Embed Size (px)
Citation preview
![Page 1: Diarrhoea and/or Vomiting (Gastroenteritis) Pathway · Consider any of the following as possible indicators of diagnoses other than gastroenteritis [See Table 3 overleaf]: • Sepsis](https://reader031.pdfslide.net/reader031/viewer/2022020206/5d36b1d888c993c93f8b7fd1/html5/thumbnails/1.jpg)
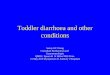
Consider Blood GlucoseAdvice from Lead ED / Paediatrician-On-Call* should be sought and/or a clear management plan agreed with parents.Begin management of clinical dehydration algorithm [see Fig 3]See [Fig 4] for Stool sample microscopy indications
Immediate Paediatric AssessmentIf clinical shock suspected or confirmed follow management plan [see Fig 1]See [Fig 4] for Stool sample microscopy indications
Amber Action Urgent Action Green Action
For all patients, continue monitoring following PEWS Chart recommendation
This guidance is written in the following context:
This document was arrived at after careful consideration of the evidence available including but not exclusively NICE, SIGN, EBM data and NHS evidence, as applicable. Healthcare professionals are expected to take it fully into account when exercising their clinical judgement. The guidance does not, however, override the individual responsibility of healthcare professionals to make decisions appropriate to the circumstances of the individual patient in consultation with the patient and / or carer.
Fig 3 Management of Clinical Dehydration• Increase oral fluid intake to 2 mls/kg every 10 mins with an oral
rehydration solution (ORS) aiming for 50 ml/kg over 4 hours• Continue breast / bottle feeding, little and often is best• Give ORS via nasogastric tube if the child is unable to drink or
vomits persistently• A&E - Refer to Paediatrics if after 2 hours and child is still amber• Consider use of Ondansetron as per local policy
Yes
ClinicalFindings Green - low risk Amber - intermediate risk Red - high riskAge
Behaviour
Over 3 months old
• Responds normally to social cues
• Content / smiles
• Stays awake / awakens quickly
• Strong normal crying / not crying
Under 3 months old
• Altered response to social cues• No smile
• Decreased activity• Irritable • Lethargic• Appears unwell
• No response to social cues
• Unable to rouse or if roused does not stay awake• Appears ill to a healthcare professional• Weak, high pitched or continuous cry
Skin
Hydration
• Normal skin colour• Normal turgor• Warm extremities • Not dehydrated• CRT < 2 secs • Moist mucous membranes (except after a drink) • Normal urine output• Fontanelle normal
• Normal skin colour • Warm extremities • Reduced skin turgor
• Clinically dehydrated• CRT 2-3 secs • Dry mucous membranes (except for mouth breather) • History of reduced urine output or fewer wet nappies than usual • Sunken fontanelle
• Pale / mottled / ashen blue • Cold extremities
• Clinical Shock• CRT> 3 secs• History of significant reduction in output or dry nappies > 18 hours• Markedly sunken fontanelle
RespiratoryMeasured at rest for 30 seconds
• Normal breathing pattern and rate** • Normal breathing pattern and rate** • Abnormal breathing / tachypnoea**
Heart Rate • Heart rate normal • Peripheral pulses normal
• Mild tachycardia* • Peripheral pulses normal • Severe tachycardia*
Blood pressure
• Normal* • Normal* • Hypotensive*
Eyes • Normal Eyes • Not sunken • Sunken Eyes Sunken eyes
Younger
Firs
t Dra
ft Ve
rsio
n: M
ay 2
011
Sub
sequ
ent V
ersi
ons
have
bee
n pu
blis
hed
in N
ov 2
013,
Jan
201
5 an
d M
ay 2
015.
