Embed Size (px)
Citation preview

Code:Page:
DANIEL MERCADO MEDICAL CENTERSerology and Immunology
Standard Operating Procedure
Issue Date: Revision Date:Revision No. 0.0
ELECSYS 2010
Engineered for continuous, random access operation, the Elecsys 2010 System is the solution for medium to large volume laboratories that want to maximize productivity and efficiency. The Elecsys 2010 System offers simplicity, flexibility and STAT capabilities, plus it can be adapted to the changing needs of an aggressive laboratory testing environment.
A true random access system, the Elecsys 2010 provides automatic opening and closing of reagent caps, as well as a temperature controlled reagent compartment, which maximizes kit stability and allows storage of kits on the instrument. For maximum flexibility, the Elecsys 2010 System can be equipped with a sample disk or a rack handling system.
PRINCIPLE OF THE MACHINE IN USE:
Electrochemiluminescence (ECL) technology, found exclusively on the Elecsys 2010 and MODULAR ANALYTICS E 170 systems, cobas® 6000 analyzer series and the cobas e 411 analyzer is so sensitive it can parallel the sensitivity of PCR3. This is the equivalent of reliably finding one red M&M® in an Olympic-sized pool of blue ones—in just 18 minutes.
ECL is a unique and highly sensitive luminescence (light) detection system that amplifies the signal you want and reduces any signals you don't want to deliver unmatched low-end sensitivity and broad dynamic measuring ranges.
The measuring cell uses an amplified signal to detect ultra-low concentrations of analyte. By precisely controlling electrically-initiated reactions, ECL technology virtually eliminates unnecessary repeats and reruns, providing accurate results the first time. Through the use of a constant electrical field to stimulate the electrochemical luminescent reaction, ECL provides a stable, constant light output throughout the entire measurement cycle. As long as the electrical field is on, the light is on, making it easy to take many measurements. Twenty measurements in 400 milliseconds are combined to produce one determination. The high number of measurements improves precision and reliability of the result and adds to the overall sensitivity of the assay.
Prepared by:
Faminialagao, Kate
Checked by:
Jon Paul Reyes RMT
Noted by:
Rozani Odono Navarro MD, FPSP
Medical Technologist Chief Medical Technologist PathologistCode:Page:
DANIEL MERCADO MEDICAL CENTERSerology and Immunology
Standard Operating Procedure
Issue Date: Revision Date:Revision No. 0.0
Separation of signal from background noise is the key to determining sensitivity. ECL makes it possible to differentiate true signals from background noise. By enhancing the signal while reducing the noise, ECL improves sensitivity, especially at ultra-low levels. This is critical, particularly at the low end of sensitivity where the ability to measure precisely becomes vital to clinical decision-making. Improving the precision of an assay improves the assay's sensitivity, making it possible to provide numbers and results that are useful to the physician. At low measuring ranges, the clinical decision point can rest on a small but clinically important deviation. Sensitivity becomes vitally important. ECL leaves the light on long enough to obtain precise counts. Greater precision drives better sensitivity. Sensitivity drives better clinical decisions and improved patient outcomes.
PROCEDURE:
Before start up of machine check the following: Wash is filled (30 mL Syswash + 3 liters distilled water) Liquid waste is empty Solid waste is empty Presence of reaction caps and tips 2 sets of Pro cell and Clean cell Reagents are in place and partially open only
(START UP) 1. Pull up breaker of machine at the side of elecsys 20102. Press power buttons at the front of the machine.3. Wait for 7 minutes.4. Touch the screen at the appearance of Elecsys 20105. Touch Inventory (located at the upper left corner of the screen) 6. Touch reagent scan upon machine is on standby.
* Take note that the barcode of the reagents are not scratched and are facing the outer part of the reagent rack.
7. Wait until machine is done.
(PATIENT AUTOMATIC ENTRY)1. Place samples in sample rack with barcode facing the outside area2. Place stopper tube at end of sample cups3. Place sample rack in position4. Press status 5. Select open requests6. Press delete7. Start
(PATIENT MANUAL ENTRY)1. Touch Order2. Press ID number assigned to patient 3. Place position number where the sample cup is to be placed in sample rack4. Press the test to be selected as per request of the patient5. Select register.6. Press start button.7. touch resume.
Prepared by:
Faminialagao, Kate
Checked by:
Jon Paul Reyes RMT
Noted by:
Rozani Odono Navarro MD, FPSP
Medical Technologist Chief Medical Technologist PathologistCode:Page:
DANIEL MERCADO MEDICAL CENTERSerology and Immunology
Standard Operating Procedure
Issue Date: Revision Date:Revision No. 0.0
(CONTROLS- ENTERING NEW SETS OF CONTROLS)1. Utility2. Control definition3. enter bar code4. BC card scan5. Controls6. Select the control entered7. OK8. Select the control chosen9. active10. OK11. Place controls in position, yellow 1st before brown12. start13. resume
(CONTROLS – USING OLD CONTROLS)1. Place controls on sample rack, yellow 1st before brown2. start3. resume
(CALIBRATION OF HEPATITIS REAGENTS) 1. Place calibrators, white 1st before black2. Reagents should be in position3. start
(CALIBRATION OF REAGENTS WITH NEW BAR CODE)1. Machine should be on standby2. Utility3. Calibration definition4. enter bar code5. BC card scan6. Place calibrators in position white 1st before black7. Select status8. Select calibrator9. Select the test with new calibration10. Select the code of the new calibrator11. Place the position number where the calibrator is placed12. Select register13. Start
*****when performing all these, make sure machine is on STAND BY first*****
****do not remove reagents unless machine is on STAND BY first****
Prepared by:
Faminialagao, KateMedical Technologist
Checked by:
Jon Paul Reyes RMTChief Medical Technologist
Noted by:
Rozani Odono Navarro MD, FPSPPathologist
Code:Page:
DANIEL MERCADO MEDICAL CENTERSerology and Immunology
Standard Operating Procedure
Issue Date: Revision Date:Revision No. 0.0
THE TESTS:
TSH (Thyrotropin)
INTENDED USE: Immunoassay for the in vitro quantitative determination of thyrotropin in human serum and plasma. The electrchemiluminescence immunoassay “ECLIA” is intended for use on elecsys and cobas e immunoassay analyzers.
SUMMARY: Thyroid stimulating hormone (TSH, thyrotropin) is a glycoprotein having a molecular weight of approximately 30000 daltons and consists of 2 subunits. The β-subunit carries the TSH-specific immunological and biological information, whereas the α-chain carries species-specific information and has an identical amino acid sequence to the α-chains of LH. FSH, and hCG. TSH is formed in specific basophile cells of the anterior pituitary and is subject to a circadian secretion sequence. The hypophyseal release of TSH (thyrotropic hormone) is the central regulating mechanism for the biological action of thyroid hormones. TSH has a stimulating action in all stages of the thyroid hormone formation and secretion; it also has a proliferative effect. The determination of TSH serves as the initial test in thyroid diagnostics. Even very slight changes in the concentrations of the free thyroid hormones bring about much greater opposite changes in the TSH level. Accordingly, TSH is a very sensitive and specific parameter for assessing thyroid function and is particularly suitable for the early detection of exclusion of disorders in the central regulating circuit between the hypothalamus, pituitary and thyroid. The Elecsys TSH assay employs monoclonal antibodies specifically directed against human TSH. The antibodies labeled with ruthenium complex consist of a chimeric construct from human and mouse-specific components. As a result, interfering effects due to HAMA (human anti-mouse antibodies) are largely eliminated.
TEST PRINCIPLE: Sandwich principle. Total duration of assay is 18 minutes. 1st incubation: 50ul of sample, a biotinylated monoclonal TSH-specific antibody and a monoclonal TSH-
specific antibody labeled with ruthenium complex react to form a sandwich complex. 2nd incubation: After addition of streptavidin-coated microparticles, the complex becomes bound to the
solid phase via interaction of biotin and streptavidin. The reaction mixture is aspirated into the measuring cell where the microparticles are magnetically
captured onto the surface of the electrode. Unbound substances are the removed with ProCell. Application of a voltage to the electrode then induces chemiluminescent emission which is measured by a photomultiplier.
Results are determined via a calibration curve which is instrument-specifically generated by 2-point calibration and a master curve via a reagent barcode.
PRECAUTIONS AND WARNINGS: for in vitro diagnostic use. Exercise the normal precautions required for handling all laboratory reagents. Disposal of all waste material should be in accordance with local guidelines. Avoid formation of foam with all reagents and sample types (specimen, calibrators, and controls).
STORAGE AND STABILITY: Store at 2-8 degrees Celsius. Store the Elecsys TSH reagent kit in UPRIGHT to ensure complete availability of the microparticles during automatic mixing prior to use. Stability:
Unopened at 2-8 degrees Celsius Up to the stated expiration dateAfter opening at 2-8 degrees Celsius 12 weeksOn Elecsys 2010 8 weeks
Prepared by:
Faminialagao, KateMedical Technologist
Checked by:
Jon Paul Reyes RMTChief Medical Technologist
Noted by:
Rozani Odono Navarro MD, FPSPPathologist

Code:Page:
DANIEL MERCADO MEDICAL CENTERSerology and Immunology
Standard Operating Procedure
Issue Date: Revision Date:Revision No. 0.0
SPECIMEN COLLECTION AND PREPARATION:
Serum collected using standard sampling tubes or tubes containing separating gel.Li-, Na-, NH4
+-heparin, K3-EDTA, sodium citrate and sodium fluoride/potassium oxalate plasma.Stable for 7 days at 2-8°C, 1 month at -20°C. Freeze only once. Sample collection systems from various manufacturers may contain differing materials which could affect the test results in some cases. When processing samples in primary tubes (sample collection systems), follow the instructions of the tube manufacturer. Centrifuge samples containing precipitates before performing the assat. DO NOT USE HEAT INACTIVATED SAMPLES. Do not use samples and controls stabilized with azide. Ensure the patients’ samples, calibrators, and controls are at ambient temperature (20-25°C) before measurement. Because of possible evaporation effects, samples, calibrators, and controls on the analyzer should be measured within 2 hours.
CALIBRATION FREQUENCY: calibration must be performed once per reagent lot using fresh reagent (i.e not more than 24 hours since the kit was registered on the analyzer) Renewed calibration is recommended for Elecsys 2010as follows:
After 1 month (28 days) when using the same reagent lot After 7 days (when using the same reagent kit on the analyzer)
MEASURING RANGE: 0.005-100.0 uIU/mL (defined by the lower detection limit and the maximum of the master curve). The functional sensitivity is 0.014 uIU/mL. Values below the detection limit are reported as < 0.005 uIU/mL. Values above the measuring range are reported as >100 uIU/mL (or up to 1000 uIU/mL for 10-fold diluted samples).
EXPECTED VALUES: 0.27-4.2 uIU/Ml
Prepared by:
Faminialagao, KateMedical Technologist
Checked by:
Jon Paul Reyes RMTChief Medical Technologist
Noted by:
Rozani Odono Navarro MD, FPSPPathologist
Code:Page:
DANIEL MERCADO MEDICAL CENTERSerology and Immunology
Standard Operating Procedure
Issue Date: Revision Date:Revision No. 0.0
T3 (Triiodothyronine)
INTENDED USE: Immunoassay for the in vitro quantitative determination of total triiodothyronine in human serum and plasma. The electrchemiluminescence immunoassay “ECLIA” is intended for use on elecsys and cobas e immunoassay analyzers.
SUMMARY: Triiodothyronine (T3) is the hormone principally responsible for the development of the effects of the thyroid hormones on the various target organs. T3 ( 3,5,3,’-triiodothyronine is mainly formed extrathyroidally, particularly in the liver, by enzymatic 5’-deiodination of T4. Accordingly, the T3 concentration in serum is more a reflection of functional state of the peripheral tissue than the secretory performance of the thyroid gland. A reduction in the conversion of T4 to T3 results in a decreased in the T3 concentration. It occurs under the influence of medicaments such as propanolol, glucocorticoids, or amiodarone and in server non-thyroidal illness (NTI), and is referred to as “low T3 syndrome”. As with T4, over 99% of T3 is bound with transport proteins. However the affinity of T3 is around 10-fold lower. The determination of T3 is utilized in the diagnosis of T3-hyperthyroiddism, the detection of early stages of hyperthyroidism and for indicating a diagnosis of thyrotoxicosis factitia. The Elecsys T3 assay employs a competitive test principle with polyclonal antibodies specificvally directed against T3. Endogenous T3, released by the action of 8-anilino-1-naphthalene sulfonic acid (ANS), competes with the added biotinylated T3-derivative for the binding sites on the antibodies labeled with the ruthenium complex.
TEST PRINCIPLE: Sandwich principle. Total duration of assay is 18 minutes. 1st incubation: 30ul of sample, and a T3-specific antibody labeled with ruthenium complex; bound T3 is
release from the binding proteins in the sample by ANS. 2nd incubation: After addition of streptavidin-coated and biotinylated T3, the still-free binding sites of the
labeled antibody become occupied, with formation of an antibody-hapten complex. The entire complex becomes bound to the solid phase via interaction of biotin and streptavidin.
The reaction mixture is aspirated into the measuring cell where the microparticles are magnetically captured onto the surface of the electrode. Unbound substances are the removed with ProCell. Application of a voltage to the electrode then induces chemiluminescent emission which is measured by a photomultiplier.
Results are determined via a calibration curve which is instrument-specifically generated by 2-point calibration and a master curve via a reagent barcode.
PRECAUTIONS AND WARNINGS: for in vitro diagnostic use. Exercise the normal precautions required for handling all laboratory reagents. Disposal of all waste material should be in accordance with local guidelines. Avoid formation of foam with all reagents and sample types (specimen, calibrators, and controls).
STORAGE AND STABILITY: Store at 2-8 degrees Celsius. Store the Elecsys T3 reagent kit in UPRIGHT to ensure complete availability of the microparticles during automatic mixing prior to use. Stability:
Unopened at 2-8 degrees Celsius Up to the stated expiration dateAfter opening at 2-8 degrees Celsius 12 weeksOn Elecsys 2010 8 weeks
SPECIMEN COLLECTION AND PREPARATION:
Serum collected using standard sampling tubes or tubes containing separating gel.Li-, Na-, NH4
+-heparin, K3-EDTA, sodium citrate and sodium fluoride/potassium oxalate plasma.Stable for 7 days at 2-8°C, 1 month at -20°C. Freeze only once. Sample collection systems from various manufacturers may contain differing materials which could affect the test results in some cases. When processing samples in primary tubes (sample collection systems), follow the instructions of the tube manufacturer. Centrifuge samples containing precipitates before performing the assat. DO NOT USE HEAT INACTIVATED SAMPLES. Do not use samples and controls stabilized with azide. Ensure the patients’ samples, calibrators, and controls are at ambient temperature (20-25°C) before measurement. Because of possible evaporation effects, samples, calibrators, and controls on the analyzer should be measured within 2 hours.
