Embed Size (px)
Citation preview
LYNN B. OERTEL, MS, NP‐BC, CACPNURSING PRACTICE SPECIALIST
ANTICOAGULATION MANAGEMENT SERVICEMASSACHUSETTS GENERAL HOSPITAL
THSNA –March 7, 2018, San DiegoNursing Pre‐Summit Workshop 1 – 4pm
Thrombosis and Hemostasis Patient Education: Kernels and Pearls
Developing a management plan to incorporate DOACs into what was a traditional warfarin clinic
Disclosures
Alere
Roche
Pfizer
Challenges at the start….
Gain consensus among stakeholders that this is the ‘right thing’ to do
Identify knowledge gaps and plan staff education and patient education materials
Address technical challenges within clinic and institution
Lack of quality examples for ‘how to do’ this
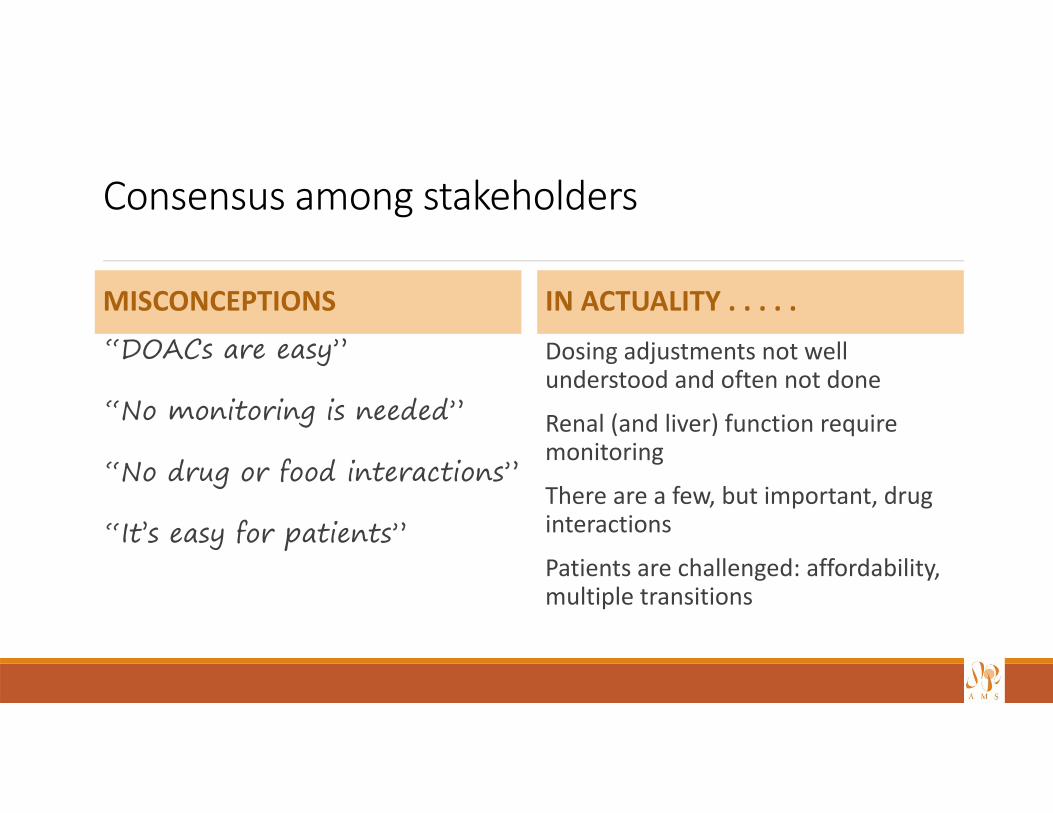
Consensus among stakeholders
MISCONCEPTIONS“DOACs are easy”
“No monitoring is needed”
“No drug or food interactions”
“It’s easy for patients”
IN ACTUALITY . . . . .
Dosing adjustments not well understood and often not done
Renal (and liver) function require monitoring
There are a few, but important, drug interactions
Patients are challenged: affordability, multiple transitions
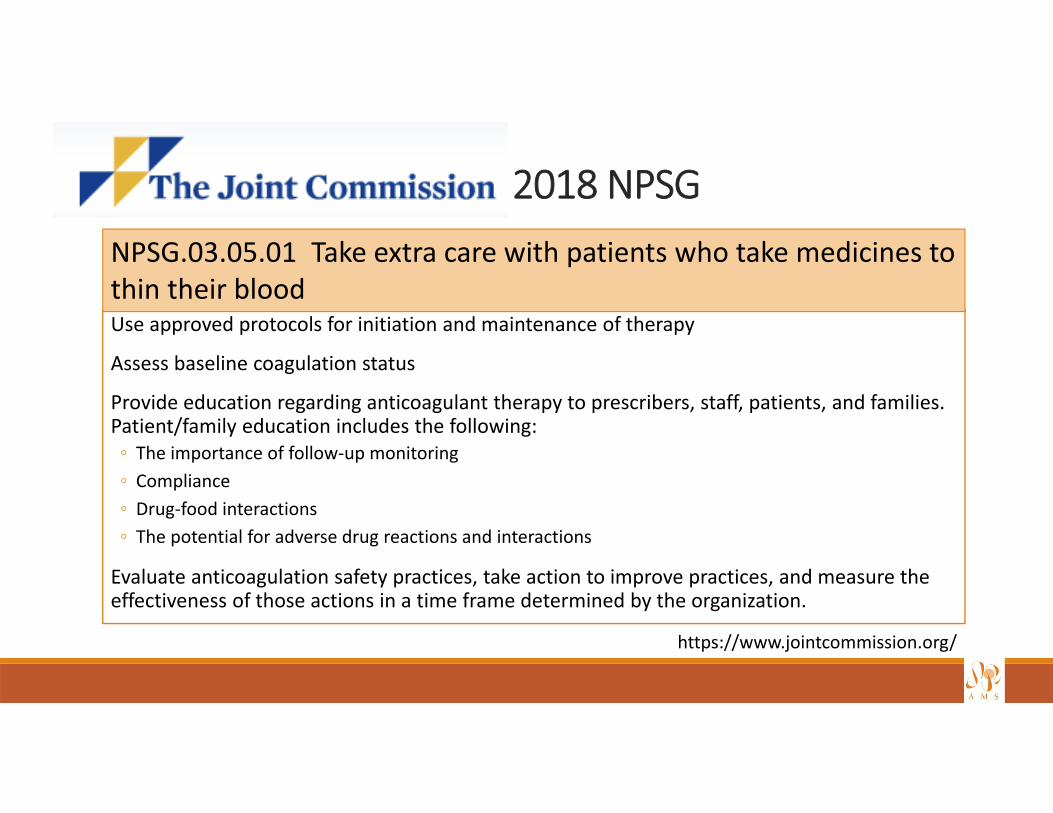
2018 NPSG
Use approved protocols for initiation and maintenance of therapy
Assess baseline coagulation status
Provide education regarding anticoagulant therapy to prescribers, staff, patients, and families. Patient/family education includes the following:◦ The importance of follow‐up monitoring◦ Compliance◦ Drug‐food interactions◦ The potential for adverse drug reactions and interactions
Evaluate anticoagulation safety practices, take action to improve practices, and measure the effectiveness of those actions in a time frame determined by the organization.
