Embed Size (px)
DESCRIPTION
Diagnosis Related Groups and AR-DRGs - Introduction. Prof Ric Marshall OAM The University of Sydney. QUESTIONS. When asked to use DRGs people want to know. What are DRGs? What are DRGs useful for? People wanting to use DRGs usually have some purpose in mind. How can DRGs help us to … ? - PowerPoint PPT Presentation
Citation preview
DRG Workshop Belgrade, 18-22.November 2013.
Diagnosis Related Groups and AR-DRGs - Introduction
Prof Ric Marshall OAMThe University of Sydney.
DRG Workshop Belgrade, 18-22.November 2013.
QUESTIONS• When asked to use DRGs people want to
know.– What are DRGs?– What are DRGs useful for?
• People wanting to use DRGs usually have some purpose in mind.– How can DRGs help us to … ?
• What people who use them want to know about how they work – their limitations.
DRG Workshop Belgrade, 18-22.November 2013.
Paying for health services based on activity rather than expenditure
The usual context:-
DRG Workshop Belgrade, 18-22.November 2013.
WHY DRG’S?
• IF USED EFFECTIVELY AS A FUNDING TOOL– DRG’s help to focus on hospital efficiency and
quality.– DRG’s help to contain growth in hospital costs.
• THE DRG IS JUST THE TOOL NOT THE POLICY
DRG Workshop Belgrade, 18-22.November 2013.
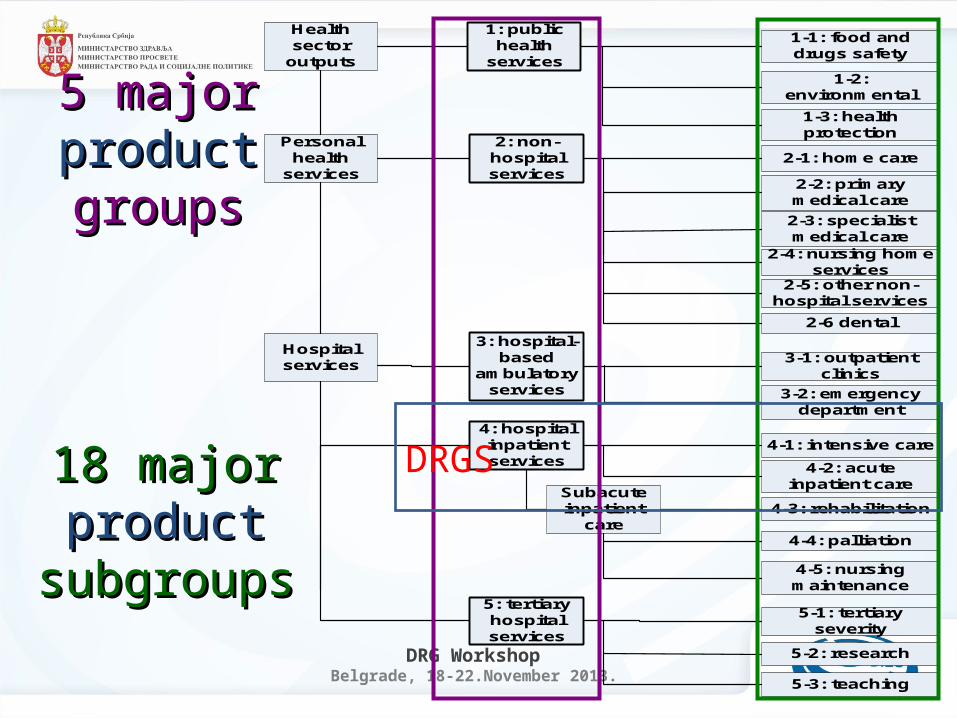
Health sector
outputs
Hospital services
Personal health
services
1: public health
services
5: tertiary hospital services
4: hospital inpatient services
3: hospital-based
ambulatory services
2: non-hospital services
2-1: home care
5-1: tertiary severity
5-3: teaching
5-2: research
4-5: nursing maintenance
4-4: palliation
4-3: rehabilitation
4-2: acute inpatient care
4-1: intensive care
3-2: emergency department
1-1: food and drugs safety
1-2: environmental
1-3: health protection
3-1: outpatient clinics
2-6 dental
2-5: other non-hospital services
2-4: nursing home services
2-3: specialist medical care
2-2: primary medical care
Subacute inpatient
care
5 major 5 major productproduct groupsgroups
18 major 18 major product product
subgroupssubgroups
DRGS
DRG Workshop Belgrade, 18-22.November 2013.
Hospital Inpatient Care
• Goals, incentives– efficient use of available resources such as
same day surgery– close integration with non-acute care settings
to support early discharge and effective post discharge care
– good health outcomes and minimisation of adverse events
– optimisation of patient convenience
• Episode focus – eg DRGs
DRG Workshop Belgrade, 18-22.November 2013.
