Embed Size (px)
Citation preview

Digestive Pathology Lecture 1
Reproduction Prohibited
This file contains original text and images as well as materials adapted from copyrighted sources
For use only as a temporary educational aidPartially or completely copying or distributing the contents of this file may constitute an infringement of the fair use exception for teaching
faculty of the U.S. Copyright Law
LSUHSC-New Orleans, 2015
Last modified on September 21, 2015
…

ESOPHAGUS
1. Anatomical considerations2. Congenital anomalies
3. Webs and Rings
4. Achalasia
5. Hiatal hernias
6. Diverticula
7. Lacerations
8. Varices
9. Esophagitis
10. Neoplasia
---

Three narrow points
Upper sphincter (cricopharyngeus muscle)
– 70% foreign body impaction
Aortic arch crossover (middle esophagus)
Lower sphincter (diaphragm)

Adventitia The esophagus lacks serosal lining
– Outer lining is known as adventitia
– Rapid dissemination of infections and neoplasms

Stratified squamous epithelium
Some skin disorders have esophageal manifestations
– Blistering (bullous) conditions such as pemphigus vulgaris or Stevens-Johnson syndrome
– Hyperkeratotic conditions such as lichen planus
– Collagen-vascular disorders such as scleroderma

Striated muscle
The proximal esophagus contains striated muscle
– Skeletal muscle disorders can affect the esophagus

ESOPHAGUS
1. Anatomical considerations
2. Congenital anomalies– Agenesis
– Atresia
– Stenosis
– Duplications3. Webs and Rings
4. Achalasia
5. Hiatal hernias
6. Diverticula
7. Lacerations
8. Varices
9. Esophagitis
10. Neoplasia---

Agenesis, atresia
Agenesis: absence
Atresia: lack of canalization
– Usually at the level of the tracheal bifurcation
– Usually associated with a fistula

Atresia
The most common presentation:
– A blind proximal segment
– A fistula connecting the distal segment with the trachea or mainstem bronchus

Stenosis: Narrowing, stricture
Barium swallow test (barium is given orally; its transit through the esophagus can be visualized radiologically highlighting the stenotic areas)

Stenosis
More commonly, acquired:– Peptic (gastroesophageal reflux disease GERD)
– Pill esophagitis (potassium chloride, ferrous sulfate, antibiotics, bisphosphonates)
– Ingestion of excessively hot fluids
– Corrosive, caustics (lye)
– Intubation, sclerotherapy
– Connective tissue disorders (scleroderma)
– Tumors , radiation therapy, chemotherapy
Results in progressive dysphagia: first to solids, then to solids and liquids
Duplications
Esophageal duplications:
– Closed at both ends (duplication cyst)• The most common
– Open
• At one end (giant diverticulum)
• At both ends (double esophagus)

Esophageal Duplication Cyst
HumPath
RadioGraphics
60% occur in the lower esophagus

Eso
phageal D
uplic
ation, O
pen, D
ouble
Eso
phagus
RadioGraphics

ESOPHAGUS
1. Anatomical considerations
2. Congenital anomalies
3. Webs and Rings– Plummer Vinson syndrome
4. Achalasia
5. Hiatal hernias
6. Diverticula
7. Lacerations
8. Varices
9. Esophagitis
10. Neoplasia
---

Webs Membranous ridge, semi-circumferential
Mucosa and submucosa
Cervical esophagus
Women over age 40
Dysphagia to SOLIDS
Uncertain etiology

learningradiology
Esophageal Web: semi-circumferential, eccentric
endoatlas
Plummer-Vinson syndrome
Also called Paterson-Brown-Kelly syndrome:– Upper esophageal web
– Dysphagia
– Iron deficiency (sideropenic dysphagia)
Mostly women
Etiology uncertain: iron deficiency, genetic predisposition, autoimmune
May respond to iron supplementation
Balloon dilatation
Risk for squamous carcinoma

Cheilosis
Plummer Vinson syndrome
Atrophic glossitis
Koilonychia

Rings (Schatzki rings)
Circumferential
Lower esophagus
Mucosa, submucosa, muscularis propria
– A ring: rare, proximal to GE junction, has muscle
– B ring: common, at the GE junction, no muscle
No sex predilection
Most older than 40
May cause dysphagia to SOLIDS
Etiology is uncertain, may be associated with GERD

Eso
phageal Rin
g
ESOPHAGUS
1. Anatomical considerations
2. Congenital anomalies
3. Webs and Rings
4. Achalasia– Other dysmotility disorders
5. Hiatal hernias
6. Diverticula
7. Lacerations
8. Varices
9. Esophagitis
10. Neoplasia
---

