Embed Size (px)
Citation preview

Healio.com The new online home of ORTHOPEDICS | Healio.com/Orthopedics
n Case Report
abstractFull article available online at Healio.com/Orthopedics. Search: 20120525-49
Because osseous abnormalities result in distal radioulnar joint instability, a sigmoid notch osteotomy is used to restore stability. This article describes a case of distal ra-dioulnar joint volar instability treated with sigmoid notch osteotomy of the volar rim.
A 22-year-old man presented with a 9-month history of right wrist pain with volar in-stability after a fall, which was treated conservatively. He reported a history of remote trauma when he was 7 years old but had been asymptomatic since then. Four months later, he underwent anatomical distal radioulnar joint ligament reconstruction at an-other hospital after a diagnosis of distal radioulnar joint instability, but the instability had persisted.
Computed tomography revealed dynamic volar subluxation of the ulnar head with hypoplasia and a flattened volar lip of the sigmoid notch. Therefore, a sigmoid notch osteotomy of the volar rim was performed. Postoperatively, an above-elbow cast was applied with forearm pronation for 6 weeks. Six months later, the patient had regained 60° of supination and 70° of pronation. He reported minor pain and no instability. Computed tomography scan at 6 months postoperatively revealed union of the oste-otomy site and confirmed the maintenance of reduction. The patient returned to work.
Drs Kim (Byung-Sung), Song, Jung, and Kim (Hyung-Tae) are from the Department of Orthopedic Surgery, Soonchunhyang University Bucheon Hospital, Wonmi-Gu, Bucheon-Si, Gyeonggi-Do, Republic of Korea.
Drs Kim (Byung-Sung), Song, Jung, and Kim (Hyung-Tae) have no relevant financial relationships to disclose.
Correspondence should be addressed to: Hyung-Tae Kim, MD, Department of Orthopedic Surgery, Soonchunhyang University Bucheon Hospital, 1174 Jung-1-dong, Wonmi-gu, Bucheon-si, Gyeonggi-do 420-767, Republic of Korea ([email protected]).
doi: 10.3928/01477447-20120525-49
Distal Radioulnar Joint Volar Instability After Ligament Reconstruction Failure Treated with Sigmoid Notch OsteotomyByung-Sung Kim, mD, PhD; hyun-SeoK Song, mD; Koo-hwang Jung, mD; hyung-Tae Kim, mD
e984
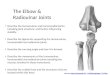
Figure: Diagram of the 3 osteotomies performed 2 mm proximal to the radiocarpal joint and 5 mm radial to the sigmoid notch.

JUNE 2012 | Volume 35 • Number 6
Distal raDioulnar Joint Volar instability | Kim et al
The sigmoid notch of the radius con-tributes to distal radioulnar joint sta-bility because the normal curvature
of the sigmoid notch plays an important role as a mechanical restraint to dorsal and vo-lar instability.1,2 This article describes a case in which congruency had been restored to the distal radioulnar joint via osteotomy of the sigmoid notch, and bony abnormalities in the distal ulnar head had resulted in joint instability. This article also describes the os-seous cause of joint instability and the pit-falls of soft tissue reconstruction for distal radioulnar joint volar instability associated with a hypoplastic ulnar head.
A sigmoid notch osteotomy was per-formed to reconstruct the distal radioul-nar joint volar rim for a hypoplastic ulnar head with persistent distal radioulnar joint volar instability after a failed distal radio-ulnar joint soft tissue reconstruction.
Case RepoRtA 22-year-old right-handed man pre-
sented with right wrist pain after a fall on his right hand. He reported a history of remote trauma at age 7 years but had been asymp-tomatic. He was treated conservatively with immobilization for 3 weeks. Four months later, he underwent anatomical distal radio-ulnar joint ligament reconstruction at anoth-er hospital under a diagnosis of distal radio-ulnar joint volar instability (Figure 1), but the instability had persisted postoperatively. He reported pain arising from the ulnar side of the wrist. Physical examination revealed volar subluxation of the ulnar head when he pushed his hand down on a table in forearm pronation and relocation of the ulnar head if the downward force was relieved.
Plain radiographs prior to ligament re-construction showed an absence of ulnar styloid, including the styloid base with mi-nus ulnar variance on the lesion side, but no bony abnormality existed on the contralater-al side. The ulnar head was small, but align-ment was within normal range. Magnetic resonance imaging revealed a dorsally sub-luxated ulnar head resting on the dorsal rim of the sigmoid notch and reconstructed dor-
sal and palmar radioulnar ligaments associ-ated with a triangular fibrocartilage com-plex ulnar side peripheral tear (Figure 2). Computed tomography scan revealed dorsal subluxation of the hypoplastic ulnar head, particularly in pronation, compared with the contralateral side according to criteria re-ported by Kihara et al,1 where the ulnar head in a normal distal radioulnar joint should lie
between 2 lines marking the dorsal and pal-mar borders of the radius (Figure 3). A flat-tened sigmoid notch was also measured by the sector angles of the articulating surface of the sigmoid notch of the radius. The cor-responding surface of the ulnar head facing toward the sigmoid notch was measured by the method of tangents, as reported by af Ekenstam and Hagert.3
Figure 1: Anteroposterior (A) and lateral (B) plain radiographs showing anatomical distal radioulnar joint liga-ment reconstruction 4 months after presentation.
