Embed Size (px)
Citation preview
Vol. 17, No. 1JOURNAL OF CLINICAL MICROBIOLOGY, Jan. 1983, p. 149-1540095-1137/83/010149-06$02.00/0Copyright © 1983, American Society for Microbiology
Detection of Genital Herpes Simplex Infections by a TissueCulture-Fluorescent-Antibody Technique with Biotin-Avidin
LATA S. NERURKAR,* ANNAMMA J. JACOB, DAVID L. MADDEN, AND JOHN L. SEVER
Infectious Diseases Branch, National Institute of Neurological and Communicative Disorders and Stroke,Bethesda, Marvland 20205
Received 1 September 1982/Accepted 13 October 1982
Several cell lines were evaluated for their suitability for rapid detection ofherpes simplex virus (HSV) from clinical genital specimens. Human foreskinfibroblast (Flow 7000) cells were found to be most suitable in terms of sensitivityand adherence characteristics. HSV in clinical specimens was isolated by astandard tissue culture method by monitoring the cytopathic effect, and the titersof the HSV-positive specimens were determined. More than 65% of the HSV-positive genital specimens showed titers of <104 50% tissue culture infectivedoses per ml. The standard tissue culture-cytopathic effect method required 3 to10 days for detection ofHSV in clinical specimens of low infectivity. A more rapidtechnique was developed which involved a short-term tissue culture (24 h) onLab-Tek chambers followed by staining with biotin-linked HSV antibody andavidin-fluorescein conjugate. Because of the high binding affinity of this systemdue to multiple binding of biotin to avidin and multiple attachment of biotin to theantibody molecule, the biotin-avidin fluorescent-antibody technique produced aquality of fluorescence far superior to that of the conventional fluorescent-antibody techniques. The tissue culture-biotin-avidin fluorescent-antibody meth-od was as sensitive as the tissue culture-cytopathic effect test. This methodprovides an improved, more rapid test (26 h) for detecting HSV in clinicalspecimens.
Herpes simplex virus (HSV) genital infectionin pregnancy may cause severe damage to thenewborn (28). Most often, the baby acquires theinfection from the mother at the time of delivery(4, 16, 20). If the infection can be diagnosed inthe mother before delivery, cesarean section canbe performed to avoid exposure of the child tothe infected genital area. High-risk women arethose who have had prior genital herpes or asexual partner with genital herpes. These wom-en should have vaginal or cervical culturesweekly for HSV beginning at week 34 of gesta-tion (7). A child born to an infected mothershould be examined for virus to determinewhether the infection has been transmitted andshould be treated. To diagnose a maternal ornewborn infection requires the most rapid andsensitive diagnostic technique available. Theobjective of the present research was to developa more rapid, sensitive technique for the detec-tion of HSV in infected women and babies.
Tissue culture (TC) isolation of virus has beenthe most sensitive technique available to detectHSV (6, 8, 19, 22); however, it is relatively slowand may take up to 7 to 10 days for a finaldetermination in specimens with low infectivity.In many instances, this is too long an interval in
relation to pending delivery of a pregnancy orfor early confirmation of fetal infection. Fluores-cent-antibody (FA) (24), direct immunoperoxi-dase (8), and Papanicolaou or crystal violet (5)staining of the scrapings of HSV lesions havebeen tried, but these methods are less sensitivefor detecting HSV than is TC virus isolation.The present report describes a combination ofTC for 24 h and a highly specific and sensitiveFA test with biotin-linked anti-HSV type 2(HSV-2) antibody and avidin-fluorescein conju-gate for the detection of HSV.
(This work was presented in part at the 66thAnnual Meeting of the Federation of AmericanSocieties for Experimental Biology, New Or-leans, April 1982 [L. Nerurkar, A. Jacob, andD. L. Madden, Fed. Proc. 41:789, 1982].)