Achalasia, “failure to relax”
Increased resting tone of the LES
Incomplete relaxation after swallowing
Most cases have absence of peristalsis
Progressive dilatation (megaesophagus)
Autoimmune injury of myenteric plexus ganglion cells
HSV-1 infection in genetically predisposed individuals
Cause FLUCTUANT dysphagia for solids AND liquids
Regurgitation, nocturnal coughing spells, aspiration
Myotomy, balloon dilatation, Botulinum toxin, medications that relax the LES
Risk for squamous carcinoma

Ach
ala
sia, m
egaeso
phagus
Indian Radiology

Achalasia, secondary causes Chagas disease (Trypanosoma cruzi)
Diabetic neuropathy
Infiltrative injury, amyloidosis, sarcoidosis, tumors
Vagus nerve injury

Other dysmotility disorders
Nutcracker esophagus– Intense peristaltic contractions
Diffuse esophageal spasm– Multiple segments contract at the same time
(absence of normal peristalsis)

Dysmotility disorders: Nutcracker esophagus
INTPC - DIFES

ESOPHAGUS
1. Anatomical considerations
2. Congenital anomalies
3. Webs and Rings
4. Achalasia
5. Hiatal hernias6. Diverticula
7. Lacerations
8. Varices
9. Esophagitis
10. Neoplasia
---

Hiatal hernias
Herniation of stomach through esophageal hiatus
Congenital
Acquired:– Muscle weakness (LES), aging
– Increased abdominal pressure• Obesity, pregnancy, constipation
– Can cause or can be caused by GERD
Two major types:– Sliding (axial)
– Paraesophageal (rolling)

Hia
tal H
ern
ias
Sliding
Rolling

Hiatal Hernia, Sliding, Paraesophageal
Hiatal hernias
Sliding
– Frequent (90% or more)
– Most are asymptomatic
– Some associated with GERD symptoms
– Cameron ulcers
Paraesophageal (rolling)
– Most are symptomatic
• Dysphagia, postprandial discomfort
– Volvulus (torsion) and strangulation can occur
– Early surgical repair recommended

Ulcers where the diaphragm impinges on the stomach.
Journal of Pediatric Gastroenterology & Nutrition. 56(5):e29, May 2013
Cameron ulcers

Hiatal Hernia Gastric volvulus
AJR. 2003;181: 403-414. 10.22

Hiatal hernias
EGJ
EGJ
EGJ
Type I Type II
Type III Type IV
ESOPHAGUS
1. Anatomical considerations
2. Congenital anomalies
3. Webs and Rings
4. Achalasia
5. Hiatal hernias
6. Diverticula– Zenker
– Traction
– Epiphrenic7. Lacerations
8. Varices
9. Esophagitis
10. Neoplasia
---
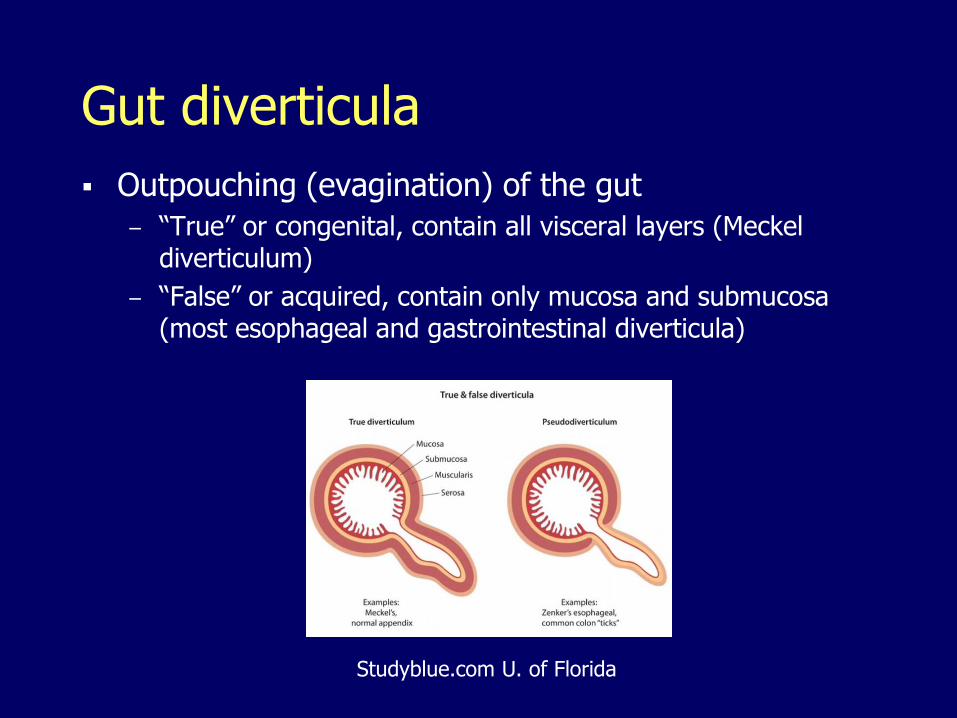
Gut diverticula
Outpouching (evagination) of the gut
– “True” or congenital, contain all visceral layers (Meckel diverticulum)
– “False” or acquired, contain only mucosa and submucosa (most esophageal and gastrointestinal diverticula)
Studyblue.com U. of Florida

