Embed Size (px)
Citation preview

Elizabeth Roquemore*, Rahman Ismail, Sharon Davies, Catherine Hather, Elizabeth Price, Alexander Harrison+, P J Kemp+, N D Allen+ and Stephen Minger GE Healthcare, Amersham Place, Little Chalfont, Buckinghamshire, England, UK HP7 9NA. Tel: +44 (0)29 2052 6499; Fax: +44 (0)29 2052 6230
*e-mail: [email protected]. + Cardiff School of Biosciences, Biomedical Sciences Building, Museum Avenue, Cardiff, CF10 3AX
HIGH CONTENT CYTOTOXICITY APPLICATION
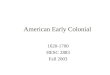
HCA toxicity assays The well-characterized GE Healthcare cardiomyocytes comprise a physiologically relevant and robust model for cardiotoxicity testing. In live multiplexed cytotoxicity assays, four fluorescent probes were used to report on the status of nuclei, cytosolic free calcium, mitochondria, and plasma membrane integrity (Figures 6 and 7).
Figure 6. Images of Cardiomyocytes from a live multiplexed cytotoxicity assay. Fluorescent probes report cytotoxic changes in cell and organelle status. Cardiomyocytes were incubated for 24h in the absence (left) or presence (right) of 3.7µM amiodarone, and then imaged live after probe addition (40X/0.6NA).
Dose-response plots (Figure 7) indicate marked differences in the pharmacodynamic effects of doxorubicin and amiodarone. Such differences are more readily apparent when using fluorescent probes in combination, rather than individually in separate assays.
Figure 7. Pharmacodyamic responses differ for doxorubicin and amiodarone.
A large number of measurements can be extracted on a cell-by-cell basis for each fluorescent probe used in the assay. Hierarchical cluster analysis based on a sub-set of extracted parameters (Figure 8) shows that different compounds induce characteristic multi-parametric signatures that may be informative in predictive toxicity assessments.
Figure 8. Hierarchical multi-parametric clustering of compound effects.
Two-dimensional scatter plots are helpful in exploring relationships between parameters. For example, Figure 9 reveals a correlation between mitochondrial area and nuclear area in cells treated with doxorubicin and amiodarone.
Figure 9. Scatter-plot visualization of parameter relationships. Both mitochondrial area and nuclear area decrease in cells treated with doxorubicin, amiodarone or antimycin A, but not in cells treated with the less accutely toxic compounds, zidovudine, diclofenac and nifedipine.
ABSTRACT Failure to detect cardiotoxic side effects of new drugs before clinical launch has had a significant impact on the pharmaceutical industry, patients and regulators—lengthening time to market, raising costs, and increasing the risk that a drug will be withdrawn due to unanticipated safety issues. Cardiac toxicity assays and screens are often reliant on the use of animal models or highly proliferative immmortalized cell lines. While these models can be less costly, renewable and more tractable than primary cells and tissues, they do not always accurately predict human responses. As a result, there is an increasing demand for more relevant and predictive in vitro screening models for cardiotoxicity testing. Human embryonic stem cells have the potential to serve as an abundant and reliable source of cardiomyocytes. We have developed a robust process for generation of differentiated spontaneously contracting cardiomyocytes from human embryonic stem cells (hESC). We present results demonstrating their functional and phenotypic characterization, and their configuration for use in in vitro safety and toxicity testing.
METHODS
Cardiomyocyte production To produce differentiated cardiomyocytes, hESCs (H7 cell line) were cultivated and expanded under feeder-free conditions, and then subjected to a controlled differentiation process (Figure 1). Briefly, hESCs were adapted to alternative growth conditions, subjected to a proprietary growth factor regime, and then matured. At the end of the process, cells were harvested and cryopreserved at 105-106 cardiomyocytes per vial. All vials were stored at -140oC until use. Cryopreserved cardiomyocytes were the starting material for all experimental methods described below.