Dat
e of
this
Ref
resh
ed V
ersi
on: D
ec 2
016
Rev
iew
Dat
e: D
ec 2
018
TriageAssessment (PEWS Score)Temp, Heart Rate, RR, CRT, O2 Sats BP, Blood Glucose (if indicated) Consider Stool Microscopy [Fig 4]Nursing Assessment -History Hydration AntipyreticsOral Rehydration Solution (ORS) 1 ml / kg every 10 minutes and/or continue breastfeedingTry to isolate to limit cross infection
Consider any of the following as possible indicators of diagnoses other than gastroenteritis [See Table 3 overleaf]:• Sepsis • Fever: Temperature of > 38°C (younger than 3 months) • Temperature of > 39°C (3 months or older) • Shortness of breath or tachypnoea • Altered state of consciousness • Consider a diagnosis of diabetes • Neck stiffness • Bulging fontanelle in infants • Non blanching rash • Blood and/or mucous in stool • Bilious (green) or blood-stained vomit • Projectile vomiting • Vomiting alone • Head Injury • Severe localised abdominal pain • Abdominal distension or rebound tenderness • History/Suspicion of poisoning e.g. Carbon Monoxide
Discuss with Lead ED / Paediatric Doctor
Fig 1 Management when clinical shock suspected• Give 20 ml/kg 0.9% Sodium Chloride First Bolus Reassess Give 20 ml/kg 0.9% Sodium Chloride as First Bolus and alert Paediatric Emergency Service
Fig 2 IV Fluid TherapyOnly use IV fluid therapy if in shock or red flag patient and deteriorates despite ORS or persistently vomits ORS therapy. Always use isotonic solutions. Use maintenance plus replacement 50 – 100 mls/kg over 48 hours dependent on severity.
If you need language support or translation please inform the member of staff to whom you are speaking.
To feedback or for further information including how to obtain more copies of this document (Please Quote Ref: DV1) we have one mailbox for
these queries on behalf of the South East Clinical Networks area (Kent, Surrey and Sussex). Please email: [email protected]
Some useful phone numbers (You may want to add some numbers on here too)
Self Care
Using the advice overleaf
you can provide the care
your child needs at homeIf none of the above features are present, most children
with Diarrhoea and / or Vomiting can be safely managed at home.
(Please note that children younger than 1 year or those who were born with a low birth
weight may be more prone to become dehydrated. If your child appears otherwise well,
but you still have concerns please contact your GP surgery or call NHS 111).
How is your child? (traffic light advice)
You need to contact a
doctor or nurse today
Please ring your
GP surgery or call
NHS 111 - dial 111If your child:
seems dehydrated: ie. dry mouth, sunken eyes, no tears, sunken
fontanelle (soft spot on baby’s head), drowsy or passing less urine than normal
has blood in the stool (poo) or constant tummy pain
has stopped drinking or breastfeeding and / or is unable to keep down
drinks / tolerate oral fluids during this illness
becomes irritable or lethargic
their breathing is rapid or deep
has cold feet and hands with no mottling of skin
blood in the vomit
is under 3 months old
You need urgent help
please phone 999
or go to the nearest
Hospital Emergency
(A&E) DepartmentIf your child is / has:
becomes difficult to rouse / unresponsive
becomes pale and floppy
finding it difficult to breathe
Diabetes
cold feet and hands with mottled skin
No wet nappies or wees for > 18 hours
Further advice / Follow upName of Child
Age Date / Time advice given
Name of Professional
Signature of Professional
Red
Amber
Green
Diarrhoea and/or Vomiting Advice Sheet
(Gastroenteritis) - Advice for parents and carers
of children younger than 5 years
Most children with diarrhoea and / or vomiting get better very quickly, but some children can get worse. You need to
regularly check your child and follow the advice given to you by your healthcare professional and / or as listed on this sheet.
For online advice: NHS Choices www.nhs.uk (available 24 hrs - 7 days a week)
Family Information Service: All areas have an online service providing useful information for Families
set up by local councils
GP Surgery
(make a note of number here)
......................................
.........
NHS 111 dial 111
(available 24 hrs -
7 days a week)
School Nurse /
Health Visiting Team
(make a note of number here)
......................................
.........
......................................
.........
December 2016
Kent, Surrey & Sussex
Version
Children and Young PeopleSouth East Clinical Networks
Patient presents with or has a history of
diarrhoea & / or vomiting
Diarrhoea and/or Vomiting (Gastroenteritis) PathwayClinical Assessment / Management Tool for Children Younger than 5 years with suspected Gastroenteritis
Management - Acute Setting
(APLS†)
< 1 year1-2 years
> 2-5 years
Respiratory Rate at rest: [b/min]
30 - 4025 - 3525 - 30
Heart Rate[bpm]
110 - 160100 - 15095 - 140
Table 2 Normal Paediatric Values: Systolic Blood Pressure [mmHg]
70 - 9080 - 95
80 - 100
Table 1
Do the symptoms and/or signs suggest an immediately life threatening (high risk) illness?
