Embed Size (px)
Citation preview

Genitourin Med 1997;73:314-319
Should aciclovir prophylaxis be used in latepregnancy in women with recurrent genital herpesinfection? How to use a clinical decision analysis
Peter Brocklehurst, Tracy Roberts
IntroductionThe purpose of this article is to explore thebenefits of using decision analysis in clinicaldecision making when the published evidenceabout the effectiveness of an intervention isuncertain. The use of decision analysis will beexplored using the example of aciclovir pro-phylaxis in late pregnancy for women withrecurrent genital herpes infection.' The articledraws on the guidelines published byRichardson and others which set out a frame-work for evaluating the usefulness of a clinicaldecision analysis model (table 1).2 3
National PerinatalEpidemiology Unit,Radcliffe Infirmary,Oxford OX2 6HEP BrocklehurstT RobertsAccepted for publication7 May 1997
THE CLINICAL PROBLEMWomen with genital herpes infection in preg-nancy are at risk of transmitting herpes to theirbaby at the time of delivery resulting in neona-tal herpes infection. Neonatal herpes is a
severe illness with a high mortality and mor-
bidity even with prompt antiviral treatment.4Current management of women with recur-rent genital herpes infection during pregnancyin the UK rests almost entirely on whether thewoman experiences a symptomatic recurrenceat the time of labour. If there is evidence of anactive recurrence then delivery by caesareansection is recommended to avoid the risk ofmother to child transmission.5 If there is noevidence of an active recurrence then a vaginaldelivery is anticipated. The risk of mother tochild transmission is unknown but estimatessuggest that it can be no higher than 8%6although many authorities believe it is signifi-cantly lower than this and some have sug-
gested that it is negligible.7 As a consequenceof the current management policy manywomen with recurrent genital herpes infectionpresent at the time of labour undergo cae-
sarean section when the risk to the neonateappears to be small. An alternative manage-ment strategy which has been suggested is theuse of suppressive aciclovir starting in latepregnancy, usually around 36 weeks, to pre-
vent symptomatic recurrences of herpes andtherefore allow women to anticipate a normalvaginal delivery.8 If breakthrough recurrences
do occur at the time of labour there are twomanagement options. Either deliver by cae-sarean section or allow vaginal delivery andtake viral cultures from the neonate and thenmonitor for signs of herpes infection and treataggressively if either the cultures are positiveor signs occur.
THE EVIDENCE FOR ACICLOVIR SUPPRESSIONA Medline search for randomised trials whichevaluate the effectiveness of aciclovir suppres-
sion in late pregnancy will reveal only one.9