THE 4 Components of a drg funding system
What is needed to fund a hospital system by DRG payments???
DRG Workshop Belgrade, 18-22.November 2013.
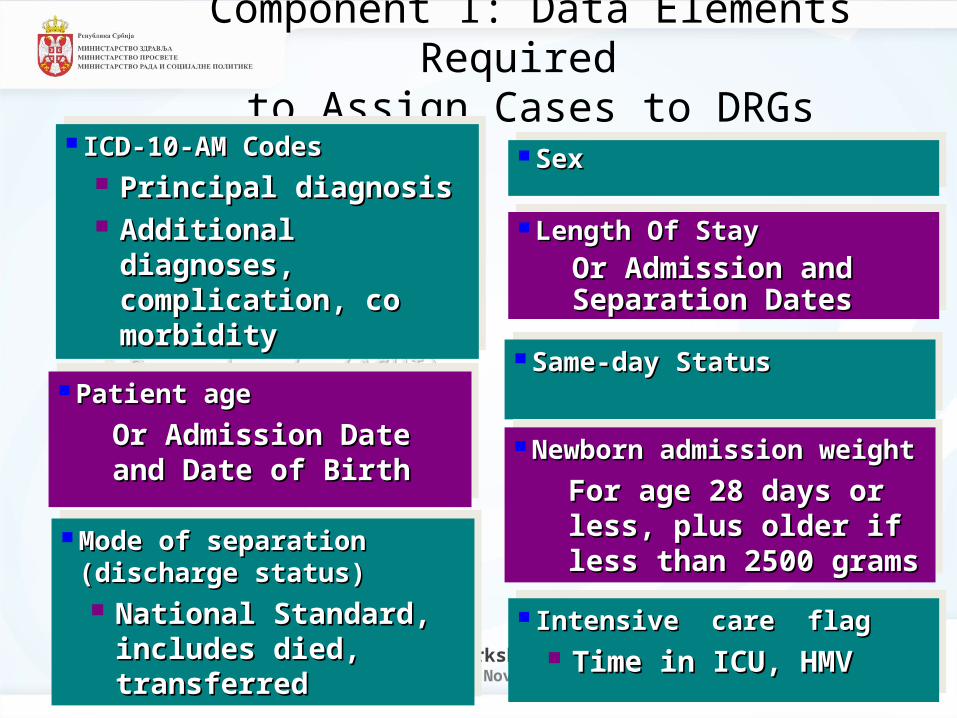
Component 1: Data Elements Required to Assign Cases to DRGs
ICD-10-AM CodesICD-10-AM Codes Principal diagnosisPrincipal diagnosis Additional diagnoses, Additional diagnoses,
complication, co morbiditycomplication, co morbidity Procedure/s (ACHI)Procedure/s (ACHI)
ICD-10-AM CodesICD-10-AM Codes Principal diagnosisPrincipal diagnosis Additional diagnoses, Additional diagnoses,
complication, co morbiditycomplication, co morbidity Procedure/s (ACHI)Procedure/s (ACHI)
Patient agePatient age Or Admission Date and Date Or Admission Date and Date
of Birthof Birth
Patient agePatient age Or Admission Date and Date Or Admission Date and Date
of Birthof Birth
Mode of separation (discharge Mode of separation (discharge status)status) National Standard, includes National Standard, includes
died, transferreddied, transferred
Mode of separation (discharge Mode of separation (discharge status)status) National Standard, includes National Standard, includes
died, transferreddied, transferred
SexSex SexSex
Same-day StatusSame-day Status Same-day StatusSame-day Status
Newborn admission weightNewborn admission weight For age 28 days or less, plus For age 28 days or less, plus
older if less than 2500 gramsolder if less than 2500 grams
Newborn admission weightNewborn admission weight For age 28 days or less, plus For age 28 days or less, plus
older if less than 2500 gramsolder if less than 2500 grams
Intensive care flagIntensive care flag Time in ICU, HMVTime in ICU, HMV
Intensive care flagIntensive care flag Time in ICU, HMVTime in ICU, HMV
Length Of StayLength Of Stay Or Admission and Separation Or Admission and Separation
DatesDates
Length Of StayLength Of Stay Or Admission and Separation Or Admission and Separation
DatesDates
DRG Workshop Belgrade, 18-22.November 2013.