Zenker diverticulum
Above the UES
Between thyropharyngeus and cricopharyngeus
Sensation of mass
Regurgitation (spontaneously or by applying pressure)
Halitosis

Zenker Diverticulum

Traction, epiphrenic
Traction: mid esophagus
– Scarring from mediastinal lymphadenitis (tuberculosis, histoplasmosis)
– Usually asymptomatic
Epiphrenic: immediately above LES
– Spasm of LES
– May result in regurgitation

Zenker, traction, epiphrenic diverticula

ESOPHAGUS
1. Anatomical considerations
2. Congenital anomalies
3. Webs and Rings
4. Achalasia
5. Hiatal hernias
6. Diverticula
7. Lacerations– Mallory-Weiss tear
– Boerhaave’s syndrome8. Varices
9. Esophagitis
10. Neoplasia
---

Lacerations
Mallory-Weiss tear
– Non-transmural (mucosal) laceration at esophagogastric junction, after forceful retching (alcoholic binge)
– Severe hematemesis, shock
Boerhaave syndrome
– Transmural rupture
– Severe hematemesis, shock
– Mediastinitis, sepsis
– High mortality

Mallory-Weiss tear, Boerhaave syndrome

ESOPHAGUS
1. Anatomical considerations
2. Congenital anomalies
3. Webs and Rings
4. Achalasia
5. Hiatal hernias
6. Diverticula
7. Lacerations
8. Varices9. Esophagitis
10. Neoplasia
---

Esophageal varices
Varicose dilatation of mucosal and submucosal veins
Mostly caused by portal hypertension
– Bypass through gastric coronary veins
Rupture, massive hematemesis, high mortality

Esophageal varices

Portal vein (PV), splenic vein (SPLV), gastric coronary vein (CV), esophageal varices (*)
RadioGraphics

ESOPHAGUS
1. Anatomical considerations
2. Congenital anomalies
3. Webs and Rings
4. Achalasia
5. Hiatal hernias
6. Diverticula
7. Lacerations
8. Varices
9. Esophagitis– GERD, Barrett esophagus
– Eosinophilic esophagitis
– Infectious esophagitis10. Neoplasia
---

Gastroesophageal reflux disease (GERD)
High prevalence (heartburn)
Excessive reflux of:– Stomach contents (acid reflux)
– Duodenal contents (bile reflux)
Caused by:– Decreased LES tone
– Hiatal hernia
– Smoking, alcohol, medications (calcium channel blockers, beta blockers, nitrates)
– Obesity, pregnancy
– Delayed gastric emptying (meals of larger weight and caloric content)

GERD Symptoms
– Heartburn
– Regurgitation
– Dysphagia
May result in:
– Erosion, ulceration
– Stenosis
– Shortening of the esophagus (hiatal hernia)
– Barrett esophagus, adenocarcinoma

GERD: Dilatation of intercellular spaces, papilla elongation/basal zone hyperplasia
Dent J., Clin Gastroenterol Hepatol

GERD: Papilla elongation/basal zone hyperplasia, intraepithelial PMNs
Barrett esophagus
Columnar (intestinal) metaplasia of the distal esophagus
Consequence of long-standing reflux
– The columnar epithelium is more resistant to acid
Long-segment Barrett: 3 cm or more
Risk of dysplasia and adenocarcinoma
– The most important risk factor
– Previously reported markedly increased cancer risk was exaggerated