Prepared by:
Faminialagao, KateMedical Technologist
Checked by:
Jon Paul Reyes RMTChief Medical Technologist
Noted by:
Rozani Odono Navarro MD, FPSPPathologist
Code:Page:
DANIEL MERCADO MEDICAL CENTERSerology and Immunology
Standard Operating Procedure
Issue Date: Revision Date:Revision No. 0.0
CALIBRATION FREQUENCY: calibration must be performed once per reagent lot using fresh reagent (i.e not more than 24 hours since the kit was registered on the analyzer) Renewed calibration is recommended for Elecsys 2010as follows:
After 1 month (28 days) when using the same reagent lot After 7 days (when using the same reagent kit on the analyzer)
CALCULATION: the analyzer automatically calculates the analyte concentration of each sample (either in nmol/L, ng/mL or ng/dL)Conversion factors: nmol/L x 0.651 = ng/mL
nmol/L x 65.09998 = ng/dLng/mL x 1.536 = nmol/L
MEASURING RANGE: 0.300-10.00nmol/L or 0.195-6.51 ng/dL (defined by the lower detection limit and the maximum of the master curve) Values below the detection limit are reported as < 0.300 nmol/L or <0.195 ng/dL. Values above the measuring range are reported as >10nmol/L or > 6.51 ng/dL.
EXPECTED VALUES: 1.3-3.1 nmol/L or 0.8-2.0 ng/mL: euthyroid.
Prepared by:
Faminialagao, KateMedical Technologist
Checked by:
Jon Paul Reyes RMTChief Medical Technologist
Noted by:
Rozani Odono Navarro MD, FPSPPathologist
Code:Page:
DANIEL MERCADO MEDICAL CENTERSerology and Immunology
Standard Operating Procedure
Issue Date: Revision Date:Revision No. 0.0
T4 (Thyroxine)
INTENDED USE: Immunoassay for the in vitro quantitative determination of thyroxine in human serum and plasma. The electrchemiluminescence immunoassay “ECLIA” is intended for use on elecsys and cobas e immunoassay analyzers.
SUMMARY: The hormone thyroxine (T4) is the main product secreted by the thyroid gland and is an integral component of the hypothalamus-anterior pituitary-thyroid regulating system. It has the function of anabolically influencing metabolism. Thyroxine is formed in the coupling reaction of 2 DIT molecules(3,5-diiodotyrosine) in the thyroid gland. It is stored bound to thyroglobulin in the lumina of the thyroid follicles and is secreted as required under the influence of TSH. The major part (>99%) of the total thyroxine (T4) in serum is present in protein bound form. As the concentrations in the transport proteins in serum are subject to endogenous and exogenous effects, the status of the binding proteins must also be taken into account in the assessment of the thyroid hormone concentration in serum. If this is ignored, changes in the binding proteins (e.g. due to estrogen containing preparations, during pregnancy of in presence of nephritic syndrome, etc.) can lead to erroneous assessments of the thyroid metabolic state. The determination of T4 can be utilized for the following indications: The detection of hyperthyroidism, the detection of primary and secondary hypothyroidism, and the monitoring of TSH suppression therapy.
TEST PRINCIPLE: Sandwich principle. Total duration of assay is 18 minutes. 1st incubation: 15ul of sample, and a T4-specific antibody labeled with ruthenium complex; bound T4 is
release from the binding proteins in the sample by ANS. 2nd incubation: After addition of streptavidin-coated and biotinylated T4, the still-free binding sites of the
labeled antibody become occupied, with formation of an antibody-hapten complex. The entire complex becomes bound to the solid phase via interaction of biotin and streptavidin.
The reaction mixture is aspirated into the measuring cell where the microparticles are magnetically captured onto the surface of the electrode. Unbound substances are the removed with ProCell. Application of a voltage to the electrode then induces chemiluminescent emission which is measured by a photomultiplier.
Results are determined via a calibration curve which is instrument-specifically generated by 2-point calibration and a master curve via a reagent barcode.
PRECAUTIONS AND WARNINGS: for in vitro diagnostic use. Exercise the normal precautions required for handling all laboratory reagents. Disposal of all waste material should be in accordance with local guidelines. Avoid formation of foam with all reagents and sample types (specimen, calibrators, and controls).
STORAGE AND STABILITY: Store at 2-8 degrees Celsius. Store the Elecsys T4 reagent kit in UPRIGHT to ensure complete availability of the microparticles during automatic mixing prior to use. Stability:
Unopened at 2-8 degrees Celsius Up to the stated expiration dateAfter opening at 2-8 degrees Celsius 12 weeksOn Elecsys 2010 8 weeks
Prepared by:
Faminialagao, KateMedical Technologist
Checked by:
Jon Paul Reyes RMTChief Medical Technologist
Noted by:
Rozani Odono Navarro MD, FPSPPathologist

Code:Page:
DANIEL MERCADO MEDICAL CENTERSerology and Immunology
Standard Operating Procedure
Issue Date: Revision Date:Revision No. 0.0
SPECIMEN COLLECTION AND PREPARATION:
Serum collected using standard sampling tubes or tubes containing separating gel.Li-, Na-, NH4
+-heparin, K3-EDTA, sodium citrate and sodium fluoride/potassium oxalate plasma.Stable for 7 days at 2-8°C, 1 month at -20°C. Freeze only once. Sample collection systems from various manufacturers may contain differing materials which could affect the test results in some cases. When processing samples in primary tubes (sample collection systems), follow the instructions of the tube manufacturer. Centrifuge samples containing precipitates before performing the assay. DO NOT USE HEAT INACTIVATED SAMPLES. Do not use samples and controls stabilized with azide. Ensure the patients’ samples, calibrators, and controls are at ambient temperature (20-25°C) before measurement. Because of possible evaporation effects, samples, calibrators, and controls on the analyzer should be measured within 2 hours. The Elecsys T4 assay employs a competitive test principle with polyclonal antibodies specifically directed against T4. Endogenous T4, released by the action of 8-anilino-1-naphthalene sulfonic acid (ANS), competes with the added biotinylated T4-derivative for the binding sites on the antibodies labeled with the ruthenium complex.
CALIBRATION FREQUENCY: calibration must be performed once per reagent lot using fresh reagent (i.e not more than 24 hours since the kit was registered on the analyzer) Renewed calibration is recommended for Elecsys 2010as follows:
After 1 month (28 days) when using the same reagent lot After 7 days (when using the same reagent kit on the analyzer)
CALCULATION: the analyzer automatically calculates the analyte concentration of each sample (either in nmol/L, ug/dL or ug/L)Conversion factors: nmol/L x 0.077688 = ug/dL
ug/dL x 12.872 = nmol/Lnmol/L x 0.77688 = ug/L
MEASURING RANGE: 5.40-320.00nmol/L or 0.420-24.86 ug/dL (defined by the lower detection limit and the maximum of the master curve) Values below the detection limit are reported as < 5.40 nmol/L or <0.420 ug/dL. Values above the measuring range are reported as >320.0nmol/L or > 24.86 ug/dL.
EXPECTED VALUES: 66-181 nmol/L or 5.1-14.1 ug/dL
Prepared by:
Faminialagao, KateMedical Technologist
Checked by:
Jon Paul Reyes RMTChief Medical Technologist
Noted by:
Rozani Odono Navarro MD, FPSPPathologist
Code:Page:
DANIEL MERCADO MEDICAL CENTERSerology and Immunology
Standard Operating Procedure
Issue Date: Revision Date:Revision No. 0.0
FT3 (Free Triiodothyronine)
INTENDED USE: Immunoassay for the in vitro quantitative determination of free triiodothyronine in human serum and plasma. The electrchemiluminescence immunoassay “ECLIA” is intended for use on elecsys and cobas e immunoassay analyzers.
SUMMARY: Triiodothyronine is one of the thyroid hormones present in serum which regulate metabolism. Determination of this hormone concentration is important for the diagnostic differentiation of euthyroid, hyperthyroid and hypothyroid states. The major fraction of total Triiodothyronine is bound to the transport proteins (TBG, prealbumin, albumin). Free Triiodothyronine (fT3) is the physiologically active form of the thyroid hormone Triiodothyronine (T3). The determination of free T3 has the advantage of being independent of changes in the concentrations and binding properties of the binding protein, additional determination of a binding parameter (T-uptake, TBG) is therefore unnecessary. The sequential testing procedure and the use of a labeled antibody reduced the possibility of interference due to altered binding properties of the serum as can occur with assays employing labeled antigen (analog method). A variety of methods are available for estimating the free thyroid hormone levels. The direct measurement of fT3 and fT4 via equilibrium dialysis or ultrafiltration is mainly used as a reference method for standardizing the immunological procedures generally used for routine diagnostic purposes. In the Elecsys FT3 test the determination of free Triiodothyronine is made with the aid of a specific anti-T3 antibody labeled with ruthenium complex.
TEST PRINCIPLE: Sandwich principle. Total duration of assay is 18 minutes. 1st incubation: 15ul of sample, and an anti-T3-specific antibody labeled with ruthenium complex. 2nd incubation: After addition of biotinylated T3 and streptavidin-coated microparticles, the still-free
binding sites of the labeled antibody become occupied, with formation of an antibody-hapten complex. The entire complex becomes bound to the solid phase via interaction of biotin and streptavidin.
The reaction mixture is aspirated into the measuring cell where the microparticles are magnetically captured onto the surface of the electrode. Unbound substances are the removed with ProCell. Application of a voltage to the electrode then induces chemiluminescent emission which is measured by a photomultiplier.
Results are determined via a calibration curve which is instrument-specifically generated by 2-point calibration and a master curve via a reagent barcode.
PRECAUTIONS AND WARNINGS: for in vitro diagnostic use. Exercise the normal precautions required for handling all laboratory reagents. Disposal of all waste material should be in accordance with local guidelines. Avoid formation of foam with all reagents and sample types (specimen, calibrators, and controls).
STORAGE AND STABILITY: Store at 2-8 degrees Celsius. Store the Elecsys FT3 reagent kit in UPRIGHT to ensure complete availability of the microparticles during automatic mixing prior to use. Stability:
Unopened at 2-8 degrees Celsius Up to the stated expiration dateAfter opening at 2-8 degrees Celsius 12 weeksOn Elecsys 2010 6 weeks
Prepared by:
Faminialagao, KateMedical Technologist
Checked by:
Jon Paul Reyes RMTChief Medical Technologist
Noted by:
Rozani Odono Navarro MD, FPSPPathologist
Code:Page:
DANIEL MERCADO MEDICAL CENTERSerology and Immunology
Standard Operating Procedure
Issue Date: Revision Date:Revision No. 0.0
SPECIMEN COLLECTION AND PREPARATION:
Serum collected using standard sampling tubes or tubes containing separating gel.Li-, Na-, NH4
+-heparin, K3-EDTA, sodium citrate and sodium fluoride/potassium oxalate plasma.Stable for 7 days at 2-8°C, 1 month at -20°C. Freeze only once. Sample collection systems from various manufacturers may contain differing materials which could affect the test results in some cases. When processing samples in primary tubes (sample collection systems), follow the instructions of the tube manufacturer. Centrifuge samples containing precipitates before performing the assay. DO NOT USE HEAT INACTIVATED SAMPLES. Do not use samples and controls stabilized with azide. Ensure the patients’ samples, calibrators, and controls are at ambient temperature (20-25°C) before measurement. Because of possible evaporation effects, samples, calibrators, and controls on the analyzer should be measured within 2 hours. The Elecsys T4 assay employs a competitive test principle with polyclonal antibodies specifically directed against T4. Endogenous T4, released by the action of 8-anilino-1-naphthalene sulfonic acid (ANS), competes with the added biotinylated T4-derivative for the binding sites on the antibodies labeled with the ruthenium complex.
CALIBRATION FREQUENCY: calibration must be performed once per reagent lot using fresh reagent (i.e not more than 24 hours since the kit was registered on the analyzer) Renewed calibration is recommended for Elecsys 2010as follows:
After 1 month (28 days) when using the same reagent lot After 7 days (when using the same reagent kit on the analyzer)
CALCULATION: the analyzer automatically calculates the analyte concentration of each sample (either in pmol/L, pg/mL or ng/dL)Conversion factors: pmol/L x 0.651 = pg/mL
pg/mL x 1.536 = pmol/Lpg/mL x 0.1 = ng/dL
MEASURING RANGE: 0.4-50.00 pmol/L or 0.260-32.55 pg/mL (defined by the lower detection limit and the maximum of the master curve) Values below the detection limit are reported as < 0.400 pmol/L or <0.260 pg/mL. Values above the measuring range are reported as >50.0 pmol/L or > 32.55 pg/mL.
