 2:1M:F = ratio 2:1 Ill defined bluish nodule Ill defined bluish nodule resembles a bruise resembles a bruise
often with an erythematous ring.often with an erythematous ring. Satellite Satellite nodules, bleeding are common.nodules, bleeding are common.
TX: Complete excision with radiation.TX: Complete excision with radiation. Multicentric nature and rapid metastasis Multicentric nature and rapid metastasis
usually results in death in two years.usually results in death in two years.
2.) In area of chronic lyphedema.2.) In area of chronic lyphedema. Appears 4-27 years following duration of Appears 4-27 years following duration of
lympedemalympedema Classically after mastectomy (Stewart-Treves)Classically after mastectomy (Stewart-Treves) Appears 10 years after surgery in 0.45 % of pts.Appears 10 years after surgery in 0.45 % of pts. Mets to lungs = death in 19-31 months. (6% -5 Mets to lungs = death in 19-31 months. (6% -5
year)year)
AngiosarcomaAngiosarcoma
3.) Previously irradiated sites3.) Previously irradiated sites Interval of tumor development depends Interval of tumor development depends
on nature of lesion for which radiation on nature of lesion for which radiation was given:was given: Benign – 23 years to develop.Benign – 23 years to develop. Malignant – 12 years.Malignant – 12 years.
Prognosis: death in 6-24 months.Prognosis: death in 6-24 months.
4.) Miscellaneous subset.4.) Miscellaneous subset.
AngiosarcoAngiosarcomama
AngiosarcomaAngiosarcoma
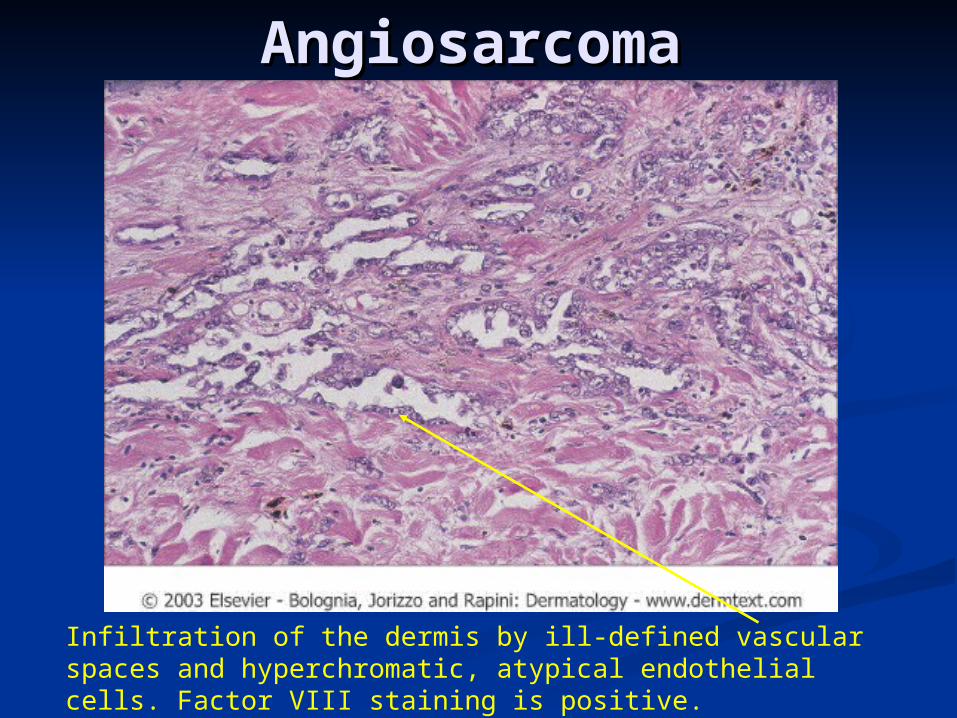
Infiltration of the dermis by ill-defined vascular spaces and hyperchromatic, atypical endothelial cells. Factor VIII staining is positive.
Fibrous Tissue Fibrous Tissue AbnormalitiesAbnormalities
KeloidsKeloids Firm, irregularly shaped, fibrous excrescence Firm, irregularly shaped, fibrous excrescence
usually at a site of previous trauma. Claw-like usually at a site of previous trauma. Claw-like projections overgrow wound boundary.projections overgrow wound boundary.
May occur at any body site. Most common site - May occur at any body site. Most common site - sternal.sternal.
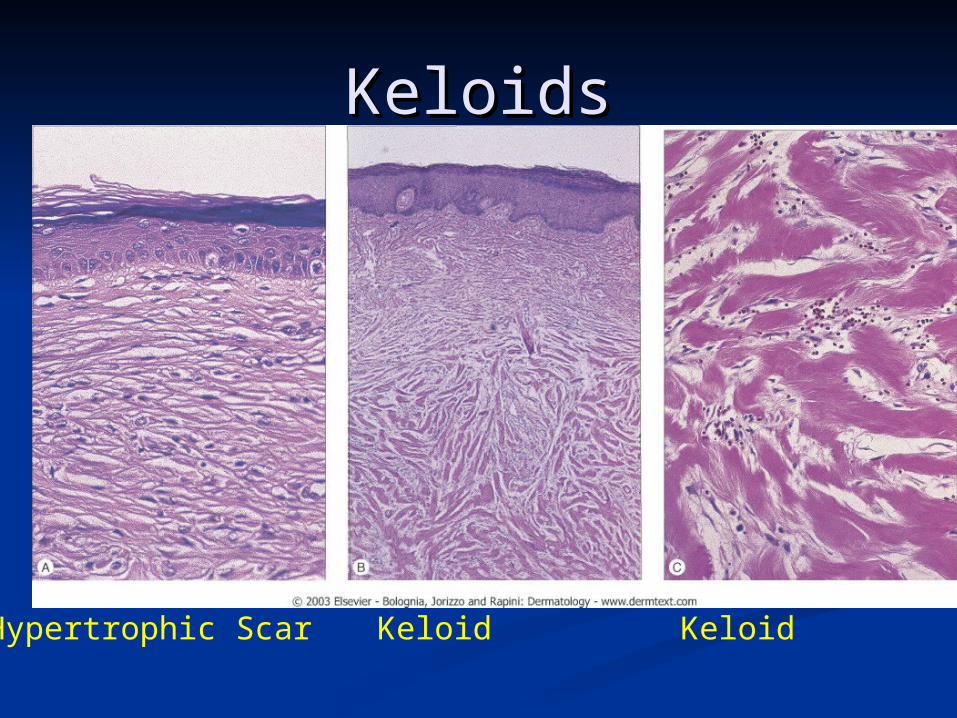
Histopathology: Growth of myofibroblast and Histopathology: Growth of myofibroblast and collagen in the dermis with a whirl like arrangement collagen in the dermis with a whirl like arrangement of hyalinized bundles of collagen. There is a paucity of hyalinized bundles of collagen. There is a paucity of elastic tissue and thinning of the overlying of elastic tissue and thinning of the overlying papillary dermis.papillary dermis.
DDX: Hypertrophic scar- No claw like extensions. DDX: Hypertrophic scar- No claw like extensions. Stays in wound boundaries. Often improves in 6 mo.Stays in wound boundaries. Often improves in 6 mo.
TX: Intralesional kenalog 20-40 mg/cc. Lasers. TX: Intralesional kenalog 20-40 mg/cc. Lasers. Excision with intralesional injections. Silicone Excision with intralesional injections. Silicone sheeting.sheeting.

KeloidsKeloids
Hypertrophic Scar at 5 months and 1 year

Spontaneous KeloidsSpontaneous Keloids
KeloidsKeloids
Hypertrophic Scar Keloid Keloid


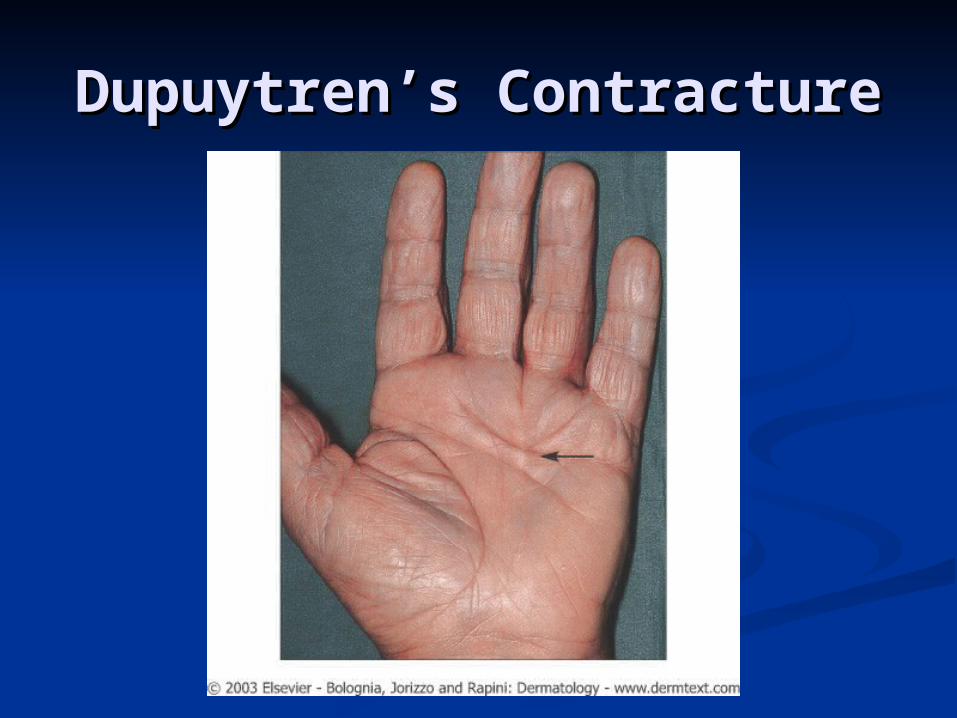
Dupuytren’s ContractureDupuytren’s Contracture Fibromatosis of the palmar Fibromatosis of the palmar
aponeurosis. Plantar Fibromatosis is aponeurosis. Plantar Fibromatosis is seen on soles.seen on soles.
Men 30-50 years. Multiple firm Men 30-50 years. Multiple firm nodules in the palm, 1 cm in diameter, nodules in the palm, 1 cm in diameter, proximal to the 4proximal to the 4thth finger. finger. Contractures develop with time.Contractures develop with time.