Barrett, intestinal metaplasia-dysplasia-malignancy

Barrett, intestinal metaplasia-dysplasia-malignancy

Eosinophilic esophagitis
Marked infiltration of the squamous epithelium by eosinophils
Peripheral (blood) eosinophilia may be present
The majority of patients are allergic (atopic dermatitis/eczema, allergic rhinitis, asthma)
Causes GERD-like symptoms in the absence of acid reflux
Does not respond to acid suppression therapy
May respond to dietary changes and corticosteroids
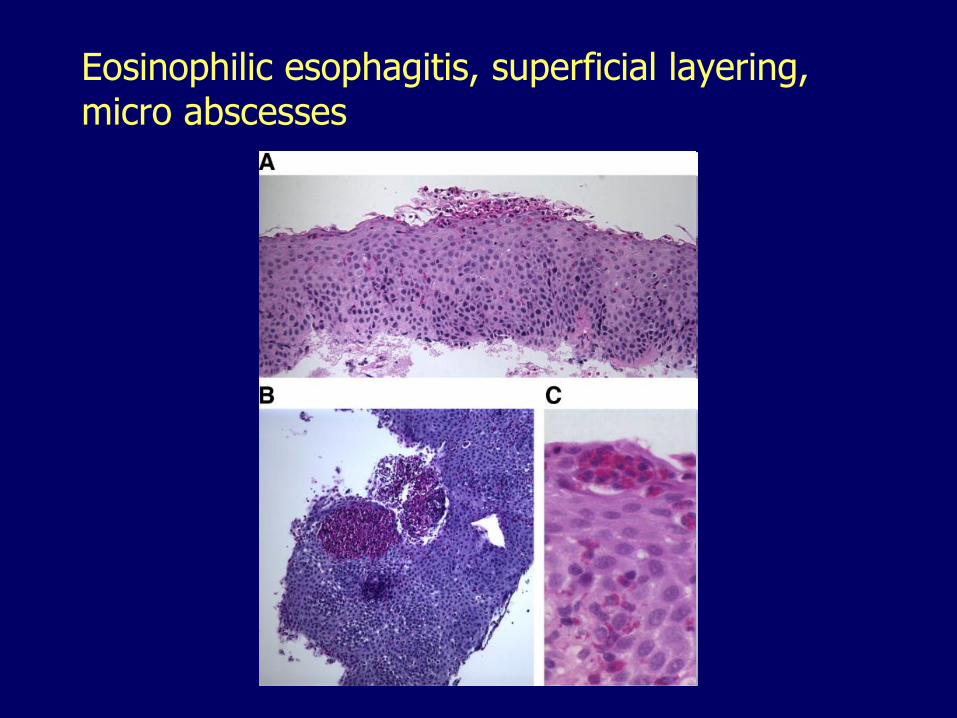
Eosinophilic esophagitis, superficial layering, micro abscesses

Infectious esophagitis
Candidiasis
Herpes
Cytomegalovirus

CandidiasisGray-white patches

Herpes, grossSmall punch-out ulcers

Herpes
Viral inclusions in squamous epithelial cells at the ulcers margins

Cytomegalovirus
Gaping ulcers
Viral inclusions in capillary endothelium and stromal cells
ESOPHAGUS
1. Anatomical considerations
2. Congenital anomalies
3. Webs and Rings
4. Achalasia
5. Hiatal hernias
6. Diverticula
7. Lacerations
8. Varices
9. Esophagitis
10. Neoplasms
---

Benign tumors
Leiomyomas, the most common
Squamous papillomas

Leiomyoma

Papilloma

Carcinoma of the esophagus
Two main types
– Squamous cell carcinoma
– Adenocarcinoma

Carcinoma of the esophagus, trends
Declining: squamous cell carcinoma
Increasing: adenocarcinomas (white males)
Worldwide, squamous carcinomas, 90%
In the U.S. adenocarcinoma, more than half
Most cancers (regardless of type), diagnosed after invasion and dissemination
Poor prognosis

Actual and projected esophageal cancer incidence rates, CDC
Squamous cell carcinoma
Men > women
Blacks > whites
The most common type among blacks
Middle third (50%), lower third (30%), upper third (20%)
Preceded by squamous dysplasia-carcinoma in situ

Squamous cell carcinoma, risk factors
Smoking
Alcohol
Vitamin, micronutrients deficiencies
Chronic esophagitis
Plummer-Vinson syndrome
Achalasia
HPV
Mold contaminated grains
Coarse food
Yerba mate

Betel nut

Mursik

Squamous cell carcinoma, mid esophagus

Squamous cell carcinoma
Odze. Surgical Pathology of the GI Tract, Liver, Biliary Tract and Pancreas

Adenocarcinoma
Men > women
Whites > blacks (most common type among whites)
White males particularly at risk
Most occur in the lower third
Follows Barrett esophagus, dysplasia
Risk factors:
– Those associated with reflux esophagitis and Barrett esophagus
Stomach infection with H. pylori may be protective

Esophageal adenocarcinoma vs. squamous cell carcinoma, US WHITE MALES, CDC

Why mostly white males?
Greater abdominal visceral adiposity, lessHelicobacter pyloriinfection and atrophic gastritis

Adenocarcinoma, lower esophagus

Adenocarcinoma forming glands and signet ring cells. Odze. Surgical Pathology of the GI Tract, Liver, Biliary Tract and Pancreas

STOMACH
1. Congenital anomalies
– Heterotopias
– Pyloric stenosis2. Gastritis
3. Hyperplastic gastropathies
4. Neoplasia
---

Heterotopias
Pancreatic heterotopia
Gastric heterotopia
– Proximal esophagus (inlet patch)
– Duodenum
– Meckel diverticulum