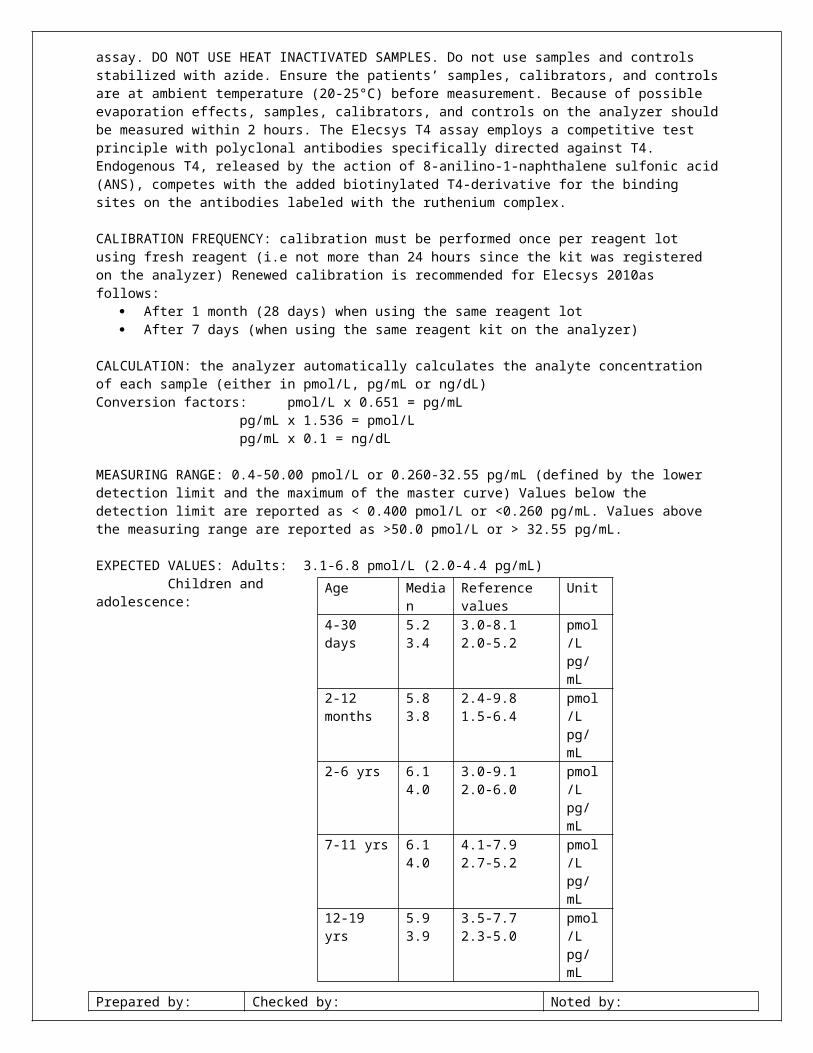
EXPECTED VALUES: Adults: 3.1-6.8 pmol/L (2.0-4.4 pg/mL) Children and adolescence:
Prepared by:
Faminialagao, KateMedical Technologist
Checked by:
Jon Paul Reyes RMTChief Medical Technologist
Noted by:
Rozani Odono Navarro MD, FPSPPathologist
Age Median Reference values Unit4-30 days 5.2
3.43.0-8.12.0-5.2
pmol/Lpg/mL
2-12 months
5.83.8
2.4-9.81.5-6.4
pmol/Lpg/mL
2-6 yrs 6.14.0
3.0-9.12.0-6.0
pmol/Lpg/mL
7-11 yrs 6.14.0
4.1-7.92.7-5.2
pmol/Lpg/mL
12-19 yrs 5.93.9
3.5-7.72.3-5.0
pmol/Lpg/mL
Code:Page:
DANIEL MERCADO MEDICAL CENTERSerology and Immunology
Standard Operating Procedure
Issue Date: Revision Date:Revision No. 0.0
FT4 (Free Thyroxine)
INTENDED USE: Immunoassay for the in vitro quantitative determination of free thyroxine in human serum and plasma. The electrchemiluminescence immunoassay “ECLIA” is intended for use on elecsys and cobas e immunoassay analyzers.
SUMMARY: The thyroid hormone thyroxine (T4) is physiologically part of the regulating circuit of the thyroid gland and has an effect on general metabolism. The major fraction of total Thyroxine is bound to the transport proteins (TBG, prealbumin, albumin). The free thyroxine (fT4) is the physiologically active thyroxine component. The determination of free thyroxine (fT4) is an important element in clinical routine diagnostics. Free T4 is measured together with TSH when thyroid function disorders are suspected. The determination of fT4 is also suitable for monitoring thyrosuppressive therapy. The determination of free T4 has the advantage of being independent of changes in the concentrations and binding properties of the binding proteins; additional determination of a binding parameter (T-uptake, TBG) is therefore unnecessary. A variety of methods are available for estimating the free thyroid hormone levels. The direct measurement of fT3 and fT4 via equilibrium dialysis or ultrafiltration is mainly used as a reference method for standardizing the immunological procedures generally used for routine diagnostic purposes. In the Elecsys fT4 test the determination of free thyroxine is made with a specific anti-T4 antibody labeled with ruthenium complex. The quantity of antibody used is so small (equivalent approx. 1-2% of the total T4 content of a normal serum sample) that the equilibrium between bound and unbound T4 remains virtually unaffected.
TEST PRINCIPLE: Sandwich principle. Total duration of assay is 18 minutes. 1st incubation: 15ul of sample, and an T4-specific antibody labeled with ruthenium complex. 2nd incubation: After addition of biotinylated T4 and streptavidin-coated microparticles, the still-free
binding sites of the labeled antibody become occupied, with formation of an antibody-hapten complex. The entire complex becomes bound to the solid phase via interaction of biotin and streptavidin.
The reaction mixture is aspirated into the measuring cell where the microparticles are magnetically captured onto the surface of the electrode. Unbound substances are the removed with ProCell. Application of a voltage to the electrode then induces chemiluminescent emission which is measured by a photomultiplier.
Results are determined via a calibration curve which is instrument-specifically generated by 2-point calibration and a master curve via a reagent barcode.
PRECAUTIONS AND WARNINGS: for in vitro diagnostic use. Exercise the normal precautions required for handling all laboratory reagents. Disposal of all waste material should be in accordance with local guidelines. Avoid formation of foam with all reagents and sample types (specimen, calibrators, and controls).
STORAGE AND STABILITY: Store at 2-8 degrees Celsius. Store the Elecsys FT4 reagent kit in UPRIGHT to ensure complete availability of the microparticles during automatic mixing prior to use. Stability:
Unopened at 2-8 degrees Celsius Up to the stated expiration dateAfter opening at 2-8 degrees Celsius 12 weeksOn Elecsys 2010 6 weeks
Prepared by:
Faminialagao, KateMedical Technologist
Checked by:
Jon Paul Reyes RMTChief Medical Technologist
Noted by:
Rozani Odono Navarro MD, FPSPPathologist
Code:Page:
DANIEL MERCADO MEDICAL CENTERSerology and Immunology
Standard Operating Procedure
Issue Date: Revision Date:Revision No. 0.0
SPECIMEN COLLECTION AND PREPARATION:
Serum collected using standard sampling tubes or tubes containing separating gel.Li-, Na-, NH4
+-heparin, K3-EDTA, sodium citrate and sodium fluoride/potassium oxalate plasma.Stable for 7 days at 2-8°C, 1 month at -20°C. Freeze only once. Sample collection systems from various manufacturers may contain differing materials which could affect the test results in some cases. When processing samples in primary tubes (sample collection systems), follow the instructions of the tube manufacturer. Centrifuge samples containing precipitates before performing the assay. DO NOT USE HEAT INACTIVATED SAMPLES. Do not use samples and controls stabilized with azide. Ensure the patients’ samples, calibrators, and controls are at ambient temperature (20-25°C) before measurement. Because of possible evaporation effects, samples, calibrators, and controls on the analyzer should be measured within 2 hours. The Elecsys T4 assay employs a competitive test principle with polyclonal antibodies specifically directed against T4. Endogenous T4, released by the action of 8-anilino-1-naphthalene sulfonic acid (ANS), competes with the added biotinylated T4-derivative for the binding sites on the antibodies labeled with the ruthenium complex.
CALIBRATION FREQUENCY: calibration must be performed once per reagent lot using fresh reagent (i.e not more than 24 hours since the kit was registered on the analyzer) Renewed calibration is recommended for Elecsys 2010as follows:
After 1 month (28 days) when using the same reagent lot After 7 days (when using the same reagent kit on the analyzer)
CALCULATION: the analyzer automatically calculates the analyte concentration of each sample (either in pmol/L, ng/dL or ng/L)Conversion factors: pmol/L x 0.077688 = ng/dL
ng/dL x 12.872 = pmol/Lpmol/L x 0.77688 = ng/L
MEASURING RANGE: 0.300-100.00 pmol/L or 0.023-7.77 ng/dL (defined by the lower detection limit and the maximum of the master curve) Values below the detection limit are reported as < 0.300 pmol/L or <0.023 ng/dL. Values above the measuring range are reported as >100.0 pmol/L or > 7.77 ng/dL.
EXPECTED VALUES: Euthyroid: 12-22 pmol/L (0.93-1.7 ng/dL)
Prepared by:
Faminialagao, KateMedical Technologist
Checked by:
Jon Paul Reyes RMTChief Medical Technologist
Noted by:
Rozani Odono Navarro MD, FPSPPathologist
Code:Page:
DANIEL MERCADO MEDICAL CENTERSerology and Immunology
Standard Operating Procedure
Issue Date: Revision Date:Revision No. 0.0
TOTAL PSA Total (free + complexed) PSA – Prostate specific Antigen (tPSA)
Please note: The measure tPSA value of a patients’ sample can vary depending on the tsting procedure used. The laboratory finding must therefore always contain a statement on the tPSA method used. tPSA values determined on patient samples by different testing procedures cannot be directly compared with one another and could be the cause of erroneous medical interpretations. If there is a change in the tPSA assay procedure used while monitoring therapy, then the tPSA values obtained upon changing over to the new procedure must be confirmed by parallel measurements with both methods.
INTENDED USE: the Elecsys total PSA immunoassay, a quantitative in vitro diagnostic tets for total (free+complexed) prostate-specific antigen (tPSA) in human serum and plasma, is indicated for the measurement of total PSA in conjunction with digital rectal examination (DRE) as an aid in the detection of prostate cancer in men aged 50 years or older. Prostate biopsy is required for diagnosis of prostate cancer. The test is further indicated for serial measurement of tPSA to aid in the management of cancer patient. The electrchemiluminescence immunoassay “ECLIA” is intended for use on elecsys and cobas e immunoassay analyzers.
SUMMARY: Prostate-specific antigen (PSA) is a glycoprotein (MW:30000-34000 daltons) having a close structural relationship with the glandular kallikreins. It has the function of a serine proteinase. The proteolytic activity of PSA in blood is inhibited by the irreversible formation of complexes with protease inhibitors such as alpha-1-antichymotrypsin, alpha-2-macroglobulin, and other acute phase proteins. Beside these complexes, about 30% of the PSA present in blood occurs in the free form, but is proteolytically inactive. Elevated concentrations of PSA in serum are generally indicative of pathologic condition of the prostate (prostatitis, benign benign hyperplasia or carcinoma). As PSA is also present in para-urethral and anal glands, as well as in breast tissue or with breast cancer, low levels of PSA can also be detected in sera for women. PSA may still be detectable even after radical prostatectomy. The main areas in which PSA determinations are employed are the monitoring of progress and efficiency of therapy in patients with prostate carcinoma or receiving hormonal therapy. The steepness of the rate of fall in PSa down to no-longer detectable levels following radiotherapy, hormonal therapy or radical surgical removal of the prostate provides information of the success of therapy. An inflammation or trauma of the prostate (e.g. in cases of urinary retention or following rectal examination, cystoscopy, coloscopy, transurethral biopsy, laser treatment or ergometry) can lead to PSA elevations of varying duration and magnitude. The 2 monoclonal antibodies used in the Elecsys total PSA recognize PSA and PSA_ACL on an equimolar basis in the range of 10-50% free PSA/total PSA which are the free PSA-ratios as seen in clinical practice.
TEST PRINCIPLE: Sandwich principle. Total duration of assay is 18 minutes. 1st incubation: 20ul of sample, a biotinylated monoclona PSA-specific antibody, and a monoclonal PSA
specific antibody labeled with ruthenium complex react to form a sandwich complex. 2nd incubation: After addition of streptavidin-coated microparticles, the complex becomes bound to the
solid phase via interaction of biotin and streptavidin. The reaction mixture is aspirated into the measuring cell where the microparticles are magnetically
captured onto the surface of the electrode. Unbound substances are the removed with ProCell. Application of a voltage to the electrode then induces chemiluminescent emission which is measured by a photomultiplier.
Results are determined via a calibration curve which is instrument-specifically generated by 2-point calibration and a master curve via a reagent barcode.
PRECAUTIONS AND WARNINGS: for in vitro diagnostic use. Exercise the normal precautions required for handling all laboratory reagents. Disposal of all waste material should be in accordance with local guidelines. Avoid formation of foam with all reagents and sample types (specimen, calibrators, and controls).
Prepared by:
Faminialagao, KateMedical Technologist
Checked by:
Jon Paul Reyes RMTChief Medical Technologist
Noted by:
Rozani Odono Navarro MD, FPSPPathologist
Code:Page:
DANIEL MERCADO MEDICAL CENTERSerology and Immunology
Standard Operating Procedure
Issue Date: Revision Date:Revision No. 0.0
STORAGE AND STABILITY: Store at 2-8 degrees Celsius. Store the Elecsys TPSA reagent kit in UPRIGHT to ensure complete availability of the microparticles during automatic mixing prior to use. Stability:
Unopened at 2-8 degrees Celsius Up to the stated expiration dateAfter opening at 2-8 degrees Celsius 12 weeksOn Elecsys 2010 8 weeks
SPECIMEN COLLECTION AND PREPARATION:
Serum collected using standard sampling tubes or tubes containing separating gel.Li-, Na-, NH4
+-heparin, K3-EDTA, sodium citrate and sodium fluoride/potassium oxalate plasma.Stable for 5 days at 2-8°C, 6 months at -20°C. Freeze only once. Sample collection systems from various manufacturers may contain differing materials which could affect the test results in some cases. When processing samples in primary tubes (sample collection systems), follow the instructions of the tube manufacturer. Centrifuge samples containing precipitates before performing the assay. DO NOT USE HEAT INACTIVATED SAMPLES. Do not use samples and controls stabilized with azide. Ensure the patients’ samples, calibrators, and controls are at ambient temperature (20-25°C) before measurement. Because of possible evaporation effects, samples, calibrators, and controls on the analyzer should be measured within 2 hours. The Elecsys T4 assay employs a competitive test principle with polyclonal antibodies specifically directed against T4. Endogenous T4, released by the action of 8-anilino-1-naphthalene sulfonic acid (ANS), competes with the added biotinylated T4-derivative for the binding sites on the antibodies labeled with the ruthenium complex.
CALIBRATION FREQUENCY: calibration must be performed once per reagent lot using fresh reagent (i.e not more than 24 hours since the kit was registered on the analyzer) Renewed calibration is recommended for Elecsys 2010as follows:
After 1 month (28 days) when using the same reagent lot After 7 days (when using the same reagent kit on the analyzer) As required: e.g. quality control findings outside the specified limits
CALCULATION: the analyzer automatically calculates the analyte concentration of each sample (either in ng/mL or ug/L)
MEASURING RANGE: 0.002-100.00 ng/mL (defined by the lower detection limit and the maximum of the master curve) Values below the detection limit are reported as <0.002 ng/mL. Values above the measuring range are reported as >100.0 ng/mL (or up to 5000 ng/mL for 50-fold diluted samples).