MATERIALS AND METHODS
Collection of specimens. The specimens were collect-ed by rubbing lesions in genital or vaginal areas withcotton swabs. The swabs were transported in 3 ml ofEagle minimum essential medium containing strepto-mycin, penicillin, and mycostatin (henceforth referredto as collection medium), refrigerated before trans-port, and frozen at -70°C if not studied immediately(22). Some of the cultures studied were obtained as
149
on May 28, 2019 by guest
http://jcm.asm
.org/D
ownloaded from
150 NERURKAR ET AL.
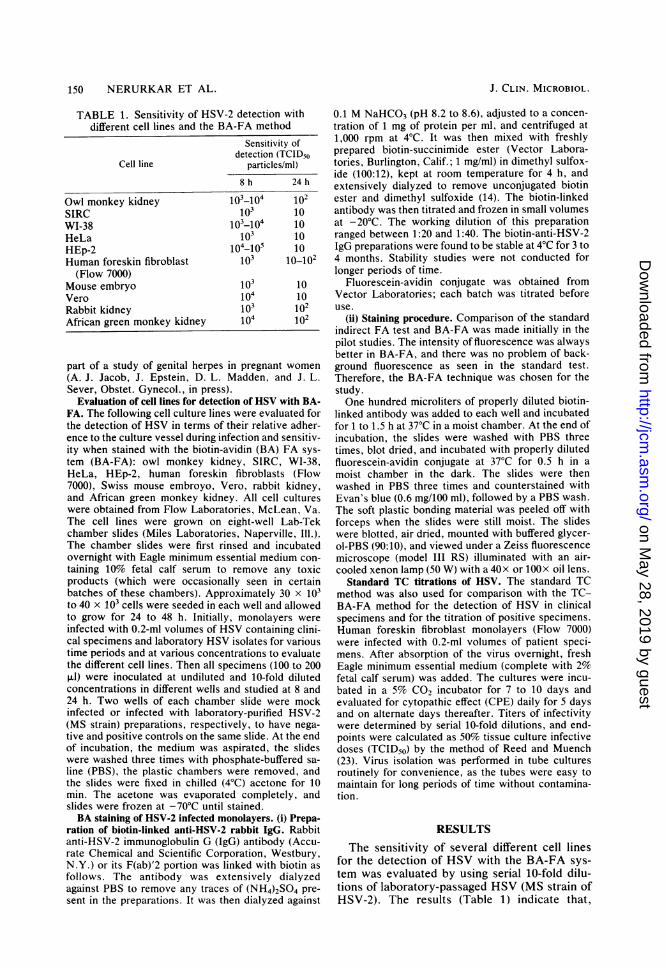
TABLE 1. Sensitivity of HSV-2 detection withdifferent cell lines and the BA-FA method
Sensitivity ofdetection (TCID50
Cell line particles/ml)
8 h 24 h
Owl monkey kidney 10-_104 102SIRC 103 10WI-38 103-104 10HeLa 103 10HEp-2 104-105 10Human foreskin fibroblast 103 10_102(Flow 7000)
Mouse embryo 103 10Vero 104 10Rabbit kidney 103 102African green monkey kidney 104 102
part of a study of genital herpes in pregnant women
(A. J. Jacob, J. Epstein, D. L. Madden, and J. L.Sever, Obstet. Gynecol., in press).
Evaluation of cell lines for detection of HSV with BA-FA. The following cell culture lines were evaluated forthe detection of HSV in terms of their relative adher-ence to the culture vessel during infection and sensitiv-ity when stained with the biotin-avidin (BA) FA sys-
tem (BA-FA): owl monkey kidney, SIRC, WI-38,HeLa, HEp-2, human foreskin fibroblasts (Flow7000), Swiss mouse embroyo, Vero, rabbit kidney,and African green monkey kidney. All cell cultureswere obtained from Flow Laboratories, McLean, Va.The cell lines were grown on eight-well Lab-Tekchamber slides (Miles Laboratories, Naperville, Ill.).The chamber slides were first rinsed and incubatedovernight with Eagle minimum essential medium con-
taining 10% fetal calf serum to remove any toxicproducts (which were occasionally seen in certainbatches of these chambers). Approximately 30 x 103to 40 x 103 cells were seeded in each well and allowedto grow for 24 to 48 h. Initially, monolayers were
infected with 0.2-ml volumes of HSV containing clini-cal specimens and laboratory HSV isolates for varioustime periods and at various concentrations to evaluatethe different cell lines. Then all specimens (100 to 200p.l) were inoculated at undiluted and 10-fold dilutedconcentrations in different wells and studied at 8 and24 h. Two wells of each chamber slide were mockinfected or infected with laboratory-purified HSV-2(MS strain) preparations, respectively, to have nega-
tive and positive controls on the same slide. At the endof incubation, the medium was aspirated, the slideswere washed three times with phosphate-buffered sa-
line (PBS), the plastic chambers were removed, andthe slides were fixed in chilled (4°C) acetone for 10min. The acetone was evaporated completely, andslides were frozen at -70°C until stained.BA staining of HSV-2 infected monolayers. (i) Prepa-
ration of biotin-linked anti-HSV-2 rabbit IgG. Rabbitanti-HSV-2 immunoglobulin G (IgG) antibody (Accu-rate Chemical and Scientific Corporation, Westbury,N.Y.) or its F(ab)'2 portion was linked with biotin as
follows. The antibody was extensively dialyzedagainst PBS to remove any traces of (NH4)2SO4 pre-
sent in the preparations. It was then dialyzed against