https://www.jointcommission.org/
NPSG.03.05.01 Take extra care with patients who take medicines to thin their blood
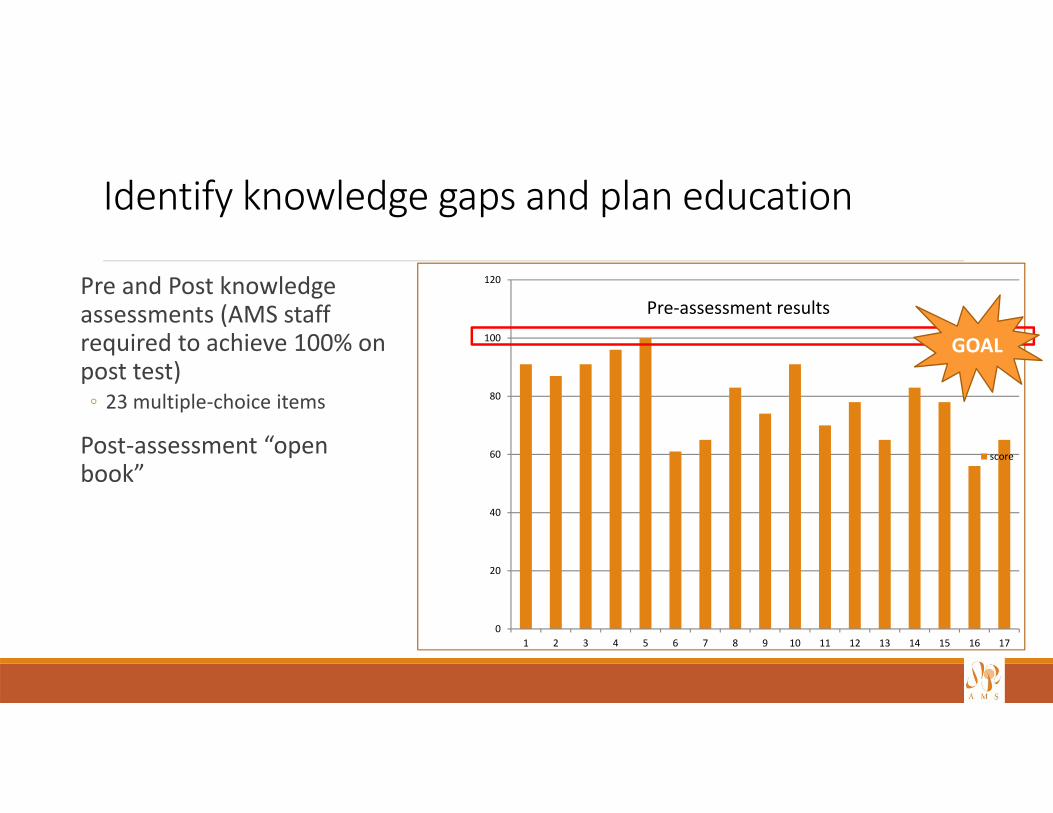
Identify knowledge gaps and plan education
Pre and Post knowledge assessments (AMS staff required to achieve 100% on post test)◦ 23 multiple‐choice items
Post‐assessment “open book”
0
20
40
60
80
100
120
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17
score
Pre‐assessment results
GOAL
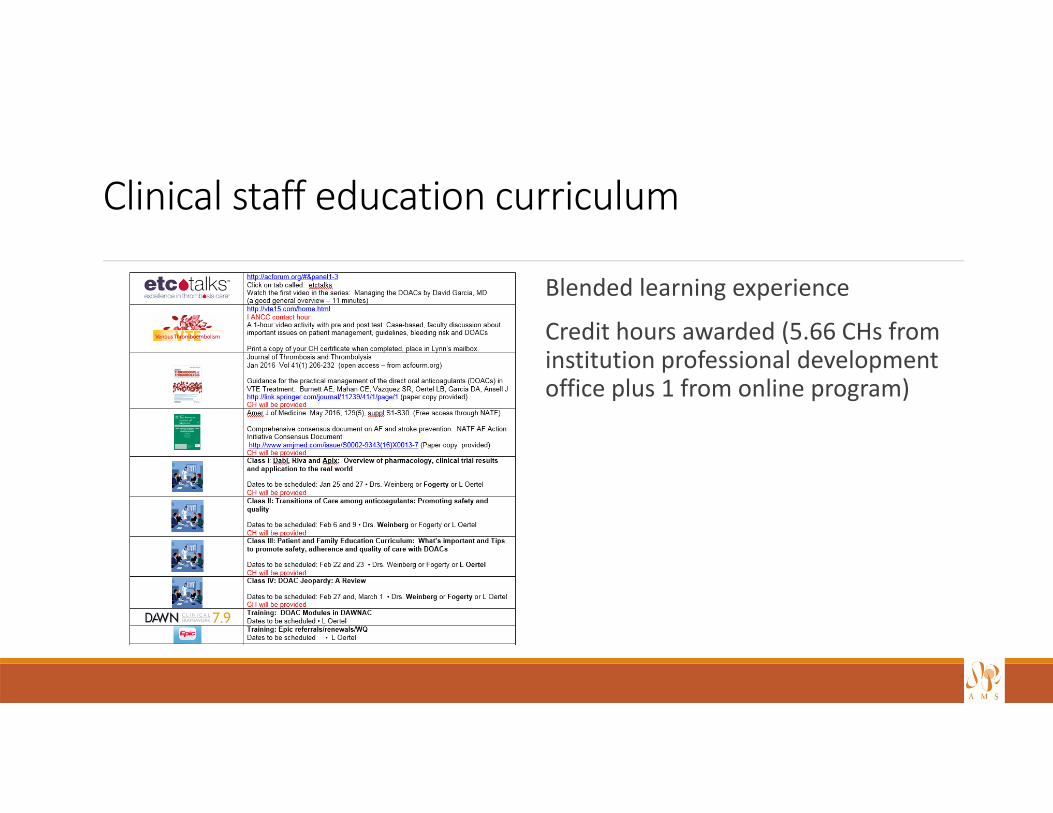
Clinical staff education curriculum
Blended learning experience
Credit hours awarded (5.66 CHs from institution professional development office plus 1 from online program)
Required reading assignments
RUFF CT ET AL. THE AMERICAN JOURNAL OF MEDICINE (2016) 129, S1‐S29
BURNETT AE ET AL. J THROMBTHROMBOLYSIS (2016) 41:206–232
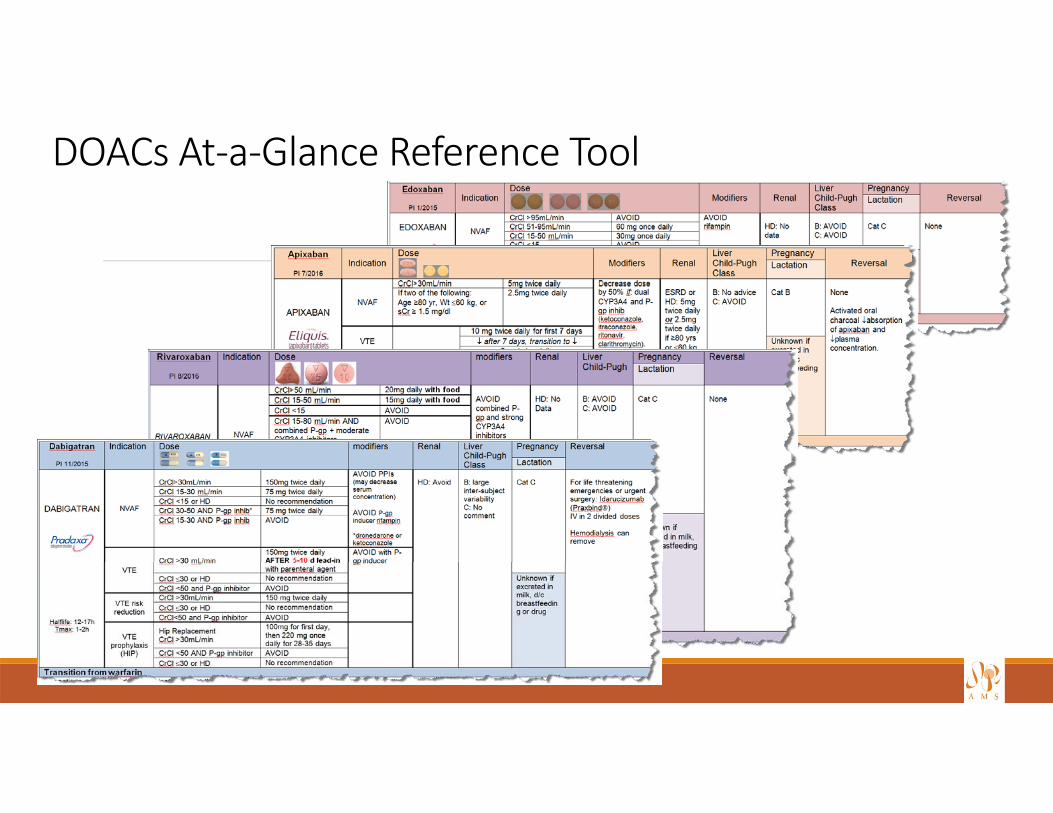
DOACs At‐a‐Glance Reference Tool
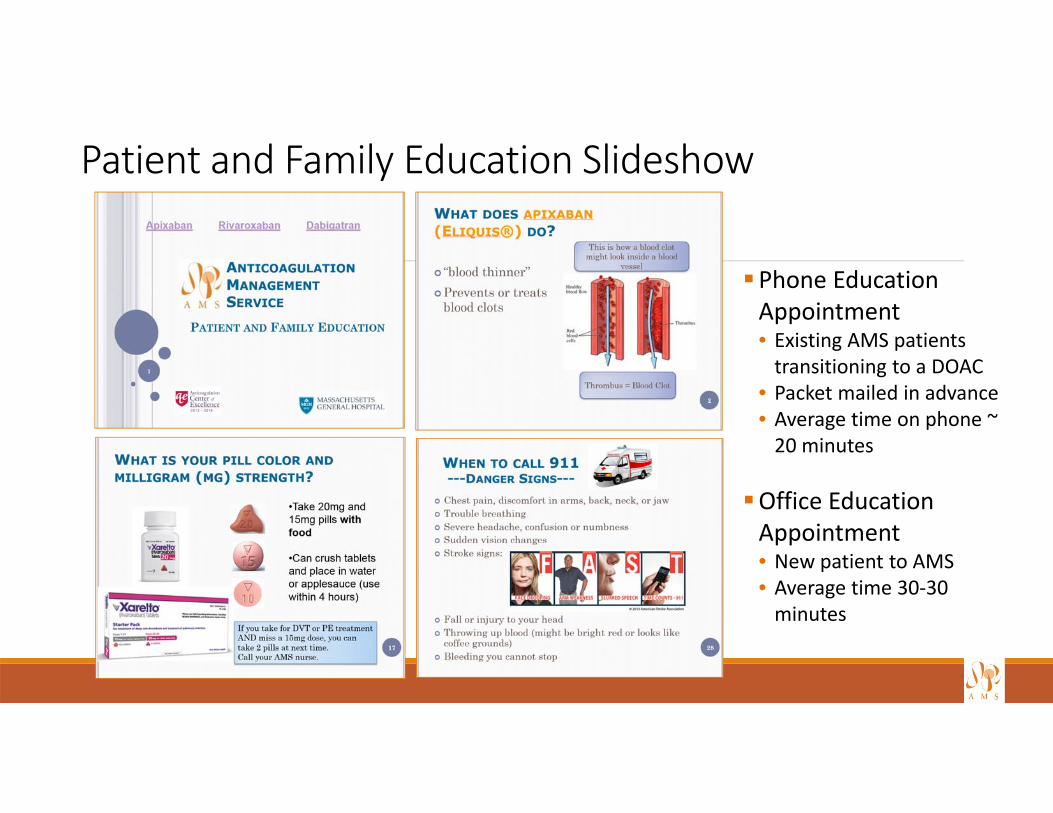
Patient and Family Education Slideshow
Phone Education Appointment• Existing AMS patients transitioning to a DOAC
• Packet mailed in advance• Average time on phone ~ 20 minutes
Office Education Appointment• New patient to AMS• Average time 30‐30 minutes
DOAC Medication Guides – Spanish translations available
Revised existing Patient Agreement to incorporate DOACs
Technical Challenges
Purchase and install DOAC modules for DawnAC®• Staff training
Interfaces with hospital systems• Outbound message from DawnAC® to populate AMS Icon for DOAC patients