EXPECTED VALUES: Normal healthy males: 0.00-4.00 ng/mL
Prepared by:
Faminialagao, KateMedical Technologist
Checked by:
Jon Paul Reyes RMTChief Medical Technologist
Noted by:
Rozani Odono Navarro MD, FPSPPathologist
Code:Page:
DANIEL MERCADO MEDICAL CENTERSerology and Immunology
Standard Operating Procedure
Issue Date: Revision Date:Revision No. 0.0
HBsAg II (Hepatitis B surface Antigen 2nd generation)
INTENDED USE: Immunoassay for the in vitro quantitative determination of hepatitis B surface antigen in human serum and plasma. The electrchemiluminescence immunoassay “ECLIA” is intended for use on elecsys and cobas e immunoassay analyzers.
SUMMARY: The hepatitis B surface antigen, a polypeptide of varying size, is a component of the external envelop of the hepatitis B virus (HBV). The blood of persons infected with HBV contains, in addition to intact infectious HBV particles, small non-infectious “empty” envelop particles, which are formed in great excess and also contain the hepatitis B surface antigen. The HBsAg determinant a, against which the immune response is mainly directed, is common to all HBsAg particles. Within this a determinant several HBsAg subtypr determinants could be defined as d, y, w1-w4, r and q. Under selective pressure (caused by antiviral theyrapy or by the action of the immune system itself) the virus can express many different viable HBsAg mutants (so-called escape mutants). Some mutants might lead to a loss of detection in commercially available HBsAg assays. The Elecsys HBsAg II assay was especially developed in order to detect a multitude of these mutants. The detection of HBsAg in human serum or plasma indicates an infection by the hepatitis B virus. HBsAg is the first immunological marker and is generally present some days or weeks before clinical symptoms begin to appear. HBsAg is observed in persons with acute and chronic hepatitis B infections. In rare cases a HBV infection can also take place without HBsAg being detectable. HBsAg are used within the scope of diagnostic procedures to identify persons infected with HBV and to prevent transmission of the hepatitis B virus by blood and blood products. HBsAg tests are also used to monitor the course of the disease in persons with acute or chronic HBV infections and if necessary, to check the efficacy of an antiviral therapy. In addition HBsAg tests are recommended as part of prenatal care, in order to be able to initiate suitable measures for preventing as far as possible the transmission of HBV infection to the newborn child. The Elecsys HBsAg test uses monoclonal and polyclonal anti-HBs antibodies (mouse and sheep) for the HBsAg determination.
TEST PRINCIPLE: Sandwich principle. Total duration of assay is 18 minutes. 1st incubation: 50ul of sample, two biotinylated monoclonal HBsAg-specific antibody, and a mixture of
monoclonal HBsAg and polyclonal anti-HBsAg antibodies labeled with ruthenium complex react to form a sandwich complex.
2nd incubation: After addition of streptavidin-coated microparticles, the complex becomes bound to the solid phase via interaction of biotin and streptavidin.
The reaction mixture is aspirated into the measuring cell where the microparticles are magnetically captured onto the surface of the electrode. Unbound substances are the removed with ProCell. Application of a voltage to the electrode then induces chemiluminescent emission which is measured by a photomultiplier.
Results are determined automatically by the software by comparing the electrochemiluminescence signal obtained from the reaction product of the sample with the signal of the cutoff value previously obtained by HBsAg calibration
PRECAUTIONS AND WARNINGS: for in vitro diagnostic use. Exercise the normal precautions required for handling all laboratory reagents. Disposal of all waste material should be in accordance with local guidelines. The reagents may not be used after the stated expiration date. Avoid formation of foam with all reagents and sample types (specimen, calibrators, and controls).
STORAGE AND STABILITY: Store at 2-8 degrees Celsius. Store the Elecsys HBsAg II reagent kit in UPRIGHT to ensure complete availability of the microparticles during automatic mixing prior to use. Stability:
Unopened at 2-8 degrees Celsius Up to the stated expiration dateAfter opening at 2-8 degrees Celsius 12 weeksOn Elecsys 2010 4 weeksCal1, cal2 after opening at 2-8 degrees Celsius 8 weeks (STORE UPRIGHT!)
Prepared by:
Faminialagao, KateMedical Technologist
Checked by:
Jon Paul Reyes RMTChief Medical Technologist
Noted by:
Rozani Odono Navarro MD, FPSPPathologist
Code:Page:
DANIEL MERCADO MEDICAL CENTERSerology and Immunology
Standard Operating Procedure
Issue Date: Revision Date:Revision No. 0.0
SPECIMEN COLLECTION AND PREPARATION:
Serum collected using standard sampling tubes or tubes containing separating gel.Li-, Na-, NH4
+-heparin, K3-EDTA, sodium citrate and sodium fluoride/potassium oxalate plasma.Stable for 5 days at 2-8°C, 3 months at -20°C. Freeze samples 4 times. Sample collection systems from various manufacturers may contain differing materials which could affect the test results in some cases. When processing samples in primary tubes (sample collection systems), follow the instructions of the tube manufacturer. Centrifuge samples containing precipitates before performing the assay. DO NOT USE HEAT INACTIVATED SAMPLES. Do not use samples and controls stabilized with azide. Ensure the patients’ samples, calibrators, and controls are at ambient temperature (20-25°C) before measurement. Because of possible evaporation effects, samples, calibrators, and controls on the analyzer should be measured within 2 hours. The Elecsys T4 assay employs a competitive test principle with polyclonal antibodies specifically directed against T4. Endogenous T4, released by the action of 8-anilino-1-naphthalene sulfonic acid (ANS), competes with the added biotinylated T4-derivative for the binding sites on the antibodies labeled with the ruthenium complex.
CALIBRATION FREQUENCY: calibration must be performed once per reagent lot using fresh reagent (i.e not more than 24 hours since the kit was registered on the analyzer) Renewed calibration is recommended for Elecsys 2010as follows:
After 1 month (28 days) when using the same reagent lot After 7 days (when using the same reagent kit on the analyzer)
CALCULATION: the analyzer automatically calculates the cutoff based on the measurement of Cal1 and Cal2. The result of a sample is given either as reactive or non-reactive as well as in the form of a cutoff index (signal sample/cutoff)
INTERPRATATION OF THE RESULTS: Samples with a cutoff index < 0.900 are non reactive in the Elecsys HBsAg II test. These samples are considered negative for HBsAg and do not need further testing. Samples with a cutoff index ≥ 0.900 to <1.00 are considered borderline in the Elecsys HBsAg II test. Samples with a cutoff index ≥ 1.00 are considered reactive in the Elecsys HBsAg II test. All samples found to be reactive or borderline in the initial test should be retested in duplicate with the Elecsys HBsAg II assay. If these samples yield mean cutoff index of <0.900 upon redetermination, they are considered as negative for HBsAg. Samples confirmed by neutralization with human anti-HBs are regarded as positive for HbsAg.
Prepared by:
Faminialagao, KateMedical Technologist
Checked by:
Jon Paul Reyes RMTChief Medical Technologist
Noted by:
Rozani Odono Navarro MD, FPSPPathologist
Code:Page:
DANIEL MERCADO MEDICAL CENTERSerology and Immunology
Standard Operating Procedure
Issue Date: Revision Date:Revision No. 0.0
ANTI-HBs (Antibody to Hepatitis B surface antigen = anti-HBs)
INTENDED USE: Immunoassay for the in vitro quantitative determination of human antibodies hepatitis B surface antigen in human serum and plasma. The electrchemiluminescence immunoassay “ECLIA” is intended for use on elecsys and cobas e immunoassay analyzers.
SUMMARY: Anti-HBs is a specific (generally IgG) antibody that is directed against the hepatitis B surface antigen. Anti-HBs can be formed following a hepatitis infection or after hepatitis B vaccination. Antibodies are formed against the HBsAg determinant a, which is common to all subtypes and against subtype-specific determinants. Anti-HBs tests are used within the scope of hepatitis vaccination. In addition, Anti-HBs tests are used to monitor the course of disease following acute hepatitis infection. The Elecsys Anti-HBs assa uses a mixture of purified antigens of the HbsAg subtypes ad and ay from human sera.
TEST PRINCIPLE: Sandwich principle. Total duration of assay is 18 minutes. 1st incubation: Anti-HBs in the sample (40ul), biotinylated HBsAg (ad/ay) and HBsAg (ad/ay) with
ruthenium complex react to form a sandwich complex. 2nd incubation: After addition of streptavidin-coated microparticles, the complex becomes bound to the
solid phase via interaction of biotin and streptavidin. The reaction mixture is aspirated into the measuring cell where the microparticles are magnetically
captured onto the surface of the electrode. Unbound substances are the removed with ProCell. Application of a voltage to the electrode then induces chemiluminescent emission which is measured by a photomultiplier.
Results are determined via a calibration curve which is instrument-specifically generated by 2-point calibration and a master curve via a reagent barcode.
PRECAUTIONS AND WARNINGS: for in vitro diagnostic use. Exercise the normal precautions required for handling all laboratory reagents. Disposal of all waste material should be in accordance with local guidelines. The reagents may not be used after the stated expiration date. Avoid formation of foam with all reagents and sample types (specimen, calibrators, and controls).
STORAGE AND STABILITY: Store at 2-8 degrees Celsius. Store the Elecsys ANTI-HBs reagent kit in UPRIGHT to ensure complete availability of the microparticles during automatic mixing prior to use. Stability:
Unopened at 2-8 degrees Celsius Up to the stated expiration dateAfter opening at 2-8 degrees Celsius 8 weeksOn Elecsys 2010 4 weeksCal1, cal2 after opening at 2-8 degrees Celsius 8 weeks (STORE UPRIGHT!)
SPECIMEN COLLECTION AND PREPARATION:
Serum collected using standard sampling tubes or tubes containing separating gel.Li-, Na-, NH4
+-heparin, K3-EDTA, sodium citrate and sodium fluoride/potassium oxalate plasma.Stable for 5 days at 2-8°C, 3 months at -20°C. Freeze samples 4 times. Sample collection systems from various manufacturers may contain differing materials which could affect the test results in some cases. When processing samples in primary tubes (sample collection systems), follow the instructions of the tube manufacturer. Centrifuge samples containing precipitates before performing the assay. DO NOT USE HEAT INACTIVATED SAMPLES. Do not use samples and controls stabilized with azide. Ensure the patients’ samples, calibrators, and controls are at ambient temperature (20-25°C) before measurement. Because of possible evaporation effects, samples, calibrators, and controls on the analyzer should be measured within 2 hours. The Elecsys T4 assay employs a competitive test principle with polyclonal antibodies specifically directed against T4. Endogenous T4, released by the action of 8-anilino-1-naphthalene sulfonic acid (ANS), competes with the added biotinylated T4-derivative for the binding sites on the antibodies labeled with the ruthenium complex.
Prepared by:
Faminialagao, KateMedical Technologist
Checked by:
Jon Paul Reyes RMTChief Medical Technologist
Noted by:
Rozani Odono Navarro MD, FPSPPathologist

Code:Page:
DANIEL MERCADO MEDICAL CENTERSerology and Immunology
Standard Operating Procedure
Issue Date: Revision Date:Revision No. 0.0
CALIBRATION FREQUENCY: calibration must be performed once per reagent lot using fresh reagent (i.e not more than 24 hours since the kit was registered on the analyzer) Renewed calibration is recommended for Elecsys 2010as follows:
After 1 month (28 days) when using the same reagent lot After 7 days (when using the same reagent kit on the analyzer)
CALCULATION: the analyzer automatically calculates the analyte concentration of each sample in IU/L.
INTERPRATATION OF THE RESULTS: Samples with concentrations < 10 IU/L are considered non reactive in the Elecsys anti-HBs test. Samples with concentrations ≥ 10 IU/L are considered reactive in the Elecsys anti-HBs test.
Prepared by:
Faminialagao, KateMedical Technologist
Checked by:
Jon Paul Reyes RMTChief Medical Technologist
Noted by:
Rozani Odono Navarro MD, FPSPPathologist
Code:Page:
DANIEL MERCADO MEDICAL CENTERSerology and Immunology
Standard Operating Procedure
Issue Date: Revision Date:Revision No. 0.0
TROPONIN I STAT
INTENDED USE: Immunoassay for the in vitro quantitative determination of cardiac troponin I in human serum and plasma. The Elecsys Troponin I stat assay is intended to aid in the diagnosis and treatment of myocardial infarction and cardiac muscle damage. Cardiac troponin I determinations aid in the risk stratification of patients with unstable angina pectoris or non-ST-segment elevation acute coronary syndrome with respect to relative risk of mortality, myocardial infarction, or increased probability of ischemic events requiring urgent revascularization procedures.
SUMMARY: Troponin I (TnI) is a key regulatory protein of the striated musculature. Although its function in the contractile apparatus is the same in all striated muscles. TnI originating from the myocardium (cardiac TnI, molecular weight 23.9kD) clearly differs from skeletal muscle TnI. Due to this high tissue-specificity, cardiac troponin I is a highly sensitive marker for myocardial damage. Cardiac TnI (cTnI) allows to differentiate between skeletal muscle lesions (e.g. rhabdomyolysis and polytraumatism) and myocardial injury. In cases of acute myocardial infarction (AMI), cTnI levels in serum rise about 3-6hours after the onset of cardiac symptoms, peak at 12-16 hours and can remain elevated for 4-9 days. Elevated cTnI levels have been reported in cases of unstable angina pectoris (UAP) and congestive heart failure (CHF). Cardiac TnI is a well established prognostic marker which can predict near-, mid-, and even long-term outcome of patients with acute coronary syndrome (ACS). In summary, elevated troponin levels point to myocardial injury, but are not necessarily indicative of an ischemic mechanism. The term MI should be used when there is evidence of cardiac damage, as detected by marker proteins in a clinical setting consistent with myocardial ischemia. If the clinical circumstance suggests that the ischemic mechanism is unlikely, other causes of cardiac injury should be considered. The elecsys troponin I assay employs two pairs of monoclonal antibodies specifically directed against human cardiac troponin i.
TEST PRINCIPLE: Sandwich principle. Total duration of assay: 9 minutesElecsys 2010 and cobas e 411 analysers:
1st incubation: 30 ul of sample, 2 biotinylated monoclonal anti-cardiac troponin I antibodies, and 2 monoclonal anti-cardiac troponin I antibodies labeled with a ruthenium complex react to form a sandwich complex.
2nd incubation: after addition of streptavidin-coated microparticles, the complx becomes bound to the solid phase via interaction of biotin and streptavidin.