0.1 M NaHCO3 (pH 8.2 to 8.6), adjusted to a concen-tration of 1 mg of protein per ml, and centrifuged at1,000 rpm at 4°C. It was then mixed with freshlyprepared biotin-succinimide ester (Vector Labora-tories, Burlington, Calif.; 1 mg/ml) in dimethyl sulfox-ide (100:12), kept at room temperature for 4 h, andextensively dialyzed to remove unconjugated biotinester and dimethyl sulfoxide (14). The biotin-linkedantibody was then titrated and frozen in small volumesat -20°C. The working dilution of this preparationranged between 1:20 and 1:40. The biotin-anti-HSV-2IgG preparations were found to be stable at 4°C for 3 to4 months. Stability studies were not conducted forlonger periods of time.
Fluorescein-avidin conjugate was obtained fromVector Laboratories; each batch was titrated beforeuse.
(ii) Staining procedure. Comparison of the standardindirect FA test and BA-FA was made initially in thepilot studies. The intensity of fluorescence was alwaysbetter in BA-FA, and there was no problem of back-ground fluorescence as seen in the standard test.Therefore, the BA-FA technique was chosen for thestudy.One hundred microliters of properly diluted biotin-
linked antibody was added to each well and incubatedfor 1 to 1.5 h at 37°C in a moist chamber. At the end ofincubation, the slides were washed with PBS threetimes, blot dried, and incubated with properly dilutedfluorescein-avidin conjugate at 37°C for 0.5 h in amoist chamber in the dark. The slides were thenwashed in PBS three times and counterstained withEvan's blue (0.6 mg/100 ml), followed by a PBS wash.The soft plastic bonding material was peeled off withforceps when the slides were still moist. The slideswere blotted, air dried, mounted with buffered glycer-ol-PBS (90:10), and viewed under a Zeiss fluorescencemicroscope (model III RS) illuminated with an air-cooled xenon lamp (50 W) with a 40x or 100x oil lens.
Standard TC titrations of HSV. The standard TCmethod was also used for comparison with the TC-BA-FA method for the detection of HSV in clinicalspecimens and for the titration of positive specimens.Human foreskin fibroblast monolayers (Flow 7000)were infected with 0.2-ml volumes of patient speci-mens. After absorption of the virus overnight, freshEagle minimum essential medium (complete with 2%fetal calf serum) was added. The cultures were incu-bated in a 5% CO2 incubator for 7 to 10 days andevaluated for cytopathic effect (CPE) daily for 5 daysand on alternate days thereafter. Titers of infectivitywere determined by serial 10-fold dilutions, and end-points were calculated as 50% tissue culture infectivedoses (TCID50) by the method of Reed and Muench(23). Virus isolation was performed in tube culturesroutinely for convenience, as the tubes were easy tomaintain for long periods of time without contamina-tion.
RESULTSThe sensitivity of several different cell lines
for the detection of HSV with the BA-FA sys-tem was evaluated by using serial 10-fold dilu-tions of laboratory-passaged HSV (MS strain ofHSV-2). The results (Table 1) indicate that,
J. CLIN. MICROBIOL.
on May 28, 2019 by guest
http://jcm.asm
.org/D
ownloaded from
DETECTION OF HSV BY TISSUE CULTURE-FA
TABLE 2. Quantitation of infectivity of HSV ingenital herpes specimens (n = 416)"
TCID51, No. of Type of infectionparticles/ml specimens Primary Recurrent
>106.1 3 1 2_A16 O 2 2 0
1041105O 6 2 41031-104o0 5 0 5102 _1103. 2 0 210lo l1020 4 0 4
'10 13 0 13Negative 381
a Mean titerTCID50/ml.