Figure 1. Cardiomyocyte differentiation process. Electrophysiological characterization of Cardiomyocytes Cardiomyoctes were seeded onto MatrigelTM (BD Biosciences)-coated glass coverslips and maintained in culture for 96 hours before use. Cellular activity was recorded by whole cell patch clamping, employing standard electrophysiological solutions. For investigation of spontaneous activity, voltages were recorded in current-clamp mode with zero current injection. For induced action potential studies, variable depolarizing current pulses (500-2000 pA, 10 ms) were applied to stimulate a single induced action potential. For voltage ramp studies, cells were voltage clamped at -70 mV, stepped to -120 mV and ramped up to +60 mV over 50 ms. The recorded current was leak-subtracted and plotted against the voltage to give the current-voltage relationship. For calcium imaging, cells were incubated in the presence of 2 µM Fluo-3-AM for 20 minutes at 37OC. Cells were excited at 488 nm and the emission intensity was measured at 505 nm, after which all signals were background subtracted. In all studies, and where indicated, ion channel blockers were applied directly to cells using a gravity-fed rapid solution system with between 20 and 100ms solution switch times. Immunocytochemistry for Flow Cytometry Cells were fixed with 2% paraformaldehyde and permeabilized with Perm/Wash buffer (BD Biosciences). Primary antibodies were added to each tube and incubated for 1hr at 40C before addition of fluor-conjugated secondary antibody for a further 1hr at 40C. Labeled cells were analyzed using a BD FACSCaliburTM flow cytometer (BD Biosciences). Immunocytochemistry for IN Cell Analyzer 2000 Image Acquisition
Cardiomyocytes were seeded onto Matrigel-coated 96-well µClear
plates (Greiner), and incubated at 370C for 48 hours. Medium was refreshed on alternate days thereafter. Cells were fixed for immunocytochemistry with 2% paraformaldehyde, and then blocked with 5% serum /1% human IgG for 20mins at 4oC. Primary antibodies were added to each well and incubated for 1hr at 40C before addition of fluor-conjugated secondary antibodies for a further 1hr at 40C, followed by washing. Cell nuclei were labeled with Hoechst 33342 (Invitrogen). Live multiplexed cytotoxicity assays Cells were seeded into Matrigel-coated 96-well µClear plates, and incubated at 37oC for 48h. After this time, the medium was replaced, compound was added, and the incubation was continued for a further 24-72h. Prior to live imaging, cells were incubated for 1h at 37oC in the presence of Hoechst 33342, Fluo-4 AM, Mitotracker® Red CMXRos or TMRM, and TOTO®-3 iodide (all from Invitrogen). Image Acquisition Images were acquired with an IN Cell Analyzer 2000 high content imaging system (GE Healthcare) configured with the standard size CCD camera option. Images were acquired using the 20x/0.45NA or 40x/0.6NA objective. Analysis protcols were developed with IN Cell InvestigatorTM software (GE Healthcare), which provides a link to the Spotfire® DecisionSite visualization tools used to generate heat maps and scatter plots.
D
H
100x 0.9NA, 3D-Dcon
P
40x/0.6NA, 2D-Decon
40x/0.6NA, 2D-Decon
CARDIOMYOCYTE CHARACTERIZATION
Cytometric Characterization Throughout the development process, both flow cytometry and high content image analysis were used to assess cardiomyocyte phenotype (Figures 2 and 3).
A B
Figure 2. Examples GE Healthcare Cardiomyocyte cytometric characterization. A) Flow cytometry plot of cardiac troponin I fluorescence intensity versus forward scatter in cardiomyocytes recovered from cryopreserved stocks; B) High content analysis scatter plot, with thresholds applied to classify each cell into one
of four sub-populations based on staining intensities of α-Actinin and GATA-4.
When resurrected from cryopreservation, the differentiated cardiomyocytes adhere in monolayers with an efficiency of greater than 50% (data not shown). After growth in culture for several days, the cells develop a rhythmic contractile phenotype. Immunocytochemistry at this stage (Figure 3) demonstrates cardiomyocyte-specific expression and correct localization of cardiac-related transcription factors and structural proteins.