Associations: Alcoholic cirrhosis, DM, Associations: Alcoholic cirrhosis, DM, epilepsy, plantar fibromatosis, epilepsy, plantar fibromatosis, Peyronies dx. Familiar predispositions.Peyronies dx. Familiar predispositions.
TX: Early intralesional Triamcinolone, TX: Early intralesional Triamcinolone, Surgery.Surgery.
Dupuytren’s ContractureDupuytren’s Contracture
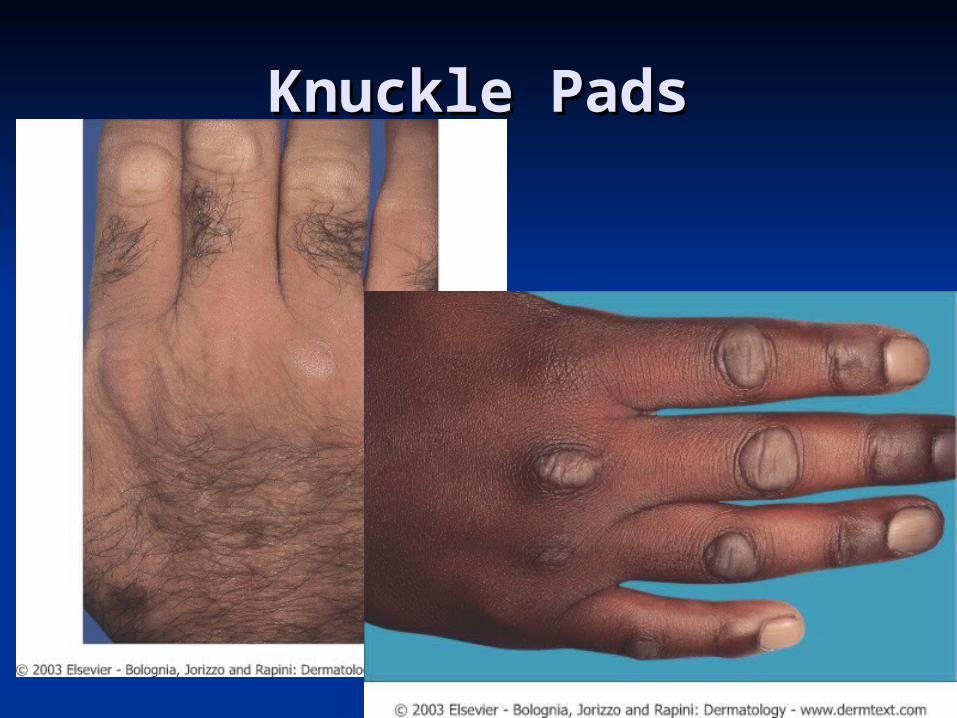
Knuckle PadsKnuckle Pads Well defined, round, plaque-like fibrous Well defined, round, plaque-like fibrous
thickenings that develop over the proximal thickenings that develop over the proximal interphalangeal joints on toes and fingers.interphalangeal joints on toes and fingers.
May become 10-15mm in diameter and May become 10-15mm in diameter and persist permanently. Remain freely persist permanently. Remain freely mobile.mobile.
Assoc with Dupuytren’s contractures and Assoc with Dupuytren’s contractures and some autosomal dominate familial cases some autosomal dominate familial cases have been reported.have been reported.
Histology: FibromasHistology: Fibromas TX: intralesional steroids.TX: intralesional steroids.
Knuckle PadsKnuckle Pads
Peyronie’s DiseasePeyronie’s Disease
Fibrous infiltration of intercavernous Fibrous infiltration of intercavernous septum of the penis results in septum of the penis results in nodules and plaques. A fibrous nodules and plaques. A fibrous chordee is produced with curvature chordee is produced with curvature of on erection.of on erection.
Assoc with Dupuytren’s contractorAssoc with Dupuytren’s contractor TX: Intralesional Triamcinolone may TX: Intralesional Triamcinolone may
be curative.be curative.
Peyronie’s DiseasePeyronie’s Disease
As Dr. Ladd would say: ‘Something just ain’t right…..’
Desmoid TumorDesmoid Tumor
Deep seated well circumscribed mass Deep seated well circumscribed mass arising from muscular aponeurosis. arising from muscular aponeurosis.
Most common on abdominal wall esp. in Most common on abdominal wall esp. in women during or after pregnancy.women during or after pregnancy.
May be fatal if invade or compress vital May be fatal if invade or compress vital structures. Most dangerous are those of structures. Most dangerous are those of neck and intra-abdominalneck and intra-abdominal
TX: MRI to evaluate extent of tumor. TX: MRI to evaluate extent of tumor. Excision. Radiotherapy and hormonal Excision. Radiotherapy and hormonal manipulation are other optionsmanipulation are other options

Desmoid TumorDesmoid Tumor 5 subtypes5 subtypes
Abdominal wallAbdominal wall ExtrabdominalExtrabdominal IntrabdominalIntrabdominal MultipleMultiple Gardner’s Gardner’s
syndromesyndrome
Aponeourotic FibromaAponeourotic Fibroma Juvenile aponeurotic fibroma.Juvenile aponeurotic fibroma. Slow growing cyst-like masses Slow growing cyst-like masses
occurring on the limbs. occurring on the limbs. X-ray reveals Stippled calcification.X-ray reveals Stippled calcification.
Congenital Generalized Congenital Generalized FibromatosisFibromatosis Multiple firm dermal and subdermal Multiple firm dermal and subdermal
nodules presenting at near birth.nodules presenting at near birth. 2 types of involvement:2 types of involvement:
Dermal and Skeletal (metaphyseal) – resolution 2 Dermal and Skeletal (metaphyseal) – resolution 2 yrs.yrs.
Involvement of viscera - 80% mortality. If live past Involvement of viscera - 80% mortality. If live past 4 mo. then regression.4 mo. then regression.

Juvenile aponeurotic Juvenile aponeurotic fibromafibroma
Aponeourotic FibromaAponeourotic Fibroma Juvenile aponeurotic fibroma.Juvenile aponeurotic fibroma. Slow growing cyst-like masses occurring Slow growing cyst-like masses occurring
on the limbs. on the limbs. X-ray reveals Stippled calcification.X-ray reveals Stippled calcification.
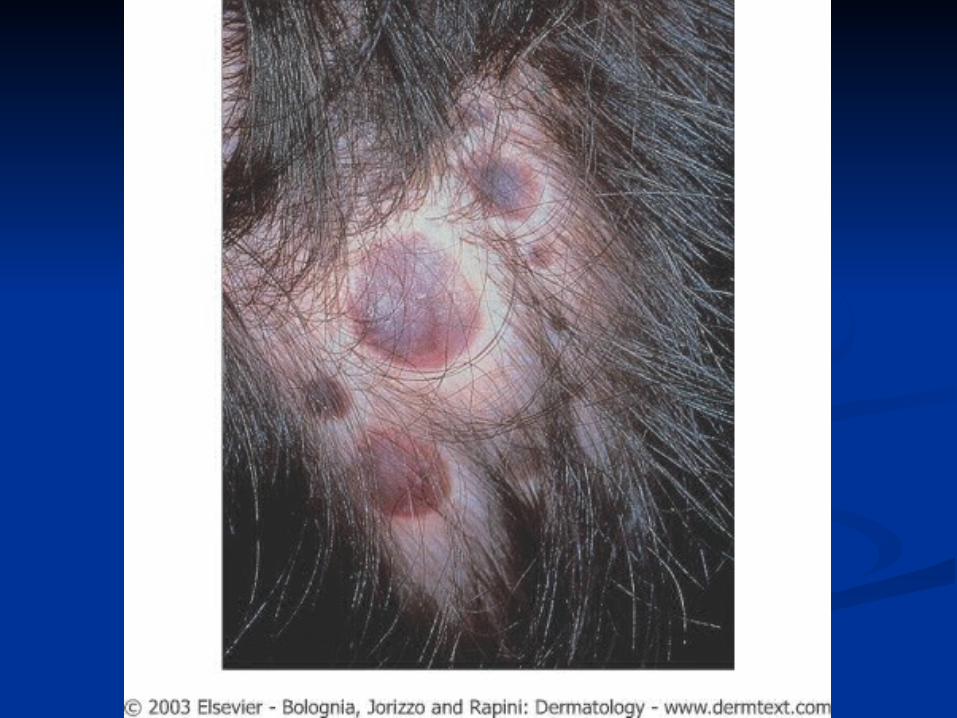
Congenital Generalized Congenital Generalized FibromatosisFibromatosis Infantile myofibromatosisInfantile myofibromatosis Multiple firm dermal and subdermal Multiple firm dermal and subdermal
nodules presenting at near birth.nodules presenting at near birth. 2 types of involvement:2 types of involvement:
Dermal and Skeletal (metaphyseal) – resolution 2 yrs.Dermal and Skeletal (metaphyseal) – resolution 2 yrs. Involvement of viscera - 80% mortality. If live past 4 Involvement of viscera - 80% mortality. If live past 4
mo. then regression.mo. then regression.
Asymptomatic, firm, red, 1 cm. Asymptomatic, firm, red, 1 cm. diameter nodules on DIP of fingers diameter nodules on DIP of fingers or toes during the first year of life. or toes during the first year of life. No metastasis.No metastasis.
Whorled fascicles of spindle cells Whorled fascicles of spindle cells eosinophilic inclusion bodieseosinophilic inclusion bodies
Surgical excision has high Surgical excision has high recurrence.recurrence.
TX: Observation, hope for TX: Observation, hope for spontaneous resolution.spontaneous resolution.
Infantile Digital Fibromatosis

Infantile Digital Infantile Digital FibromatosisFibromatosis
Whorled fascicles of spindle cells Eosinophilic inclusion bodies
Fibrous Harmartoma of infancyFibrous Harmartoma of infancy Single dermal or sub-q nodule of upper Single dermal or sub-q nodule of upper
trunk present at birth.trunk present at birth. Excision.Excision.
Fibomatosis ColliFibomatosis Colli Fibrous proliferation infiltration Fibrous proliferation infiltration
sternocleidomastoid m. at birth.sternocleidomastoid m. at birth. Spontaneous remission in a few months.Spontaneous remission in a few months.
Diffuse Infantile FibromatosisDiffuse Infantile Fibromatosis Multicentric fibrous infiltration of m. of Multicentric fibrous infiltration of m. of
arms, neck and shoulder area.arms, neck and shoulder area.