of HSV-positive specimens = 102.8
although there were some differences in sensitiv-ity at 8 h, all the cell lines studied gave quitecomparable sensitivities after 24 h of incubation(sensitivity to approximately 10 TCID50 parti-cles of virus per ml, the highest dilution evaluat-ed). The final choice of the cell line to be used inthe routine assay was made on the basis ofrelative adherence to the culture vessel andintactness of the monolayers with high HSVinfective doses (-104 TCID50 particles per ml).With the low infective doses (<104 TCID50particles per ml), cell cultures generally main-tained good integrity up to 24 h. Human foreskinfibroblasts (Flow 7000) or WI-38 cell lines gavethe best adherence for BA-FA testing. Other cellcultures tended to round up and slough from themonolayer. The human fibroblast line (Flow7000) was selected for all subsequent studies.The clinical genital HSV specimens were then
tested with the standard TC-CPE method, andthe sensitivity was compared with that of theTC-BA-FA method. It was possible to test only41 of 381 negative specimens (Table 2). Thetiters of specimens which were found to containHSV by the TC-CPE method were then deter-mined by the same method. The CPE includedthe enlargement and rounding up of cells, thedevelopment of inclusions, and cell fusion. TheTCID50 titers were calculated as described pre-viously (23) (Table 2). Of 416 specimens tested,35 were found to be culture positive, and more
than 65% of the culture-positive specimens hadviral titers of 104/ml, with a mean titer of 102.8TCID50/ml. Only five specimens were from pa-tients with primary infections, and their viraltiters were relatively high compared with thoseobtained from patients with recurrent infections.The comparison of the TC-CPE method with
the TC-BA-FA technique with TC-grown refer-ence HSV showed that low-titer virus cultures(<104 TCID50/ml) required 3 to 7 days and high-titer virus cultures (2104 TCID50/ml) required 1to 3 days to show CPE evidence of infectionwith the TC-CPE method. The genital cultures
with titers of <10 required up to 10 days to showCPE. With the TC-BA-FA method, HSV wasdetected in low-titer virus cultures in 26 h and inhigh-titer virus cultures in 10 h. Care was takento examine the microscope fields which hadmonolayers and not multilayered areas, becausethe latter gave false high intensity of fluores-cence. At least 15 to 20 high-power fields werescreened before a specimen was considered neg-ative. The results of 24 h of incubation wereconsidered more reliable than 8 h, as this al-lowed sufficient viral replication to detect smalldetect small amounts of virus.The TC-BA-FA method completely correlat-
ed with the TC-CPE method for the detection ofHSV in clinical specimens. With both methods,24 positive and 37 negative specimens weredetected in swab cultures taken from patientswith suspected genital herpes.The biotin linking of anti-HSV IgG or the
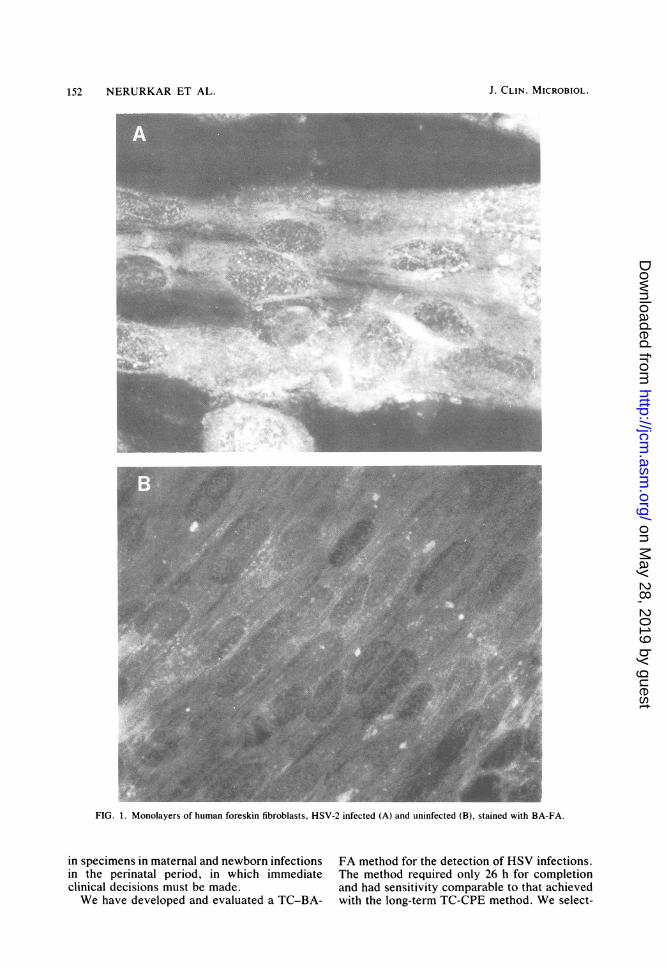