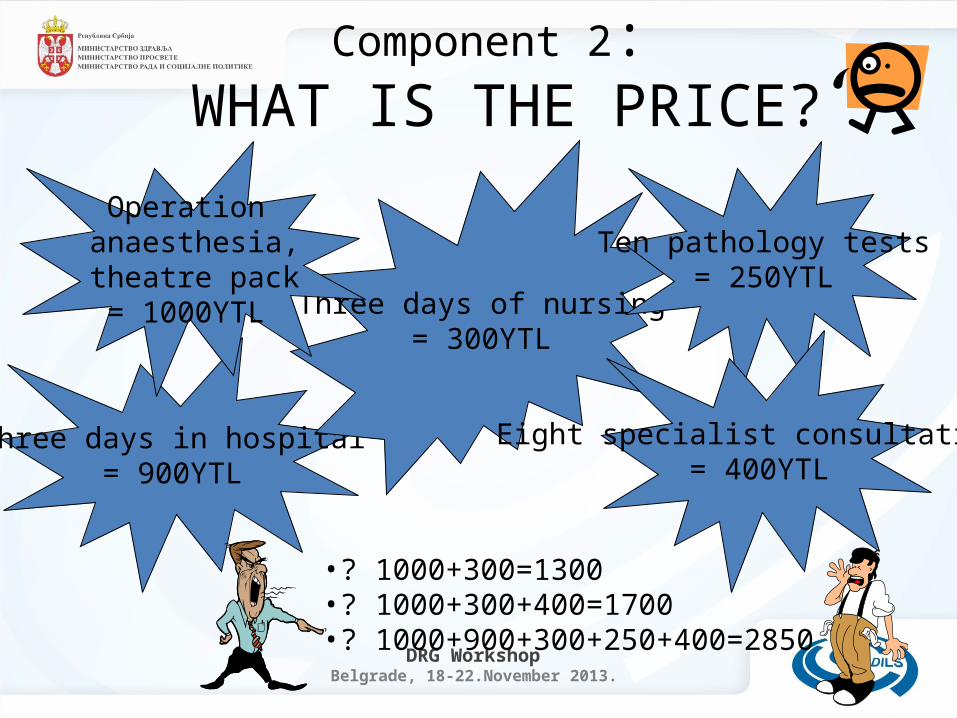
Component 2: WHAT IS THE PRICE?
Three days in hospital= 900YTL
Three days of nursing= 300YTL
Operation anaesthesia, theatre pack= 1000YTL
Ten pathology tests= 250YTL
Eight specialist consultations= 400YTL
•? 1000+300=1300•? 1000+300+400=1700•? 1000+900+300+250+400=2850
DRG Workshop Belgrade, 18-22.November 2013.
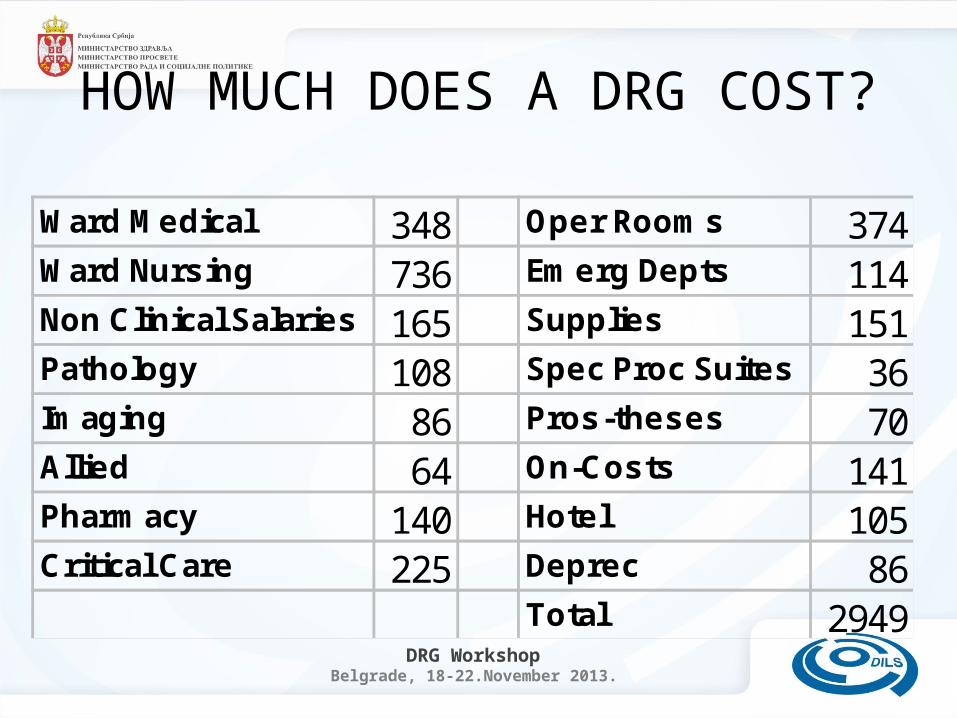
HOW MUCH DOES A DRG COST?