Giant Cell Tumor of Tendon Giant Cell Tumor of Tendon SheathSheath
Firm 1-3 cm. nodule attaches to Firm 1-3 cm. nodule attaches to tendons of fingers hand and wrist tendons of fingers hand and wrist (esp flexor).(esp flexor).
Histopathology:Histopathology: Lobules of densely hyalinized collagen. Lobules of densely hyalinized collagen.
Giant cells with eosinophilic cytoplasm Giant cells with eosinophilic cytoplasm and variable nuclei.and variable nuclei.
TX TX Excision. Recurs in 25%. Excision. Recurs in 25%.
Giant Cell Tumor of Tendon Giant Cell Tumor of Tendon SheathSheath
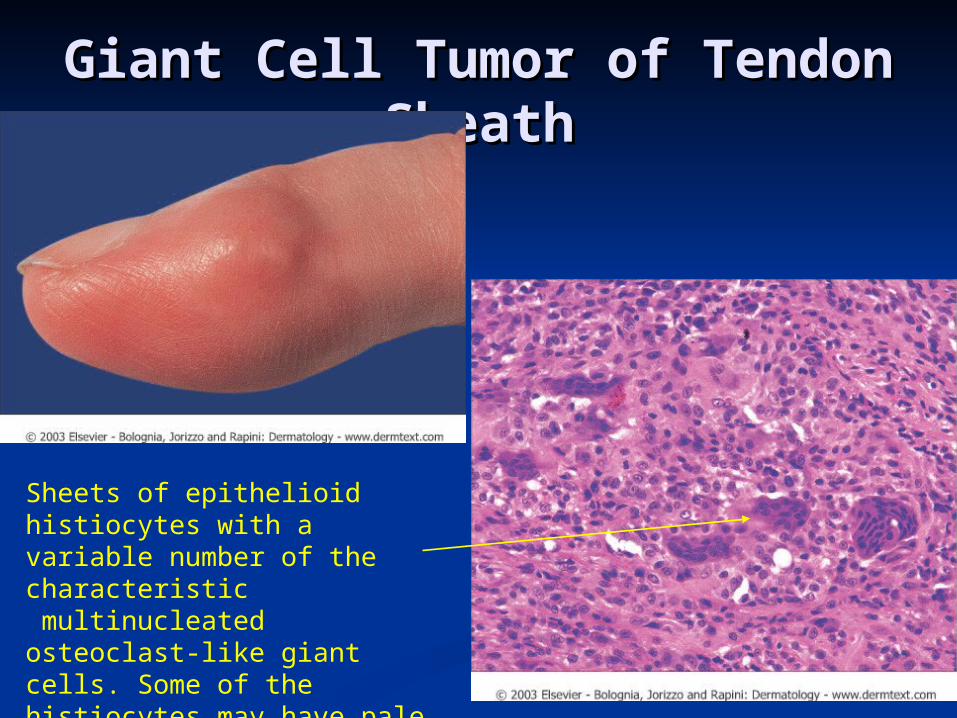
Sheets of epithelioid histiocytes with a variable number of the characteristic multinucleated osteoclast-like giant cells. Some of the histiocytes may have
pale foamy cytoplasm.
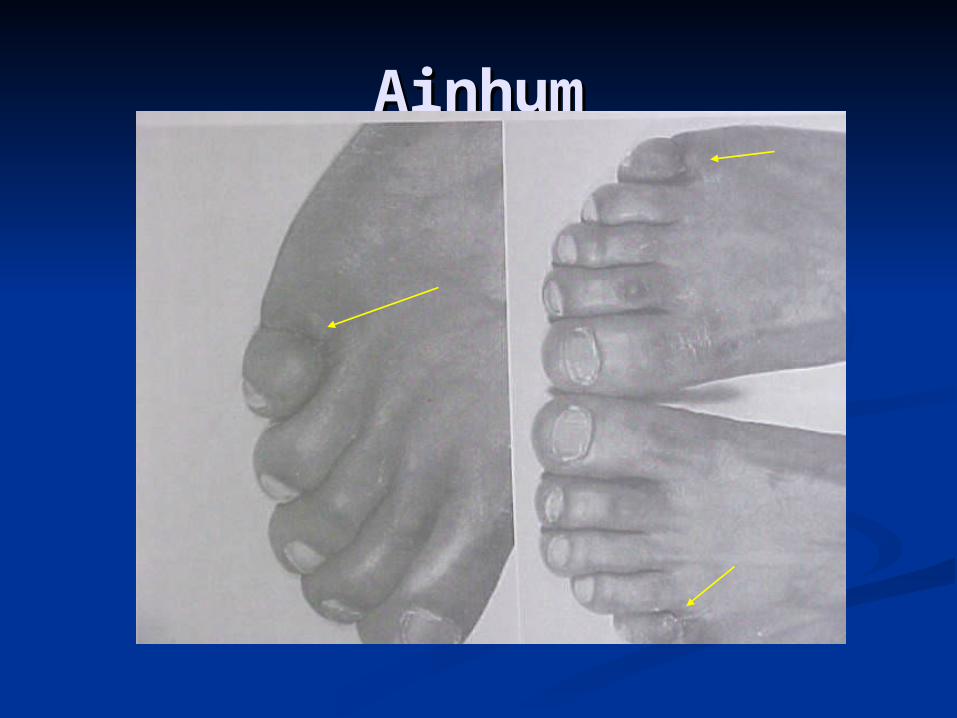
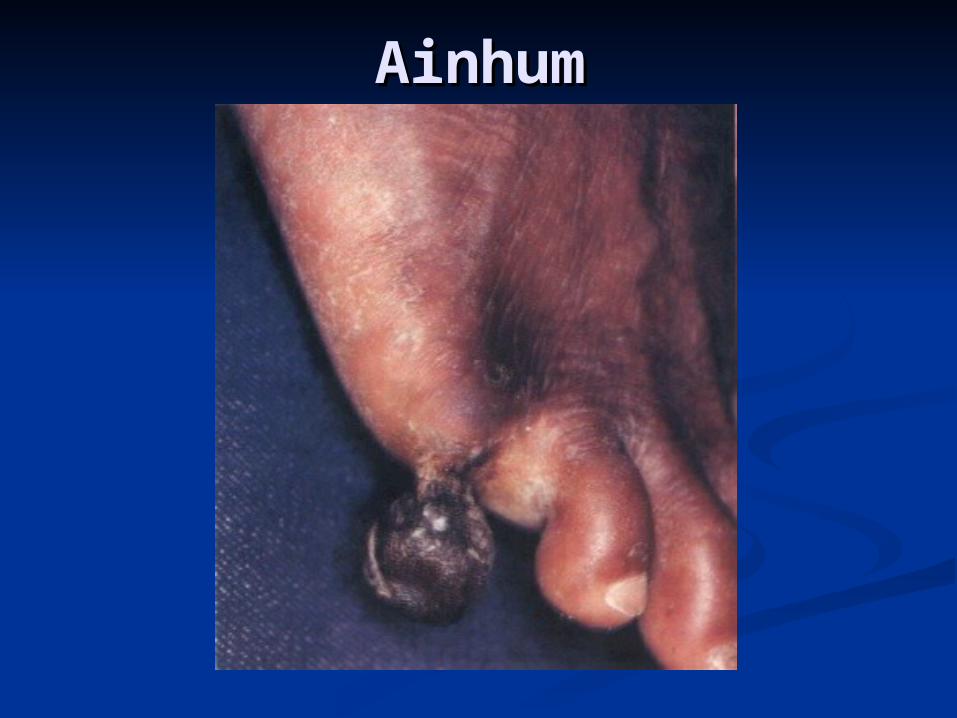
AinhumAinhum Linear constriction occurs around the Linear constriction occurs around the
toes (esp 5toes (esp 5thth at PIP) eventually at PIP) eventually resulting spontaneous amputation in resulting spontaneous amputation in 5-10 years. Begins as grove on flexor 5-10 years. Begins as grove on flexor surface and joins over time. surface and joins over time.
African Men.African Men. Etiology: Unknown. (Trauma?)Etiology: Unknown. (Trauma?) TX: Surgery sometimes helpful. TX: Surgery sometimes helpful.
Intralesional steroids.Intralesional steroids. Pseudo-Ainhum: Hereditary and Pseudo-Ainhum: Hereditary and
nonhereditary diseases associated nonhereditary diseases associated with annular constriction.with annular constriction.
AinhumAinhum
AinhumAinhum
Connective Tissue NeviConnective Tissue Nevi
Multiple or solitary plaques 1-15 cm in Multiple or solitary plaques 1-15 cm in diameter, yellow to light orange with a diameter, yellow to light orange with a shagreen leather like surface texture.shagreen leather like surface texture. Predilection for lumbosacral area. Predilection for lumbosacral area.
Acquired type: eruptive collagenoma, Acquired type: eruptive collagenoma, isolated collagenoma and isolated elastomaisolated collagenoma and isolated elastoma
Congenital Types:Congenital Types: 1.) Buschke – Ollendorf: AD. Widespread 1.) Buschke – Ollendorf: AD. Widespread
asymmetrically distributed plaques. asymmetrically distributed plaques. Osteopoikilosis of long bones is diagnostic.Osteopoikilosis of long bones is diagnostic.
Connective Tissue NeviConnective Tissue Nevi
(Continued)(Continued) 2.) Familial cutaneous collagenomas: 2.) Familial cutaneous collagenomas:
Numerous symmetrical asymptomatic nodules Numerous symmetrical asymptomatic nodules on back. Onset in teens. MEN-I assoc.on back. Onset in teens. MEN-I assoc.
In tuberous sclerosis, connective tissue In tuberous sclerosis, connective tissue nevi are shagreen patches. nevi are shagreen patches. ½ of T.S. cases are new mutations so any pt ½ of T.S. cases are new mutations so any pt
with connective tissue nevi should be with connective tissue nevi should be evaluated for tuberous sclerosis.evaluated for tuberous sclerosis.