Figure 2: Three-dimensional fat suppression spooiled gradient echo (A) and T1 fat suppression magnetic resonance imaging revealing an intact reconstructed distal radioulnar ligament (B).
1A 1B
2A 2B
e985

Healio.com The new online home of ORTHOPEDICS | Healio.com/Orthopedics
n Case Report
Therefore, the patient underwent sig-moid notch osteotomy. The palmar articular surface of the sigmoid notch was exposed through the volar approach between the ulnar neurovascular bundle and long flexor tendons. The reconstructed palmar distal radioulnar ligament was intact. Three os-teotomies were performed at 2 mm proxi-mal to the radiocarpal joint, the proximal articular margin of the sigmoid notch of the radioulnar joint, and 5 mm radial to the sigmoid notch (Figure 4). As the osteotomy was opened and reconstructed, the palmar distal radioulnar ligament tightened, the distal radioulnar joint was stable. The result-ing defect was filled with a bone graft from the volar radius and fixed with two 1.1-mm Kirschner wires.
Postoperatively, an above-elbow splint was applied in pronation for 4 weeks before range of motion exercises were started. At 6 months postoperatively, the patient had re-gained 60° of supination and 70° of prona-tion and reported minor pain.
The patient reported occasional epi-sodes of clicking but no instability. A com-puted tomography scan at 6 months post-operatively showed union of the osteotomy site and restoration of the sigmoid notch volar rim and confirmed the maintenance of reduction and congruency of the distal radioulnar joint (Figure 5). At 1-year fol-low-up, the patient had maintained range of motion with minor discomfort and no symptoms of instability. He returned to work and resumed recreational activities.
DisCussionDistal radial fractures are associated
with injuries to the distal radioulnar joint. Injury of the ligamentous stabilizers and sigmoid notch can cause distal radioulnar joint instability.4,5 The radioulnar ligaments are the primary stabilizers of the wrist joint, and the ulnocarpal complex, extensor carpi subsheath, and interosseous membrane are the secondary stabilizers.6 Although the primary ligamentous supports were sectioned, distal radioulnar joint stabil-ity can be maintained with intact second-
ary stabilizers, meaning bony and ligamentous restraints contribute to distal radioulnar joint stability.7 A flattened anatomic variant of sigmoid notch shape is associated with an un-stable distal radioulnar joint.8 Distal radioulnar joint volar instability with a flat sigmoid notch can be treated with sig-moid notch osteoplasty. Although distal radioul-nar ligament reconstruc-tion can be performed, persistent instability occurs if the sigmoid notch is deficient. Many salvage procedures to treat symptomatic and degenerate distal radioulnar joints have been described, including the Darrach pro-cedure, hemiresection interposition arthro-plasty, and the Sauve-Kapandji procedure. These procedures may result in reduced grip strength, painful ulnar shaft instability, and reossification.
This article describes a case of a distal ra-dioulnar joint volar instability after failure of a distal radioulnar joint ligament reconstruc-
tion using sigmoid notch osteotomy. Due to the patient’s young age and the integrity of the soft tissue joint supports, joint reduction was performed to avoid salvage procedures. The patient was treated initially with distal radioulnar joint ligament reconstruction to reduce the ulnar head into the sigmoid notch. Distal radioulnar joint subluxation persisted postoperatively when the patient attempted to push his hand downward on a
Figure 3: Axial computed tomography scan showing no definite ulnar head dislocation, hypoplasia, a flat-tened sigmoid notch volar lip, and no instability during 60° of supination (A) or pronation (B).
Figure 4: Diagram of the 3 osteotomies performed 2 mm proximal to the radiocarpal joint, the proximal margin of the sigmoid notch, and 5 mm radial to the sigmoid notch (A). Three-dimensional computed tomography scan of the sigmoid notch osteotomy (B).
3A 3B
4A 4B
e986

JUNE 2012 | Volume 35 • Number 6
Distal raDioulnar Joint Volar instability | Kim et al
table in forearm pronation. Distal radioulnar joint ligament stability can be achieved by appropriate bony dimension of the distal radioulnar joint. Although the ulnar head and sigmoid notch come in contact in nor-mal forearm rotation, the relative range of contact points per ulnar head dimension between the normal and hypoplastic ulnar head is different. A hypoplastic ulnar head does not match its sigmoid notch, which has a wider range of contact points with the sigmoid notch. Therefore, sigmoid notch os-teotomy can reduce its relative bony dimen-sion corresponding with the ulnar head. In addition, it increases distal radioulnar joint ligament tension by lateralization of the cen-ter of rotation.