Ward Medical 348 Oper Rooms 374Ward Nursing 736 Emerg Depts 114Non Clinical Salaries 165 Supplies 151Pathology 108 Spec Proc Suites 36Imaging 86 Pros-theses 70Allied 64 On-Costs 141Pharmacy 140 Hotel 105Critical Care 225 Deprec 86
Total 2949
DRG Workshop Belgrade, 18-22.November 2013.
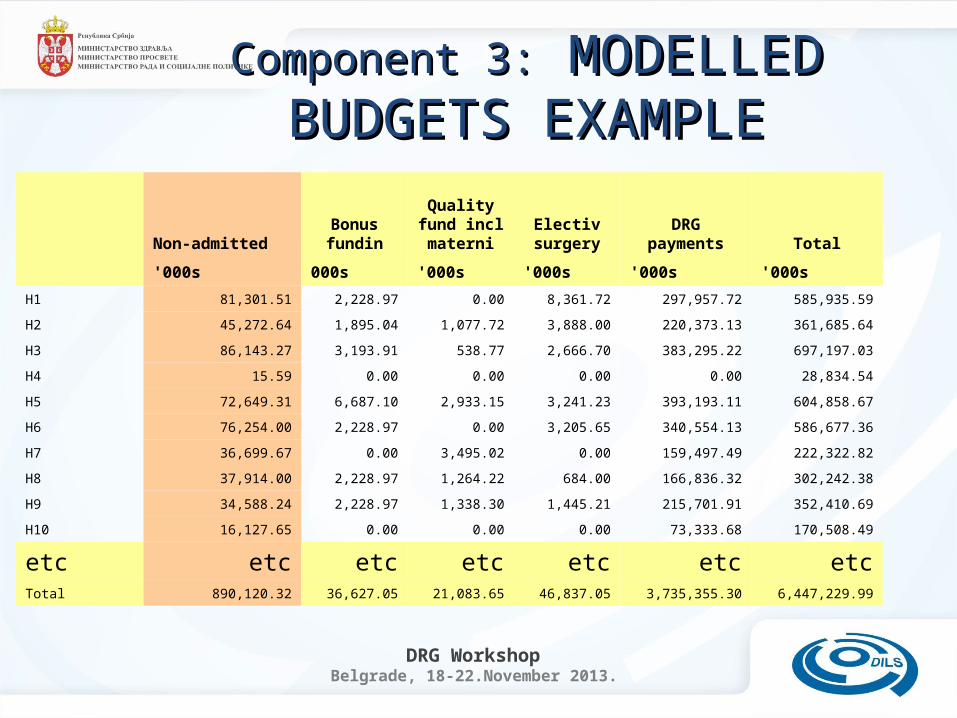
Non-admittedBonus fundin
Quality fund incl materni
Electiv surgery
DRG payments Total
'000s 000s '000s '000s '000s '000s
H1 81,301.51 2,228.97 0.00 8,361.72 297,957.72 585,935.59
H2 45,272.64 1,895.04 1,077.72 3,888.00 220,373.13 361,685.64
H3 86,143.27 3,193.91 538.77 2,666.70 383,295.22 697,197.03
H4 15.59 0.00 0.00 0.00 0.00 28,834.54
H5 72,649.31 6,687.10 2,933.15 3,241.23 393,193.11 604,858.67
H6 76,254.00 2,228.97 0.00 3,205.65 340,554.13 586,677.36
H7 36,699.67 0.00 3,495.02 0.00 159,497.49 222,322.82
H8 37,914.00 2,228.97 1,264.22 684.00 166,836.32 302,242.38
H9 34,588.24 2,228.97 1,338.30 1,445.21 215,701.91 352,410.69
H10 16,127.65 0.00 0.00 0.00 73,333.68 170,508.49
etc etc etc etc etc etc etcTotal 890,120.32 36,627.05 21,083.65 46,837.05 3,735,355.30 6,447,229.99
Component 3:Component 3: MODELLED BUDGETS MODELLED BUDGETS EXAMPLEEXAMPLE
DRG Workshop Belgrade, 18-22.November 2013.
Component 4: How do you change funding method?
• Phasing– Transition strategy– Initial steps
• Policy design• Consensus• Modelling and
demonstration
DRG Workshop Belgrade, 18-22.November 2013.