Connective Tissue NeviConnective Tissue Nevi
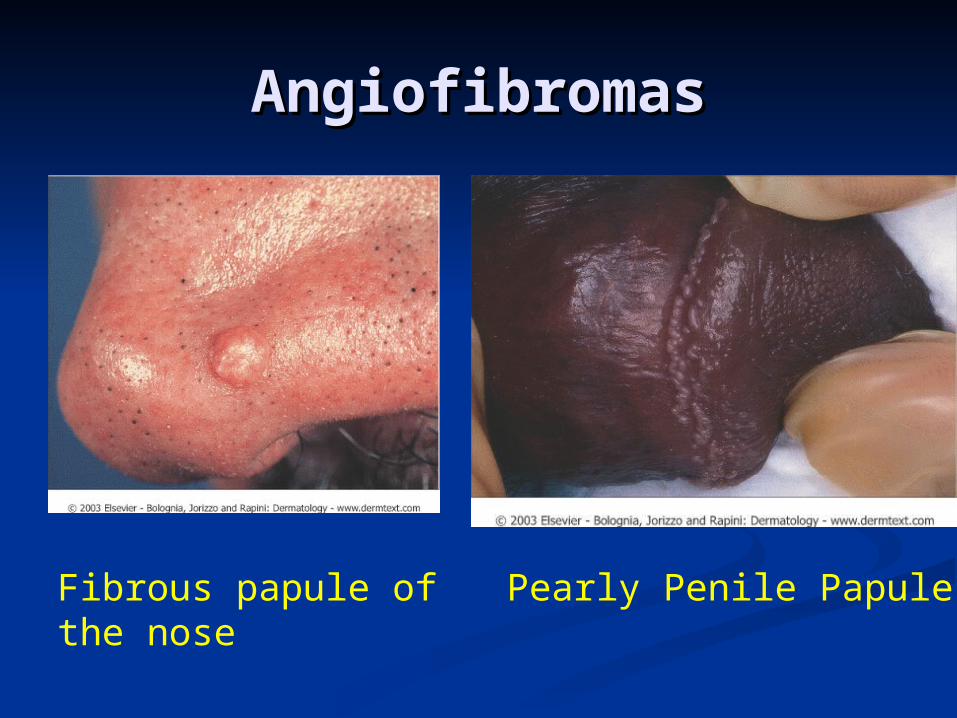
AngiofibromasAngiofibromasFibrous and vascular proliferation of Fibrous and vascular proliferation of
upper dermisupper dermisCommon types:Common types:
1.1. Fibrous papule of the nose – Fibrous papule of the nose – 3-6 mm 3-6 mm diameter, dome shaped sessile papule diameter, dome shaped sessile papule with white to reddish color. Usually with white to reddish color. Usually solitary.solitary.
2.2. Pearly Penile Papule – Pearly Penile Papule – Pearly white Pearly white papules appearing on the coronal margin papules appearing on the coronal margin and sometimes on penile shaft. No TX and sometimes on penile shaft. No TX requiredrequired
3.3. Multiple hereditary forms -Multiple hereditary forms - adenoma adenoma sebaceum (Tuberous Sclerosis) and in sebaceum (Tuberous Sclerosis) and in MEN-I MEN-I
AngiofibromasAngiofibromas
Fibrous papule of the nose
Pearly Penile Papule
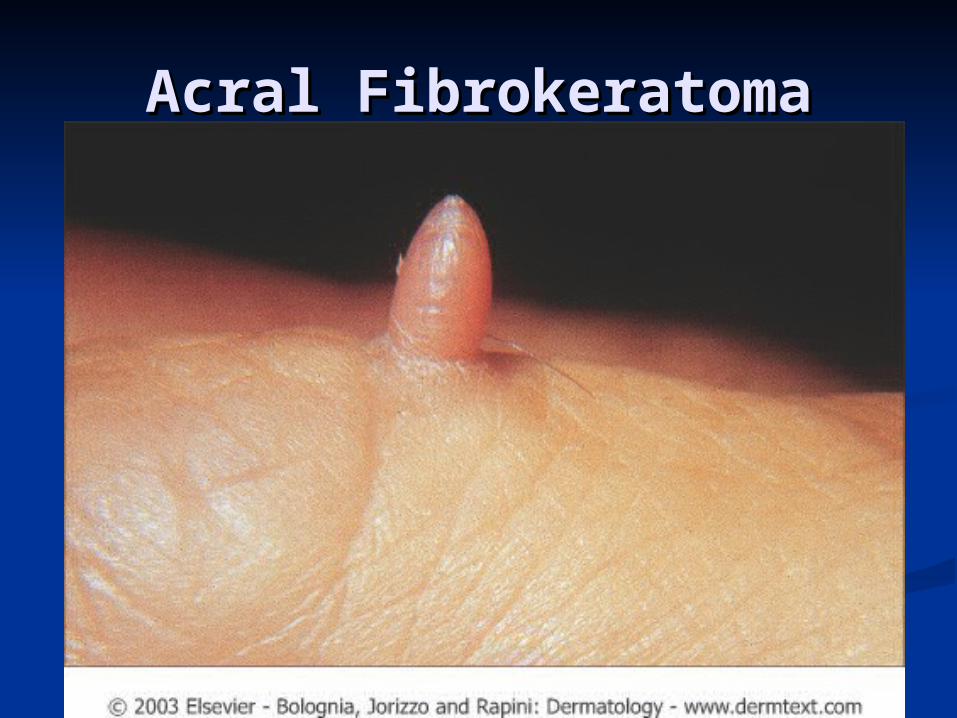
Acral FibrokeratomaAcral Fibrokeratoma
Pink, hyperkeratotic, hornlike Pink, hyperkeratotic, hornlike projection on fingers (most projection on fingers (most common) toes or palms. Emerges common) toes or palms. Emerges from a collarette of scale. from a collarette of scale.
Average age 40. Average age 40. TX: excision. Laser ablation.TX: excision. Laser ablation.
Acral FibrokeratomaAcral Fibrokeratoma
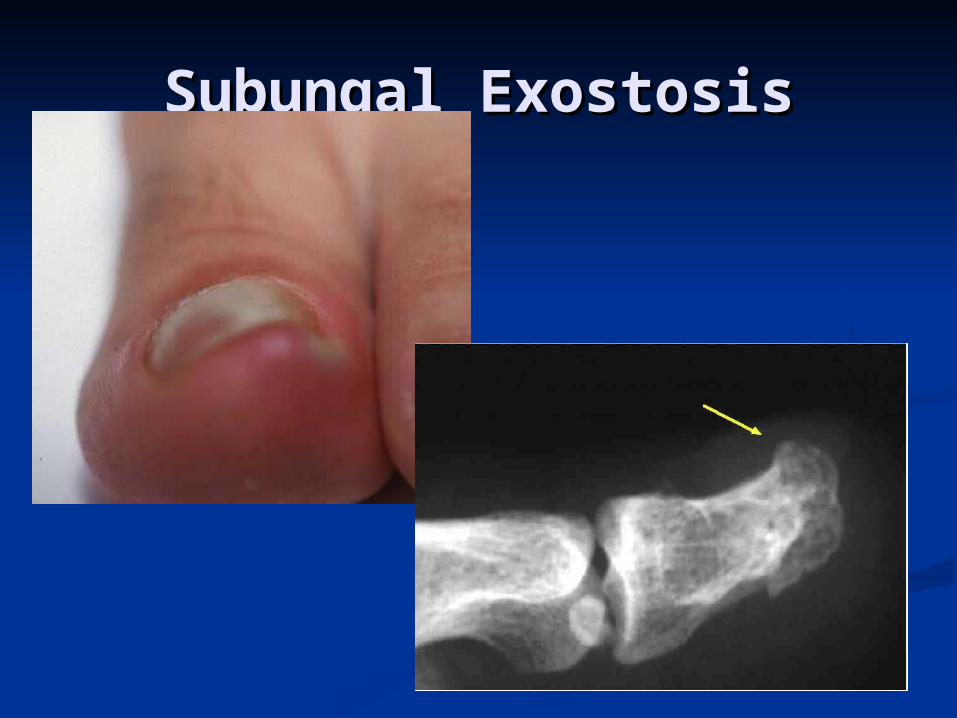
Subungal ExostosisSubungal Exostosis
Solitary, fibrous and bony nodule Solitary, fibrous and bony nodule protruding from the distal edge of the protruding from the distal edge of the nail, most commonly of the great toe.nail, most commonly of the great toe. Begins as a pink papule which destroys Begins as a pink papule which destroys
overlying nail and grows to a maximum overlying nail and grows to a maximum diameter of 8 mm. diameter of 8 mm.
Pressure causes great pain.Pressure causes great pain. X-ray is diagnosticX-ray is diagnostic TX: excision and curettage.TX: excision and curettage.
Subungal ExostosisSubungal Exostosis
Chondrodermatits Chondrodermatits Nodularis Chronica Nodularis Chronica
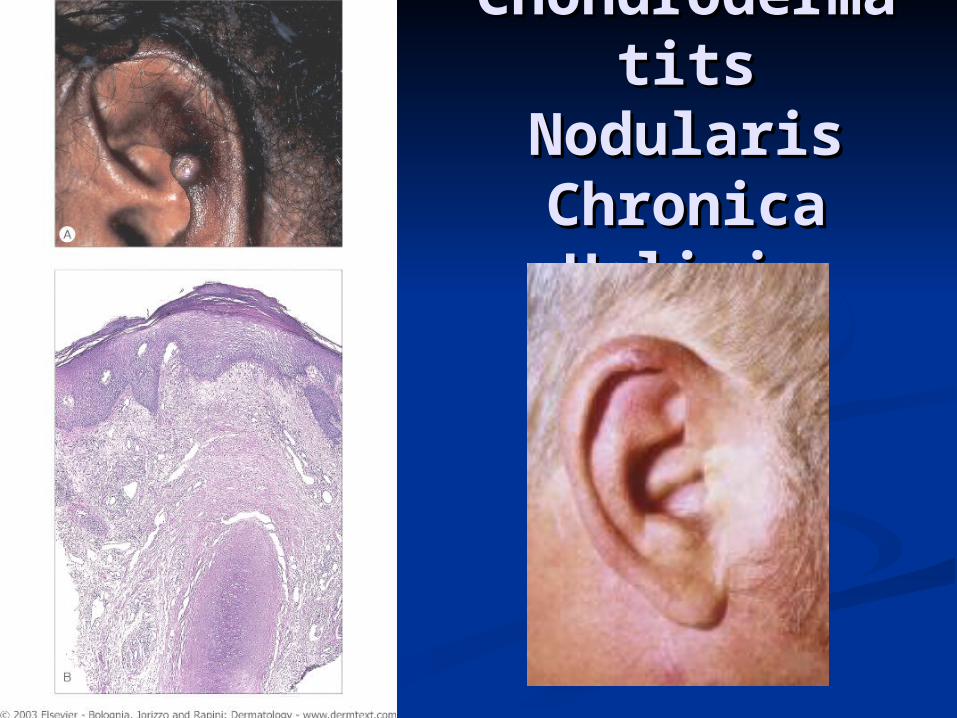
HelicisHelicis Small, tender, inflammatory nodule with gently Small, tender, inflammatory nodule with gently
sloping sides located on the outer helix. sloping sides located on the outer helix. Common in older men. No malignant potential. Common in older men. No malignant potential.