Create DOAC referral and renewal order with Epic/Cadence Team• Staff and hospital staff training
Develop strategy to measure and validate work• Patient risk stratification to guide follow‐up and measure workload• Identify value to institution (safety and quality)
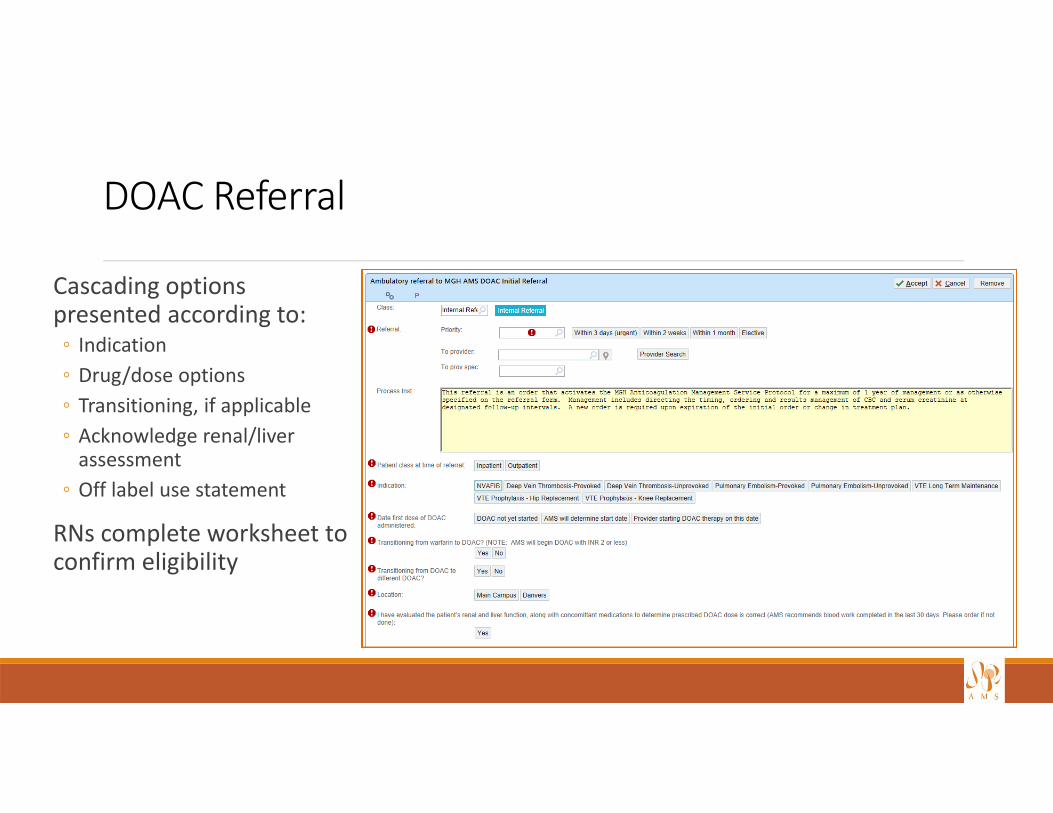
DOAC Referral
Cascading options presented according to:◦ Indication◦ Drug/dose options◦ Transitioning, if applicable◦ Acknowledge renal/liver assessment
◦ Off label use statement
RNs complete worksheet to confirm eligibility
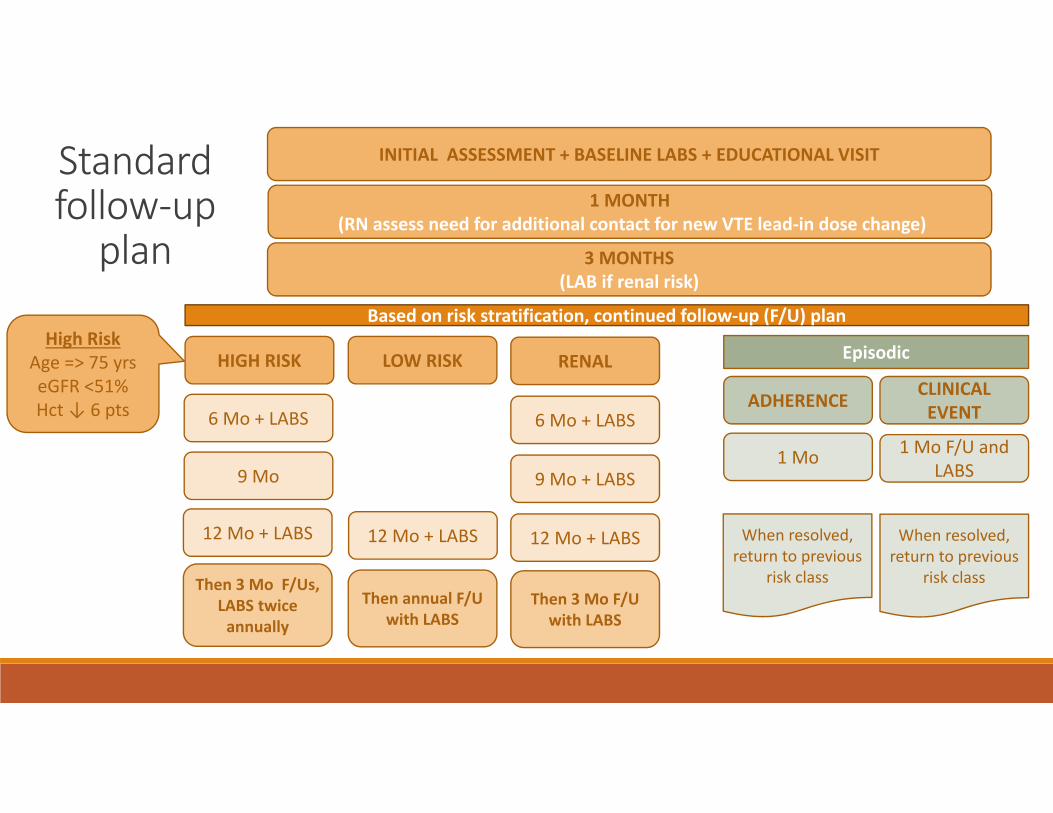
INITIAL ASSESSMENT + BASELINE LABS + EDUCATIONAL VISIT
1 MONTH(RN assess need for additional contact for new VTE lead‐in dose change)
3 MONTHS(LAB if renal risk)
LOW RISK RENAL
ADHERENCE CLINICAL EVENT
HIGH RISK
6 Mo + LABS
9 Mo + LABS
6 Mo + LABS
12 Mo + LABS
Then 3 Mo F/Us, LABS twice annually
12 Mo + LABS
9 Mo
Then annual F/U with LABS
1 Mo 1 Mo F/U and LABS
12 Mo + LABS
Then 3 Mo F/U with LABS
When resolved, return to previous
risk class
When resolved, return to previous
risk class
Based on risk stratification, continued follow‐up (F/U) plan
Standard follow‐upplan
EpisodicHigh Risk
Age => 75 yrseGFR <51%Hct↓ 6 pts
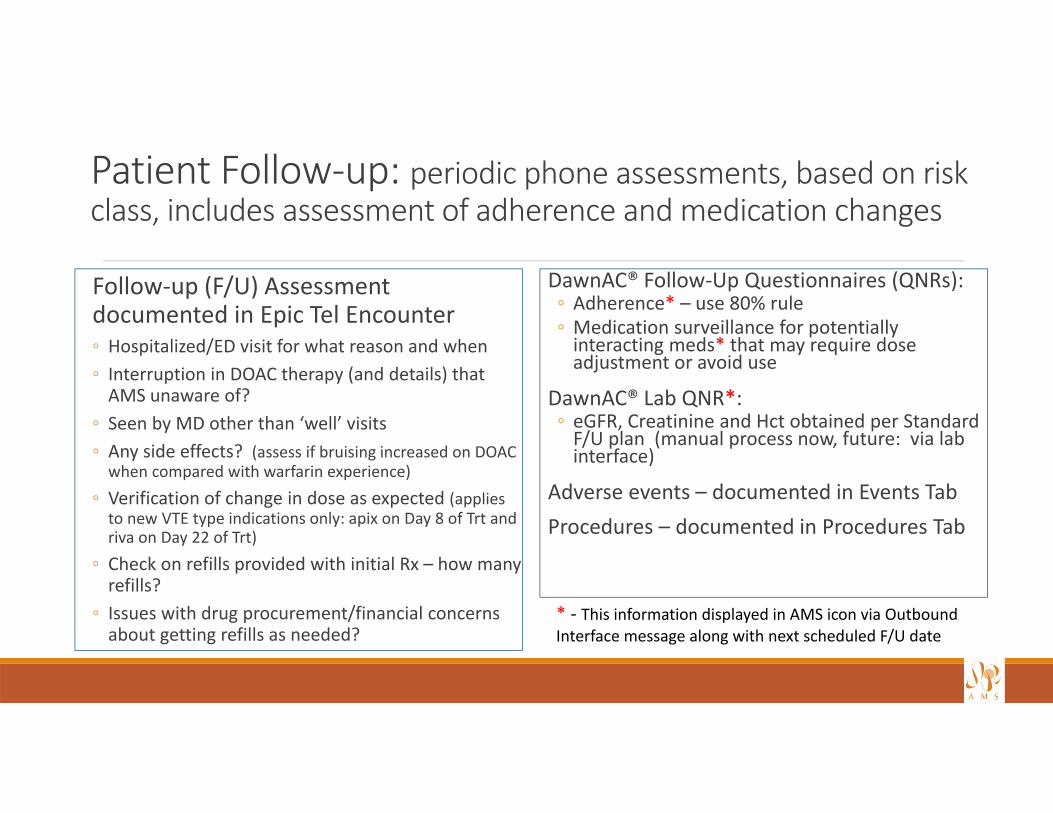
Patient Follow‐up: periodic phone assessments, based on risk class, includes assessment of adherence and medication changes