This was conducted in women experiencingtheir first episode of genital herpes infectionduring the index pregnancy. The trial demon-strated a decrease in the incidence of cae-sarean section in the women receivingaciclovir. The generalisability of these resultsto women with pre-existing recurrent herpesinfection is not straightforward. It is possiblethat subsequent recurrences during the preg-nancy in these women are more frequentand/or more severe than those experienced bywomen with pre-existing herpes infection. Inaddition, it appears that these women are at asubstantially increased risk of mother to childtransmission and other adverse neonatal out-comes than women with pre-existing infec-tion.'0 Extrapolating the results of this trial towomen with pre-existing recurrent infection,therefore, seems unwise. There has, however,been a recent economic evaluation byRandolph of the use of suppressive aciclovir inthis group of women which utilises a clinicaldecision model.' We will demonstrate how tocritically appraise this paper using the guide-lines set out by Richardson and Detsky.3
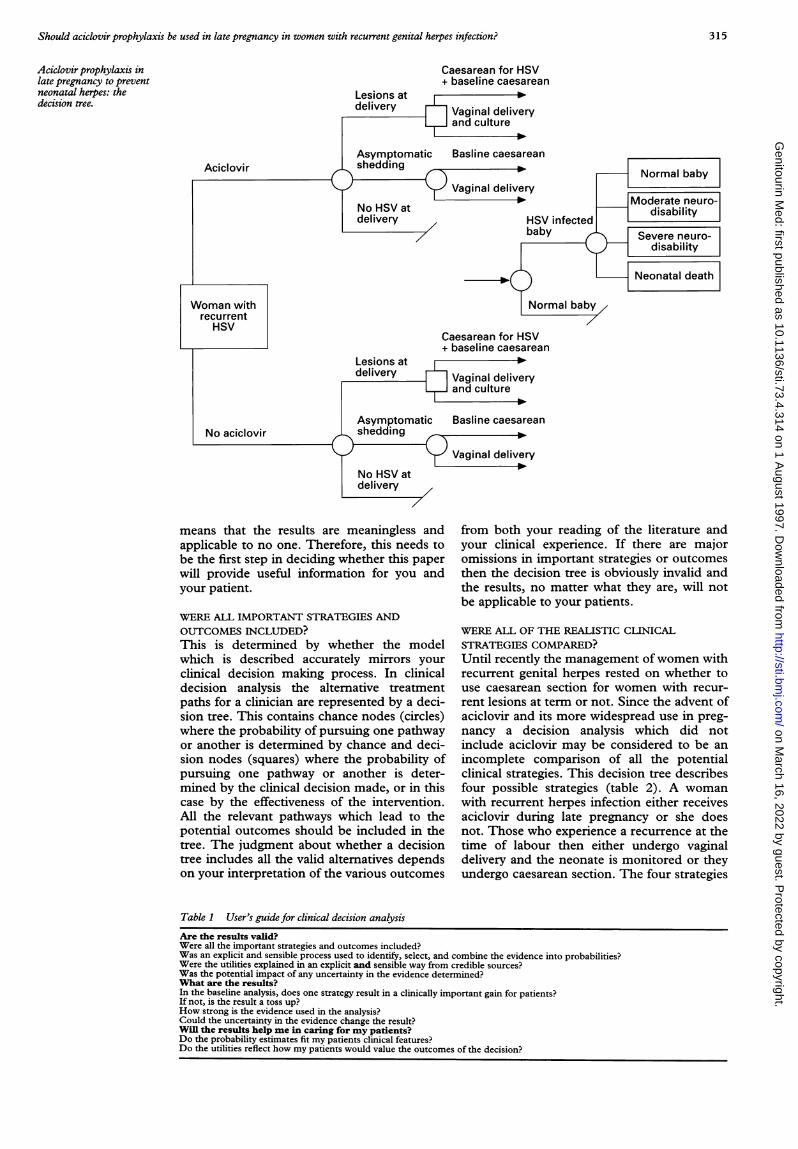
DECISION ANALYSISThe process of decision analysis makes explicitthe decisions involved in clinical practice. Thedecision tree in the paper by Randolph et al(fig) expresses the outcomes which can occurfor both mother and baby whether the womanis given aciclovir or is not given aciclovir. Ineither situation there may be symptomaticrecurrences at the time of delivery which maybe managed by caesarean section or vaginaldelivery and culture, there may be asympto-matic shedding which is not detected at thetime of delivery, or there may be no evidenceof herpes virus at the time of delivery.Probabilities can be attached to each treat-ment path of the decision tree and if there islittle certainty about these probabilities thenranges of probabilities can be incorporatedinto the model.
In order to evaluate the usefulness of anypublished decision analysis it is necessary toaddress (a) whether the results of the study arevalid and (b) what the results actually are andwhether they will help in caring for yourpatient. A framework for assessing a decisionanalysis is included in table 1. This is similarto the framework developed in previous papersin this series."
How valid are the results of the study?The validity of the results is largely determinedby the methods used. An invalid study design
314 on M
arch 16, 2022 by guest. Protected by copyright.
http://sti.bmj.com
/G
enitourin Med: first published as 10.1136/sti.73.4.314 on 1 A
ugust 1997. Dow
nloaded from
Should aciclovir prophylaxis be used in late pregnancy in women with recurrent genital herpes infection?
Aciclovir prophylaxis inlate pregnancy to preventneonatal herpes: thedecision tree.
Lesions atdelivery
Caesarean for HSV+ baseline caesarean
Aciclovir
Caesarean for HSV+ baseline caesarean
No aciclovir
means that the results are meaningless andapplicable to no one. Therefore, this needs tobe the first step in deciding whether this paperwill provide useful information for you andyour patient.