PRECAUTIONS AND WARNINGS: for in vitro diagnostic use. Exercise the normal precautions required for handling all laboratory reagents. Disposal of all waste material should be in accordance with local guidelines. The reagents may not be used after the stated expiration date. Avoid formation of foam with all reagents and sample types (specimen, calibrators, and controls).
STORAGE AND STABILITY: Store at 2-8 degrees Celsius. Store the Elecsys troponin I stat reagent kit in UPRIGHT to ensure complete availability of the microparticles during automatic mixing prior to use. Stability:
Unopened at 2-8 degrees Celsius Up to the stated expiration dateAfter opening at 2-8 degrees Celsius 4 weeksOn all analysers 14 days
SPECIMAN COLLECTION AND PREPARATION: serum collected using standard sampling tubes or tubes containing separating gel. K2-EDTA, K3-EDTA, and Li-heparin plasma. Plasma (EDTA, heparin) and serum samples should not be used interchangeably.
Prepared by:
Faminialagao, KateMedical Technologist
Checked by:
Jon Paul Reyes RMTChief Medical Technologist
Noted by:
Rozani Odono Navarro MD, FPSPPathologist
Code:Page:
DANIEL MERCADO MEDICAL CENTERSerology and Immunology
Standard Operating Procedure
Issue Date: Revision Date:Revision No. 0.0
CALIBRATION FREQUENCY: Calibration must be performed once per reagent lot using fresh reagent (i.e. not more than 24 hours since the reagent kit was registered on the analyser)Renewed calibration is recommended as follows:
After 1 month (28 days) when using the same reagent lot After 7 days (when using the same reagent kit on the analyser) As required: e.g. quality control findings outside specified limits
MEASURING RANGE:0.16-25 ug/L or ng/mL (defined by the limit of detection and the maximum of the master curve). Values below the limit of blank are reported as <0.1 ug/L or ng/mL. values above the limit of blank but below the detection limit will not be flagged by the instrument. Values above the measuring range are reported as >25 ug/L or ng/mL (or upto 250 ug/L or ng/mL for 10-fold diluted samples).
Prepared by:
Faminialagao, KateMedical Technologist
Checked by:
Jon Paul Reyes RMTChief Medical Technologist
Noted by:
Rozani Odono Navarro MD, FPSPPathologist
Code:Page:
DANIEL MERCADO MEDICAL CENTERSerology and Immunology
Standard Operating Procedure
Issue Date: Revision Date:Revision No. 0.0
DETERMINATION OF SHORTNESS OF BREATH ALERT TRIAGE PROFILER S.O.B. PANEL
INTENDED USEThe Alere Triage® Profiler SOB™ (Shortness of Breath) Panel is a fluorescence immunoassay to be used with the Alere Triage® Meters for the quantitative determination of creatine kinase MB, myoglobin, troponin I, B-type natriuretic peptide, and cross-linked fibrin degradation products containing D-dimer in EDTA anticoagulated whole blood and plasma specimens. The test is used as an aid in the diagnosis of myocardial infarction (injury), an aid in the diagnosis and assessment of severity of heart failure, an aid in the risk stratification of patients with heart failure, an aid in the assessment and evaluation of patients suspected of having disseminated intravascular coagulation or thromboembolic events including pulmonary embolism and an aid in the risk stratification of patients with acute coronary syndromes.
Principles of the Test ProcedureThe Alere Triage® Profiler SOB™ Panel is a single use fluorescence immunoassay device designed to determine the concentration of CK-MB, myoglobin, troponin I, BNP and D-dimer in EDTA anticoagulated whole blood or plasma specimens.The test procedure involves the addition of several drops of an EDTA anticoagulated whole blood or plasma specimen to the sample port on the Test Device. After addition of the specimen, the whole blood cells are separated from the plasma using a filter contained in the Test Device. The specimen reacts with fluorescent antibody conjugates and flows through the Test Device by capillary action. Complexes of each fluorescent antibody conjugate are captured on discrete zones specific for each analyte. The Test Device is inserted into the Alere Triage® Meter (hereafter referred to as Meter). The Meter is programmed to perform the analysis after the specimen has reacted with the reagents within the Test Device. The analysis is based on the amount of fluorescence the Meter detects within a measurement zone on the Test Device. The concentration of the analyte(s) in the specimen is directly proportional to the fluorescence detected. The results are displayed on the Meter screen in approximately 20 minutes from the addition of specimen. All results are stored in the Meter memory to display or print when needed. If connected, the Meter can transmit results to the lab or hospital information system.
Reagents and Materials ProvidedThe Test Device contains all the reagents necessary for the simultaneous quantification of D-dimer, CK-MB, myoglobin, troponin I and BNP in EDTA anticoagulated whole blood or plasma specimens.The Test Device Contains:• Murine monoclonal antibodies against CK-MB, myoglobin, troponin I, D-dimer and BNP• Murine polyclonal antibodies against CK-MB, myoglobin, and BNP• Goat polyclonal antibodies against troponin I• Fluorescent dye• StabilizersKit contains:
25 Test Devices25 Transfer Pipettes1 Reagent CODE CHIP™
Module1 Printer Paper Roll
Prepared by:
Faminialagao, KateMedical Technologist
Checked by:
Jon Paul Reyes RMTChief Medical Technologist
Noted by:
Rozani Odono Navarro MD, FPSPPathologist
Code:Page:
DANIEL MERCADO MEDICAL CENTERSerology and Immunology
Standard Operating Procedure
Issue Date: Revision Date:Revision No. 0.0
Specimen Collection and Preparation• A venous whole blood or plasma specimen using EDTA as the anticoagulant is required for testing with this
product. Specifically, plastic K2 EDTA tubes are recommended for sample collection to ensure optimal product performance. Other blood specimen types, draw methods or anticoagulants have not been evaluated.
• For specimen collection, follow the sample tube manufacturer’s recommended procedure.• If using whole blood, test the patient specimen within 6 hours of collection. If testing cannot be completed within
6 hours, the plasma should be separated and stored at -20°C until it can be tested.• Transport specimens at room temperature or chilled and avoid extreme temperatures.• Avoid using severely hemolyzed specimens whenever possible. If a specimen appears to be severely hemolyzed another specimen should be obtained and tested.
Test ProcedureLot Calibration Using the Reagent CODE CHIP™ Module When a new lot of Test Devices is opened, the calibration and expiration data for that lot of Test Devices must be transferred to the Meter before patient testing. Use the Reagent CODE CHIP™ module supplied with the new lot of Test Devices to transfer the data to the Meter.
Perform one time for each new lot of Test Devices1. From the main screen, select Install New Code Chip. Press Enter.2. Place the Reagent CODE CHIP™ module into the lower left front corner of the Meter and follow the prompts on
the screen. 3. Remove the Reagent CODE CHIP™ module from the Meter when data transfer is complete.4. Place the Reagent CODE CHIP™ module back into its original container for storage.Testing Patient SpecimensProcedural Notes
• Frozen plasma and refrigerated whole blood or plasma specimens must be allowed to reach room temperature and be mixed thoroughly before testing.
• Mix whole blood specimens by gently inverting the tube several times.• Mix plasma specimens by vortexing or inverting the tube several times.
STEP 1 - Add Patient Specimen1. Open the pouch and label the Test Device with the patient identification number.2. Place the Test Device on a level, horizontal surface.3. Using the transfer pipette, squeeze the larger (top) bulb completely and insert the tip into the specimen.4. Release the bulb slowly. The transfer pipette barrel should fill completely with some fluid flowing into the
smaller (lower) bulb.5. Place the tip of the transfer pipette into the sample port of the Test Device and squeeze the larger bulb completely.
The entire volume of fluid in the transfer pipette barrel must flow into the sample port. The specimen in the smaller (lower) bulb will not be expelled.
6. Remove the transfer pipette tip from the sample port and then release the larger (top) bulb.7. Discard the transfer pipette.8. Allow specimen to absorb completely before moving the Test Device.STEP 2 - Run Test1. From the main screen, select Run Test and press Enter.2. Select Patient Sample and press Enter.3. Enter the patient identification number and press Enter.4. Confirm that the number was entered correctly by selecting Confirm Patient ID and pressing Enter. If the
number was not entered correctly, select Correct Patient ID, press Enter and repeat the previous step.5. Holding the Test Device by the edges, insert the Test Device into the Meter and press Enter. The results will be
displayed when the analysis is complete.Note: The Test Device must be inserted into the Meter within 30 minutes from the time the patient specimen was added. A delay longer than 30 minutes may cause the results to be invalid and blocked out on the printout.
Prepared by:
Faminialagao, KateMedical Technologist
Checked by:
Jon Paul Reyes RMTChief Medical Technologist
Noted by:
Rozani Odono Navarro MD, FPSPPathologist
Code:Page:
DANIEL MERCADO MEDICAL CENTERSerology and Immunology
Standard Operating Procedure
Issue Date: Revision Date:Revision No. 0.0
STEP 3 - Read the Results1. The result may be printed by pressing the Print button.2. Discard the Test Device after release from the Meter.3. A blocked out result indicates the result was invalid and the test should be repeated.
ResultsThe Meter measures the target analyte(s) automatically. The results are displayed on the screen. The operator has the option to print the results. For additional information, refer to the Alere Triage® Meter User Manual.NORMAL VALUES
D-dimer: 100-5000 ng/mLTroponin I: 0.05-30 ng/mLCK-MB: 1.0-80 ng/mLMyoglobin: 5 -500ng/mLBNP: 5-5000 pg/mL
Prepared by:
Faminialagao, KateMedical Technologist
Checked by:
Jon Paul Reyes RMTChief Medical Technologist
Noted by:
Rozani Odono Navarro MD, FPSPPathologist
Code:Page:
DANIEL MERCADO MEDICAL CENTERSerology and Immunology
Standard Operating Procedure
Issue Date: Revision Date:Revision No. 0.0
DETERMINATION OF NEUTROPHIL GELATINASE-ASSOCIATED LIPOCALIN (NGAL)
Intended UseThe Alere Triage® NGAL Test is a rapid, point of care fluorescence immunoassay to be used with the Alere Triage® Meter for the quantitative determination of neutrophil gelatinase-associated lipocalin (NGAL) in EDTA anticoagulated whole blood and plasma specimens. The test is used as an aid in the diagnosis of acute kidney injury.
Principles of the Test ProcedureThe test procedure involves the addition of several drops of an EDTA anti-coagulated whole blood or plasma specimen to the sample port on the Test Device. After addition of the specimen, the blood cells are separated from the plasma using a filter contained in the Test Device. The specimen reacts with fluorescent antibody conjugates and flows through the Test Device by capillary action. Complexes of each fluorescent conjugate are captured on a discrete zone specific for each analyte. The Test Device is inserted into the Alere Triage® Meter (hereafter referred to as Meter). The Meter is programmed to perform the analysis after the specimen has reacted with the reagents within the Test Device. The analysis is based on the amount of fluorescence the Meter detects within a measurement zone on the Test Device. The concentration of NGAL in the specimen is directly proportional to the fluorescence detected. The results are displayed on the Meter screen in approximately 20 minutes. All results are stored in the Meter memory to display or print when needed. If connected, the Meter can transmit results to the lab or hospital information system.
Reagents and Materials ProvidedThe Alere Triage® NGAL Test Device contains all the reagents necessary for the quantification of NGAL in EDTA anticoagulated whole blood or plasma specimens.The Test Device contains:• Recombinant antibodies against NGAL• Fluorescent dye• StabilizersKit contains:
25 Test Devices25 Transfer Pipettes1 Reagent CODE CHIP™
Module1 Printer Paper Roll
Specimen Collection and Preparation• A venous whole blood or plasma specimen using EDTA as the anticoagulant is required for testing with this
product. Other specimen types have not been evaluated. Plastic K2 EDTA tubes are required for sample collection to ensure optimal product performance.
• For sample collection, follow the sample tube manufacturer’s recommended procedure.• Anticoagulated whole blood and plasma specimens may be stored at room temperature for testing within 12 hours
of collection. Plasma specimens may be stored at 2-8°C for testing within 24 hours of collection. Transport specimens at room temperature or chilled and avoid extreme temperatures.
• If testing cannot be completed within 24 hours, the plasma should be stored at -20°C until it can be tested. • No more than a single freeze/thaw cycle is recommended.• Avoid using severely hemolyzed specimens whenever possible. If a specimen appears to be severely hemolyzed, another specimen should be obtained and tested.
Prepared by:
Faminialagao, KateMedical Technologist
Checked by:
Jon Paul Reyes RMTChief Medical Technologist
Noted by:
Rozani Odono Navarro MD, FPSPPathologist

Code:Page:
DANIEL MERCADO MEDICAL CENTERSerology and Immunology
Standard Operating Procedure
Issue Date: Revision Date:Revision No. 0.0
Test ProcedureLot Calibration Using the Reagent CODE CHIP™ Module When a new lot of Test Devices is opened, the calibration and expiration data for that lot of Test Devices must be transferred to the Meter before patient testing. Use the Reagent CODE CHIP™ module supplied with the new lot of Test Devices to transfer the data to the Meter. Perform one time for each new lot of Test Devices1. From the main screen, select Install New Code Chip. Press Enter.2. Place the Reagent CODE CHIP™ module into the lower left front corner of the Meter and follow the prompts on
the screen. 3. Remove the Reagent CODE CHIP™ module from the Meter when data transfer is complete.4. Place the Reagent CODE CHIP™ module back into its original container for storage.
Testing Patient SpecimensProcedural Notes• Frozen plasma and refrigerated whole blood or plasma specimens must be allowed to reach room temperature and
be mixed thoroughly before testing.• Mix whole blood specimens by gently inverting the tube several times.• Mix plasma specimens by vortexing or inverting the tube several times.
STEP 1 - Add Patient Specimen1. Open the pouch and label the Test Device with the patient identification number.2. Place the Test Device on a level, horizontal surface.3. Using the transfer pipette, squeeze the larger (top) bulb completely and insert the tip into the patient specimen.4. Release the bulb slowly. The transfer pipette barrel should fill completely with some fluid flowing into the
smaller (lower) bulb.5. Place the transfer pipette tip into the sample port of the Test Device and squeeze the larger bulb completely. The
entire volume of fluid in the transfer pipette barrel must flow into the sample port. The specimen in the smaller (lower) bulb will not be expelled.
6. Remove the transfer pipette tip from the sample port and then release the larger (top) bulb.7. Discard the transfer pipette.8. Allow specimen to absorb completely before moving the Test Device.
