Embed Size (px)
Citation preview
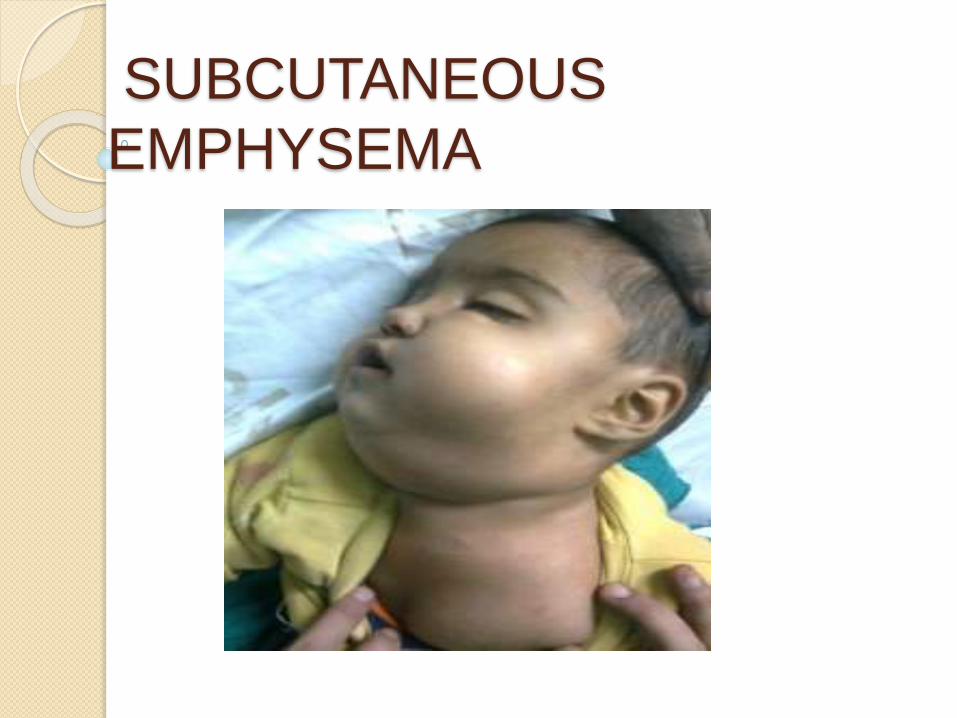
SUBCUTANEOUS
EMPHYSEMA
INTRODUCTION
Emphysema - Greek word, ‘whick’ - ‘to blow in.’
Subcutaneous emphysema of the head,neck, and thorax is caused by the introduction of air into the fascial planes of the connective tissue.
Because of the looseness of the connective tissue and its distensible walls, air can accumulate in these crevices and convert them into spaces of considerable size.
Periorbital emphysema is
subcutaneous emphysema that arises
when air is introduced into the
periorbital tissues.
Subcutaneous emphysema arises
when air is forced, under pressure, into
the subcutaneous fascia leading to a
sudden
onset of soft tissue swelling
compressed air {air syringe}
patent canal
periapical tissue
labial cortical plate,
periorbital space. Periorbital space - low tissue resistance air accumulates readily in this space -
sudden onset of the swelling of upper and lower eyelids.
Pressurised air
labial sinus tract gingival sulcus
periorbital emphysema
CAUSES
During apical surgery, air from a high-
speed drill can lead to air emphysema.
Blowing the nose vigorously
Habitual performance of Valsalva
manoeuvre
Playing a wind instrument after an
extraction
Trauma
Vigorous coughing
Surgical procedures during which air is
introduced into soft tissue spaces.
Endodontic origin occur following the
use of air-driven handpieces,
use of H2O2 irrigation
use of air syringe to dry the canal
Any time a stream of air is directed
toward exposed soft tissues, the
potential for a problem exists.
Signs & symptoms
Immediate
Local soft skin-
coloured swelling
without redness
Crepitus
Local discomfort
Subsequent
Diffuse swelling
Local erythema
Pyrexia and Pain
Hayduk et al. regard crepitus as
pathognomonic of tissue space emphysema
which allows one to quickly rule out
anaphylactic reaction.
Dysphagia
Dyspnea: Migration of air into the neck region
could cause respiratory difficulty, and
progression into the mediastinum could
cause death.
Pain is a variable feature of
subcutaneous emphysema and
patients usually complain of
discomfort due to soft tissue
distension.
Unlike irrigant extrusion reactions,
tissue space emphysema remains in
the subcutaneous connective tissue
and usually does not spread to the
deep anatomic spaces
Alarming to the patient and clinician.
Rarely,serious complications such as pneumomediastinum and airway compromise are seen.
On rare occasions trapped air can spread along the fascial planes to the periorbital, mediastinal,parapharyngeal, pericardial and thoracic spaces causing serious and life threatening complications.
Its occurrence in conjunction with
a dental procedure was first reported
more
than a hundred years ago when Turnbull
extracted the premolar of a musician who
blew his bugle immediately after
extraction.
MANAGEMENT
Usually a benign condition that
resolves over 3–10 days as the gas is
resorbed into the blood stream for
eventual excretion via the lungs
Supportive management
Most authors, however, recommend a
course of prophylactic antibiotics,
most commonly penicillin and
analgesics for 10 days to prevent
secondary infection from
dissemination of oral flora along the
emphysematous tract
Cough suppressants may be
prescribed to prevent further air entry
into the fascial planes
A follow-up appointment within 48
hours is imperative to monitor
resolution and signs of infection
Severe cases, hospitalization may be
necessary for observation and follow-
up radiographs
Administration of 100% oxygen via a
non breather mask can hasten the
resolution of emphysema because
oxygen, which replaces the air, is more
readily absorbed.