WERE ALL IMPORTANT STRATEGIES AND
OUTCOMES INCLUDED?
This is determined by whether the modelwhich is described accurately mirrors yourclinical decision making process. In clinicaldecision analysis the alternative treatmentpaths for a clinician are represented by a deci-sion tree. This contains chance nodes (circles)where the probability of pursuing one pathwayor another is determined by chance and deci-sion nodes (squares) where the probability ofpursuing one pathway or another is deter-mined by the clinical decision made, or in thiscase by the effectiveness of the intervention.All the relevant pathways which lead to thepotential outcomes should be included in thetree. The judgment about whether a decisiontree includes all the valid alternatives dependson your interpretation of the various outcomes
from both your reading of the literature andyour clinical experience. If there are majoromissions in important strategies or outcomesthen the decision tree is obviously invalid andthe results, no matter what they are, will notbe applicable to your patients.
WERE ALL OF THE REALISTIC CLINICAL
STRATEGIES COMPARED?
Until recently the management ofwomen withrecurrent genital herpes rested on whether touse caesarean section for women with recur-rent lesions at term or not. Since the advent ofaciclovir and its more widespread use in preg-nancy a decision analysis which did notinclude aciclovir may be considered to be an
incomplete comparison of all the potentialclinical strategies. This decision tree describesfour possible strategies (table 2). A woman
with recurrent herpes infection either receivesaciclovir during late pregnancy or she doesnot. Those who experience a recurrence at thetime of labour then either undergo vaginaldelivery and the neonate is monitored or theyundergo caesarean section. The four strategies
Table 1 User's guide for clinical decision analysis
Are the results valid?Were all the important strategies and outcomes included?Was an explicit and sensible process used to identify, select, and combine the evidence into probabilities?Were the utilities explained in an explicit and sensible way from credible sources?Was the potential impact of any uncertainty in the evidence determined?What are the results?In the baseline analysis, does one strategy result in a clinically important gain for patients?If not, is the result a toss up?How strong is the evidence used in the analysis?Could the uncertainty in the evidence change the result?Will the results help me in caring for my patients?Do the probability estimates fit my patients clinical features?Do the utilities reflect how my patients would value the outcomes of the decision?
315 on M
arch 16, 2022 by guest. Protected by copyright.
http://sti.bmj.com
/G
enitourin Med: first published as 10.1136/sti.73.4.314 on 1 A
ugust 1997. Dow
nloaded from

Brocklehurst, Roberts
Table 2 Strategies to prevent neonatal herpes infection. (The number of cases of neonatal herpes infection averted per10 000 women treated)
Number ofwomen Number ofwomen Number ofneonatalwith herpes treated with Number of HSVcasesinfection in cohort aciclovir CS averted
No aciclovir, no CS for herpes 10 000 0 0 0.0No aciclovir, CS for recurrence at labour 10 000 0 1082 2-8Aciclovir, no CS for herpes 10 000 10 000 0 5.0Aciclovir, CS for recurrence at labour 10 000 10 000 216 5-5
CS = caesarean section.Adapted from Randolph et al.'
are therefore: (a) no aciclovir and no caesareansection, (b) no aciclovir and caesarean section ifthere is a recurrence at the time of labour, (c)aciclovir and no caesarean section, and, finally(d) aciclovir and caesarean section if there is arecurrence at the time of labour.An accurate description of the intervention
should be included. The effectiveness of aci-clovir may vary depending on the dose usedand the duration of its use. If aciclovir is to bestarted at 36 weeks' gestation some womenwill have delivered before that time and someof these will have had active recurrences at thetime of delivery; hence, the model is notentirely complete. The extent to which thisalters the management of the majority ofwomen, however, is likely to be small.