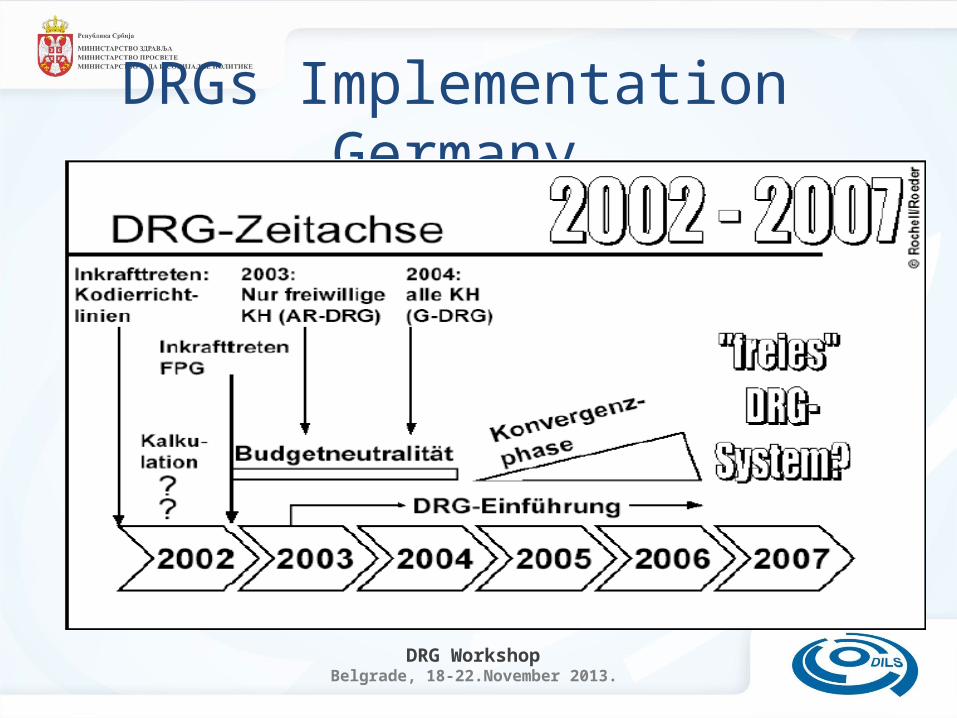
DRGs Implementation Germany
DRG Workshop Belgrade, 18-22.November 2013.
Healthcare system outputs rather than inputs
DRG Workshop Belgrade, 18-22.November 2013.
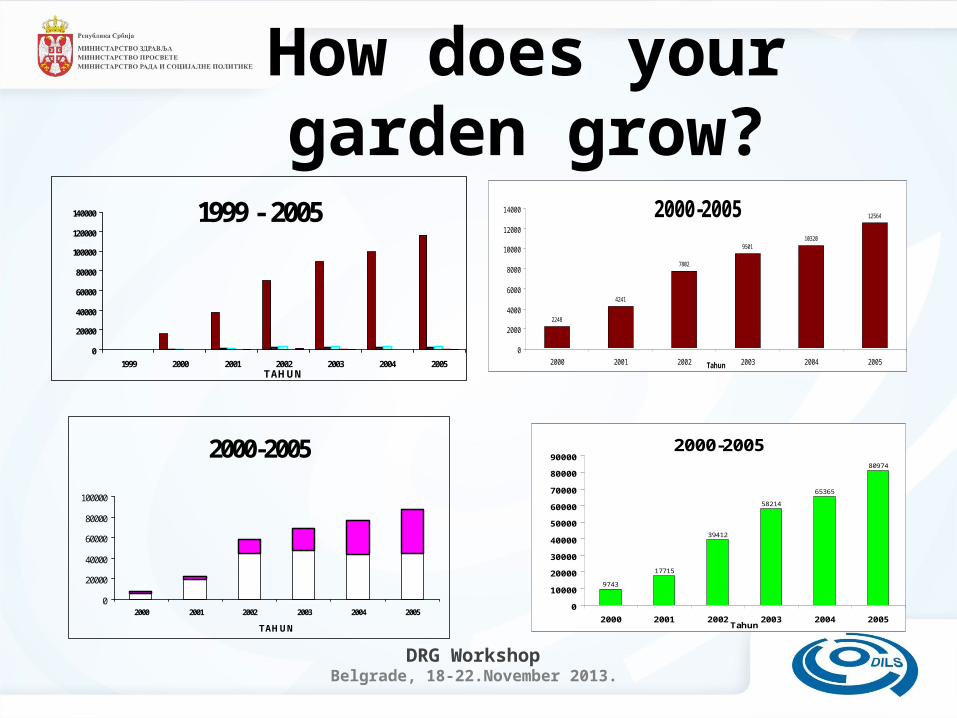
How does your garden grow?
1999 - 2005
0
20000
40000
60000
80000
100000
120000
140000
1999 2000 2001 2002 2003 2004 2005TAHUN
2000-2005
0
20000
40000
60000
80000
100000
2000 2001 2002 2003 2004 2005
TAHUN
2000-2005
9743
17715
39412
58214
65365
80974
0
10000
20000
30000
40000
50000
60000
70000
80000
90000
2000 2001 2002 2003 2004 2005Tahun
2000-2005
2248
4241
7802
950110320
12564
0
2000
4000
6000
8000
10000
12000
14000
2000 2001 2002 2003 2004 2005Tahun
DRG Workshop Belgrade, 18-22.November 2013.