Pancreatic heterotopia

Esophageal inlet patch

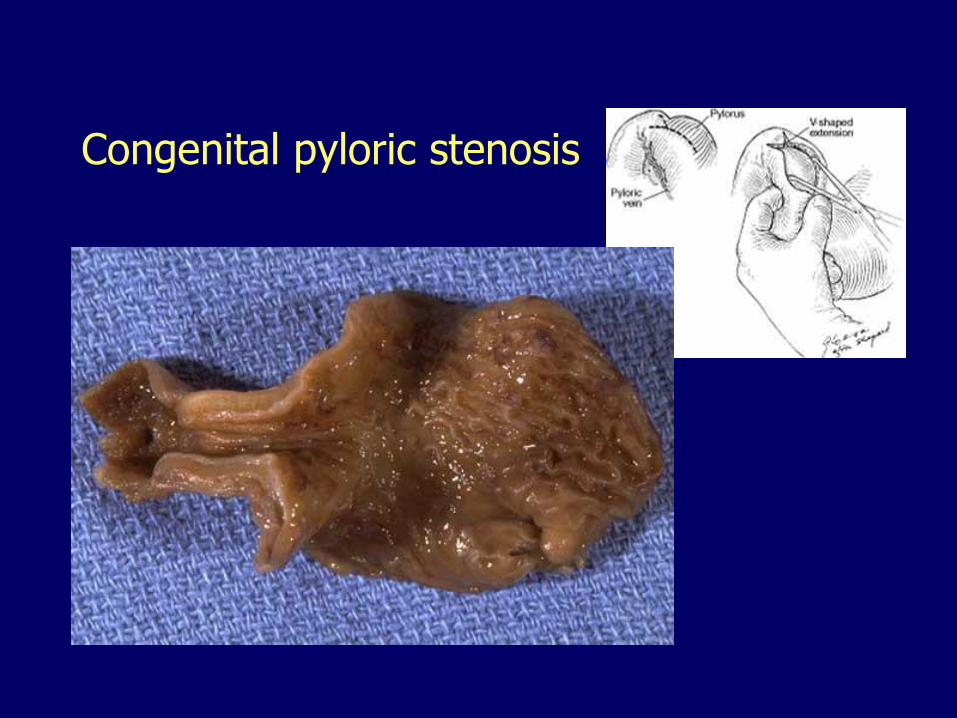
Congenital pyloric stenosis
Hypertrophy, hyperplasia, of muscularis propria
Boys more often than girls
Familial occurrence, concordance in twins
Newborns (second or third week)
Nonbilious vomiting
Visible peristalsis
Firm, ovoid mass in the region of the pylorus
Pylorotomy (muscle splitting) is curative
Congenital pyloric stenosis

Pyloric stenosis in the adult
Idiopathic, hypertrophic pyloric stenosis (rare)
Acquired gastric outlet obstruction (more common):
– Chronic gastritis
– Peptic ulcer
– Cancer

STOMACH1. Congenital anomalies
2. Gastritis
– Acute gastritis
– Chronic gastritis
– Helicobacter pylori infection3. Hyperplastic gastropathies
4. Neoplasia
---

Ulcers, a manifestation of gastritis
Acute gastritis
– Acute “stress” ulcers
Chronic gastritis
– Chronic “peptic” ulcers

Acute gastritis
Dominated by congestion, edema, PMNs
May be transient or long-lasting
Compromise of: mucus barrier, bicarbonate production, blood flow– Prostaglandin inhibitors (NSAIDS, corticosteroids)
– Ethanol
– Bile reflux (gastroenteroanastomosis)
– Shock (ischemic gastritis)
– Trauma, burns, surgery (stress gastritis)
– Cancer chemotherapy, other drugs
– Acids or alkali (acute corrosive gastritis)
– Hyperparathyroidism/ hypercalcemia
– Uremia
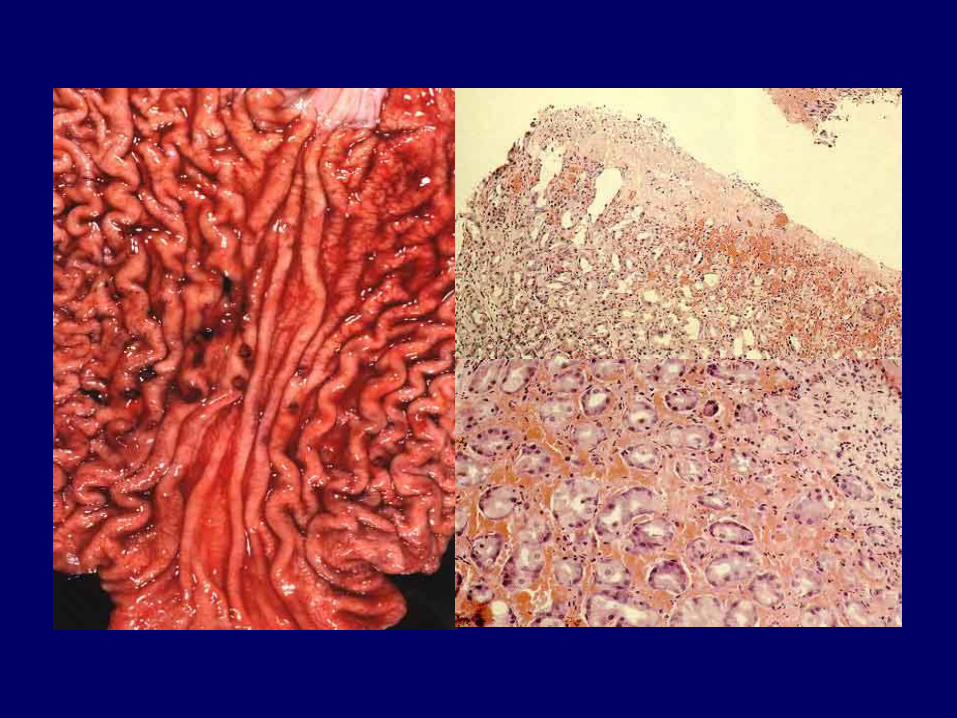
Chemical (reactive) gastropathy
Ethanol, bile reflux, NSAIDs
Congestion, edema, sparse inflammation and pronounced foveolar hyperplasia.