WERE ALL CLINICALLY RELEVANT OUTCOMESCONSIDERED?For the mother various outcomes wereincluded in the model: caesarean section forrecurrent herpes infection; caesarean sectionfor other indications regardless of the herpesinfection; or vaginal delivery with or withoutculture. For the baby the health outcomesspecified in the decision tree were either herpesinfection or no herpes infection. For herpesinfected babies there were four eventual out-comes: the baby was normal; the baby hadmoderate neurological disability; the baby hadsevere neurological disability; or the baby died.The neonatal states would appear to represent acomplete range of health outcomes. The out-comes for the mother, however, do not includethe consequences of vaginal or caesarean sec-tion delivery-for instance, post-caesarean sec-tion infectious morbidity or the increased riskof maternal mortality associated with operativedelivery when compared with vaginal delivery.This appears to be because the specific aim ofthe paper was to address the cost of a case ofneonatal herpes averted and, as a consequence,only a partial evaluation was undertaken. Thisdoes not invalidate the study, but readers needto be aware that not all the potentially relevanthealth outcomes are included.
In addition, no mention is made of thepotential side effects of aciclovir for the motherand the baby. Any side effects could beincluded in the decision tree so that an explicitweighing up between the risks and benefits canbe seen. The failure to mention side effects isprobably because of the safety of aciclovir inthis setting with no major side effects havingbeen reported for mother or baby.12Nevertheless, mention of this informationwould have been useful.
WAS AN EXPLICIT AND SENSIBLE PROCESS USEDTO IDENTIFY, SELECT, AND COMBINE THEEVIDENCE INTO PROBABILITIES?The chance and decision nodes of the decisiontree need to be accompanied by probabilitiesthat either pathway will be followed dependingon the preceding event. Probabilities will needto be assembled from a broad range of infor-mation in the medical literature. In order todetermine the probabilities it is necessary toreview critically a large volume of informationusing the processes already described in thisseries so that only those studies where themethods are valid are incorporated. The litera-ture review should be systematic and clearlyexplained if bias is to be avoided.'3 The paperby Randolph et al does not specify the searchstrategy or search terms used to searchMedline, nor does it specify the process ofselection of the studies. The paper clearlystates that "the baseline probability values werethe most plausible estimates". This statementcould be interpreted as suggesting that theauthors only included those articles whichreported estimates which agreed with theirexisting views. A clearer description of theselection process would help to satisfy thoseworried about this statement and how this maycontribute to selection bias. If the analysis isbeing taken beyond a partial analysis, as in thepaper by Randolph et al, to a complete costutility analysis then there may need to be inter-views with patient groups
Once the authors have decided what infor-mation to include they must synthesise it into aquantitative estimate of each probability.Depending on the source of this informationthese probabilities may come with some uncer-tainty, in which case a range of probabilitiesmay be incorporated into the model (seebelow). It is often useful in these publicationsto indicate the strength of the evidence whichhas been used to provide these probability esti-mates. For aciclovir prophylaxis in late preg-nancy the authors have devised a scale from Ato D which assesses the quality of the evidenceresulting in their baseline probability values.Grade A was from data with a high level ofconfidence-for example, randomised con-trolled trials or multicentre cohort studies withconsistent findings, through to grade D whichwas a best guess with no data available. Theauthors assembled an impressive list of proba-bilities with ranges. There are two probabilityestimates, however, which are particularly cru-cial to the decision tree and both these are thedecision nodes. The first is the effectiveness ofaciclovir at preventing lesions at the time of
316 on M
arch 16, 2022 by guest. Protected by copyright.
http://sti.bmj.com
/G
enitourin Med: first published as 10.1136/sti.73.4.314 on 1 A
ugust 1997. Dow
nloaded from
Should aciclovir prophylaxis be used in late pregnancy in women with recurrent genital herpes infection?
labour and hence preventing delivery by cae-sarean section. The second is the effectivenessof caesarean section at preventing mother tochild transmission. These probabilities areessential in this decision tree. As has alreadybeen discussed, however, there are no ran-domised controlled trials of the effectiveness ofaciclovir in this population ofwomen and thereare no large multicentre cohort studiesaddressing this question. Therefore, the proba-bilities used for the effectiveness of aciclovircould be considered to be weaker than is sug-gested by the paper.