STEP 2 - Run Test1. From the main screen, select Run Test and press Enter.2. Select Patient Sample and press Enter.3. Enter the patient identification number and press Enter.4. Confirm that the number was entered correctly by selecting Confirm Patient ID and pressing Enter. If the
number was not entered correctly, select Correct Patient ID, press Enter and repeat the previous step.5. Holding the Test Device by the edges, insert the Test Device into the Meter and press Enter. The result will be
displayed when the analysis is complete.Note: The Test Device must be inserted into the Meter within 30 minutes from the time the patient specimen was added. A delay longer than 30 minutes may cause the results to be invalid and blocked out on the printout.
STEP 3 - Read the Results1. Results may be printed by pressing the Print button.2. Discard the Test Device after release from the Meter.3. A blocked out result indicates the result was invalid and the test should be repeated.
ResultsThe Meter measures the target analyte automatically. The results are displayed on the screen. The operator has the option to print the results. NORMAL VALUES: NGAL: <15 ng/Ml
Prepared by:
Faminialagao, KateMedical Technologist
Checked by:
Jon Paul Reyes RMTChief Medical Technologist
Noted by:
Rozani Odono Navarro MD, FPSPPathologist
Code:Page:
DANIEL MERCADO MEDICAL CENTERSerology and Immunology
Standard Operating Procedure
Issue Date: Revision Date:Revision No. 0.0
DETERMINATION OF TROPONIN T QUANTITATIVE
INTENDED USE: Quantitative immunological test for the specific detection of cardiac troponin T in heparinised venous blood for use with the cardiac reader instrument.
TEST PRINCIPLE: The Test contains two monoclonal antibodies specific to cardiac troponin T (cTnT): one gold-labelled, the other biotinylated. The antibodies from a sandwich complex with cTnTin the blood. Following the removal of erythrocytes from the sample, plasma passes through the detection zone in which the gold-labelled cTnT sandwich complexes accumulate and the positive signal is displayed as a reddish line (the signal line). Excess gold-labeled antibodies accumulate along the control line, signaling that the test was valid. The intensity of the signal line increases in proportion to the troponin T concentration. The optical system of the Cardiac reader instrument detects the two lines and measured the intensity of the signal line. The integrated software converts the signal intensity to a quantitative result and shows it on display.
SPECIMEN: Use heparinised venous whole blood only.
SAMPLE VOLUME: 150Ul
TEST PROCEDURE:1. Slide the coding chip that was supplied with the current pact of test into the slot on the instrument until it
snaps into place.2. When instructed in the display window, insert the test as shown.3. Press the Start button – the test will automatically be transported to the correct position for reading.4. While keeping the pipette vertical, dispense 150uL of sample into the application area marked with a
triangle.5. Press start button6. As soon as the countdown ends, the result is displayed on the screen. Results may also be sent to the
printer.
EXPECTED VALUES:TROPONIN T CONCENTRATION RESULT DISPLAYED COMMENTBelow 0.03 ng/mL Trop. T negative Low risk. Further changes to the
concentration of troponin T are possible. Rule out myocardial damage by repeating the test according to recommendations.
Between 0.03 ng/mL and 0.1 ng/mL Trop T LO<0.1 ng/mL Medium risk. This indicates that myocardial cells may have been damaged. Further changes to the concentration of troponin T are possible. Confirm myocardial damage by repeating the test.
Between 0.1 ng/mL and 2 ng/mL e.g. Trop T 0.91 ng/mL High risk of damaged heart muscleAbove 2 ng/mL Trop T HI >2.0 ng/mL High risk of damaged heart muscle.
INTERPRETATION OF RESULTS: A positive result means that the concentration of troponin T in the sample is above the tests threshold value of 0.1 ng/mL
Prepared by:
Faminialagao, KateMedical Technologist
Checked by:
Jon Paul Reyes RMTChief Medical Technologist
Noted by:
Rozani Odono Navarro MD, FPSPPathologist
Code:Page:
DANIEL MERCADO MEDICAL CENTERSerology and Immunology
Standard Operating Procedure
Issue Date: Revision Date:Revision No. 0.0
DETERMINATION OF D-DIMER
INTENDED USE: Quantitative immunological test for the of d-dimer in heparinised venous blood for use with the cardiac reader. D-dimeris a degradation product of crosslinked fibrin. The d-dimer concentration is a measure of the fibrinolytic activity of plasmin in the vascular system. Elevated concentrations of d-dimer indicate increased coagulatory and fibrinolytic activity. With a normal d-dimer value, acute deep vein thrombosis and pulmonary embolisms may be ruled out with very high reliability.
TEST PRINCIPLE: The Test contains two monoclonal antibodies against fibrin degradation products which contain the d-dimer structure element. One gold-labelled, the other biotinylated. The antibodies from a sandwich complex with the d-dimer in the blood. Following the removal of erythrocytes from the sample, plasma passes through the detection zone in which the gold-labelled d-dimer sandwich complexes accumulate and the positive signal is displayed as a reddish line (the signal line). Excess gold-labeled antibodies accumulate along the control line, signaling that the test was valid. The intensity of the signal line increases in proportion to the d-dimer concentration. The optical system of the Cardiac reader instrument detects the two lines and measured the intensity of the signal line. The integrated software converts the signal intensity to a quantitative result and shows it on display.
SPECIMEN: Use heparinised venous whole blood only.
SAMPLE VOLUME: 150Ul
TEST PROCEDURE:1. Slide the coding chip that was supplied with the current pact of tets into the slot on the instrument until it
snaps into place.2. When instructed in the display window, insert the test as shown.3. Press the Start button – the test will automatically be transported to the correct position for reading.4. While keeping the pipette vertical, dispense 150uL of sample into the application area marked with a
triangle.5. Press start button6. As soon as the countdown ends, the result is displayed on the screen. Results may also be sent to the
printer.
EXPECTED VALUES: The normal range for the Roche Cardiac d-dimer test includes values up to 0.5ug/mL. Values above 0.5ug/mL are to be considered as pathologically elevated.
Prepared by:
Faminialagao, KateMedical Technologist
Checked by:
Jon Paul Reyes RMTChief Medical Technologist
Noted by:
Rozani Odono Navarro MD, FPSPPathologist
Code:Page:
DANIEL MERCADO MEDICAL CENTERSerology and Immunology
Standard Operating Procedure
Issue Date: Revision Date:Revision No. 0.0
TROPONIN T SENSITIVE
INTENDED USE: The Trop T sensitive test is intended for the qualitative determination of cardiac troponin T (cTnT) in anticoagulated venous or arterial whole blood. Both quantitative and qualitative measurements of cardiac troponin T have been shown to aid in the diagnosis of acute myocardial infarction.
Troponin T is one of three proteins that make up the troponin complex, which mediates the calcium-activation of contraction of striated muscles. Troponin T isoforms from cardiac and skeletal muscles differ in their amino acid composition and can be differentiated immunologically.
TEST PRINCIPLE: This test is based on the dual monoclonal antibody “sandwich principle” using a poly(streptavidin)-biotin capture system with gold sol particle
POLY-STRETAVIDIN GOLDSOL
MEMBRANE
SPECIMEN COLLECTION AND PREPARATION:WHOLE BLOOD: Use venous whole blood anticoagulated with EDTA (purple top) or heparin (green top)
collected by standard venipuncture technique or use arterial whole blood anticoagulated with heparin. NOTE: Do not use citrated blood or collection vessels containing gel or sodium fluoride.
TEST PROCEDURE:1. Obtain Venous whole blood sample from a purple top (EDTA) or green top (heparin) tube. Use syringe to
transfer blood from sample collection tube to the assay. After depressing the plunger to expel any air from the syringe, insert the needle to the rubber stopper of the blood collection tube.
2. Turn blood collection tube upside down and draw blood up to 150uL mark.3. Carefully dispense the blood into the round sample well. The syringe dispenses approximately 150 uL.
Underdosing or overdosing will affect results.WARNING: Dispensing too forcefully may cause splattering of the blood, loss of sample and/or hemolysis.
4. Cover the application area using adhesive tab peeled from the documentation label.5. Record patient details, date and the start time on numbered TROP T sensitive documentation label. If the
concentration of cardiac troponin T in the sample is high, a test line can be seen in the read window after a few minutes. Do not read a negative result until 15 minutes have elapsed. However, a positive result can be read immediately.
6. After 15-20 minutes, or when red-brown discoloration appears in the read window, whichever comes first, record the time and read the result. Hold the assay at such that no shadow falls onto the reading window. Bright, diffuse lighting similar to daylight is best suited for this purpose. Readings taken after 20 minutes have elapsed are not valid due to red-brown discoloration that may appear in the read window and should be disregarded. The presence of two lines in the read window (test line and control line) indicates the presence of cardiac troponin T ≥0.08 ng/mL. Even a very faint line indicates a positive test.
7. All blood-contaminated products should be disposed of properly.
Prepared by:
Faminialagao, KateMedical Technologist
Checked by:
Jon Paul Reyes RMTChief Medical Technologist
Noted by:
Rozani Odono Navarro MD FPSPPathologist
Code:Page:
DANIEL MERCADO MEDICAL CENTERSerology and Immunology
Standard Operating Procedure
Issue Date: Revision Date:Revision No. 0.0
TEST RESULTS: The presence of two lines in the read window indicates the presence of cardiac troponin T ≥0.08 ng/mL.
The result is positive even if the test line is faint.The presence of only the control line indicates that the concentration of cardiac troponin T in sample is <
0.08 ng/mL.The absence of the control line indicates an invalid test result. Repeat the test using a new assay.
Prepared by:
Faminialagao, KateMedical Technologist
Checked by:
Jon Paul Reyes RMTChief Medical Technologist
Noted by:
Rozani Odono Navarro MD FPSPPathologist
Code:Page:
DANIEL MERCADO MEDICAL CENTERSerology and Immunology
Standard Operating Procedure
Issue Date: Revision Date:Revision No. 0.0
TEST USED IN THE DETERMINATION OF RHEUMATOID FACTOR (RF)
This test is for the qualitative and semi-quantitative measurement of RF in human serum. Rheumatoid factors are antibodies directed against antigenic sites in the Fc fragment of human and animal IgG. The frequent occurrence in rheumatoid arthritis makes them useful for diagnosis and monitoring of the disease.
PRINCIPLE:The Rf reagent is based on an immunological reaction between human IgG bound to biologically inert latex
particles and rheumatoid factors in the test specimen. When serum containing rheumatoid factors is mixed with the latex reagent visible agglutination occurs.
SPECIMEN COLLECTION AND STORAGE:1. Use fresh serum collected by centrifuge clotted blood. 2. If the test cannot be carried out on the same day, the serum may be stored between 2-8◦C for no longer tha
72 hours after collection. 3. For longer periods the sample must be frozen.4. As in all serological tests, hemolytic or contaminated serummust not be used.5. Do not use plasma.
PROCEDURE:Qualitative Test:
1. Bring reagents and specimen to room temperature before use.2. Place one drop (50uL) of the Rf positive control on field #1 of the reaction slide. Place one drop (50uL) of
the Rf negative control on field #2. The remaining fields are used for the test specimen. Using pipets provided, place on drop of the undiluted specimens on successive fields.
3. Gently resuspend the RF latex reagent and add one drop to each test field. Use pipet/stir stick to spread reaction mixture over entire test field.
4. Rotate the silde for 3 minutes and read immediately under direct light.NOTE: an agglutination of the latex particle is a positive result. Agglutination indicates a RF concentration of more than 20 IU/mL. Serum with positive agglutination should be run again with the quantitative test.
Quantitative Test:1. Bring reagents and specimen to room temperature before use.2. Using Glycine Buffer, dilute the specimen 1:2, 1:4, 1:8, 1:16, 1:32 or as needed
NOTE: Dilute buffer by adding 1 part buffer to 9 parts distilled water before use.3. Place one drop (50uL) of the Rf positive control on field #1 of the reaction slide. Place one drop (50uL) of
the Rf negative control on field #2. Place one drop (50uL) of each dilution on successive fields if the reaction slide.
4. Gently resuspend the RF latex reagent and add one drop to each test field.5. Use pipet/stir stick to spread reaction mixture over entire test field.6. Rotate slide for 3 minutes and immediately read under direct light.
INTERPRETATION:Qualitative test:
A negative reaction is indicated by a uniform milky suspension with no agglutination as observed with the RF negative control. A positive reaction is indicated by an observable agglutination in the reaction mixture. The specimen reaction should be compared to the RF negative and positive controls.Semi-quantitative test:
The titer of the serum is the reciprocal of the highest dilution which exhibits a positive reaction.An estimate of the RF concentration in the specimen can be expressed in IU/mL using the following equation:
IU/mL of specimen = IU/mL control x specimen titerIU/mL of specimen = 20 IU/mL x specimen titer
Prepared by:
Faminialagao, KateMedical Technologist
Checked by:
Jon Paul Reyes RMTChief Medical Technologist
Noted by:
Rozani Odono Navarro MD FPSPPathologist
Code:Page:
DANIEL MERCADO MEDICAL CENTERSerology and Immunology
Standard Operating Procedure
Issue Date: Revision Date:Revision No. 0.0
DEFINITION AND DESCRIPTION OF ASO LATEX
The ASO latex test kit is for the qualitative and semi-quantitative determination of anti-streptolysin O (ASO) antibodies in human serum.
PRINCIPLE:The ASO is a rapid slide agglutination procedure. Latex particles are coated with streptolysin O, which, when mixed with samples containing ASO antibodies show an agglutination pattern.
SPECIMEN AND SAMPLE PREPARATION:Use fresh serum obtained by centrifugation of clotted blood. The sample may be stored at 2-8◦C for 48 hours before performing the test. For longer periods of time the serum must be frozen. Hemolysed, lipemic or contaminated serum must be discarded.
PROCEDURE:Qualitative Method:
1. Allow each component to reach room temperature.2. Gently shake the latex reagent to disperse the particles.3. Place a drop of undiluted specimen onto the circle of the test slide.4. Add one drop of the latex reagent next to the drop of serum5. Spread the reagent and serum sample over the entire area of the test circle using a separate stirrer for each
sample.6. Gently tilt the test slide backwards and forwards approximately once every two seconds for two minutes.
Positive and negative controls should be included at regular intervals.