Chemical (reactive) gastropathy

Acute (stress) erosions and ulcers
Erosion: limited to the mucosae
Ulcer: beyond the muscularis mucosae
Morphology:
– Small
– Multiple
– Punch out
– Gastric rugal pattern is normal
– No specific location (throughout stomach and duodenum)
Curling ulcers: severe burns or trauma
Cushing ulcers: intracranial injury, operations, or tumors

Chronic gastritis
Dominated by lymphocytes and plasma cells
Long-lasting
Variable acute inflammation
– Chronic “active” gastritis
Three major forms:
– Non-atrophic
– Atrophic, environmental
– Atrophic, autoimmune
Chronic non-atrophic gastritis
Associated with:
– Helicobacter pylori infection
– Hyperacidity
– Pyloric channel and duodenal ulcers
Not associated with intestinal metaplasia, dysplasia or gastric cancer
Caucasian and affluent populations

Helicobacter pylori, Giemsa stain

Chronic atrophic gastritis, environmental
Atrophy (loss of glands)
Associated with:
– Helicobacter pylori infection
– Hypochlorhydria
– Gastric ulcers
– Intestinal metaplasia, dysplasia and adenocarcinoma
Minority and underprivileged populations


Autoimmune gastritis
CD4+ T cells
Autoantibodies
Parietal cell targets:
– H+/K+-ATPase
– Intrinsic factor
– Gastrin receptor
Associated with other autoimmune conditions
Familiar occurrence, Northern European descent
Atrophy of oxyntic (acid-producing) mucosa

Oxyntic mucosa
Cardia
Fundus
Corpus
Antrum
Pylorus

Autoimmune gastritis
Associated with
– Lost of intrinsic factor, vit. B12 deficiency,
• Pernicious anemia, atrophic glossitis, peripheral neuropathy
– Hypochlorhydria
• Hypergastrinemia, carcinoid tumors
– Intestinal metaplasia, dysplasia and adenocarcinoma

Atrophic gastritis, hypergastrinemia, carcinoids

Glossitis, megaloblastic anemia
Peptic ulcer disease (chronic ulcers)
Duodenal and pyloric channel ulcers, associated with:– Non-atrophic gastritis
– Hyperacidity
– Helicobacter pylori infection
Gastric ulcers, associated with:– Atrophic gastritis
– Hypochlorhydria
– Helicobacter pylori infection
Multiple ulcers, multiple sites– Zollinger Ellison syndrome

Less than 4 cm in diameter
Punched-out margins
Not raised or indurated
Clean base
Patent or thrombosed blood vessels
Puckering of mucosal folds

Double-contrast radiograph of benign lesser curvature ulcer, smooth ovoid contour, gastric folds radiating from the edge. Radiology. 2008 Jan;246(1):33-48

Peptic ulcer disease, histology
Four zones:
– Necrotic debris
– Inflammatory exudate (neutrophils)
– Granulation tissue
– Fibrous scar

Helicobacter pylori
Adapted to gastric surface microenvironment
– Remains on the mucosal surface
– Urease, brakes urea to ammonia and bicarbonate (buffers acidity)
– Flagella
– Adhesins
– Cytotoxins (injure the epithelium releasing nutrients)
Mostly acquired in childhood
– Fecal-oral, oral-oral routes
Prevalence increases with age
Higher among minority populations