Often hx of chronic trauma. Lesions are very Often hx of chronic trauma. Lesions are very painful. Pt often complains of pain when sleeps painful. Pt often complains of pain when sleeps on lesion.on lesion.
Histology: Degeneration of collagen with Histology: Degeneration of collagen with acanthosis and hyperkeratosis and thinning of acanthosis and hyperkeratosis and thinning of epidermis. epidermis.
TX: Excision. Often a spicule of cartilage is TX: Excision. Often a spicule of cartilage is discovered. (Transdermal elimination).discovered. (Transdermal elimination).
ChondroderChondrodermatits matits
Nodularis Nodularis Chronica Chronica HelicisHelicis
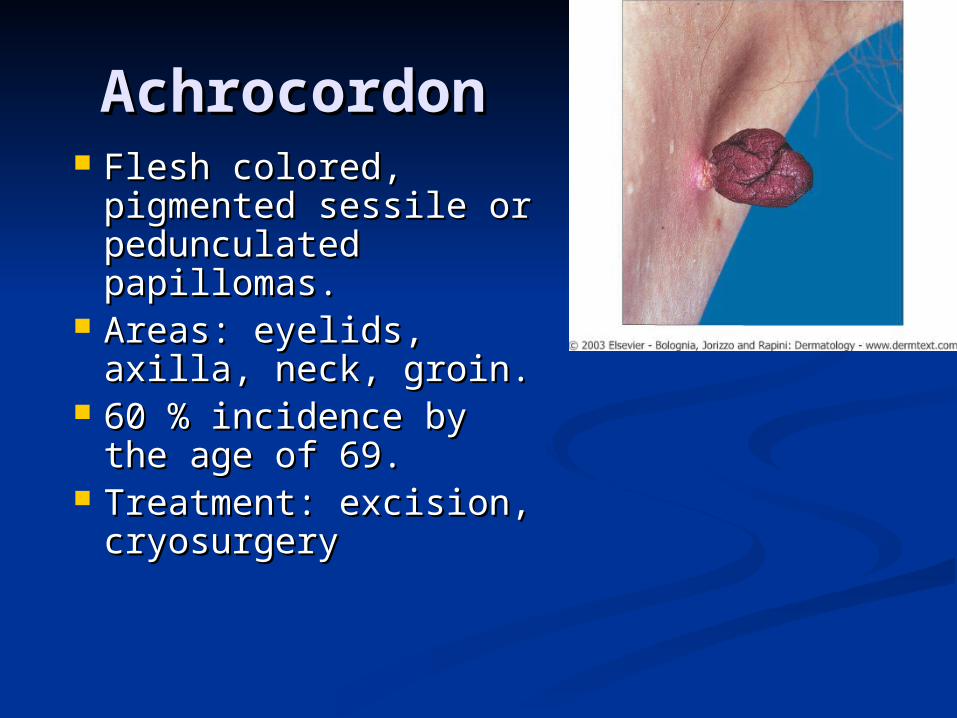
AchrocordonAchrocordon Flesh colored, Flesh colored,
pigmented sessile or pigmented sessile or pedunculated pedunculated papillomas. papillomas.
Areas: eyelids, Areas: eyelids, axilla, neck, groin.axilla, neck, groin.
60 % incidence by 60 % incidence by the age of 69.the age of 69.
Treatment: excision, Treatment: excision, cryosurgerycryosurgery
DermatofibromaDermatofibroma Lesion which grows slowly to a firm, 4-20 mm Lesion which grows slowly to a firm, 4-20 mm
diameter papule or nodule, yellow or reddish diameter papule or nodule, yellow or reddish brown in color and then stops expanding. brown in color and then stops expanding. Sharply demarcated. Chiefly located on lower Sharply demarcated. Chiefly located on lower extremities.extremities.
‘‘Dimple sign’. Seldom seen in children. May Dimple sign’. Seldom seen in children. May grow to 5 cm in size.grow to 5 cm in size.
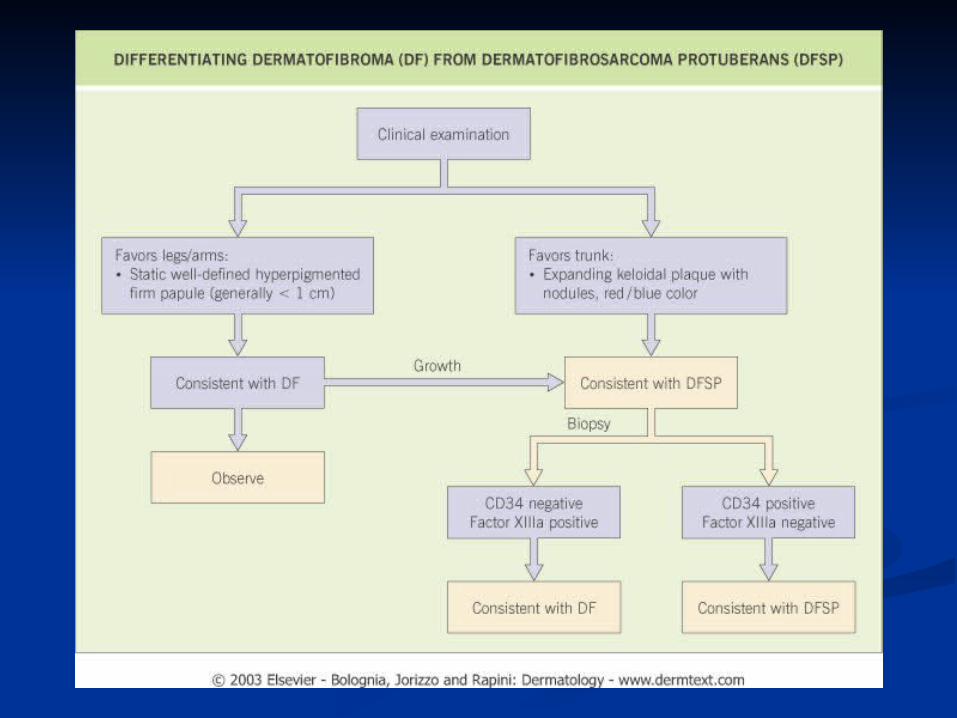
Etiology: Trauma, bites ?Etiology: Trauma, bites ? CD34 neg; Factor XIII pos; Stromolysin posCD34 neg; Factor XIII pos; Stromolysin pos Histology: Dermal mass or whorled fibrous Histology: Dermal mass or whorled fibrous
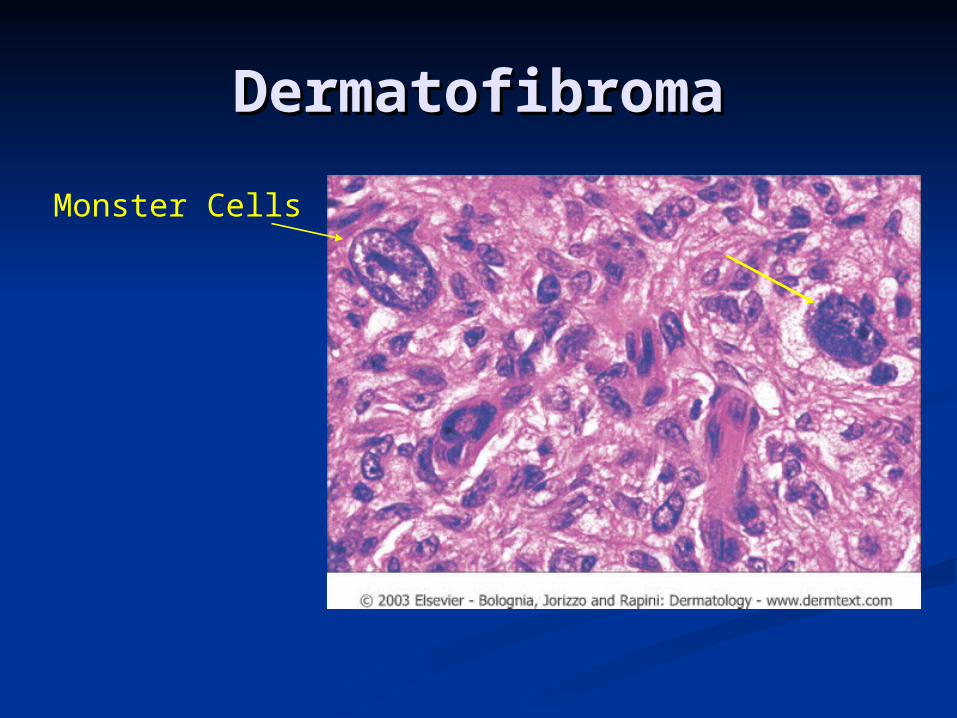
tissue. Numerous cells with large nuclei and tissue. Numerous cells with large nuclei and spindle cells. Some very atypical cells referred spindle cells. Some very atypical cells referred to as ‘Monster cells’. Respects subQ fatto as ‘Monster cells’. Respects subQ fat
TX: Reassurance. Progressive enlargement TX: Reassurance. Progressive enlargement warrants excision.warrants excision.