Nitrous oxide sedation: the
administration of nitrous oxide should
be discontinued because the gas will
diffuse into the air spaces and increase
the volume of trapped air.
PREVENTION
Avoiding the use of direct
compressed air to dry root canals.
Using remote exhaust handpieces or
electric motor driven ones.
Avoiding the use of hydrogen
peroxide as a root canal irrigant.
Using sterile cotton pellets and
endodontic paper points to dry root
canals.
In surgical procedures, once a flap is
reflected, apical access can be made
with the slowspeed or high-speed
handpieces that do not direct jets of
air into surgery sites
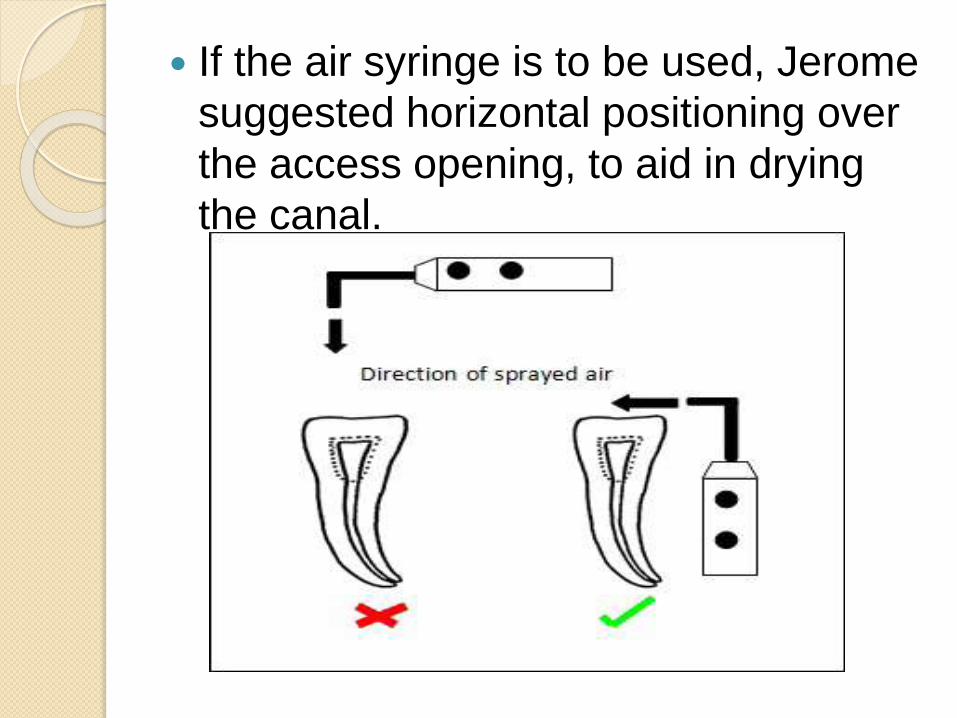
If the air syringe is to be used, Jerome
suggested horizontal positioning over
the access opening, to aid in drying
the canal.
CONCLUSION
Subcutaneous emphysema is a rare but potentially serious complication of root canal treatment.
Characterised by sudden onset of soft tissue swelling, associated with crepitus, during or shortly after the procedure.
Introduction of compressed air into tissue spaces via patent canals, sinus tracts, soft tissue lacerations, or gingival sulcus is the underlying mechanism in most cases.
Therefore, blowing compressed air
into root canals should be avoided and
paper points should be used to dry
root canals.
The majority of cases are managed
conservatively and patients should be
advised as to the nature of
emphysema
REFERENCES
A. Al-Qudah, F. Amin and Y. Hassona.
Periorbital emphysema during
endodontic retreatment of an upper
central incisor:a case report:British
Dental Journal nov 9 2013; 215(9)
Dr. Abdul Hameed.Periorbital
emphysema unexpected
complication;Your Guide on the path
of Dentistry.
Rakesh K. Yadav ,Anil Chandra ,A. P.
Tikku, K. K.Wadhwani,Promila verma;
Air emphysema - an in office
emergency: A case report.
Lora Mishra, Swarnav Patnaik,
Sangram Patro, Nitai Debnath,
Satyaranjan Mishra. Iatrogenic
Subcutaneous Emphysema of
Endodontic Origin – Case Report with
Literature Review. Journal of Clinical
and Diagnostic Research. 2014 Jan,
8(1): 279-281
Manon Paquette. Subcutaneous Emphysema; Clinical Images in Oral Medicine and Maxillofacial Radiology



![Case Report Subcutaneous Emphysema, Pneumomediastinum, … · 2019. 7. 31. · [ ]E.Hillewig,E.Aghayev,C.Jackowski,A.Christe,T.Plattner, and M. J. ali , Gas embolism following intraosseous](https://img.pdfslide.net/doc/110x75/61254bca97cc8d09c20890f9/case-report-subcutaneous-emphysema-pneumomediastinum-2019-7-31-ehillewigeaghayevcjackowskiachristetplattner.jpg)

![Case Report Subcutaneous Emphysema, …downloads.hindawi.com/journals/criem/2015/134816.pdfpneumothorax, pneumomediastinum, pneumopericardium, or subcutaneous emphysema [ ]. Diagnosis](https://img.pdfslide.net/doc/110x75/5f4072ff5627821a5534fd08/case-report-subcutaneous-emphysema-pneumothorax-pneumomediastinum-pneumopericardium.jpg)