Semi-quantitative method:1. Bring reagents and specimen to room temperature before use.2. Using Glycine Buffer, dilute the specimen 1:2, 1:4, 1:8, 1:16, 1:32 or as needed
NOTE: Dilute buffer by adding 1 part buffer to 9 parts distilled water before use.3. Place one drop of each dilution on successive fields if the reaction slide.4. Gently resuspend the ASO latex reagent and add one drop to the reaction slide5. Use pipet/stir stick to spread reaction mixture over entire test field.6. Rotate slide for 2 minutes and immediately read under direct light.
INTERPRETATION OF RESULTS:Agglutination indicates a level of ASO in the sample equal or > 200 IU/mL.No agglutination indicates a level of ASO in the sample at < 200 IU/mL.
Prepared by:
Faminialagao, KateMedical Technologist
Checked by:
Jon Paul Reyes RMTChief Medical Technologist
Noted by:
Rozani Odono Navarro MD FPSPPathologist
Code:Page:
DANIEL MERCADO MEDICAL CENTERSerology and Immunology
Standard Operating Procedure
Issue Date: Revision Date:Revision No. 0.0
DEFINITION AND DESCRIPTION OF DENGUE NS1 (DENGUE EARLY RAPID)
INTENDED USE:The panbio dengue early rapid is a dengue NS1 antigen immunochromatographic assay. It is for the
qualitative detection of NS1 antigen in serum, used as an aid in the clinical laboratory diagnosis of patients with clinical symptoms consistent with dengue fever.
PRINCIPLE:When present in the patient sample, NS1 antigens tend to bind to colloidal gold complexes containing anti-
NS1 antibodies. This immune complex is captured by anti-NS1 antibodies immobilized in a line across the dipstick membrane to give a visible pink line. A procedural control in included to indicate that the assay has been performed correctly.
SPECIMEN COLLECTION AND PREPARATION:Blood obtained by venipuncture should be allowed to clot at room temperature and then centrifuged. The
serum should be separated as soon as possible and refridgerated (2-8◦C) or stored frozen (≤-20◦C) if not tested within two days. The use of icteric serum or serum exhibiting hemolysis, lipaemia or microbial growth is not recommended.
PROCEDURE:1. Add 50 uL of serum to the test provided2. Add 25 uL of running buffer to the test tube3. Add 25 uL of Gold conjugate to the test tube (before adding make sure the conjugate is mixed
thoroughly by inverting the bottle several times)4. Mix the reagents by gently tapping the test tube.5. Put the dipstick into the test tube to touch the bottom6. Start the timer7. Read the results exactly 15 minutes after adding the dipstick to the test tube8. Any trace of a pink line in the test area indicates a positive result9. Any results read outside 15 minutes should be considered invalid and must be repeated.
INTERPRETATION OF RESULTS:
POSITIVE: pink bands appear in the test and control regions. The test is positive for dengue NS1 antigen
NEGATIVE: A pink band appears in the control region only. No detectable dengue NS1 antigen. The result does not exclude dengue infection.
INVALID: no pink bands appear in the control region. The test is invalid and should be repeated.
Prepared by:
Faminialagao, KateMedical Technologist
Checked by:
Jon Paul Reyes RMTChief Medical Technologist
Noted by:
Anacleta B. Valdez MD FPSPPathologist
Code:Page:
DANIEL MERCADO MEDICAL CENTERSerology and Immunology
Standard Operating Procedure
Issue Date: Revision Date:Revision No. 0.0
DEFINITION AND DESCRIPTION OF TYPHOID IgG/IgM RAPID TEST CASETTE
INTENDED USE:The rapid test is a lateral flow immunoassay from the simultaneous detection and differentiation of anti-Salmonella typhi (S. typhi) IgG and IgM in human serum or plasma. It is intended to be used as a screening test and as an aid in the diagnosis of infection with S. typhi.
PRINCIPLE:The rapid test is a lateral flow chromatographic immunoassay. The test cassette consists of:
a) A burgundy colored conjugate pad containing recombinant S. typhoid H antigen and O antigen conjugate with colloid gold (Typhoid conjugates) and rabbit IgG-gold conjugates
b) A nitrocellulose membrane strip containing 2 test bands (T1 and T2 bands) and a control band (C band)The T1 band is pre-coated with monoclonal anti-human IgM for the detection of IgM anti-S. typhi, T2 band is pre-coated with reagents for the collection of IgG anti-S. typhi, and the C band is pre-coated with goat anti-rabbit IgG.
When an adequate volume of test specimen is dispensed into the sample well of the cassette , the test specimen migrates by capillary action across the test cassette. Anti-S. typhi IgM if present in the specimen will bind to thee typhoid conjugates. The immunocomplex is then captured on the membrane by a pre-coated anti-human IgM antibody, forming a burgundy colored T1 band, indicating an S. typhi IgM positive test result
Anti-S. typhi IgG if present in the patient specimen will bind to the typhoid conjugates. The immonocomplex is then captured on the membrane by pre-coated reagents forming a burgundy colored T2 band, indicating S. typhi IgG positive test result.
Absence of any T bands (T1 and T2) suggests a negative result. The test contains an internal control (C band) which should exhibit a burgundy colored band of the immunocomplex of goat anti-rabbit IgG/rabbit IgG-gold conjugate regardless of the color development on any of the T bands. Otherwise, the test result is invalid and the specimen must be retested with another device.
SPECIMEN COLLECTION AND HANDLING:Plasma:
a) Collect blood specimen into a lavender, blue or green top collection tube ( containing EDTA, citrate or heparin respectively in vacutainer) by venipuncture
b) Separate the plasma by centrifugationc) Carefully withdraw the plasma into new pre-labeled tube
Serum:a) Collect specimen into a red top collection (containing no anticoagulants in vacutainer) by venipunctureb) Allow blood to clotc) Separate the serum by centrifugationd) Carefully withdraw the serum into a new pre-labeled tube.
Test specimens as soon as possible after collecting. Store specimen at 2-8◦C if not tested immediately. Store specimen at 2-8◦C upto 5 days. Specimen should be frozen at -20◦C for longer storage
ASSAY PROCEDURE:a) Bring specimen and test components to room temperature if refridgerated or frozen. Mix the specimen well
prior to assay once thawed.b) When ready to test, open the pouch at the notch of the remove device. Place the test deice on a clean flat
surface.c) Be sure to label the device with specimens ID numberd) Fill pipette dropper with the specimen.e) Holding the dropper vertically dispense 1 drop (about 30-45 uL) of specimen into the sample well making
sure that there are no air bubbles.f) The add one drop (35-50uL) of Sample diluents immediatelyg) Set up the timerh) Results can be read in 15 minutes. Positive results can be visible in as short as one minute
****Don’t read result after 15 minutes. To avoid confusion, discard the test device after interpreting the result****
Prepared by:
Faminialagao, KateMedical Technologist
Checked by:
Jon Paul Reyes RMTChief Medical Technologist
Noted by:
Rozani Odono Navarro MD FPSPPathologist
Code:Page:
DANIEL MERCADO MEDICAL CENTERSerology and Immunology
Standard Operating Procedure
Issue Date: Revision Date:Revision No. 0.0
INTERPRETATION OF ASSAY RESULT:NEGATIVE RESULT: If only the C band is present, the absence of any burgundy color in the both t bands (T1 and T2) indicates that no anti-S. typhi antibody is detected in the specimen. The result is negative
POSITIVE RESULT: a.) In addition to the presence of C band, if only T1 band developed, the test indicates for the presences anti-S. typhi IgM in the specimen. The result is positive
b.) In addition to the presence of C band, if only T2 band developed, the test indicates for the presences anti-S. typhi IgG in the specimen. The result is positive
c.) In addition to the presence of C band, both T1and T2 bands are developed, the test indicates for the presences anti-S. typhi IgG and IgM in the specimen. The result is positive
Samples with positive results should be confirmed with alternative testing method(s) and clinical findings before a positive determination is made.
INVALID RESULT: If no C band is developed, the assay is invalid regardless of any burgundy color in the T bands. Repeat the assay with a new device.
Prepared by:
Faminialagao, KateMedical Technologist
Checked by:
Jon Paul Reyes RMTChief Medical Technologist
Noted by:
Rozani Odono Navarro MD FPSPPathologist
Code:Page:
DANIEL MERCADO MEDICAL CENTERSerology and Immunology
Standard Operating Procedure
Issue Date: Revision Date:Revision No. 0.0
DEFINITION AND DESCRIPTION OF WIDAL TEST
OBJECTIVE: Utilized to detect the presence of febrile antibodies present in human serum.
PRINCIPLE: Immunologic reaction between the antibodies produced to viable bacteria (agglutinins) abd their other various counterpart febrile antigens.
CLINICAL APPLICATION AND DISCUSSION: Febrile antigens (bacterial agglutination antigens) are bacterial suspensions for use in either slide or tube agglutination tests to detect the presence of bacterial agglutinins associated with bacterial infection or previous exposure to a related organism.
SPECIMEN: serum
STORAGE: Antigens and control sera should be stored at 2-8◦C until expiration
REAGENTS/MATERIALS:Typhoid H (Salmonella flagellar d antigen) typhoid O (salmonella somatic group d antigen) paratyphoid a (salmonella flagellar a antigen), paratyphoid b (salmonella flagellar b antigen) transparent plain glass ring slide, serum pipettes, applicator sticks, test tubes, 0.9% NaCl solution, Mechanical rotator.
PROCEDURE:1. Using a clear transparent glass slide, add the following amounts of serum to be tested from left to right:
0.08mL, 0.04mL, 0.02 mL, 0.01 mL, 0.005mL2. Prepare this set up for each antigen to be tested3. Shake the antigen gently to insure uniform suspension.4. Add one drop of antigen suspension just below each quantity of serum.5. Mix the serum and antigen well using a piece of applicator stick. Use separate applicator sticks to each
serum quantity or use the same stick and proceed from right to left.6. Rotate slide by hand or on a mechanical shaker at 150 rpm for 2-3 minutes7. Observe for agglutination using a microscope at low power field
INTERPRETATION OF RESULTS:The degree of agglutination is recorded as follows:
4+ = 100% of the organisms are agglutinated3+ = 75% of the organisms are agglutinated 2+ = 50% of the organisms are agglutinated1+ = 25% of the organisms are agglutinated +/- = less than 25% of the organisms are agglutinated NEGATIVE = No agglutination is observed
Prepared by:
Faminialagao, KateMedical Technologist
Checked by:
Jon Paul Reyes RMTChief Medical Technologist
Noted by:
Rozani Odono Navarro MD FPSPPathologist
Code:Page:
DANIEL MERCADO MEDICAL CENTERSerology and Immunology
Standard Operating Procedure
Issue Date: Revision Date:Revision No. 0.0
The serum dilution in the slide test are approximately equivalent to the test tube dilutions serum below:
Serum volume app. Tube dilution0.08 mL 1:200.04 mL 1:400.02 mL 1:800.01 mL 1:1600.005mL 1:320
Prepared by:
Faminialagao, KateMedical Technologist
Checked by:
Jon Paul Reyes RMTChief Medical Technologist
Noted by:
Rozani Odono Navarro MD FPSPPathologist
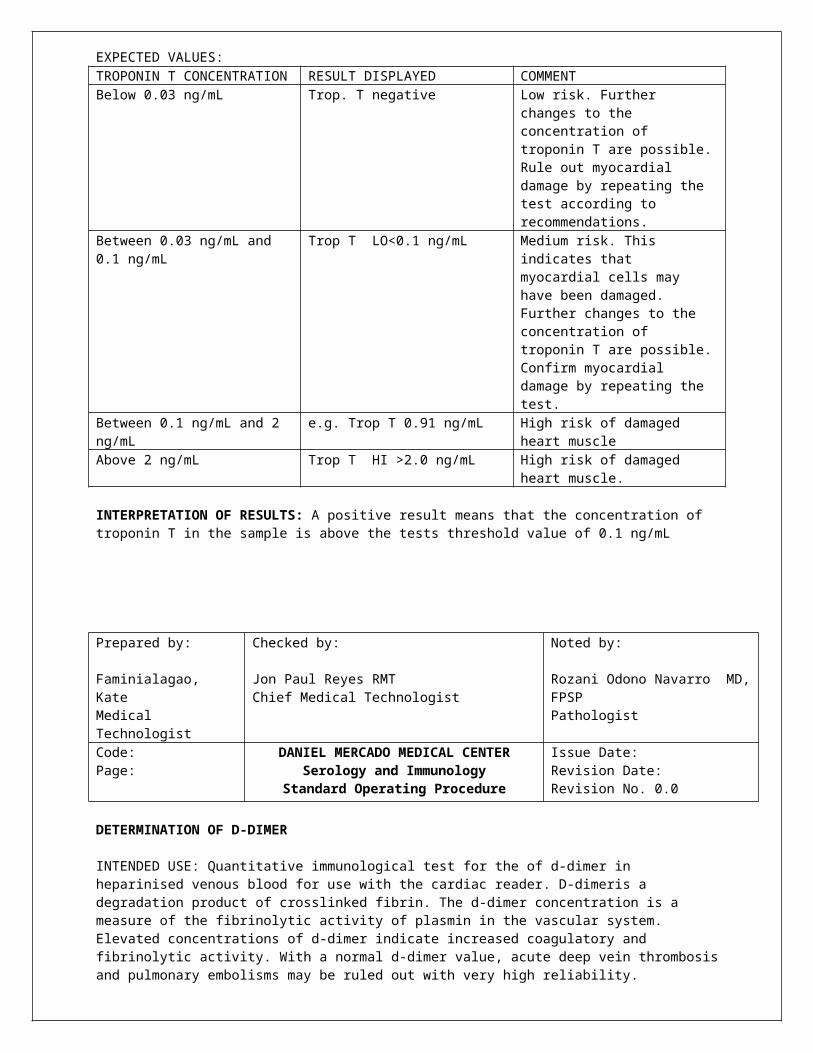
Code:Page:
DANIEL MERCADO MEDICAL CENTERSerology and Immunology
Standard Operating Procedure
Issue Date: Revision Date:Revision No. 0.0
TUBEX RAPID TYPHOID DETECTION
INTENDED USE: Tubex is a 10 minute semi quantitative in vitro diagnostic serum assay for the detection of current typhoid fever caused by Salmonella typhi. A positive result, together with clinical symptoms of typhoid fever is a strong indication of typhoid infection.