DermatofibrDermatofibromaoma
DermatofibrDermatofibromaoma
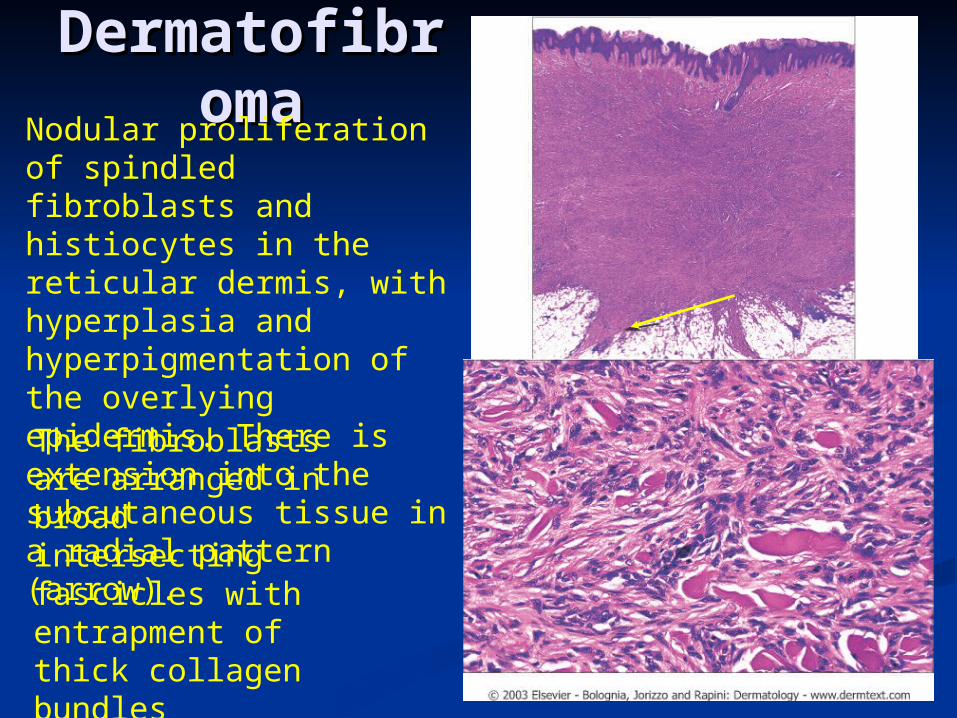
Nodular proliferation of spindled fibroblasts and histiocytes in the reticular dermis, with hyperplasia and hyperpigmentation of the overlying epidermis. There is extension into the subcutaneous tissue in a radial pattern (arrow).
The fibroblasts are arranged in broad intersecting fascicles with entrapment of thick collagen bundles
DermatofibromaDermatofibroma
Monster Cells
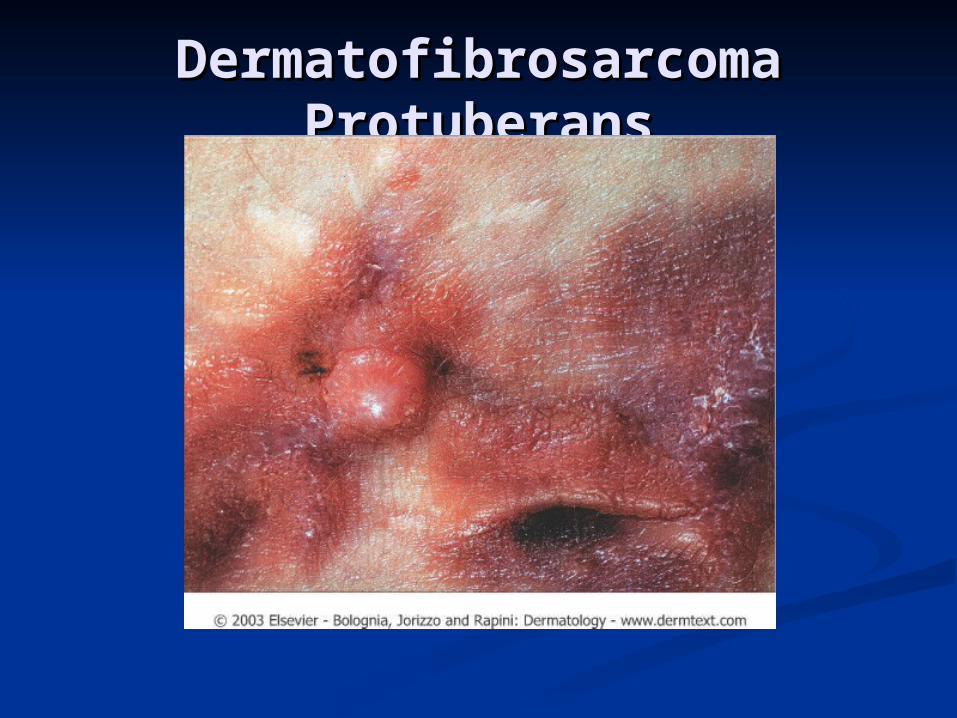
Dermatofibrosarcoma Dermatofibrosarcoma ProtuberansProtuberans On a middle aged PT, a slowly enlarging, On a middle aged PT, a slowly enlarging,
erythematous, firm nodule or plaque erythematous, firm nodule or plaque often with purulence appears on the often with purulence appears on the trunk (60%). Pain is more prominent trunk (60%). Pain is more prominent with as lesion grows and may be severe. with as lesion grows and may be severe. Early lesions resemble keloids or large DF.Early lesions resemble keloids or large DF.
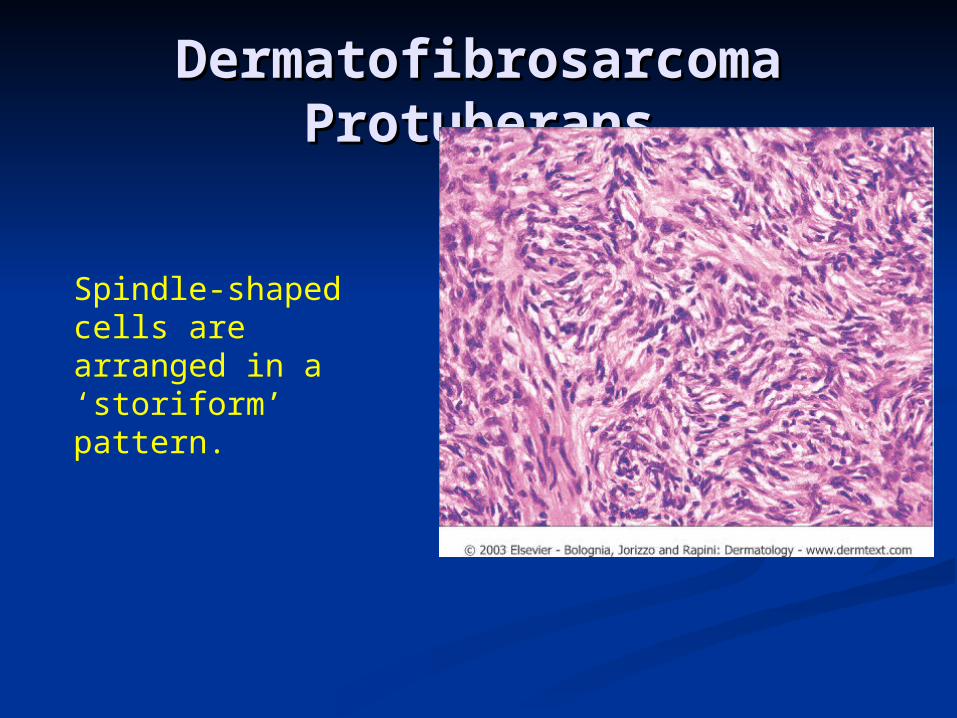
Histology: Subepidermal fibrotic plaque Histology: Subepidermal fibrotic plaque with uniform spindle cells. Cartwheel with uniform spindle cells. Cartwheel pattern of spindle cells surrounding pattern of spindle cells surrounding collagen. Pigment cells = Bednar tumor collagen. Pigment cells = Bednar tumor in dark skinned individuals. CD 34 in dark skinned individuals. CD 34 positive. positive.
TX: Mohs (2% recurrence) or wide TX: Mohs (2% recurrence) or wide excision (11-50%) recurrence.excision (11-50%) recurrence.
Dermatofibrosarcoma Dermatofibrosarcoma ProtuberansProtuberans
Dermatofibrosarcoma Dermatofibrosarcoma ProtuberansProtuberans
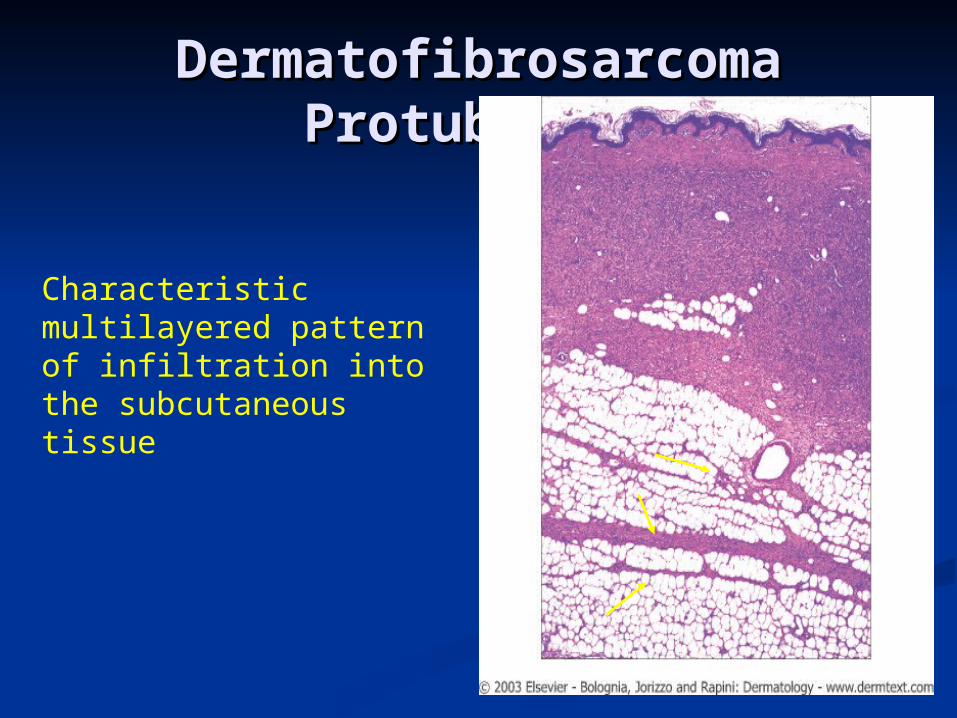
Characteristic multilayered pattern of infiltration into the subcutaneous tissue
Dermatofibrosarcoma Dermatofibrosarcoma ProtuberansProtuberans
Spindle-shaped cells are arranged in a ‘storiform’ pattern.