Many soft tissue reconstruction proce-dures for distal radioulnar joint instability are complicated and require a donor graft tendon. The current bony procedures for distal radioulnar joint instability are salvage procedures that aim to maximize function and minimize pain and are indicated for pa-tients with degenerative arthritis. Movement at the distal radioulnar joint consists of ro-tation. A gliding component is necessary to achieve complete pronation and supination range of motion. This gliding component is evident because the curvature radius of the sigmoid notch articular surface and that of the distal ulna are different.
Tolat et al8 reported that the average radius of the seat of the sigmoid notch in
50 cadaveric wrists was 19 mm, which is in contrast to that of the ulnar surface, which was 10 mm. At extreme supination, the joint has a small area of contact at the volar aspect of the sigmoid notch.7 This area is ,10% of the total joint surface. Tolat et al8 classified the osseous anatomy of the distal radioulnar joint into 12 types based on the angle of inclination of the joint surface relative to the ulnar shaft and the cross-sectional shape of the sigmoid notch. This study suggested that a flat face would be more unstable than the other shapes, which had more pronounced volar lips. However, they were able to identify a discrete palmar osteocartilaginous lip in all but 1 specimen in this group. The palmar radioulnar ligament attaches to this prominence and is extra-articular. A subset of 10 wrists with a large lip under-went mechanical testing. The lip provided a stable buttress to volar dislocation in all rotation positions. The stability was pre-served except when complete disruption of the interosseous ligament and palmar radioulnar ligament occurred or when the volar lip was fractured.
Osteoplasty reconstitutes the volar lip so that it acts as a buttress against volar instability. The volar radioulnar ligament is preserved and is effectively tightened by augmenting the volar cortical lip. The indications for this procedure are limited. The patients should have pure volar insta-
bility in supination, a flat sigmoid notch with a deficiency in the volar osteocarti-laginous lip, and no secondary degenera-tion. Osseous reconstruction of the volar buttress is an option for volar instability and may be used in other pathologies, such as distal radius fractures or com-bined with other procedures, such as tri-angular fibrocartilage complex repair.9,10
ConClusionThe volar lip of the sigmoid notch plays
an important role as a bony restraint to vo-lar distal radioulnar joint instability associ-ated with distal ulnar hypoplasia. The cur-rent patient, whose symptoms were not re-lieved by anatomical distal radioulnar joint ligament reconstruction, was treated with a sigmoid notch osteotomy to restore distal radioulnar joint stability.
RefeRenCes 1. Kihara H, Short WH, Werner FW, Fortino
MD, Palmer AK. The stabilizing mechanism of the distal radioulnar joint during prona-tion and supination. J Hand Surg Am. 1995; 20(6):930-936.
2. Tsai PC, Paksima N. The distal radioulnar joint. Bull NYU Hosp Jt Dis. 2009; 67(1):90-96.
3. af Ekenstam F, Hagert CG. Anatomical stud-ies on the geometry and stability of the dis-tal radio ulnar joint. Scand J Plast Reconstr Surg. 1985; 19(1):17-25.
4. Thomas J, Large R, Tham SK. Sigmoid notch osteotomy for posttraumatic dorsal dislocation of the distal radioulnar joint: a case report. J Hand Surg Am. 2006; 31(10):1601-1604.
5. Kleinman WB. Distal radius instability and stiffness: common complications of distal radi-us fractures. Hand Clin. 2010; 26(2):245-264.
6. Palmer AK, Werner FW. The triangular fibro-cartilage complex of the wrist--anatomy and function. J Hand Surg Am. 1981; 6(2):153-162.
7. Bowers WH. Instability of the distal radioulnar articulation. Hand Clin. 1991; 7(2):311-327.
8. Tolat AR, Stanley JK, Trail IA. A cadaveric study of the anatomy and stability of the distal radioulnar joint in the coronal and transverse planes. J Hand Surg Br. 1996; 21(5):587-594.
9. Tham SK, Bain GI. Sigmoid notch osseous reconstruction. Tech Hand Up Extrem Surg. 2007; 11(1):93-97.
10. Wallwork NA, Bain GI. Sigmoid notch os-teoplasty for chronic volar instability of the distal radioulnar joint: a case report. J Hand Surg Am. 2001; 26(3):454-459.
Figure 5: Computed tomography scan 6 months postoperatively showing union of the osteotomy site and a maintained ulnar head reduction (A). Photograph 12 months later. The patient regained 60° of supination and 70° of pronation with minor pain but no instability (B)
5A 5B
e987