Complete PEWS for all patients
Alert Paediatric Emergency Service following local hospital referral pathwayMove to Resuscitation Area [see Fig 1]Resus Call (“2222”) for Paediatric Arrest
Yes
ThinkSepsis
To avoid dehydration (see patient advice sheet) Continue with breast and / or bottle feeding Encourage fluid intake, little and often Children at increased risk of dehydration [see Fig 5 overleaf]Confirm they are comfortable with the decisions / advice given and then think “Safeguarding” before sending home.See [Fig 4] for Stool sample microscopy indications
December 2016
Kent, Surrey & Sussex Version
Children and Young PeopleSouth East Clinical Networks
* Please see Normal Paediatric Values in Table 2 above.
†Advanced Paediatric Life Support The Practical Approach Fifth Edition Advanced Life Support Group Edited by Martin Samuels; Susan Wieteska Wiley-Blackwell / 2011 BMJ Books.
Rec
ord
your
find
ings
. G
MC
Bes
t Pra
ctic
e re
com
men
datio
n ht
tp://
bit.l
y/1D
PX
l2b
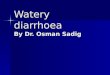
Fig 4 Stool Microscopy perform if:• Suspected septicaemia• Or immunocompromised• Or blood / mucous in stools
• Or history of travel abroad• Or no improvement in diarrhoea after 7 days
![Page 2: Diarrhoea and/or Vomiting (Gastroenteritis) Pathway · Consider any of the following as possible indicators of diagnoses other than gastroenteritis [See Table 3 overleaf]: • Sepsis](https://reader031.pdfslide.net/reader031/viewer/2022020206/5d36b1d888c993c93f8b7fd1/html5/thumbnails/2.jpg)
December 2016
Kent, Surrey & Sussex Version
Glossary of Terms and AbbreviationsAPLS Advanced Paediatric Life Support ED Hospital Emergency DepartmentB/P Blood Pressure HR Heart RateCPD Continuous Professional Development O2 SATS Oxygen Saturation in AirCRT Capillary Refill Time PEWS Paediatric Early Warning Score RR Respiratory Rate
Where can I learn more about paediatric assessment? We also recommend signing up to the online and interactive learning tool Spotting the Sick Child. It is free of charge. It was commissioned by the Department of Health to support health professionals in the assessment of the acutely sick child. It is also CPD certified.
www.spottingthesickchild.com
With many thanks to all those who have supported the development of our pathways including:
Dear Colleague,This has been produced by local clinical groups including representatives from acute, community and primary care as well as parents, education and social care and based on local independent clinical consensus. In particular we would also like to thank Wessex SCN and Paediatrics and Emergency Medicine colleagues for their support in finalising these versions for circulation. To feedback or for further information / copies (Please Quote Ref: DV3)please email: [email protected]
Yours sincerely
The Network
Aaron Gain Amanda Wood Carole Perry Carolyn Phillips Catherine Holroyd Chris Morris Christine McDermott Claire O’Callaghan Clare Lyons Amos Denise Matthams Dr Amit Bhargava Dr Ann Corkery Dr Anna MathewDr Catherine BevanDr Debbie Pullen Dr Farhana Damda
Dr Fiona Weir Dr Helen Milne Dr Neemisha Jain Dr Kamal Khoobarry Dr Kate AndrewsDr Liz McCulloch Dr Maggie WearmouthDr Mike LinneyDr Mwape Kabole Dr Nelly NinisDr Oli Rahman Dr Palla Prabhakara Dr Stuart Nicholls Dr Tim Fooks Dr Tim Taylor Dr Venkat Reddy
Dr Vijay Iyer Fiona Mackison Fiona WookeyGill Cunningham Jane Mulcahy Jason GrayJeannie Baumann Joanna Hodginkson Joanne Farrell Karen Hearnden Kate EadesKath EvansKathy Felton Kathy Walker Katie SheddenKim Morgan
Laura RobertsonLois PendleburyLois Peters Lorraine Mulroney Lucie Gamman Matthew White Melissa Hancorn Nicola MundyPatricia Breach Rebecca C ‘Aileta Rosie Courtney Rosie Rowlands Sarah West Susan NichollsSue Pumphrey Wang Cheung