Nodular FasciitisNodular Fasciitis Deep, firm, solitary, sometimes tender nodule of Deep, firm, solitary, sometimes tender nodule of
deep fascia that rapidly grows to 1-4 cm in deep fascia that rapidly grows to 1-4 cm in diameter over several weeks. Pt is otherwise diameter over several weeks. Pt is otherwise healthy and average age is 40 years.healthy and average age is 40 years.
Variants: Dermal, intravascular and proliferating.Variants: Dermal, intravascular and proliferating.
Histology: myxoid, fibroblastic and capillary Histology: myxoid, fibroblastic and capillary proliferation. Lymphocytic-histiocytic infiltration.proliferation. Lymphocytic-histiocytic infiltration.
TX: complete excision. Intralesional steroids.TX: complete excision. Intralesional steroids.
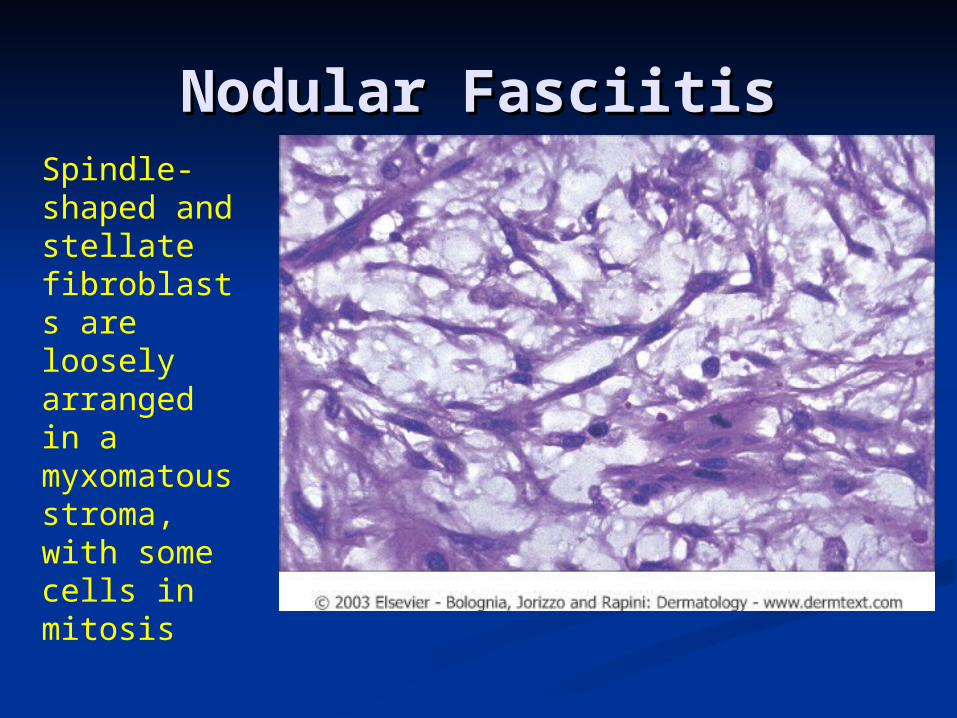
Nodular FasciitisNodular FasciitisSpindle-shaped and stellate fibroblasts are loosely arranged in a myxomatous stroma, with some cells in mitosis
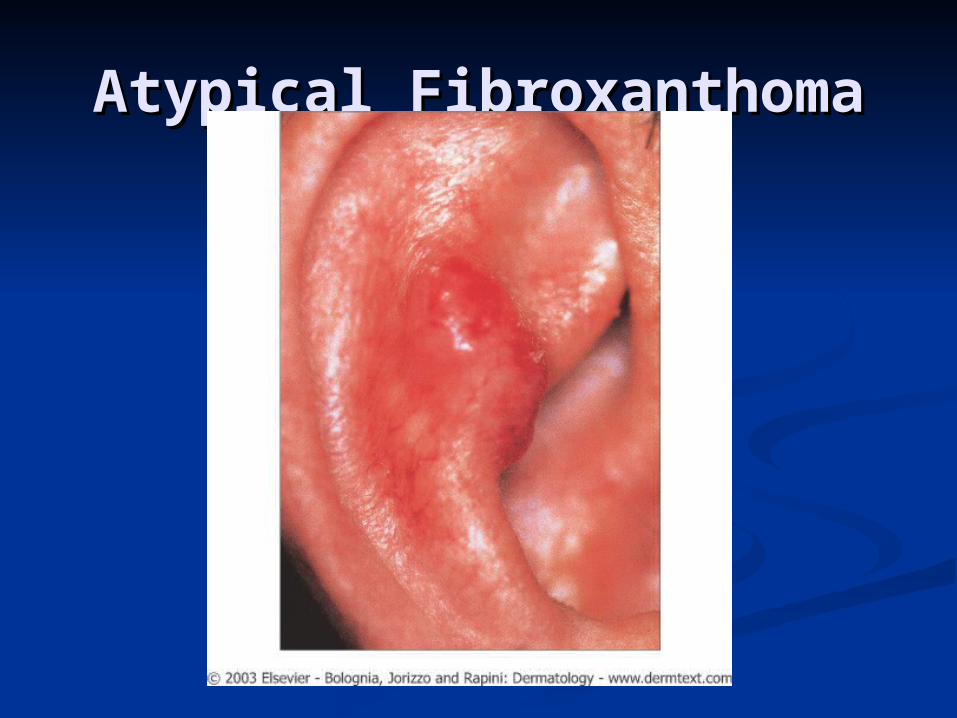
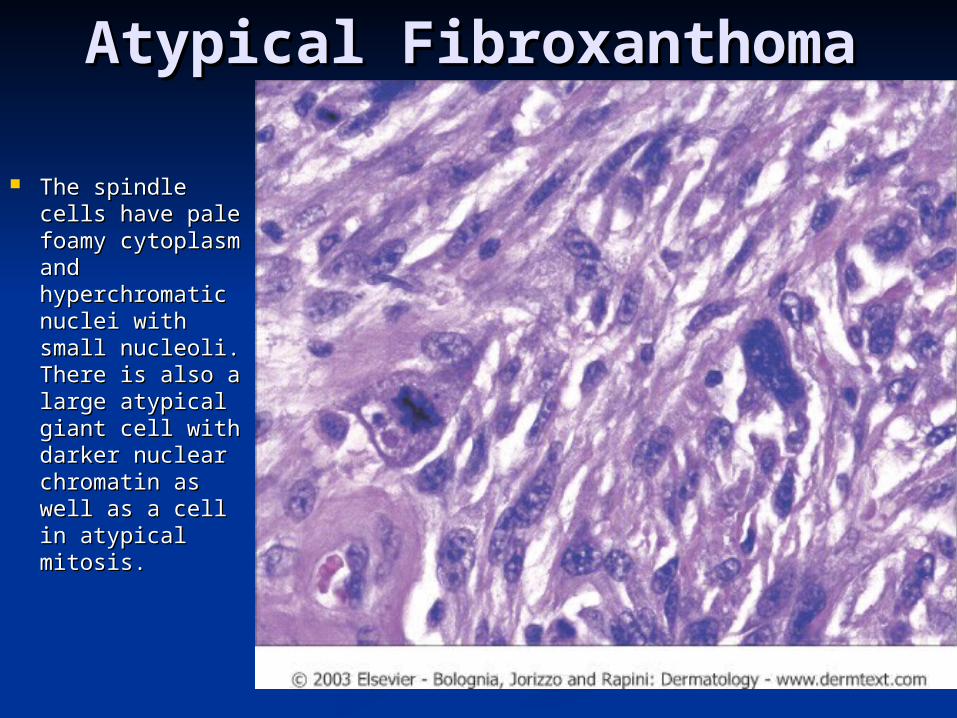
Atypical FibroxanthomaAtypical Fibroxanthoma Small, firm nodule often with eroded surface.Small, firm nodule often with eroded surface.
Usually occurs on sun exposed locations on the Usually occurs on sun exposed locations on the head and neck, Caucasians >50 yrs. old. head and neck, Caucasians >50 yrs. old. A subset occurs in 25% of patients where the tumor is located on A subset occurs in 25% of patients where the tumor is located on
covered area in person approx 40 yrs old.covered area in person approx 40 yrs old.
Histology: Bizarre spindle cells (vesicular Histology: Bizarre spindle cells (vesicular nucleus) and atypical histiocytes with mitotic nucleus) and atypical histiocytes with mitotic cells, eosinophilic nuclei and biphasic cell cells, eosinophilic nuclei and biphasic cell population.population.
TX: Surgical excision. Recurrence is frequent TX: Surgical excision. Recurrence is frequent and MOHS offers best cure rate. Possible and MOHS offers best cure rate. Possible metastasis in rare cases.metastasis in rare cases.
Atypical FibroxanthomaAtypical Fibroxanthoma
Atypical FibroxanthomaAtypical Fibroxanthoma
The spindle The spindle cells have pale cells have pale foamy foamy cytoplasm and cytoplasm and hyperchromatic hyperchromatic nuclei with nuclei with small nucleoli. small nucleoli. There is also a There is also a large atypical large atypical giant cell with giant cell with darker nuclear darker nuclear chromatin as chromatin as well as a cell in well as a cell in atypical atypical mitosis. mitosis.