WERE THE UTILITIES OBTAINED IN AN EXPLICITAND SENSIBLE WAY FROM CREDIBLE SOURCES?Utilities represent a quantitative measure ofthe value of the various outcomes to the patientor decision makers (whether this be individualclinicians or policy makers). Various methodsof measuring utilities are available and if utili-ties measures are included in a decision analysisone of the accepted methods should bedescribed.'4 This paper did not present data onthe utilities of the various health outcomes. Asthe authors state, this information can beextremely difficult to obtain and difficult tointerpret. Whether utilities have or have notbeen included does not affect the validity of astudy if the study objectives can be achievedwithout utility measurement. Readers, how-ever, need to be aware that this aspect of theclinical scenario may have been omitted.
WAS THE POTENTIAL IMPACT OF ANYUNCERTAINTY IN THE EVIDENCE DETERMINED?Uncertainty in probability estimates can beexpressed by a range of estimates. A sensitivityanalysis can then be carried out by substitutingthe highest and lowest values for the probabili-ties which were included in the original model.Which probability estimates should be variedwill be a matter of judgment and this willdepend to an extent on the level of certainty ofthe estimate. The sensitivity analyses in thepaper by Randolph et al varied three factors.The first of these was the effectiveness of aci-clovir which ranged from 45% to 95%. As hasalready been discussed, however, the estimateof effectiveness of aciclovir has not been deter-mined in this population of women. The rangeof probabilities given assumes that aciclovir iseffective (the lowest estimate used is 45%). Itmay have been more appropriate to vary theselimits between the highest estimate and 0%.The remaining factors in the sensitivity analy-ses include altering the mother to child trans-mission risk at vaginal delivery to 4% (from theoriginal model which included an estimate of1 %) and altering the effectiveness of caesareansection at preventing mother to child transmis-sion from 80% to 0%.
What are the results?IN THE BASELINE ANALYSIS, DOES ONESTRATEGY RESULT IN A CLINICALLYIMPORTANT GAIN FOR PATIENTS? IF NOT, ISTHE RESULT A TOSS UP?The four strategies investigated were com-
pared to explore the effect each had on thenumber of cases of neonatal herpes infectionwhich could be averted per 10 000 women.The strategy which was most effective in thisdecision analysis was that of aciclovir with cae-sarean section if breakthrough recurrencesoccurred at the time of labour (table 2). Thisprevented 5.5 cases of neonatal herpes forevery 10 000 women treated with aciclovir,with 216 of these women undergoing deliveryby caesarean section.
This would suggest, therefore, that usingaciclovir will prevent more cases of neonatalherpes than relying on caesarean section aloneand it will decrease the number of caesareansections by a factor of five (table 2). Theseclinical results were then translated into finan-cial costs which supported these findings andsuggested that the use of aciclovir could dra-matically reduce the cost per case of neonatalherpes averted by a factor of three when com-pared with caesarean section.
HOW STRONG IS THE EVIDENCE USED IN THEANALYSIS?As has already been discussed above thestrength of a clinical decision analysis dependson the strength of the information used withinit. Information from high methodologicalquality studies is likely to be more reliable thanthat from poor quality studies. The paper byRandolph et al has addressed this issue bygrading all the evidence included althoughonce again the evidence to support the clinicaleffectiveness of aciclovir is said to come fromgrade A information and as we have alreadyseen this is not the case. The strength of theremaining evidence is also relatively weak. Theeffectiveness of caesarean section in reducingtransmission is grade D-that is, there are nodata to support this estimate. Likewise the riskof mother to child transmission and the sensi-tivity and specificity of herpes culture aregrade C. As a consequence, a more cautiousinterpretation of the results would seemappropriate.
COULD THE UNCERTAINTY IN THE EVIDENCECHANGE THE RESULT?Sensitivity analyses will demonstrate whetherincluding the extremes of range in the modelwill produce a different result and therefore adifferent interpretation of the relative advan-tages or disadvantages of the various strate-gies. The sensitivity analyses can be verysophisticated and involve two dimensionalgraphs of the variables with various thresholdvalues for probabilities above which one par-ticular strategy is preferred over another andvice versa.The more precise the estimates of probabili-
ties the more likely a sensitivity analysis is toproduce a similar result to the original model.The less robust the evidence, however, themore likely a sensitivity analysis is to produce amodel with a differing result and interpreta-tion. The paper by Randolph et al includes theeffectiveness of aciclovir, the mother to childtransmission rate, and the effectiveness of cae-sarean section in separate sensitivity analyses
317 on M
arch 16, 2022 by guest. Protected by copyright.