Figure 3. Cardiac-related markers are expressed and correctly localized. Staining and imaging as in Methods. Font color indicates immunofluorescence channel for the respective marker. For Mef 2C, Nkx 2.5, Gata 4 and Connexin 43 imaging, cells were counterstained for Troponin I (red).
Electrophysiological Characterisation Whole cell current-clamp recording (Figure 4A) and calcium imaging (Figure 4B) demonstrate spontaneous activity that can be reversibly inhibited by the L-type Ca2+ channel blocker nifedipine. Complete block of spontaneous activity by nifedipine suggests that L-type Ca2+ channels are responsible for induction of the action potential.
Figure 4. GE Healthcare Cardiomyocytes show pacemaker activity. A) Whole cell current-clamp recording shows repeatable 10µM nifedipine inhibition of spontaneous action potentials followed by wash off and restoration of spontaneous activity; B) Fluo-3 calcium imaging demonstrates spontaneous cytosolic calcium increase via nifedipine-sensitive Ca2+ influx.
Depolarizing current pulses evoke action potentials in cells current-clamped at 0 picoAmps in the whole-cell patch clamp configuration. Examples of ventricular myocyte activity are shown in Figure 5.
Figure 5. Examples of ventricular myocyte activity. A) Inducible action potentials are lengthened by a TEA block of K+ channels, and are slightly reduced by TTX; B) 100 µM bupivicaine and 1 µM nifedipine reduce induced action potential length; C) Voltage ramp evokes whole cell currents. Activation of Na+ channels is apparent; the peak of this current is reduced dramatically by 100 µM bupivicaine, and less so by 100 nM TTX.
Conclusions
hESC-Derived cardiomyocytes have the potential to provide an unlimited supply of human cardiomyocyte-like cells for use in drug discovery and safety screening.
Flow cytometry and high content imaging confirm that GE Healthcare cardiomyocytes express and correctly localize key cardiac-related markers.
Electrophysiological studies demonstrate that the cardiomyocytes exhibit a range of ion channel activities with appropriate biological responses.
The cardiomyocytes provide a physiologically relevant model system for high content cardiotoxicity testing in a live, multiplexed, high-throughput format.
IN Cell Analyer 2000 high content analysis system and IN Cell Investigator software provide a comprehensive solution for imaging and analyzing toxicity screens employing hESC-derived cardiomyocytes.
Development of hESC-Derived Cardiomyocytes
as models for in vitro toxicity testing
GE, imagination at work, and GE Monogram are trademarks of General Electric Company. All third party trademarks are the property of their respective owners. The IN Cell Analyzer 2000 and associated analysis modules are sold under use licenses from Cellomics Inc. under US patent numbers US 5989835, 6416959, 6573039, 6620591, 6671624, 6716588, 6727071, 6759206, 6875578, 6902883, 6917884, 6970789, 6986993, 7060445, 7085765, 7117098; Canadian patent numbers CA 2282658, 2328194, 2362117, 2381334; Australian patent number AU 730100; European patent numbers EP 0983498, 1095277, 1155304, 1203214, 1348124, 1368689; Japanese patent numbers JP 3466568, 3576491, 3683591 and equivalent patents and patent applications in other countries. GE Healthcare Cardiomyocytes are sold under licence from Geron Corporation and Wisconsin Alumni Research Foundation under US patent and publication numbers: US 7,425,448, US 2009/0017465, US 6,800,480, US 5,843,780, US 6,200,806, US 7,029,913, US 7,582,479, US 7,413,902; US 7,297,539, US 2009/0047739 and US 2007/0010012 and equivalent patent and patent applications in other countries. © 2010 General Electric Company – All rights reserved. All goods and services are sold subject to terms and conditions of sale of the GE Healthcare Company which supplies them. A copy of these terms and conditions are available on request. Contact your GE Healthcare representative for the most current information and a copy of the terms and conditions. GE Healthcare Bio-Sciences AB Bjorkgatan 30 SE-751 84 Uppsala Sweden. This poster was presented at the 3rd Annual UK National Stem Cell Network Conference, Nottingham, UK, July 11-14, 2010. *To whom all correspondence should be addressed.