F(ab)'2 fragment retained the affinity for HSVbinding, unlike other procedures in which anenzyme or marker protein is conjugated withimmunoglobulin (1). The biotin linking was sta-ble for at least 3 to 5 months at 4°C, and nodissociation was noticed, as indicated by thecheckerboard titration analysis performed at dif-ferent time intervals. The quality of fluorescenceon positive specimens was far superior to theconventional indirect FA technique (IgG-fluoresceinated anti-IgG), which was initiallyused for comparison. The intensity of fluores-cence was distinctly bright in positive speci-mens, and the negative specimens were devoidof any fluorescence (Fig. 1). The clear-cut de-markation of positive and negative results is animportant criterion of a good staining technique.Figure 1 includes a positive and a negativespecimen studied by the TC-BA-FA methodwith the human fibroblast cell line. The non-fluorescing negative results indicate that avidinreagent does not bind to the fixed preparationsdirectly. However, its usage on unfixed prepara-tions is not yet advocated, as preliminary resultshave indicated that certain cell lines show someaffinity for nuclear binding.
DISCUSSIONWe observed that titers of most of the clinical
genital herpes specimens ranged from <10 to107.2 TCID50, with a mean of 102-8 TCID50/ml.Guinan et al. (13) reported comparable meanHSV titers (103.2) in specimens collected fromwomen with genital herpes. The wide range ofHSV titers in genital specimens may have result-ed from the differences in severity of infectionand the manner and time of specimen collection(5, 8). The high titers of HSV in primary infec-tions were of particular interest. A rapid andsensitive test is necessary for detection of HSV
VOL. 17, 1983 151
on May 28, 2019 by guest
http://jcm.asm
.org/D
ownloaded from
152 NERURKAR ET AL.
.1 .., . '9.1"'.011. l.., :,-.,A ''A.. .; t %. I,-:5,1% ..,
PR
$. Pt
FIG. 1. Monolayers of human foreskin fibroblasts, HSV-2 infected (A) and uninfected (B), stained with BA-FA.
in specimens in maternal and newborn infectionsin the perinatal period, in which immediateclinical decisions must be made.We have developed and evaluated a TC-BA-
FA method for the detection of HSV infections.The method required only 26 h for completionand had sensitivity comparable to that achievedwith the long-term TC-CPE method. We select-
J. CLIN. MICROBIOL.
on May 28, 2019 by guest
http://jcm.asm
.org/D
ownloaded from
DETECTION OF HSV BY TJSSUE CULTURE-FA 153
ed a human fibroblast line for the test to providegood initial growth of the virus and adherence ofthe cells to the culture surface. This was fol-lowed by the highly sensitive and specific FAtest with the BA system. This test reduced thetime required for diagnosis of HSV to 24 h ofgrowth in TC and 2 h of staining.The choice of tissue culture cell lines for
standard TC-CPE detection of HSV varies indifferent laboratories. Human embryonic lungfibroblasts (WI-38), primary rabbit kidney cells,and Vero cells are the more commonly used celllines (22). Recently, guinea pig embryonic cellcultures have been shown to be equally sensitivefor HSV isolation (15). With all of these celllines, cultures of HSV must be observed for 7 to10 days before they can be reported as negative.
Direct staining of scrapings from genital le-sions is a rapid and easy method. The outcome,however, depends on the number of intact cellsshowing morphological changes or the presenceof viral antigens or both. Hence, the propertiming and manner of specimen collection be-comes very important. In most studies, thesetests detect only 40 to 80% of the virus-positivespecimens (5, 8, 24).