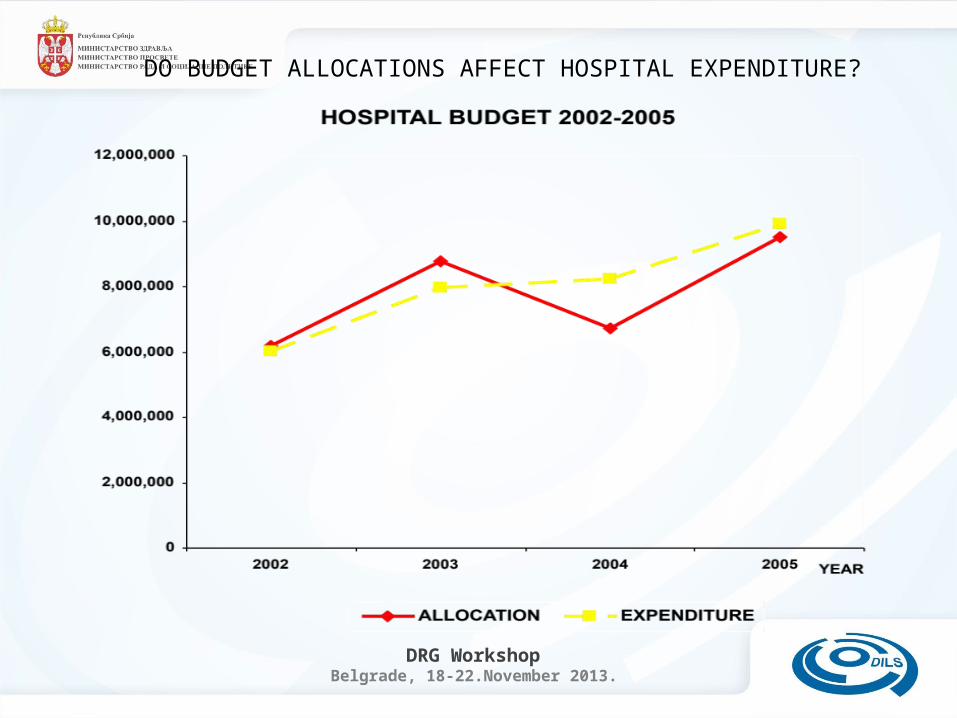
DO BUDGET ALLOCATIONS AFFECT HOSPITAL EXPENDITURE?
DRG Workshop Belgrade, 18-22.November 2013.
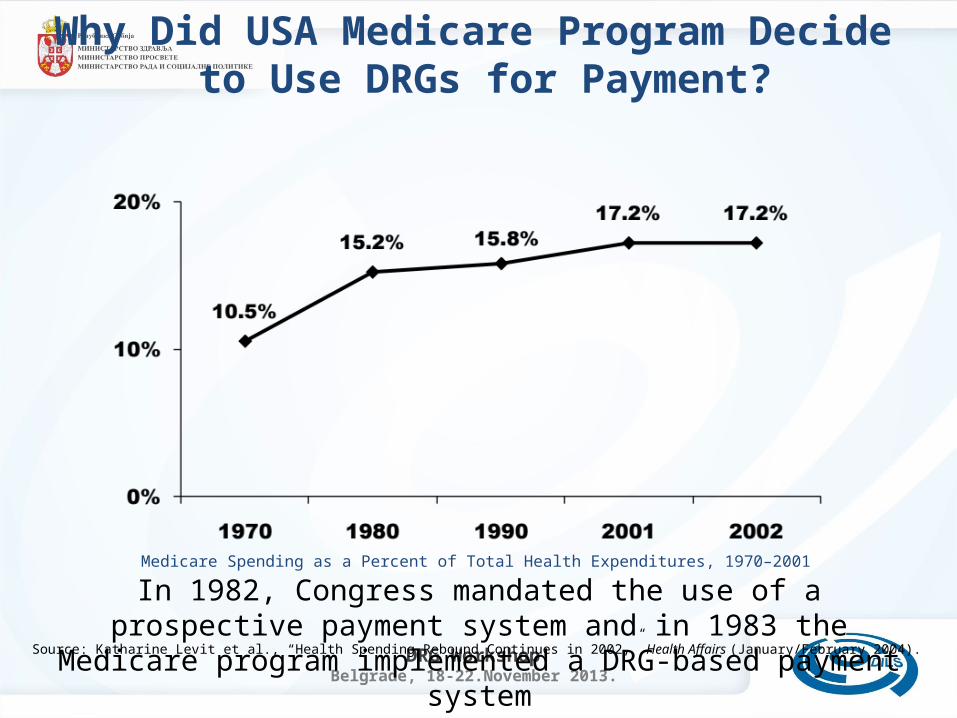
In 1982, Congress mandated the use of a prospective payment system and in 1983 the Medicare program implemented a DRG-based payment system
Medicare Spending as a Percent of Total Health Expenditures, 1970–2001
Why Did USA Medicare Program Decide to Use DRGs for Payment?