Helicobacter pylori, Steiner stain

Helicobacter pylori
Not clear why some develop non-atrophic gastritis while others develop atrophic gastritis
– Age at infection, environmental factors
– Inflammatory response genes polymorphisms
– H. pylori strains virulence
Responsible for most peptic ulcers, both gastric and duodenal
Contributes to the pathogenesis of gastric carcinomas and lymphomas

STOMACH1. Congenital anomalies
2. Gastritis
3. Hyperplastic gastropathies
– Ménétrier's disease
– Zollinger Ellison syndrome4. Neoplasms
---

Ménétrier's disease
Giant rugae on body and fundus
Oxyntic mucosa:– Foveolar hyperplasia
– Glandular atrophy
Excessive mucus secretion
Hypochlorhydria
May be precipitated by infection:– CMV, H. pylori
Overproduction of TGF-α
Stimulation of EGFR

Ménétrier's disease
Ménétrier's disease
Pediatric: Self limited
Adult: Protracted
May respond to:– Treatment for CMV, H. pylori
– Cetuximab (antibodies against EGFR)

Zollinger-Ellison syndrome
Gastrin-secreting tumors (gastrinomas):
– Hypergastrinemia
– Multiple peptic ulcers
Most gastrinomas are located in the pancreas
Hypergastrinemia causes:
– Hyperplasia of the oxyntic mucosa (parietal cells)
– Hyperplasia of endocrine cells
– Carcinoid tumors

Zollinger-EllisonParietal Cell Hyperplasia

STOMACH1. Congenital anomalies
2. Gastritis
3. Hyperplastic gastropathies
4. Neoplasms
– Benign (polyps)
• Hyperplastic
• Fundic gland
• Adenomatous
– Malignant
---
Benign tumors
Polyps: any nodule or mass that projects above the level of the surrounding mucosa
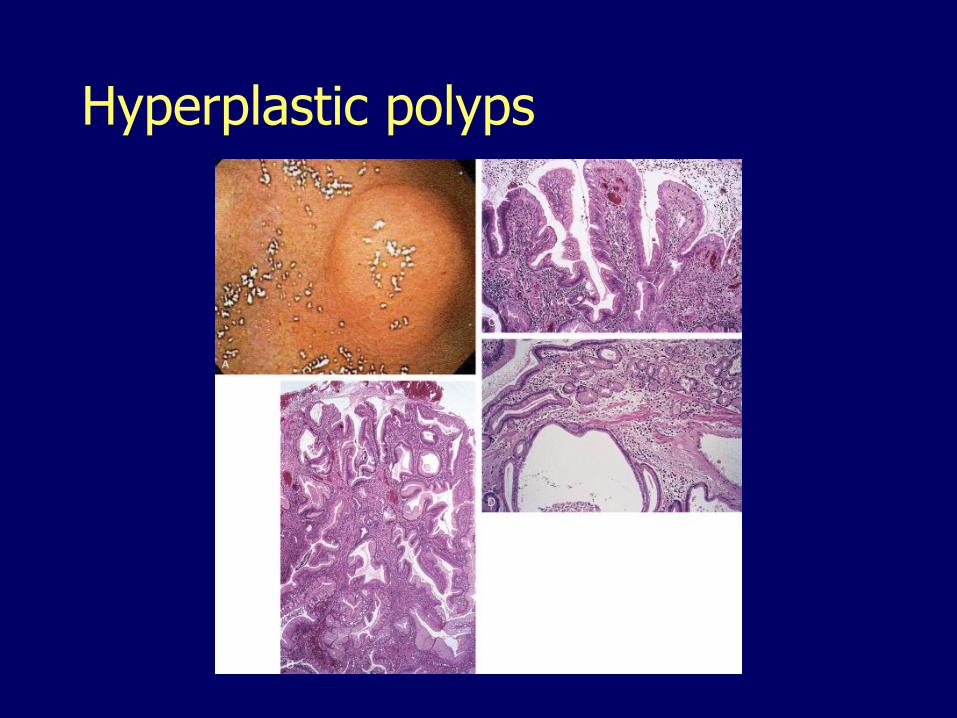
Hyperplastic polyps

Fundic gland polyp

Adenomatous polyps

Malignant gastric tumors
Adenocarcinoma 90-95%
Gastrointestinal stromal tumors
Lymphomas
Carcinoids

Gastric adenocarcinoma
In the US, incidence and mortality declined dramatically
Still the second cause of cancer death worldwide
More common in:– Lower socioeconomic groups
– Asians and Hispanics
Two histologic subtypes:– Intestinal type
– Diffuse type


Intestinal (expanding) typeForms glands

Intestinal (expanding) type
Grow with a cohesive expanding pattern
Mean age 55
Male-to-female ratio of 2:1
Related to environmental factors
Show geographic variation in incidence
Decreasing incidence