http://sti.bmj.com
/G
enitourin Med: first published as 10.1136/sti.73.4.314 on 1 A
ugust 1997. Dow
nloaded from
Brocklehurst, Roberts
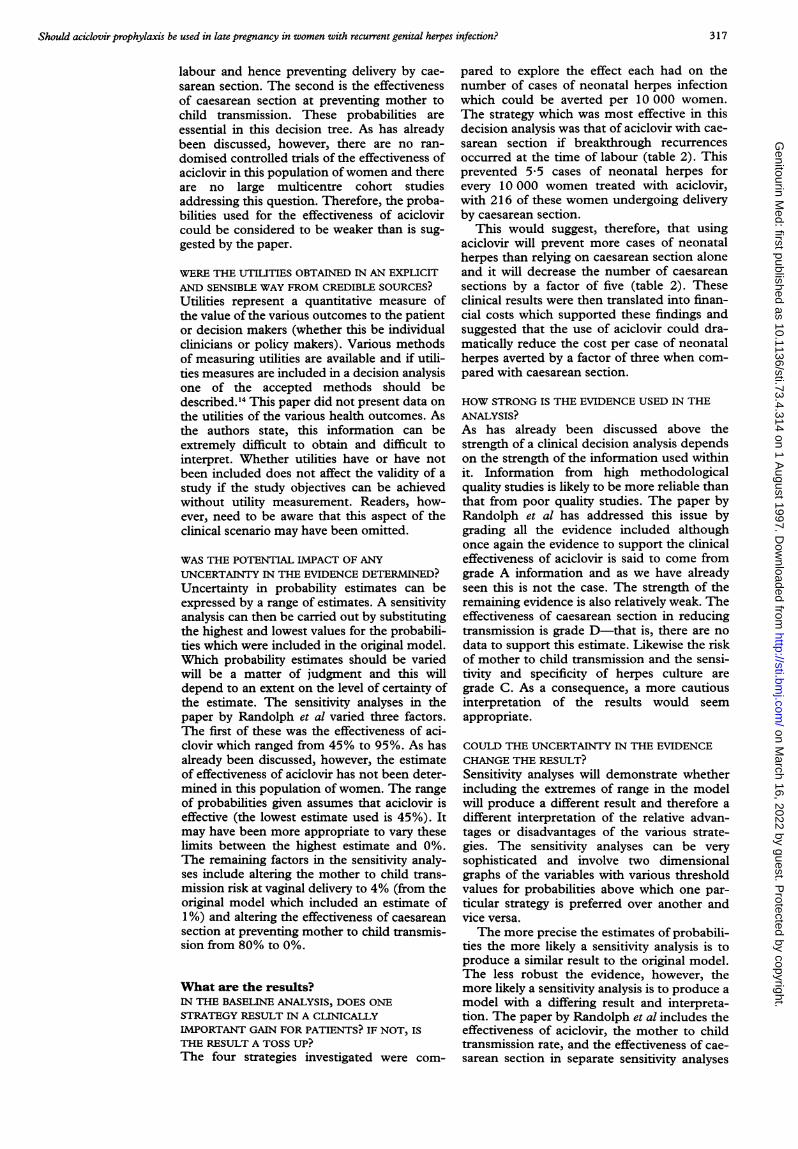
Table 3 Aciclovir to prevent neonatal herpes. Results of the sensitivity analyses
Number of neonatal HSV cases averted per 10 000 women for each of the treatment strategies
No aciclovir, No aciclovir, Aciclovir, Aciclovir,no CS CSfor recurrence no CS for CSfor recurrence
Factor varied in sensitivity analysis for herpes at labour herpes at labour
Effectiveness of aciclovir:80% effective (as in original model) 0.0 2-8 5.0 5-595% effective 0 0 2-8 5.9 6-045% effective 0.0 2-8 2-8 4-3
HSV transmission risk:0-1% (as in original model) 0.0 2-8 5.0 5-50.4% increase in number 1-1 2-0 2-2
of casesEffectiveness of CS:80% effective (as in original model) 0.0 2-8 5.0 5-50% effective 0.0 0.0 6-1 6-1
CS = caesarean section.Adapted from Randolph et al.'
