-
8/9/2019 Diagnostic Oral Radiology
1/27
-
8/9/2019 Diagnostic Oral Radiology
2/27
Penyusun :
Harris Kusnandar
Deasty Elvina Jo Carolina
Leonita Hartanti
Inosensius Adi
-
8/9/2019 Diagnostic Oral Radiology
3/27
Disorder of the temporomandibular joint are
abnormalities that interfere with the normalform or function of
the joint.
Arthritides, inflammation, growthabnormalities.
-
8/9/2019 Diagnostic Oral Radiology
4/27
Clinical Features
Temporomandibular joint (TMJ) disfunction is
the most common jaw disorder, 86% adults
and adolescent showing >1 clinical symptoms.
Signs and symptoms: pain in the TMJ or ear or
both, headache, muscle tenderness, joint
stiffness, clicking or other joint noises,
reduced range of motion, and subluxation.
-
8/9/2019 Diagnostic Oral Radiology
5/27
Application of Diagnostic
Imaging As a supplement information, when: osseus
abnormalities or infection suspected,
conservative treatment failed, symptoms
worsening, history of trauma, clinical signs.
To evaluate: integrity and relationship of the
hard and soft tissues, confirm the extent stage
of progression of known disease, and evaluatethe effects of
treatment.
-
8/9/2019 Diagnostic Oral Radiology
6/27
Radiographic anatomy of TMJ
-
8/9/2019 Diagnostic Oral Radiology
7/27
Condyle
A bonny ellipsoid structure connected to the
mandibular ramus by a narrow neck.
The shape of the condyle varies considerably,and these
variations may cause difficulty with
radiographic interpretation, this underlines
the importance of understanding the range of
normal appearance.
-
8/9/2019 Diagnostic Oral Radiology
8/27
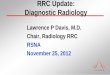
Most condyles have a pronounced ridge
oriented mediolaterally on the anteriorsurface, marking the
anterioinferior limit ofthe articulating area.
The ridge is the upper limit of the pterygoid
fovea, a small depression on the anteriorsurface at the junction
of the condyle andneck.
It is the attachment site of the superior head
of the lateral pterygoid muscle and shouldntbe mistaken for an
osteophyte (spur), whichindicate degenerative joint disease.
-
8/9/2019 Diagnostic Oral Radiology
9/27
Fig 26-1
-
8/9/2019 Diagnostic Oral Radiology
10/27
Temporal components ofTMJ are calcified by
6 months of age, complete calcification ofcortical borders may
not be complete until 20
years of age.
Radiographs of condyles in children may so a
little or no evidence of a cortical border.
In the absence of disease, the cortical borders
in adults are visible radographically.
-
8/9/2019 Diagnostic Oral Radiology
11/27
Mandibular Fossa
Located at the inferior aspect of the squamous
part of the temporal bone, is composed of the
glenoid fossa and articular eminence of the
temporal bone. Covered with a thin layer of
fibrocartilage.
temporal component ofTMJ
In normal TMJ, the roof of the fossa , the
posterior slope of the articular eminence, and
the eminence itself form an S shape when
viewed in sagital plane.
-
8/9/2019 Diagnostic Oral Radiology
12/27
Fossa depth varies, and the development of
the articular eminence relies on functionalstimulus from the
condyle.
The mandibular fossa very flat andunderdeveloped in patients
with micrognathia
or condylar agenesis.
-
8/9/2019 Diagnostic Oral Radiology
13/27
All aspects of the temporal component may
be pneumatized with small air cells derived
from the mastoid air complex. Seen in
approximately in 2% of patients.
FIG 26-3
-
8/9/2019 Diagnostic Oral Radiology
14/27
-
8/9/2019 Diagnostic Oral Radiology
15/27
During mandibular opening, as the condyle
rotates and translates downward and forward, the disk also moves
forward and rotates so
thats its thin central portion remains between
the articulating convexities of the condylar
head and articular eminence.
-
8/9/2019 Diagnostic Oral Radiology
16/27
Retrodiskal Tissues
Consists of a bilaminar zone of vascularized
and innervated loose fibroelastic tissue.
As the condyle moves forward, tissue ofposterior attachment
expand in volume,
primarily as a result of venous distention, and
as the disk move forward, tension is produced
in the elastic posterior attachment.Smooth recoil of the
disk
-
8/9/2019 Diagnostic Oral Radiology
17/27
Temporomandibular Joint Bony
Relationships
Radiographic joint Space; between the
condyle and temporal component.
The left and right condylar position within the
fossa can be determined and compared by thedimensions of the
radiographic joint space
viewed on collateral lateral images.
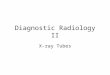
Because the radiographic outline of theglenoid fossa and the
condyle do not match
like a smooth ball and socket joint, the joint
space often varies from medial to lateral
aspects of the joint.
-
8/9/2019 Diagnostic Oral Radiology
18/27
Fig 26-5
-
8/9/2019 Diagnostic Oral Radiology
19/27
Markedly eccentric condylar positioning
usually represents an abnormality.
Exp, inferior condylar positioning (widened
joint space) maybe seen in case involving fluid
or blood within the joint. Superior condylar positioning
(decreased OR
no joint space) may indicate loss,
displacement, or perforation of intracapsular
soft tissue components.
-
8/9/2019 Diagnostic Oral Radiology
20/27
Condylar Movement
The condyle typically found within a range of
2-5 mm posterior and 5-8 mm anterior in the
crest of the eminence.
Reduce condylar translation, has little Or nodownward and
forward movement and
doesnt leave the mandibular fossa seen in
patient who clinically have a reduced degree
of mouth opening.
Hypermobility : translate >5 mm anterior to
the eminence.
-
8/9/2019 Diagnostic Oral Radiology
21/27
Diagnostic Imaging of the
TMJ Depends on the specific clinical problems.
Both joints should be imaged during the
examination, for comparison.
-
8/9/2019 Diagnostic Oral Radiology
22/27
Osseus Structures
Panoramic Projection
Provide: overall view of teeth and jaws,
comparing the left and right sides of themandible, as a
screening projection to identify
odontogenic diseases and other disorder that
maybe the source ofTMJ symptoms.
Limitation : distorted view of the joints,
severe image quality.
-
8/9/2019 Diagnostic Oral Radiology
23/27
Fig 26-6
-
8/9/2019 Diagnostic Oral Radiology
24/27
Gross osseus changes in the condylus,
asymmetries, extensive erosions, largeosteophytes, tumors,
fractures.
Shouldnt be used as a sole imaging modality.
Plain Film Imaging Modality
Combined of: transcranial, transpharyngeal,
transorbital, and submentovertex projection.
-
8/9/2019 Diagnostic Oral Radiology
25/27
Conventional Tomography
Is a radiographic technique that producesmultiple thin image
slices, permitting
visualization of the osseus structures
essentially free of superimpositions of
overlapping structures.
Computed Tomography
Two devices available: Conventional CT and
CBCT, but only conventional CT provides
images of the surrounding soft tissues.
-
8/9/2019 Diagnostic Oral Radiology
26/27
CT useful for determining the presence and
extent of ankylosis and neoplasms and degreeof bone involvement
in arthritides, imaging
complex fractures, for evaluating
complications from the use of
polytetrafluoroethylene or silicon sheet
implants.
-
8/9/2019 Diagnostic Oral Radiology
27/27
Soft Tissue Structures
Indications : TMJ pain and dysfunction, clinical
finding suggest disk displacement, and
symptoms unresponsive to conservative
therapy.