Malignant Fibrous Malignant Fibrous HistiocytomaHistiocytoma
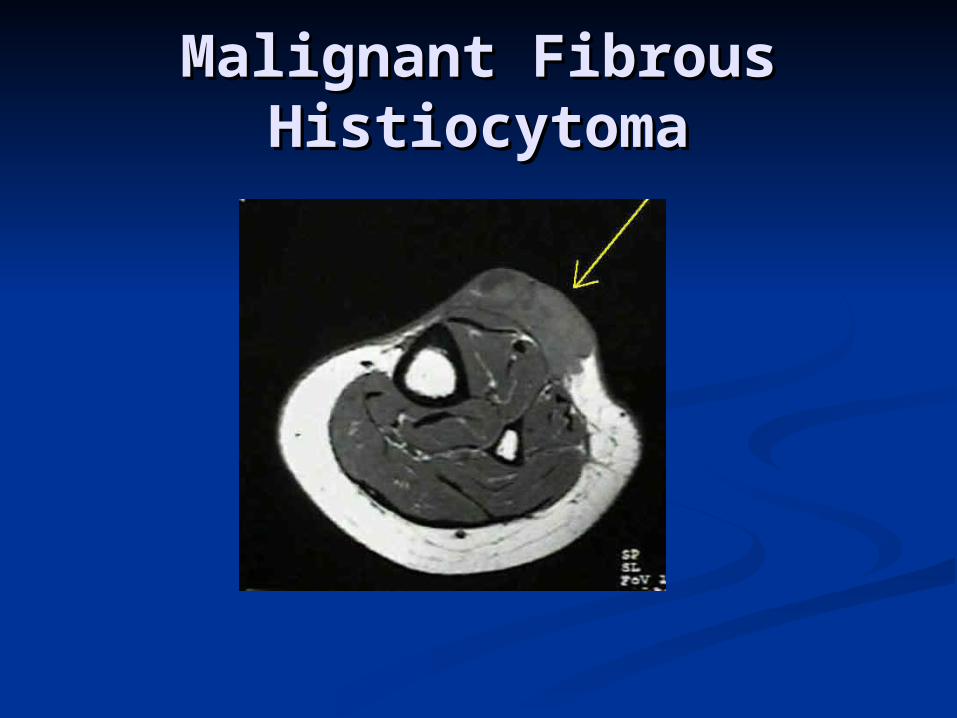
Most common soft tissue sarcoma of middle Most common soft tissue sarcoma of middle age and late adulthood. Resembles DFSP.age and late adulthood. Resembles DFSP.
Progressively enlarging, 1-3 cm diameter, Progressively enlarging, 1-3 cm diameter, protruding, tumor with a reddish or duskyprotruding, tumor with a reddish or dusky 1/3 on thigh or buttocks. Peak incidence in 71/3 on thigh or buttocks. Peak incidence in 7thth
decade.decade. Association with radiodermatitis and chronic ulcers.Association with radiodermatitis and chronic ulcers.
Histology: Polygonal and spindle cells with Histology: Polygonal and spindle cells with large bizarre multinucleated types. large bizarre multinucleated types. Pleomorphic cellular elements and bizarre Pleomorphic cellular elements and bizarre mitotic figures.mitotic figures.
TX: Excision. Recurrence in 25 % of cases. TX: Excision. Recurrence in 25 % of cases. Metastasis in 35%. Overall survival of 50%Metastasis in 35%. Overall survival of 50%
Prognosis: Prognosis: Deeper and proximal = poorer prognosis. Deeper and proximal = poorer prognosis. Assoc with radiodermatitis = esp poor prognosisAssoc with radiodermatitis = esp poor prognosis
Malignant Fibrous Malignant Fibrous HistiocytomaHistiocytoma
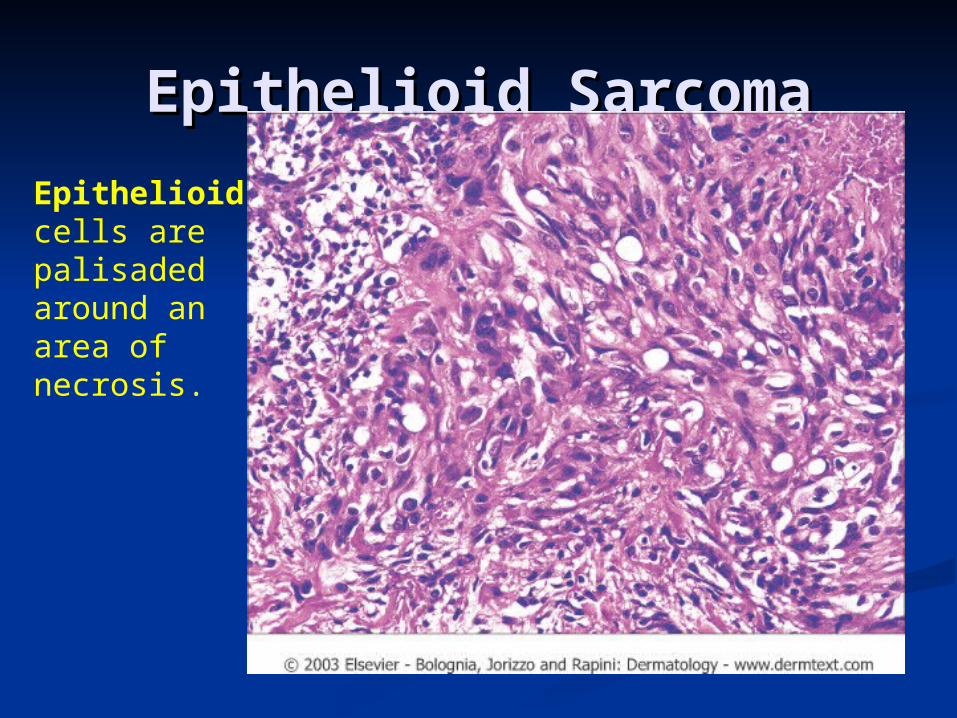
Epithelioid SarcomaEpithelioid Sarcoma Tumor of the extremities (half on hands) of Tumor of the extremities (half on hands) of
young men (2/3 of cases), ages 20-40 young men (2/3 of cases), ages 20-40 years.years.
Slow growing tumor among fascial Slow growing tumor among fascial structures and tendons with nodules and structures and tendons with nodules and overlying ulceration. overlying ulceration. DDX: G.A. fibroma, EIC, ganglion, SSC.DDX: G.A. fibroma, EIC, ganglion, SSC.
HX: Acidophilic polygonal cells merging HX: Acidophilic polygonal cells merging with spindle cells and hyalinized collagen.with spindle cells and hyalinized collagen.
TX: Wide local excision in early disease. TX: Wide local excision in early disease. Recurrence in 3 of 4 cases. Late mets in Recurrence in 3 of 4 cases. Late mets in 45%45%
Epithelioid SarcomaEpithelioid Sarcoma
Epithelioid cells are palisaded around an area of necrosis.
MyxomasMyxomas2 types:2 types:
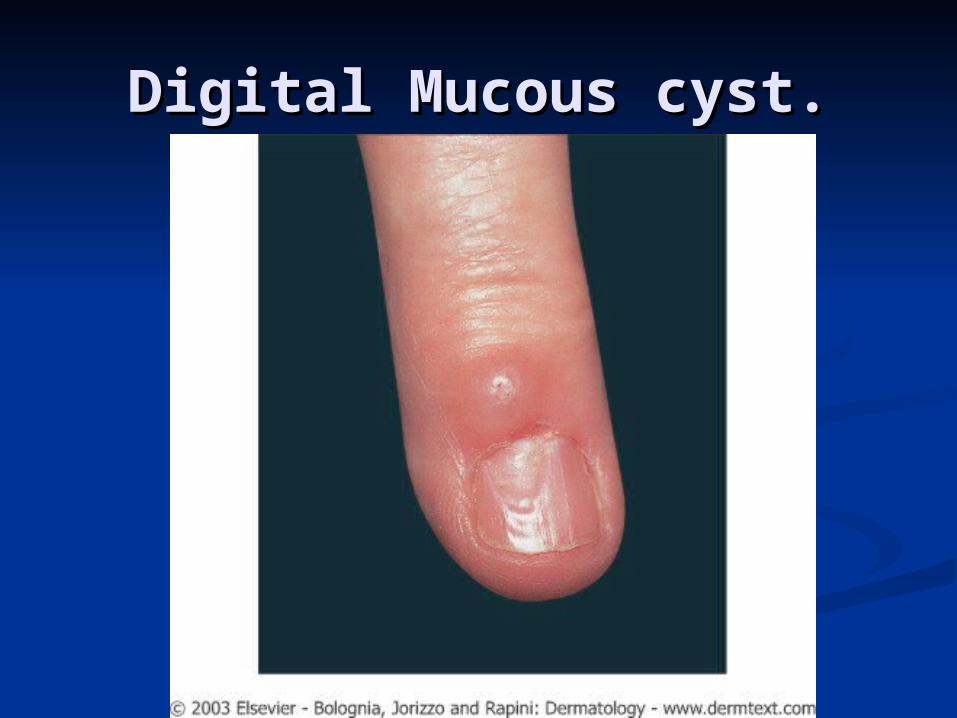
1.) Digital Mucous cyst.1.) Digital Mucous cyst. Taut, shiny translucent white or pink Taut, shiny translucent white or pink
dome shaped lesions typically located dome shaped lesions typically located distal to the DIP joint. Often with distal to the DIP joint. Often with accompanying grooving and dystrophy of accompanying grooving and dystrophy of the associated nail.the associated nail.
Focal accumulations of mucin without a Focal accumulations of mucin without a true lining.true lining.
Etiology: Assoc with joint space and forms Etiology: Assoc with joint space and forms by extrusion of jt. space mucin? by extrusion of jt. space mucin? Independent of jt. space?Independent of jt. space?
TX: Drain, Excision. Intralesional steroids.TX: Drain, Excision. Intralesional steroids.
Digital Mucous cyst.Digital Mucous cyst.
MyxomasMyxomas2.) Cutaneous Myxomas2.) Cutaneous Myxomas Solitary of multiple flesh colored Solitary of multiple flesh colored
nodules of the trunk, face or nodules of the trunk, face or extremities.extremities.
Syndromes: CarneySyndromes: Carney (Also called: NAME, LAMB (Also called: NAME, LAMB ect.)ect.)
Autosomal dominate inheritanceAutosomal dominate inheritance
Carney syndrome (2+ of following)Carney syndrome (2+ of following)1.1. Cardiac Atrial Myxoma (79%) Can be life threatening.Cardiac Atrial Myxoma (79%) Can be life threatening.
2.2. Cutaneous myxomasCutaneous myxomas (45%) <1 cm flesh colored papules (45%) <1 cm flesh colored papules which develop by the age of 18 and occur on ears, eyelids and which develop by the age of 18 and occur on ears, eyelids and nipples.nipples.
3.3. Mammary myxoid fibromas (30%)Mammary myxoid fibromas (30%)
4.4. Spotty mucocutaneous pigmentation (blue nevi) (65%)Spotty mucocutaneous pigmentation (blue nevi) (65%)
5.5. Prim. Pig. Nodular adrenocortical disease. (45%)Prim. Pig. Nodular adrenocortical disease. (45%)
6.6. Testicular tumors (56%)Testicular tumors (56%)
7.7. Pituitary G.H. secreting tumors. (10%)Pituitary G.H. secreting tumors. (10%)





