DawnAC® Follow‐Up Questionnaires (QNRs):◦ Adherence* – use 80% rule◦ Medication surveillance for potentially interacting meds* that may require dose adjustment or avoid use
DawnAC® Lab QNR*:◦ eGFR, Creatinine and Hct obtained per Standard F/U plan (manual process now, future: via lab interface)
Adverse events – documented in Events TabProcedures – documented in Procedures Tab
Follow‐up (F/U) Assessment documented in Epic Tel Encounter ◦ Hospitalized/ED visit for what reason and when◦ Interruption in DOAC therapy (and details) that AMS unaware of?
◦ Seen by MD other than ‘well’ visits◦ Any side effects? (assess if bruising increased on DOAC when compared with warfarin experience)
◦ Verification of change in dose as expected (applies to new VTE type indications only: apix on Day 8 of Trt and riva on Day 22 of Trt)
◦ Check on refills provided with initial Rx – how many refills?
◦ Issues with drug procurement/financial concerns about getting refills as needed?
* ‐ This information displayed in AMS icon via Outbound Interface message along with next scheduled F/U date
How do I assess DOAC adherence?
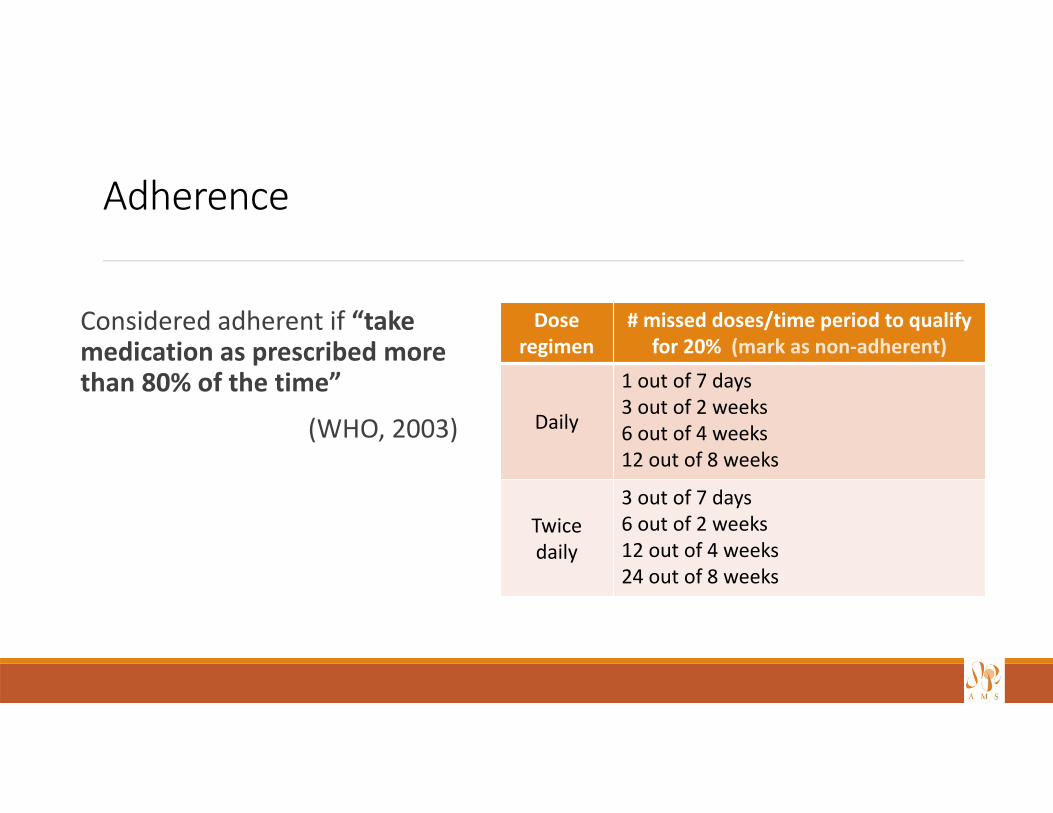
Adherence
Considered adherent if “take medication as prescribed more than 80% of the time”
(WHO, 2003)
Dose regimen
# missed doses/time period to qualifyfor 20% (mark as non‐adherent)
Daily
1 out of 7 days3 out of 2 weeks6 out of 4 weeks12 out of 8 weeks
Twice daily
3 out of 7 days6 out of 2 weeks12 out of 4 weeks24 out of 8 weeks
How to Dose a DOAC . . .