(table 3). Some of these analyses change theresult but not the relation between each of thestrategies. For example, decreasing the motherto child transmission risk increased the num-
ber of women undergoing caesarean sectionand needing treatment with aciclovir to pre-vent a case of neonatal herpes infection.However, the various strategies all maintainthe same position in terms of their relativeeffectiveness to each other. Changing theeffectiveness of caesarean section in preventingmother to child transmission from 80% to 0%,however, would greatly increase the relativeeffectiveness of aciclovir as the strategy of cae-
sarean section for women with herpes wouldprevent no cases but would be at an increasedcost to the women and the health services.
Varying the effectiveness of aciclovir to 95%makes the intervention even more effective at a
lower cost. If aciclovir is 45% effective, how-ever, the use of aciclovir with culture becomesequally effective with no aciclovir and cae-
sarean section (although at a lower cost). Ashas already been discussed lowering the effec-tiveness of aciclovir to 0% (compatible with an
ineffective intervention) may be a more realisticview of our current knowledge and would pro-
duce effects the same as for the strategies notincluding aciclovir but at an increased cost(the extra cost of the aciclovir).
Will the results help me in caring for mypatients?DO THE PROBABILITY ESTIMATES FIT MYPATIENTS' CLINICAL FEATURES?The answer to this question depends on howwell the clinical characteristics described in thedecision analysis fit the situation of your
patients. Probably the most important consid-eration in this decision analysis is the risk ofsymptomatic recurrences occurring at deliv-ery. This has been assumed in the Randolphmodel to be 14%. Therefore, if you are coun-
selling a woman in clinic who has a recurrence
of her herpes infection once every 2 years it isunlikely that she has a risk of a recurrence atthe time of delivery similar to this and this par-
ticular decision analysis may not help you inmaking a decision about the best way forwardfor this particular patient. If it is likely howeverthat the woman sitting in front of you has a
risk of a recurrence at the time of labour similar
to the population in the model then this deci-sion analysis may be of some help if you feelthat the results are valid.
This baseline risk of 14% has not beenincorporated into the sensitivity analyses andtherefore all your patients must fall into thiscategory in order for this decision analysis tobe of clinical value. It is likely however that thelower the risk of recurrence for a particularwoman the more women will need to betreated to avert one case of neonatal herpesand the more caesarean sections will need tobe undertaken. The threshold at which itbecomes unacceptable to undertake a largenumber of interventions in order to preventone extra case of neonatal herpes has not beenaddressed in this model.
DO THE UTILITIES REFLECT HOW MY PATIENTWOULD VALUE THE OUTCOMES OF THEDECISION?Utility ratings can have a strong influence onthe choice of strategies as patients may preferone outcome much more than another. Thisdecision analysis has not been influenced byutilities. However, it is possible to imaginewhat those utilities may be and to weigh up inone's own mind the relative trade offs betweenthe various outcome including maternal out-comes which were not explicitly considered inthe paper by Randolph et al. This may helpyou in deciding whether this analysis is of usewhen dealing with your patients.
Resolution of the scenarioWithout a good and relevant randomised con-trolled trial of the effectiveness of aciclovir inwomen with recurrent genital herpes infectionyour ability to decide the most effective man-agement for your patient will be limited.Aciclovir is not licensed for use in pregnancyand although no long term side effects havebeen reported with its use the lack of strongdata supporting its effectiveness has to betaken into consideration when assessing theusefulness of this decision analysis.The decision analysis however has been
useful in defining those parts of the clinicalpathway which are important and where morerobust information needs to be obtainedbefore firm recommendations can be given.Until that time, however, the decision analysis,
318 on M
arch 16, 2022 by guest. Protected by copyright.
http://sti.bmj.com
/G
enitourin Med: first published as 10.1136/sti.73.4.314 on 1 A
ugust 1997. Dow
nloaded from

Should aciclovir prophylaxis be used in late pregnancy in women with recurrent genital herpes infection?
by making the process explicit, should havemade you much better informed and betterable to judge how to manage your patients.