Short-term TC followed by the detection ofviral antigens (TC-BA-FA) is a reliable, relative-ly rapid method. It permits detection of bothextracellular and cell-associated infectious viruspresent in specimens. The method amplifiessmall amounts of virus present in some speci-mens, thus improving the sensitivity of the test.TC in combination with either immunologicalstaining or electron microscopy has been used inthe past for detection of HSV (10, 17, 18) orother viruses (9, 25, 26). These studies haveused conventional methods, employing direct orindirect FA techniques with fluorescein or per-oxidase labels.We believe this is the first report of the use of
the BA-FA method for the detection of viralantigens (L. Nerurkar, A. Jacob, and D. L.Madden, Fed. Proc. 41:789, 1982). This systemshould be able to improve the detection of otherviral antigens and antibodies if the proper choiceof reagents is made (12). There has been apreliminary report describing the use of thisreagent in the detection of antibodies to hepatitisB antigen (C. Kendall, I. Ionescu-Matiu, andG. R. Dreesman, Fed. Proc. 41:789, 1982). Thehigh affinity of binding of biotin to avidin, multi-ple binding of biotin to antibody, multiple bind-ing of avidin to individual biotin molecules,which is almost irreversible (3, 11), and ease ofpreparation of reagents may eventually causethis system to replace the use of antiglobulinconjugates in the conventional indirect stainingprocedures. The combination of TC followed bystaining with the BA system seems to reduce
both false-positive and false-negative results,which makes the detection more reliable ascompared with the direct tissue staining proce-dures previously described (8, 19). Furthermore,it appears to minimize or eliminate interferenceby Fc receptors binding to the Fc portion of theantibody (2, 21, 27), which may give some false-positive results.Emphasis in the future will have to be on
further shortening the time required to accurate-ly diagnose HSV infections. In the meantime,this method appears to be particularly valuablefor clinical situations which require the rapiddetection of HSV.
ACKNOWLEDGMENTS
The authors gratefully acknowledge the excellent technicalhelp of Frank West, Kenneth Rich, and Michael May and thediligent typing of Lin Aspinall in the preparation of themanuscript. We are grateful to Maternity Center Associates,Bethesda, Md., Sigma Clinic, Wheaton, Md., Ob/Gyn Asso-ciates, Bethesda, Md., and R. S. Margolis and R. Orleans,Bethesda, Md., for participating in the clinical phases of thisstudy.
LITERATURE CITED
1. Avrameas, S., T. Ternynck, and J. L. Guesdon. 1978.Coupling of enzymes to antibodies and antigens. Scand. J.Immunol. 8(Suppl. 7):7-23.
2. Baucke, R. B., and P. G. Spear. 1979. Membrane proteinsspecified by herpes simplex viruses. V. Identification ofan Fc binding glycoprotein. J. Virol. 32:779-789.
3. Bayer, E., and M. Wilchek. 1975. Insolubilized biotin forthe purification of avidin. Methods Enzymol. 34:265-267.
4. Brann, A. W., R. T. Hall, R. G. Harper, G. A. Little,M. J. Maisels, G. H. McCracken, R. L. Poland, P. Sun-shine, and J. A. Whittinghill. 1980. Perinatal herpes sim-plex infections. Committee on fetus and newborn andcommittee on infectious disease. Pediatrics 66:147-149.
5. Brown, S. T., H. W. Jaffe, A. Zaidi, R. Filker, K. L.Herrmann, H. C. Lylerla, D. F. Jove, and J. W. Budell.1979. Sensitivity and specificity of diagnostic tests forgenital infection with herpes virus hominis. Sex. Transm.Dis. 6:10-13.
6. Cho, C. T., and K. K. Feng. 1978. Sensitivity of virusisolation and immunofluorescent staining methods in diag-nosis of infections with herpes simplex virus. J. Infect.Dis. 138:536-540.
7. Committee on Obstetrics. 1980. Maternal and fetal medi-cine committee statement. American College of Obstet-rics and Gynecology, Chicago, Ill.
8. Corey, L., J. Dragavon, and D. Benjamin. 1982. Immuno-peroxidase staining in the clinical virology laboratory, p.246-253. In R. C. Tilton (ed.), Rapid methods and auto-mation in microbiology. American Society for Microbiolo-gy, Washington, D.C.
9. Gardner, P. S., and J. McQuillin. 1980. Rapid virus diag-nosis application of immunofluorescence. The WhitefriarsPress Ltd., London.
10. Gardner, P. S., J. McQuillin, M. M. Black, and J. Rich-ardson. 1968. Rapid diagnosis of herpesvirus hominisinfections in superficial lesions by immunofluorescentantibody techniques. Br. Med. J. 4:89-92.
11. Green, N. M. 1975. Avidin. Adv. Protein Chem. 29:85-133.
12. Guesdon, J. L., T. Ternynck, and S. Avrameas. 1979. Theuse of avidin-biotin interaction in immunoenzymatic tech-niques. J. Histochem. Cytochem. 27:1131-1139.