Indication
Age
Renal function
Potential interacting med
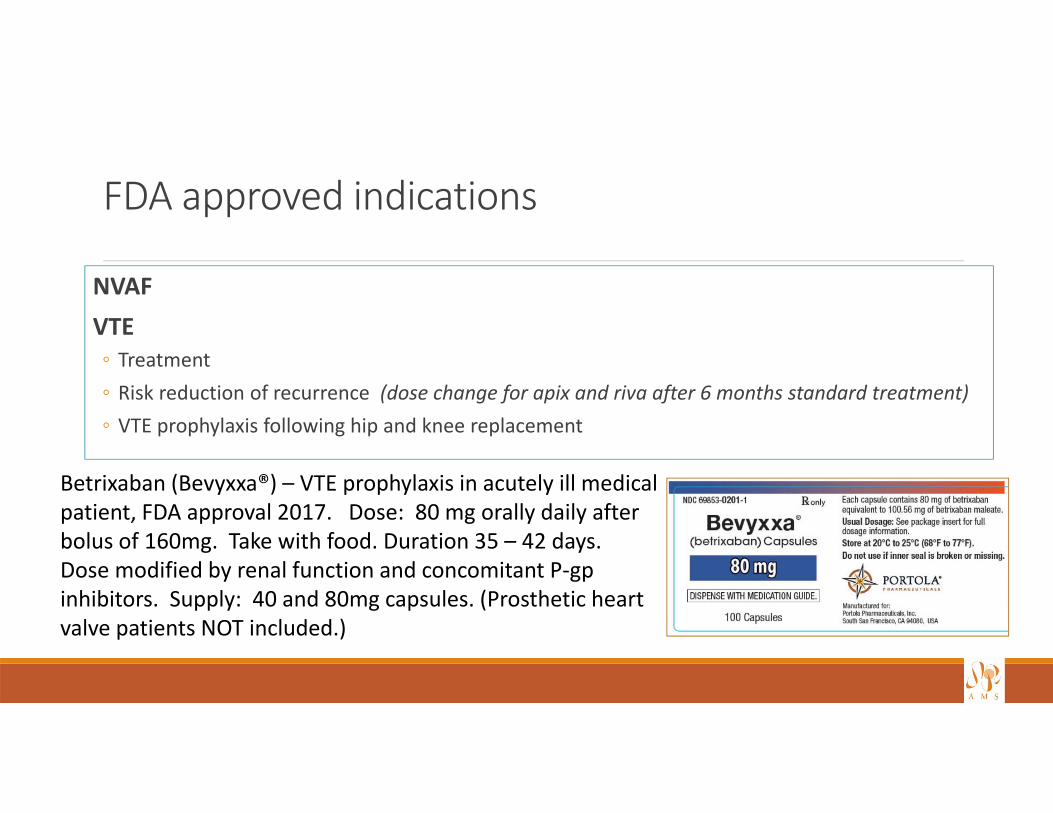
FDA approved indications
NVAFVTE◦ Treatment◦ Risk reduction of recurrence (dose change for apix and riva after 6 months standard treatment)◦ VTE prophylaxis following hip and knee replacement
Betrixaban (Bevyxxa®) – VTE prophylaxis in acutely ill medical patient, FDA approval 2017. Dose: 80 mg orally daily after bolus of 160mg. Take with food. Duration 35 – 42 days. Dose modified by renal function and concomitant P‐gpinhibitors. Supply: 40 and 80mg capsules. (Prosthetic heart valve patients NOT included.)
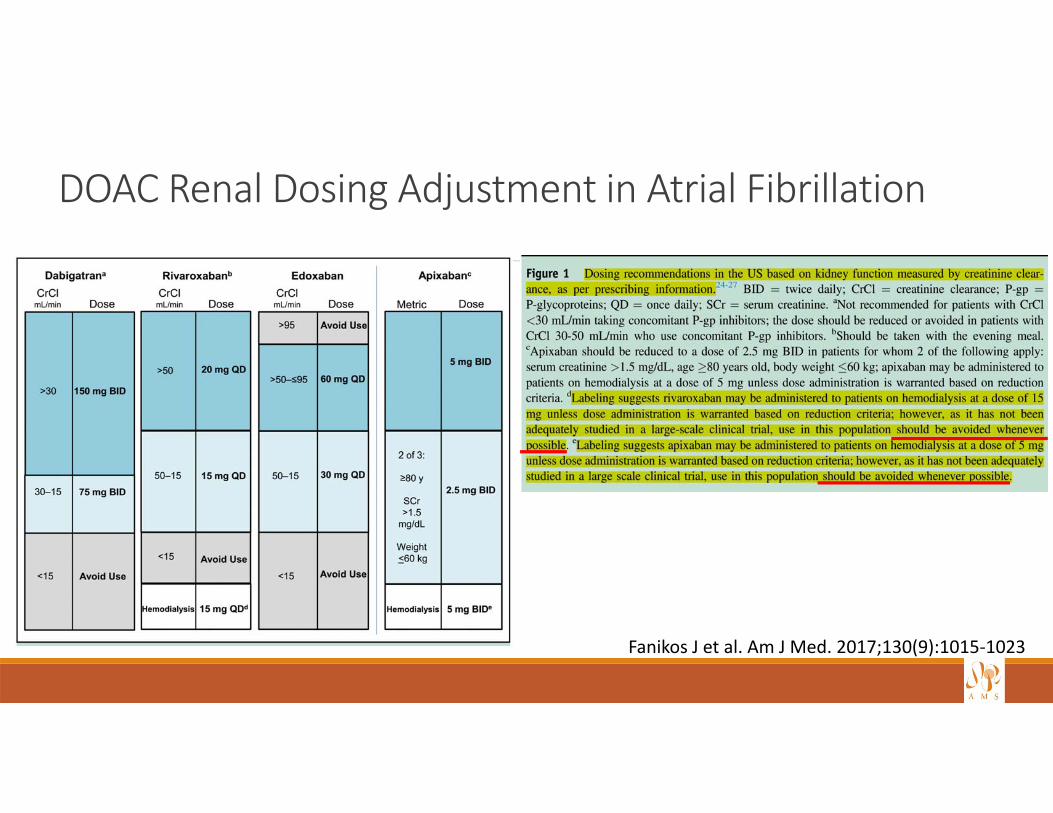
DOAC Renal Dosing Adjustment in Atrial Fibrillation
Fanikos J et al. Am J Med. 2017;130(9):1015‐1023
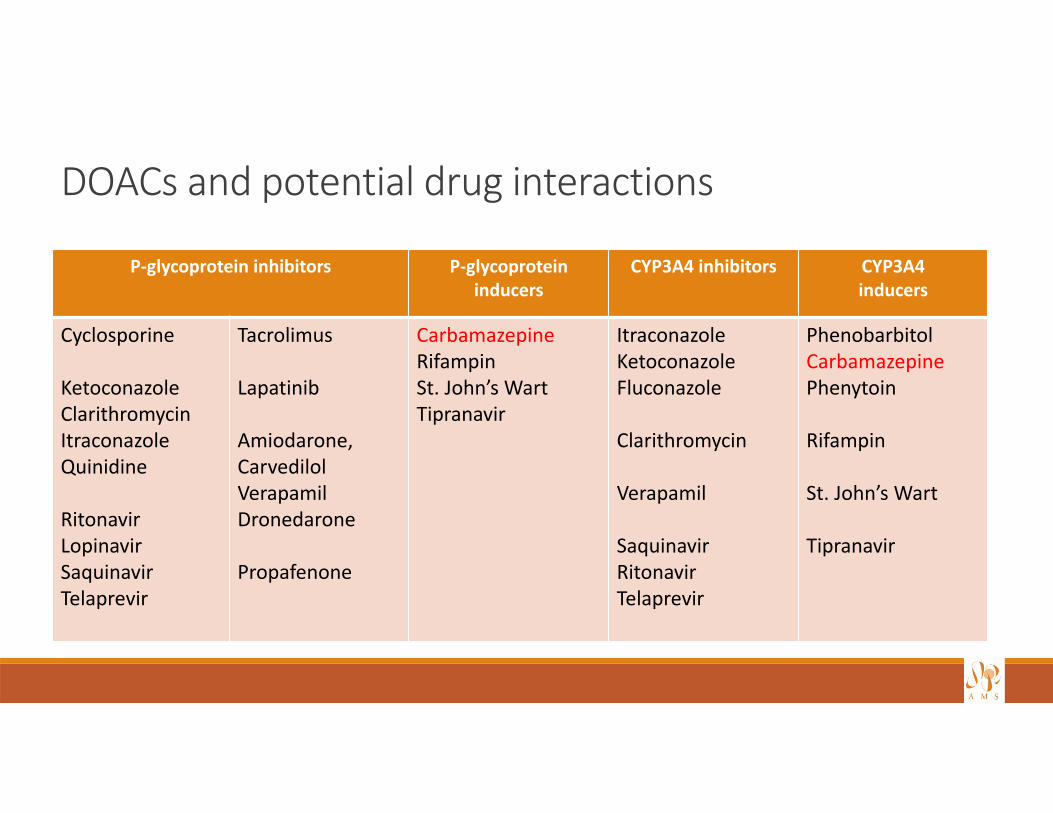
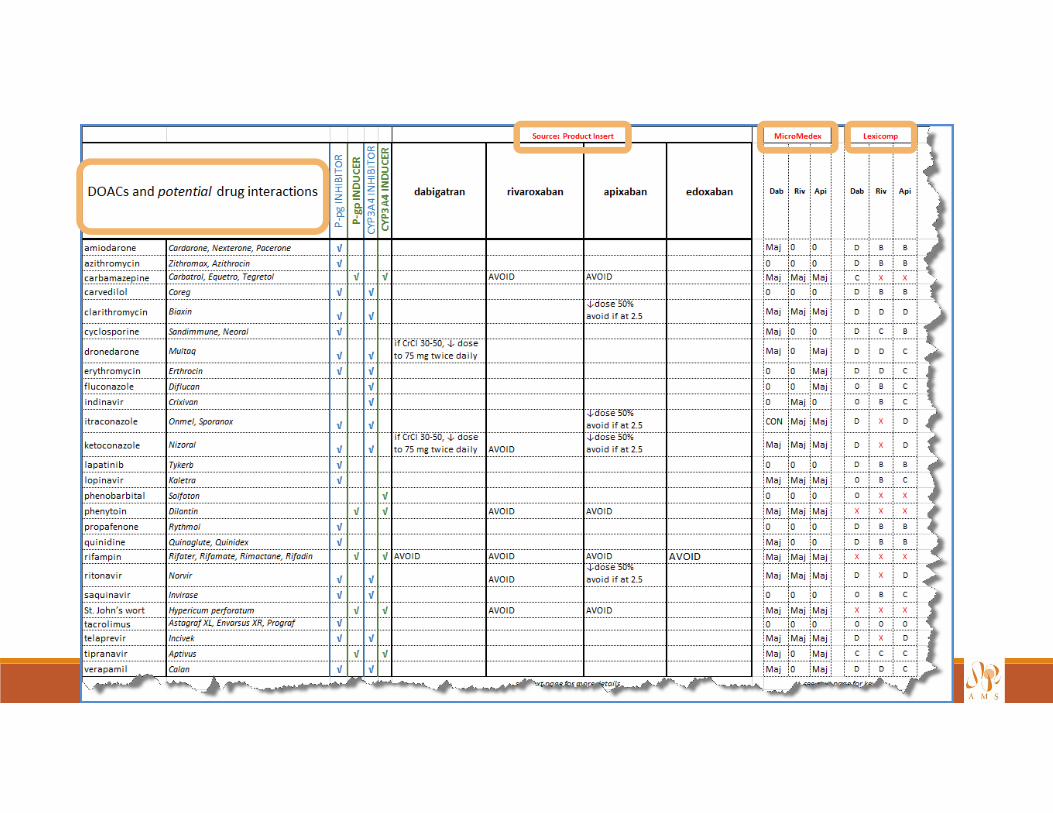
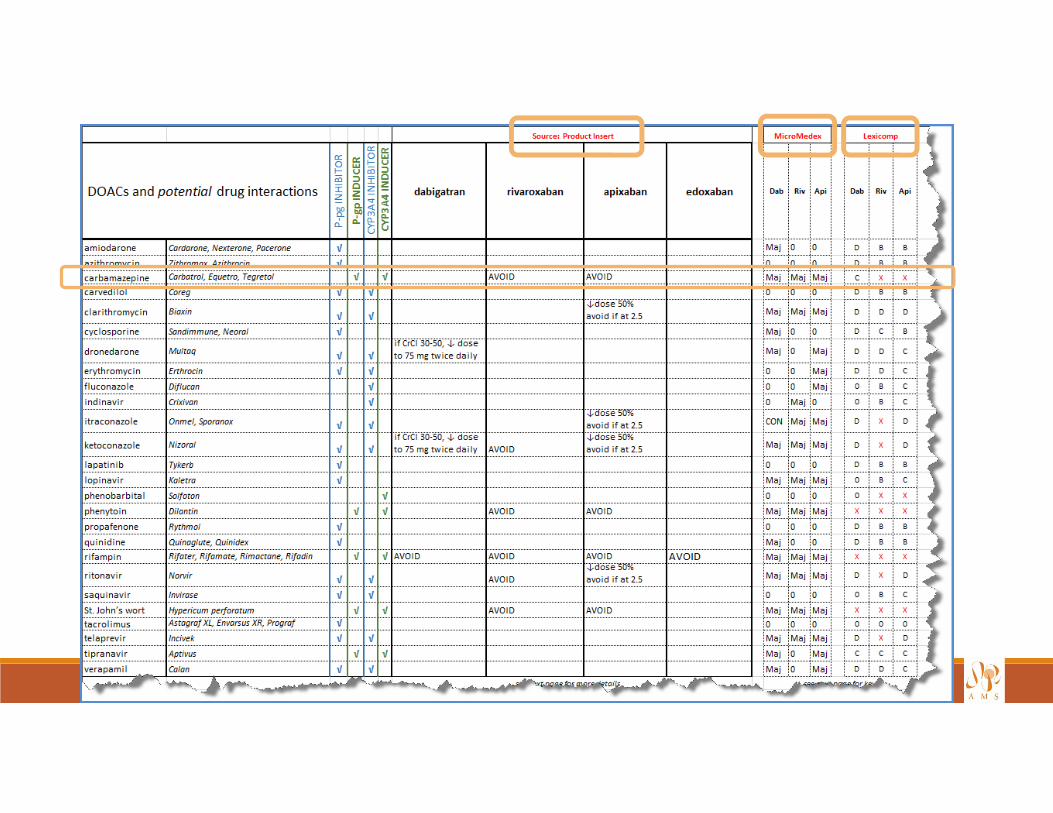
DOACs and potential drug interactions
P‐glycoprotein inhibitors P‐glycoprotein inducers
CYP3A4 inhibitors CYP3A4inducers
Cyclosporine
KetoconazoleClarithromycinItraconazoleQuinidine
RitonavirLopinavirSaquinavirTelaprevir
Tacrolimus
Lapatinib
Amiodarone, CarvedilolVerapamilDronedarone
Propafenone
CarbamazepineRifampinSt. John’s WartTipranavir
ItraconazoleKetoconazole Fluconazole
Clarithromycin
Verapamil
SaquinavirRitonavirTelaprevir
PhenobarbitolCarbamazepinePhenytoin
Rifampin
St. John’s Wart