Bas
ed o
n: D
iarr
hoea
and
vom
iting
in c
hild
ren
unde
r 5 2
009
NIC
E c
linic
al g
uide
line
84
Supporting Information
Table 3
Differential Diagnosis Most important features
Sepsis Sepsis - fever (especially >38°C in under 3 month old infants; >39°C in 3-6 month infants); tachypnoea/ tachycardia; non blanching rash; altered conscious level
Appendicitis Fever, anorexia, nausea/vomiting, migration of pain from central to RIF (see Appendicitis score – Table 4)
Constipation Positive bowel habit history. Pain mainly left sided/ supra pubic. If acute look for organic causes (ie obstruction)
Diabetic ketoacidosis Known diabetic or history of polydipsia/ polyuria and weight loss, BM >11, metabolic acidosis (pH< 7.3 / HCO3 <15 ) and blood ketones > 3 or ketone sticks more than 2+. (tests where available)
HUS Unwell child with bloody diarrhoea and triad of: anaemia, thrombocytopenia & renal failure
Infantile reflux / cows milk protein intolerance (CMPI)
Infant with inconsolable crying, drawing up of knees, back arching and sometimes blood in stools (CMPI) For more detail on the Infant Feeding pathways please see website or email:[email protected]
Infective Diarrhoea Blood or mucous in stools; foreign travel
Intussusception Mostly < 2 yrs, pain intermittent with increasing frequency, vomits (sometimes with bile), drawing up of knees, ‘red currant jelly’ stool (late sign)
Irreducible hernia Painful enlargement of previously reducible hernia +/- signs of bowel obstruction
Meckel’s diverticulum Usually painless rectal bleeding. Symptoms of intestinal obstruction. Can mimic appendicitis
Neurological Pathology Bulging fontanelle; head injury; altered conscious level; neck stiffness; headache
Pyloric Stenosis Projectile vomiting; worsening vomiting; clinically dehydrated(sunken fontanelle, dry nappies + mucous membranes; lethargy); weight loss; usually presents between 3-6 weeks old
Surgical Abdomen Localised abdominal pain; abdominal distention; rebound tenderness; bilious(green) vomitus
Urinary Tract Infection (UTI) Fever, dysuria, loin/ abdominal pain, urine dipstick positive for nitrites/ leucocytes. Follow local guidelines.
Children and Young PeopleSouth East Clinical Networks
Table 4 - Appendicitis Score
Sign / symptom Scoring
Fever (axillary temp > 38°C) 1Anorexia 1
Nausea or vomits 1
Pain on cough/ percussion or hopping 2RIF tenderness 2Migration of pain (from central to RIF) 1
WCC > 10,000 (where available) 1
Neutrophils > 7,500 (where available) 1Likelihood of appendicitis increase with total score (Maximum 10 points). When total score is <3 then appendicitis is unlikely and if it is > 6 appendicitis is likely. In borderline cases abdominal imaging (USS, CT) may be helpful after discussion with surgeon and radiologist - Samuel et al, J of Paed Surgery 2002, 6: 877 and Goldman et al, J Pediatr,2008,153:278
Fig 5 Children at increased risk of dehydration are those:• Aged <1 year old (and especially the < 6 month age group) • Low birth weight • Has had six or more episodes of diarrhoea in the past 24 hours• Have vomited three times or more in the last 24 hours
• Have not taken or have not been offered fluids before presentation
• Infants who have stopped breastfeeding during the illness • Children with malnutrition or faltering growth
![Diarrhoea and/or Vomiting (Gastroenteritis) Pathway fileConsider any of the following as possible indicators of diagnoses other than gastroenteritis [See Table 3 overleaf]: • Sepsis](https://img.pdfslide.net/doc/110x75/5d18907c88c99313688de58e/diarrhoea-andor-vomiting-gastroenteritis-pathway-any-of-the-following-as-possible.jpg)