Further readingDrummond MF, Stoddart GL, Torrance GW. Methods for the
economic evaluation of health care programmes. Oxford: OxfordMedical Publications, 1987.
Thornton J, Lilford RJ, Johnson N. Decision analysis in medi-cine. BMJ 1992;304:1099-103.
Hopkins HL, ed. Analysing how we reach clinical decisions.London: Royal College of Physicians Publishing, 1993.
1 Randolph AG, Harshorn RM, Washington AE. Acyclovirprophylaxis in late pregnancy to prevent neonatal herpes:a cost-effectiveness analysis. Obstet Gynecol 1996;88:603-10.
2 Richardson WS, Detsky AS. Users guide to the medicalliterature. VII How to use a clinical decision analysis.A. Are the results of the study valid? JAMA 1995;273:1292-5.
3 Richardson WS, Detsky AS. Users guide to the medicalliterature. VII How to use a clinical decision analysis.B. What are the results and will they help me in caring formy patients?J7AMA 1995;273:1610-3.
4 Whitley R, Arvin A, Prober C, Burchett S, Corey L, PowellD, et al. A controlled trial comparing vidarabine with acy-clovir in neonatal herpes simplex virus infection. N Engl J7Med 1991;324:444-9.
5 Brocklehurst P, Camey 0, Ross E, Mindel A. The manage-ment of recurrent genital herpes infection in pregnancy: apostal survey of obstetric practice. Br 7 Obstet Gynaecol1995;102:791-7.
6 Prober CG, Sullender WM, Yasukawa LL, Au DS, ArvinAM. Low risk of herpes simplex virus infections inneonates exposed to the virus at the time of vaginal deliv-ery to mothers with recurrent genital herpes simplex virusinfection. N EnglJ Med 1987;316:240-4.
7 van Everdingen JJE, Peeters MF, ten Have P. Neonatalherpes policy in the Netherlands. Five years after a con-sensus conference. J Perinat Med 1993;21:371 -5.
8 Mercey DE, Mindel A. Preventing neonatal herpes?Genitourin Med 1991;67:1-2.
9 Scott LL, Sanchez PJ, Jackson GL, Zeray F, Wendel GD.Acyclovir suppression to prevent caesarean delivery afterfirst-episode genital herpes. Obstet Gynecol 1996;87:69-73.
10 Brown Z, Vontver LA, Benedetti J, Critchlow CW, SellsCJ, Berry S, et al. Effects on infants of a first episode ofgenital herpes during pregnancy. N Engl _rMed 199 1;317:1246-51.
11 Stephenson JM, Williams IG. Is rifabutin prophylaxisagainst Mycobacterium avium complex infection in HIVinfection worthwhile? The net impact on patients sug-gests not. Genitourin Med 1996;72:272-6.
12 Andrews EB, Yankaskas BC, Cordero JF, Schoeffier K,Hampp S. Acyclovir in pregnancy registry: six years expe-rience. Obstet Gynecol 1992;79:7-13.
13 Chalmers I, Altman DG. Systematic reviews. London: BMJPublishing Group, 1995.
14 Drummond MF, Stoddart GL, Torrance GW. Methods forthe economic evaluation of health care programmes. Oxford:Oxford Medical Publications, 1987.
319 on M
arch 16, 2022 by guest. Protected by copyright.
http://sti.bmj.com
/G
enitourin Med: first published as 10.1136/sti.73.4.314 on 1 A
ugust 1997. Dow
nloaded from














![The effect of Vesicular stomatitis virus and Herpes ... · herpes and keratitis [1, 29, 30, 39-43]. Primary herpetic oral, genital and ocular diseases are Primary herpetic oral, genital](https://img.pdfslide.net/doc/110x75/5e0ec17e158f1d2c96378503/the-effect-of-vesicular-stomatitis-virus-and-herpes-herpes-and-keratitis-1.jpg)