Tipranavir
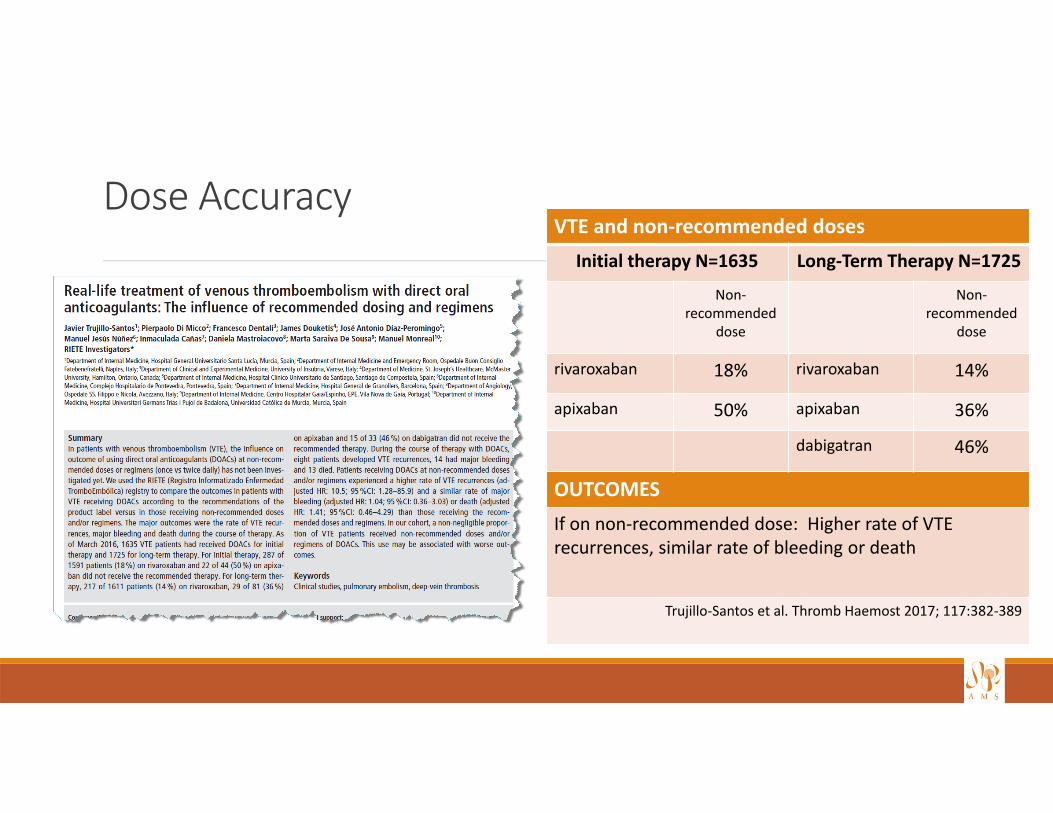
Dose AccuracyVTE and non‐recommended doses
Initial therapy N=1635 Long‐Term Therapy N=1725
Non‐recommended
dose
Non‐recommended
dose
rivaroxaban 18% rivaroxaban 14%
apixaban 50% apixaban 36%
dabigatran 46%
OUTCOMESIf on non‐recommended dose: Higher rate of VTE recurrences, similar rate of bleeding or death
Trujillo‐Santos et al. Thromb Haemost 2017; 117:382‐389
Temporary interruptions in therapy
Approx. 10% of VTE patients needed a temporary interruption annually
Surgical or other invasive procedures were required in:◦ 25% of patients in RE‐LY◦ 33% of patients in ROCKET AF and ARISTOTLE
Burnett AE, et al. J Thromb Thrombolysis 2016; 41:206‐232Lip GYH, et al. Up‐to‐date
Bleeding risk
Thrombotic risk
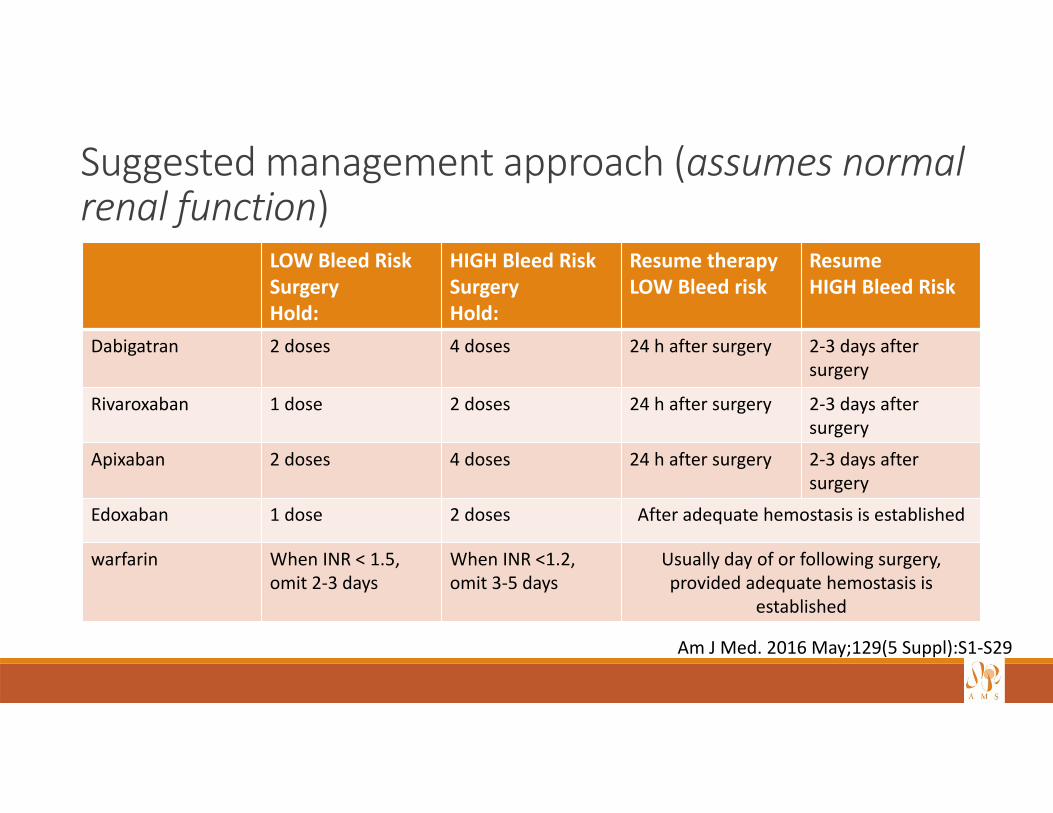
Suggested management approach (assumes normal renal function)
LOW Bleed Risk SurgeryHold:
HIGH Bleed RiskSurgeryHold:
Resume therapyLOW Bleed risk
Resume HIGH Bleed Risk
Dabigatran 2 doses 4 doses 24 h after surgery 2‐3 days after surgery
Rivaroxaban 1 dose 2 doses 24 h after surgery 2‐3 days after surgery
Apixaban 2 doses 4 doses 24 h after surgery 2‐3 days after surgery
Edoxaban 1 dose 2 doses After adequate hemostasis is established
warfarin When INR < 1.5,omit 2‐3 days
When INR <1.2, omit 3‐5 days
Usually day of or following surgery, provided adequate hemostasis is