Source: Katharine Levit et al., “Health Spending Rebound Continues in 2002,” Health Affairs (January/February 2004).
DRG Workshop Belgrade, 18-22.November 2013.
Provider Payment Methods
• ITEMISED BILLING – “Fee for Service”
• BUNDLED BILLING – “Per episode”
• CAPITATION FUNDING – “Per patient”
• GLOBAL BUDGETS – “Historic plus”
DRG Workshop Belgrade, 18-22.November 2013.
Why diagnoses are more useful than procedures
• They allow clinical discretion
• The clinician is the resource manager
• Paying on procedures means more procedures results in more payment
• Best value for money (outcome) is more important than the lowest cost or the greatest quantity of treatment
DRG Workshop Belgrade, 18-22.November 2013.
The idea of resource homogenous categories
• Payment within groups should be related to the average or benchmark cost of providing the service.
• If cost is too variable: – some providers may select only the least
complex lowest cost cases. “cream skimming”– some providers may be at risk of getting the
most complex and expensive cases.– ANALYSIS OF DATA – BOTH PAYER AND HOSPITAL
DRG Workshop Belgrade, 18-22.November 2013.
The idea of clinically meaningful categories
• for describing healthcare services
• Classes must contain like with like cases from a clinical point of view – eg – Similar skills and facilities required to treat. – Similar care protocols used– Comparable in terms of outcome
expectations.
DRG Workshop Belgrade, 18-22.November 2013.
The idea of the Diagnosis Related Group
DRG Workshop Belgrade, 18-22.November 2013.
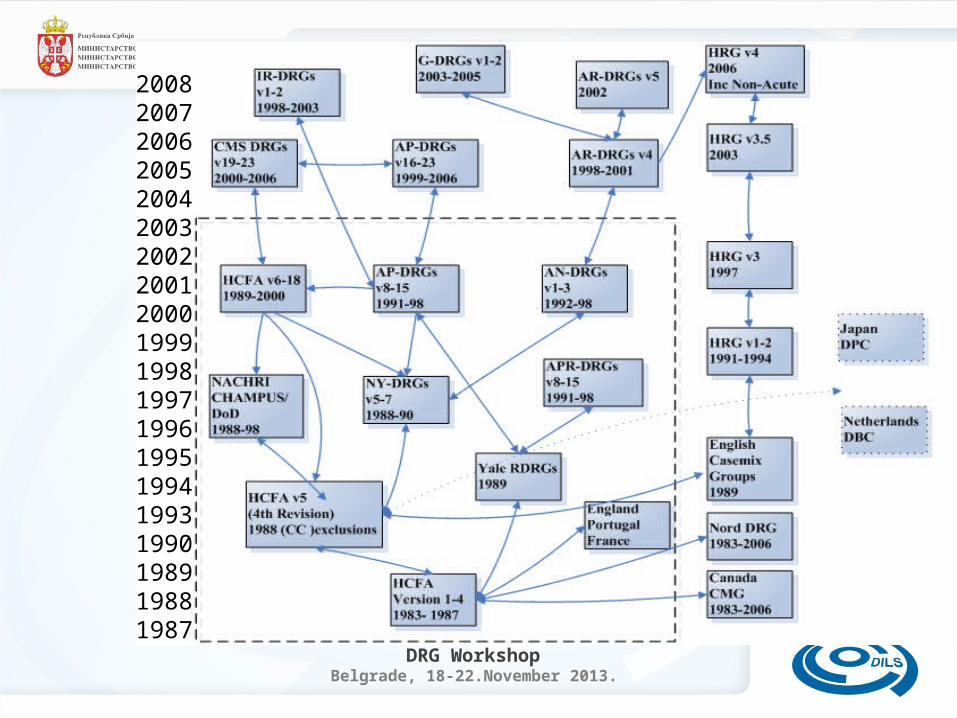
20082007200620052004200320022001200019991998199719961995199419931990198919881987
DRG Workshop Belgrade, 18-22.November 2013.