Intestinal (expanding) type
Related to Helicobacter pylori
Preceded by:
– Atrophy
– Intestinal metaplasia small intestinal type
– Intestinal metaplasia colonic type
– Low-grade dysplasia
– High-grade dysplasia
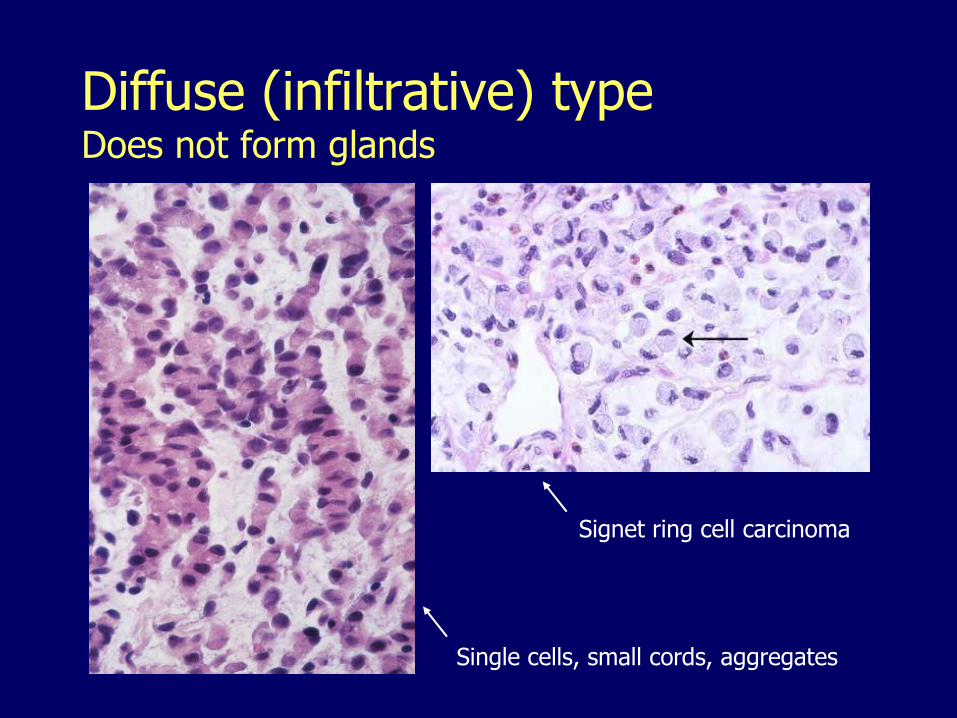
Diffuse (infiltrative) typeDoes not form glands
Signet ring cell carcinoma
Single cells, small cords, aggregates

Diffuse (infiltrative) type
Mean age 48
Equal male-to-female ratio
Not related to environmental factors
Little geographic variation
Mutations in CDH1, which encodes E-cadherin
No change in incidence
Not related to chronic gastritis or H. pylori
No clear premalignant conditions
Environmental influences
Infection by H. pylori
Lack of refrigeration, consumption of preserved, smoked, cured, pickled and salted foods
Water contamination with nitrates
Lack of fresh fruits and vegetables

Other risk factors
Partial gastrectomy
– Favors reflux of bilious fluid
Blood group A
Family history
Autoimmune gastritis

Gastric adenocarcinoma, gross
Exophytic
Flat
Depressed
Excavated
Ulcerated




Gastric adenocarcinoma, gross
Malignant ulcers have:
– Large size
– Heaped-up, beaded, indurated margins
– Shaggy, necrotic bases
Most intestinal-type carcinomas are located on the lesser curvature (incisura angularis)
The diffuse-type may not show a gross lesion or may induce with diffuse thickening of the stomach wall creating a leather bottle-like appearance (termed linitis plastica)

Linitis plastica
Surgical-tutor.org.uk

Gastric carcinoma, early vs. advanced
Early gastric carcinoma
– Confined to the mucosa and submucosa with or without lymph node involvement
– Excellent prognosis
Advanced gastric carcinoma
– Extends beyond the submucosa
– Very poor survival

Metastatic gastric carcinoma designations
Virchow’s node: left supraclavicular lymph node
Sister Mary Joseph’s node: periumbilical metastases
Krukenberg tumor: signet-ring cell type carcinoma metastatic to the ovary, usually bilateral

Sister Mary Joseph Nodule
CMAJ March 27, 2007 vol. 176 no. 7 doi: 10.1503/cmaj.060847

Krukenberg tumor
Hospital San Carlos, Madrid

Gastrointestinal stromal tumors (GIST)
Originate in interstitial cells of Cajal (the GI pacemaker) or from a common progenitor cell
Mutations of tyrosine kinase genes:– c-KIT (most common), or– Platelet-derived growth factor receptor alpha
Location:– Stomach (50-70%)– Small intestine (33%)– Colon (5-15%)
Prognosis:– Location– Size– Mitotic activity– Necrosis

GIST





