established
Am J Med. 2016 May;129(5 Suppl):S1‐S29
Transitions among oral anticoagulants: not an infrequent patient experienceRecent real‐world evidence on medication switching patterns in anticoagulant‐naïve NVAF patients (N=34,022, Commercial and Medicare claims database):◦ 1 in 5 patients switched from their index DOAC to alternate◦ Older patients switched more than younger◦ Females switched more than males
Of those that switched:◦ 29% switched once◦ 70% switched more than twice◦ 45% switched to warfarin, 44% to another DOAC
Manzoor BS et al. J Thromb Thrombolysis (2017) 44:435‐441
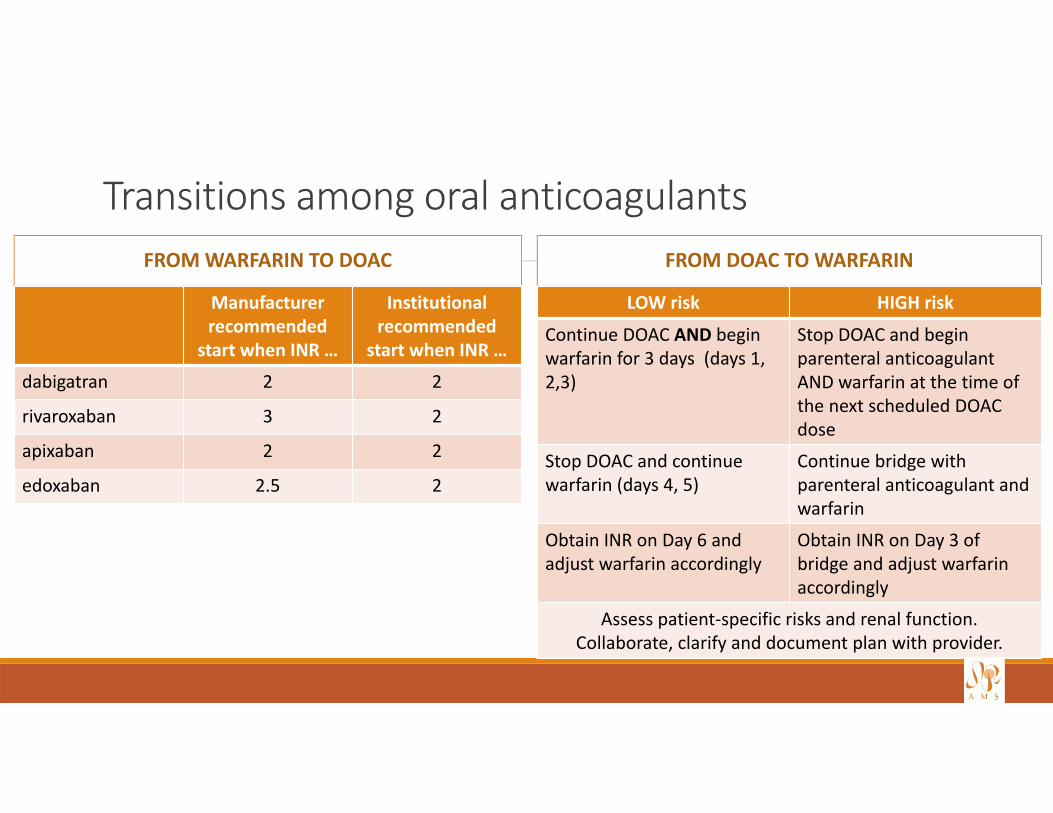
Transitions among oral anticoagulantsFROM WARFARIN TO DOAC
Manufacturerrecommended
start when INR …
Institutional recommended
start when INR …
dabigatran 2 2
rivaroxaban 3 2
apixaban 2 2
edoxaban 2.5 2
FROM DOAC TO WARFARIN
LOW risk HIGH risk
Continue DOAC AND begin warfarin for 3 days (days 1, 2,3)
Stop DOAC and begin parenteral anticoagulant AND warfarin at the time of the next scheduled DOAC dose
Stop DOAC and continue warfarin (days 4, 5)
Continue bridge with parenteral anticoagulant and warfarin
Obtain INR on Day 6 and adjust warfarin accordingly
Obtain INR on Day 3 of bridge and adjust warfarin accordingly
Assess patient‐specific risks and renal function. Collaborate, clarify and document plan with provider.