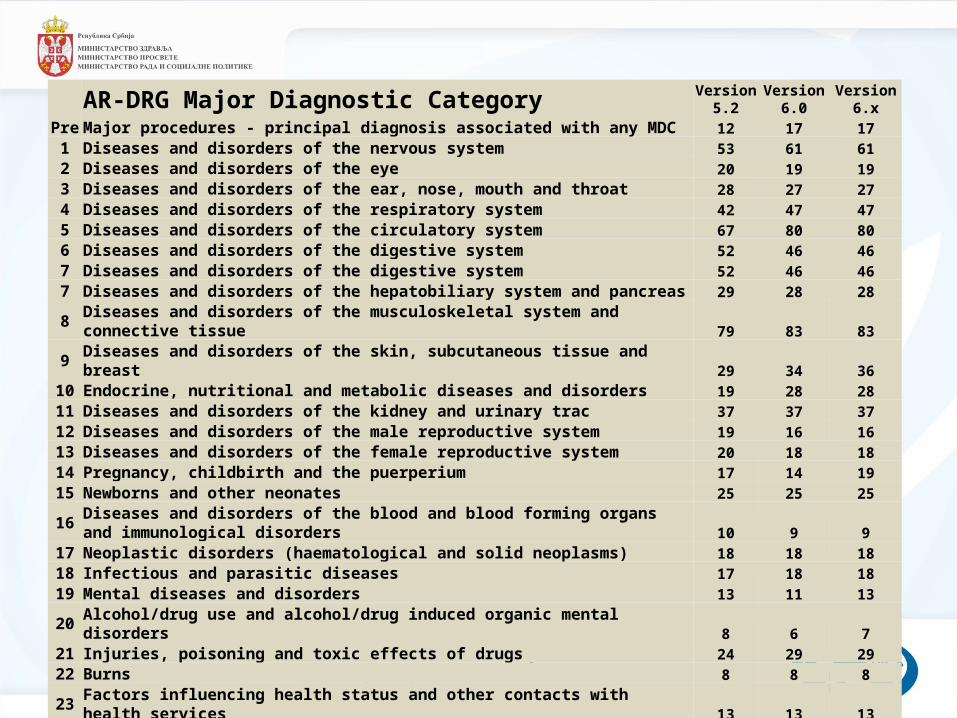
AR-DRG Major Diagnostic Category Version 5.2
Version 6.0
Version 6.x
Pre Major procedures - principal diagnosis associated with any MDC 12 17 171 Diseases and disorders of the nervous system 53 61 612 Diseases and disorders of the eye 20 19 193 Diseases and disorders of the ear, nose, mouth and throat 28 27 274 Diseases and disorders of the respiratory system 42 47 475 Diseases and disorders of the circulatory system 67 80 806 Diseases and disorders of the digestive system 52 46 467 Diseases and disorders of the digestive system 52 46 467 Diseases and disorders of the hepatobiliary system and pancreas 29 28 288 Diseases and disorders of the musculoskeletal system and connective tissue 79 83 839 Diseases and disorders of the skin, subcutaneous tissue and breast 29 34 36
10 Endocrine, nutritional and metabolic diseases and disorders 19 28 2811 Diseases and disorders of the kidney and urinary trac 37 37 3712 Diseases and disorders of the male reproductive system 19 16 1613 Diseases and disorders of the female reproductive system 20 18 1814 Pregnancy, childbirth and the puerperium 17 14 1915 Newborns and other neonates 25 25 25
16Diseases and disorders of the blood and blood forming organs and immunological disorders 10 9 9
17 Neoplastic disorders (haematological and solid neoplasms) 18 18 1818 Infectious and parasitic diseases 17 18 1819 Mental diseases and disorders 13 11 1320 Alcohol/drug use and alcohol/drug induced organic mental disorders 8 6 721 Injuries, poisoning and toxic effects of drugs 24 29 2922 Burns 8 8 823 Factors influencing health status and other contacts with health services 13 13 13
Unrelated OR DRGs 0 3 3Error DRGs 6 3 3
717 744 754
DRG Workshop Belgrade, 18-22.November 2013.
So, in summary, DRGs:-
• Describe the number and type of patients– The Mix of cases – limited number of categories
• Resource homogeneity, Clinically meaningful• Used:-
– As funding indicator or payment scale BUT ALSO– To compare how different hospitals treat patients in
different conditions– To identify treatment trends– In quality improvement activities– To identify the types of patients hospitals treat– For retrospective data analysis for research
DRG Workshop Belgrade, 18-22.November 2013.
questions








![ednet.kku.ac.thednet.kku.ac.th/~edufin/file/news/n4.pdf · (G)) (Diagnosis Related Groups : DRGs) (Adjusted Relative Weight : AdjRW) n€u b (It] - näu) d (Emergency Claim Online](https://img.pdfslide.net/doc/110x75/5a987b0f7f8b9aba4a8d237e/ednetkkuac-edufinfilenewsn4pdfg-diagnosis-related-groups-drgs-adjusted.jpg)