13. Guinan, M. E., J. MacCalman, E. R. Kern, J. C. Overall,
VOL. 17, 1983
on May 28, 2019 by guest
http://jcm.asm
.org/D
ownloaded from
154 NERURKAR ET AL.
and S. L. Spruance. 1981. The course of untreated recur-rent genital herpes simplex infection in 27 women. N.Engl. J. Med. 304:759-763.
14. Heitzmann, H., and F. M. Richards. 1974. Use of theavidin-biotin complex for specific staining of biologicalmembranes in electron microscopy. Proc. Nati. Acad.Sci. U.S.A. 71:3537-3541.
15. Landry, M. L., D. R. Mayo, and G. D. Hsiung. 1982.Comparison of guinea pig embryo cells, rabbit kidneycells and human embryonic lung fibroblast cell strains forisolation of herpes simplex virus. J. Clin. Microbiol.15:842-847.
16. Light, I. J. 1979. Postnatal acquisition of herpes simplexvirus by the newborn infant: a review of literature.Pediatrics 63:480-482.
17. Marks, M. I. 1970. Method for preparation of herpesvirushominis fluorescent conjugate for direct immunofluores-cence. Arch. Gesamte Virusforsch. 32:373-378.
18. Miller, S. E., and D. J. Lang. 1982. Rapid diagnosis ofherpes simplex infection: amplification for electron mi-croscopy by short-term in vitro replication. J. Infection4:37-41.
19. Moseley, R. C., L. Corey, D. Benjamin, C. Winter, andM. L. Remington. 1981. Comparison of viral isolation,direct immunofluorescence, and indirect immunoperoxi-dase techniques for detection of genital herpes simplexvirus infection. J. Clin. Microbiol. 13:913-918.
20. Nahmias, A. J., and B. Roizman. 1973. Infection withherpes simplex viruses 1 and 2. N. Engi. J. Med. 289:781-789.
21. Para, M. F., R. B. Bauke, and P. G. Spear. 1980. Immu-
noglobulin G (Fc)-binding receptor on virion of herpessimplex virus type 1 and transfer of these receptors to thecell surface by infection. J. Virol. 34:512-520.
22. Rawls, W. E. 1979. Herpes simplex virus types 1 and 2and herpesvirus simiae, p. 309-373. In E. H. Lennette andN. J. Schmidt (ed.), Viral, rickettsial and chlamydialinfections. American Society for Microbiology, Washing-ton, D.C.
23. Reed, L. J., and M. Muench. 1938. A simple method ofestimating fifty percent endpoints. Am. J. Hyg. 27:493-497.
24. Schmidt, N. J., D. Gallo, V. Devlin, J. D. Woodie, andR. E. Emmons. 1980. Direct immunofluorescence stainingfor detection of herpes simplex and varicella-zoster virusantigens in vesicular lesions and certain tissue specimens.J. Clin. Microbiol. 12:651-655.
25. Schmidt, N. J., H. H. Ho, and J. Chin. 1981. Applicationof immunoperoxidase staining to more rapid detection andidentification of rubella virus isolates. J. Clin. Microbiol.13:627-630.
26. Stagno, S., R. F. Pass, D. W. Reynolds, M. A. Moore,A. J. Nahmias, and C. A. Alford. 1980. Comparativestudy of diagnostic procedures for congenital cytomegalo-virus infection. Pediatrics 65:251-257.
27. Watkins, J. F. 1964. Adsorption of sensitized sheep eryth-rocytes to HeLa cells infected with herpes simplex virus.Nature (London) 202:1364-1365.
28. Whitley, R. J., A. J. Nahmias, A. M. Visintine, C. L.Fleming, and C. A. Alford. 1980. The natural history ofherpes simplex virus infection of mother and newborn.Pediatrics 66:489-494.
J. CLIN. MICROBIOL.
on May 28, 2019 by guest
http://jcm.asm
.org/D
ownloaded from










![The effect of Vesicular stomatitis virus and Herpes ... · herpes and keratitis [1, 29, 30, 39-43]. Primary herpetic oral, genital and ocular diseases are Primary herpetic oral, genital](https://img.pdfslide.net/doc/110x75/5e0ec17e158f1d2c96378503/the-effect-of-vesicular-stomatitis-virus-and-herpes-herpes-and-keratitis-1.jpg)