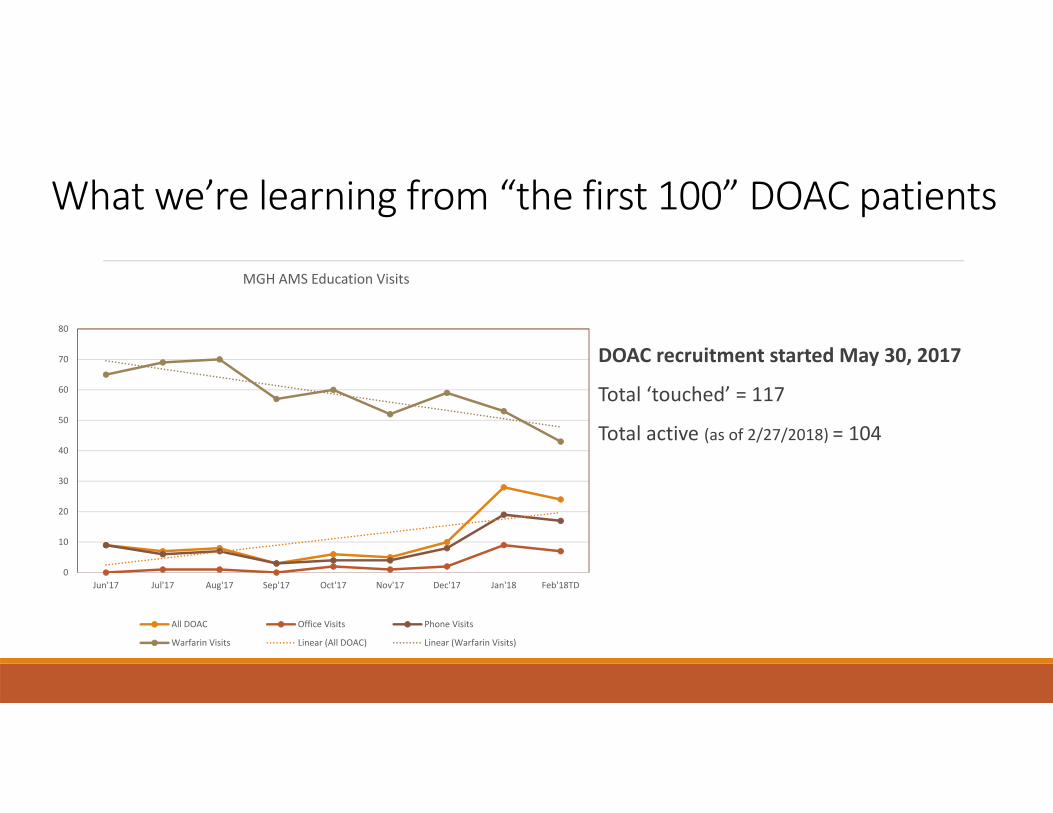
What we’re learning from “the first 100” DOAC patients
0
10
20
30
40
50
60
70
80
Jun'17 Jul'17 Aug'17 Sep'17 Oct'17 Nov'17 Dec'17 Jan'18 Feb'18TD
MGH AMS Education Visits
All DOAC Office Visits Phone Visits
Warfarin Visits Linear (All DOAC) Linear (Warfarin Visits)
DOAC recruitment started May 30, 2017
Total ‘touched’ = 117
Total active (as of 2/27/2018) = 104
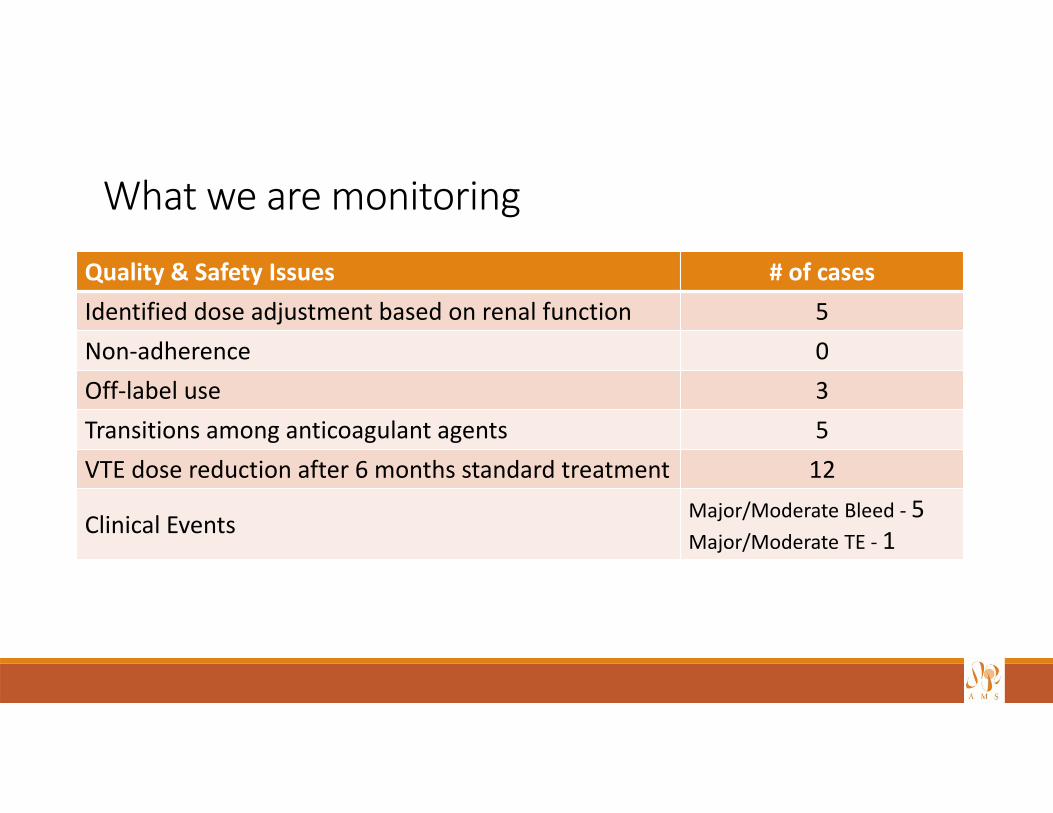
What we are monitoring
Quality & Safety Issues # of casesIdentified dose adjustment based on renal function 5Non‐adherence 0Off‐label use 3Transitions among anticoagulant agents 5VTE dose reduction after 6 months standard treatment 12
Clinical Events Major/Moderate Bleed ‐ 5Major/Moderate TE ‐ 1
Patients in need of help
More than 20 stand alone drug plans offered in MA under Medicare Part D
Free help at SHINE‐ Serving the Health Insurance Needs of Everyone (on Medicare)
SHINE saved 62,000 MA residents $105 million last year. Visit: mass.gov/health‐insurance‐counseling
Other resources:
Medicare.gov
GoodRx.com
Retail pharmacists can print Medicare Plan Finder for patients – compares plans, costs and coverage
Boston Globe Nov 11, 2017
Disseminate information
Google: mgh eedhttp://www.mghpcs.org/eed_portal/
Summary
Educate
Communicate
Evaluate
Modify