PRINCIPLE OF THE ASSAY: Tubex detects the presence of anti-O9 antibodies in the patient’s serum by assessing their ability to inhibit the reaction between the antigen coated brown and antibody coated blue reagents. The level of inhibition is proportional to the concentration of anti-O9 antibodies in the sample. Separation is enabled by magnetic force. Result is read visually against a color scale.SPECIMEN: Use clear serum samples of heparin plasma. Don not use EDTA or citrate plasma. Avoid grossly lipemic, icteric or hemolysed samples e.g. by haemoglobin (red color) and bilirubin (green color), may disturb the color of the supernatant and result in intermediate assay results. The serum samples should be stored at 2-8◦C or frozen if not used immediately.
MATERIALS:Tubex brown reagentTubex blue reagentTubex positive controlTubex negative controlTubex reaction well strip Tubex sealing tape
PROCEDURE:1. Place the tubex reaction well strip upright on the bench, well number face-front (do not place the strip on
the color scale yet)2. Add 45 uL of tubex brown reagent to each well3. Add 45 uL of sample, positive control or negative control to appropriate wells and carefully mix by
pipetting up and down 10 times. Thorough mixing is essential. Avoid foaming. Use a new pipette for each sample.
4. Incubate on the bench for 2 minutes.5. Add 90 uL of tubex blue reagent to each well.6. Cover the tubex reaction well strip with tubex sealing tape. Press the tape hard against the plastic to
prevent leakage7. Mixing should be performed using the following procedure:
a) Hold the reaction well strip across at one end using one hand’s thumb and pointing finger.b) Tilt the reaction well strip horizontally (90◦) to expose maximum well surface for the mixture.c) Shake the reaction well strip rapidly backwards and forwards for 2 minutes. Make sure that the
contents flow across the entire exposed well surface.8. Place the reaction well strip on the tubex color scale as far left as possible. Allow separation for 5 minutes
to obtain clear supernatant.
Prepared by:
Faminialagao, KateMedical Technologist
Checked by:
Jon Paul Reyes RMTChief Medical Technologist
Noted by:
Rozani Odono Navarro MD FPSPPathologist
Code:Page:
DANIEL MERCADO MEDICAL CENTERSerology and Immunology
Standard Operating Procedure
Issue Date: Revision Date:Revision No. 0.0
INTERPRETATION OF RESULTS:Read and score the results by comparing the color of each supernatant to the tubex color scale. Reading
should be performed at good light conditions within 30 minutes after separation, although results are stable for hours if not disturbed. Do not interpret results or reseparate reactions if the reaction well strip is accidentally tipped over during or after separation
Assay interpretation guide:SCORE INTERPRETATION GUIDE
≤2 NEGATIVE: No indication of current typhoid fever infection.
3 Borderline, inconclusive score. Repeat analysis. If still inconclusive, repeat sampling at a later date
4 WEAK POSITIVE: indication of current typhoid fever infection
6 – 10 POSITIVE: Strong indication of current typhoid fever infection.
INDETERMINATE No clear score obtained due to:a) Poor adherence to assay protocol. Repeat
analysis.b) Poor specimen quality. Repeat sampling and
analysis.
Prepared by:
Faminialagao, KateMedical Technologist
Checked by:
Jon Paul Reyes RMTChief Medical Technologist
Noted by:
Rozani Odono Navarro MD FPSPPathologist
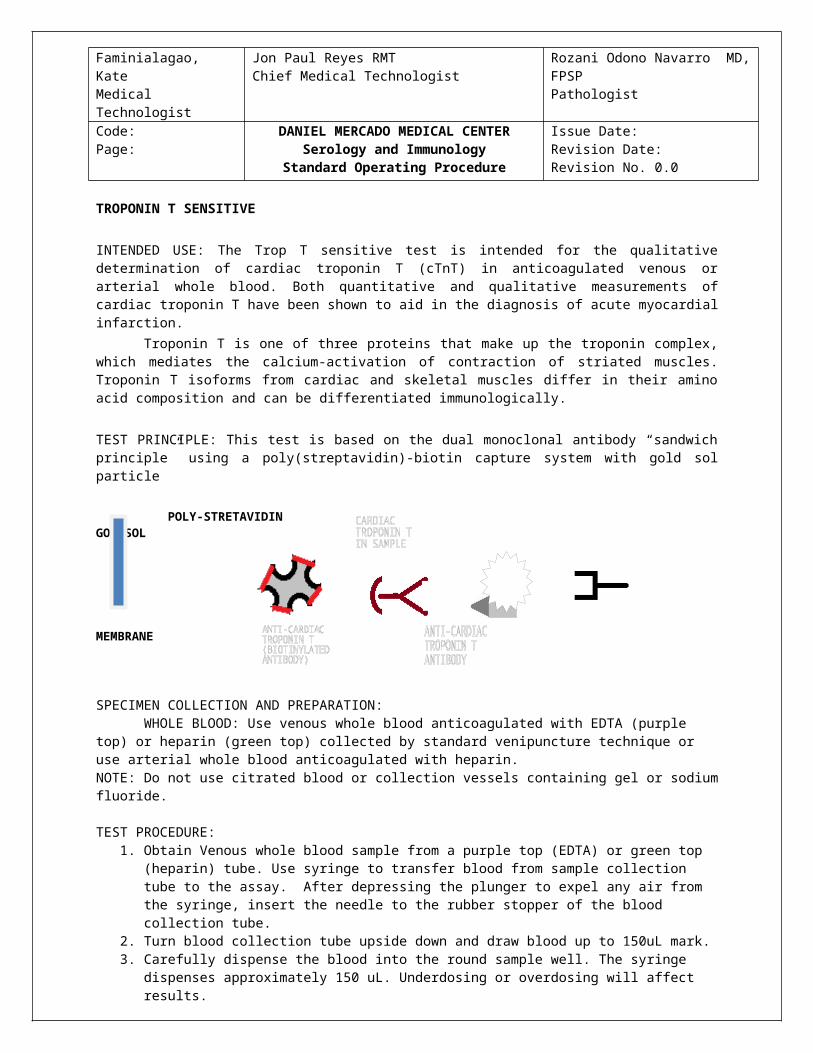
Code:Page:
DANIEL MERCADO MEDICAL CENTERSerology and Immunology
Standard Operating Procedure
Issue Date: Revision Date:Revision No. 0.0
DEFINITION AND DESCRIPTION OF H. pylori ANTIBODY TEST
INTENDED USE:H.pylori antibody test is a rapid immunochromatographic assay for the detection of antibodies to H. pylori
in human whole blood, ser or plasma. The assay is to provide an aid in diagnosis of H. pylori infection. Helicobacter pylori is a corkscrew-shaped, gram-negative rod that lives in the mucous layer of the stomach.
H. pylori infection is now accepted as the most common cause of gastritis, and is etiologically involved in gastric ulcer, duodenal ulcer, gastric adenocarcinoma and primary gastric B-cell lymphoma.
PRINCIPLE:H. pylori antibody test employs chromatographic lateral flow test device in a cassette format. Colloidal
gold conjugate H. pylori antigens (Au-Ag) are dry-immobilized at the end of nitrocellulose strip. H. pylori antigens are bond at the test zone (T). when sample is added, it migrates by capillary diffusion rehydrating the gold conjugate. If anti-H. pylori antibodies present in sample, antibodies will bind with the gold conjugated antigens forming particles. These particles will continue to migrate along the strip until the test zone (T) where they are captured by H. pylori antigens generating a visible red line. If there are no anti-H. pylori antibodies in the sample, no red line is formed in the test zone (T). A built-in control line will always appear in the control zone © when the test is performed properly, regardless of the presence or absence of anti-H. pylori antibodies in the specimen.
SPECIMEN COLLECTION AND PREPARATION:1. No prior special preparation of the patient is required before sample collection by approved techniques.2. Fresh serum/plasma is preferable. Serum/plasma may be stored at 2-8◦C up to 3 days in case of delay of
testing, for long-term storage, freeze the specimen at -20◦C for 3 months.3. The test works best on fresh whole blood samples. If testing cannot be done immediately, blood samples
collected with a suitable anticoagulant such as EDTA or heparin or oxalate should be stored at 2-8◦C up to 3 days. Blood samples should not be frozen.
4. Repeated freezing and thawing of specimen should be avoided5. Do not use hemolysed, clotted, contaminated, lipemic and viscous/turbid specimen.6. Specimen containing precepitates or particulate matter must be centrifuged and the clear supernate only
used for testing.7. Do not heat inactivate the sample.
PROCEDURE:1. Bring kit components to room temperature before testing2. Open the pouch and remove the card. Once opened, the test card must be used immediately. 3. Label the test card with patients identity4. Apply 3 drops (120-150uL) of serum, plasma or whole blood to the sample well marked as “S”5. At the end of 10 minutes read the results. A strong positive sample may show earlier results.
INTERPRETATION OF RESULTS:1. NEGATIVE: only control line appears2. POSITIVE: both control line and the test line appear. It indicates the antibodies to H. pylori have been
detected.3. INVALID: if after 10 minutes no line is visible within the control zone, the result is invalid. The test
should be repeated with a new test card
Prepared by:
Faminialagao, KateMedical Technologist
Checked by:
Jon Paul Reyes RMTChief Medical Technologist
Noted by:
Rozani Odono Navarro MD FPSPPathologist
Code:Page:
DANIEL MERCADO MEDICAL CENTERSerology and Immunology
Standard Operating Procedure
Issue Date: Revision Date:Revision No. 0.0
DEFINITION AND DESCRIPTION OF ONE STEP HBsAg TEST
INTENDED USE:The HBsAg test is a rapid one step immunochromatographic assay for the detection of hepatitis B surface
antigen (HBsAg) in human serum or plasma. The presence of 5 ng/mL HBsAg can be detected within 10 minutes and 1 ng/mL HBsAg in 15 minutes. The test provides visual qualitative result.
PRINCIPLE:One step HBsAg is a colloidal gold enhanced immunoassay that detects hepatitis B surface antigen in
human serum or plasma. The sample initially reacts with the monoclonal antibody-colloidal gold conjugate in the sample pad. This mixture migrates across the membrane by capillary action and reacts with the anti-HBsAg in the test region. If the sample contains HBsAg a line will form on the membrane a \t this point. If the antigen is not present in the sample no line is formed, indicating a negative result. The mixture continues to flow to the control area of the membrane, whre it forms a line indicating the test result is valid.
SPECIMEN COLLECTION:1. Serum or plasma may be used in this test. Anticoagulants typically used for blood collection do not
interfere with the test.2. Remove serum or plasma from the clot or red cells as soon as possible to avoid hemolysis.3. Hemolysed, extremely thickened or fatty specimens are NOT suitable for this assay. Specimens containing
particulate matter may give inconsistent results and should be clarified prior to testing.4. Serum or plasama specimens should be refridgerated 2-8◦C upto 3 days and frozen at -20◦C for longer
periods.5. Avoid frequent thaw-and-freeze of specimen (more than 3 days).
ASSAY PROCEDURE:Do not open pouch until you are ready to test the sample.
For test strips:1. Bring all reagents and specimen to room temperature.2. Remove the test strip from the foil pouch and place on a clean dry surface.3. Identify the test strip for each specimen or control.4. Apply at least 80uL of specimen to the sample pad behind the (↓↓↓) mark at the bottom of the strip.5. Interpret test results at 15 minutes.
For test cards:1. Bring all reagents and specimen to room temperature.2. Remove the test strip from the foil pouch and place on a clean dry surface.3. Identify the test strip for each specimen or control.4. Dispense 100uL (3 drops) of the specimen or control into the sample well on the card5. Interpret test results at 15 minutes.
CAUTION: use a clean pipette or tip for every sample to avoid cross-contamination Do not interpret results after 20 minutes
It is recommended to run a known positive and negative control in each performance to ensure the assay procedure.
INTERPRETATION OF RESULTS:1. NEGATIVE: only one purplish red test band appears in the control region2. POSITIVE: in addition to the control purplish red test band, a distinct purplish red band also
appears in the test region.3. INVALID: Neither test band nor control band appears. The specimen should be tested again using
a new test card
Prepared by:
Faminialagao, KateMedical Technologist
Checked by:
Jon Paul Reyes RMTChief Medical Technologist
Noted by:
Rozani Odono Navarro MD FPSPPathologist
Code:Page:
DANIEL MERCADO MEDICAL CENTERSerology and Immunology
Standard Operating Procedure
Issue Date: Revision Date:Revision No. 0.0
DEFINITION AND DESCRIPTION OF ANTI-Treponema pallidum TEST
INTENDED USE:The anti-TP (Treponema pallidum / Syphilis) test is a rapid, serological, immunochromatographic assay for
the detection of antibodies to syphilis antigen in human serum or plasma. The test is used to obtain a visual, qualitative result and is intended for healthcare professional use. Applications of the test include: screen test for sexually transmitted diseases (STD’s) among high-risk group of people, regular health examinations, and field screen test for blood bank.
SUMMARY AND BIOLOGICAL PRINCIPLE OF THE ASSAY: The anti-TP (Treponema pallidum / Syphilis) test uses double antigen “sandwich principle” for the
detection of syphilis antibody in human serum. A recombinant syphilis antigen (TP Ag2) is immobilized in the test band region, and an antibody to syphilis on the control band region of nitrocellulose membrane. Another TP antigen (TP Ag1), coupled with colloidal particles, is dried on a conjugate pad. During the assay, the specimen is allowed to react with the colored conjugate (antigen-colloid gold conjugate); the mixture then migrates chromatographically along the membrane by capillary action. If the specimen contains syphilis antibody, the recombinant antigen immobilized on the membrane will capture the antibody-antigen-colloidal-gold complex and form a colored test band on the membrane, indicating a positive result. Absence of the test band suggest a negative result. To serve as a procedural control, a colored band at control region always appears in the test area.
SAMPLE COLLECTION AND STORAGE:1. No prior special preparation of the patient is required before sample collection by approved techniques.2. Fresh serum is preferable. Serum may be stored at 2-8◦C up to 3 days in case of delay of testing, for long-
term storage, freeze the specimen at -20◦C for 3 months.3. Repeated freezing and thawing of specimen should be avoided4. Do not use hemolysed, clotted, contaminated, lipemic and viscous/turbid specimen.5. Specimen containing precepitates or particulate matter must be centrifuged and the clear supernate only
used for testing.6. Do not heat inactivate the sample.
ASSAY PROCEDURE:For test cards:
1. Bring all reagents and specimen to room temperature.2. Remove the test strip from the foil pouch and place on a clean dry surface.3. Identify the test strip for each specimen or control.4. Dispense 100uL (3 drops) of the specimen or control into the sample well on the card5. Interpret test results at 15 minutes. DO NOT INTERPRET RESULTS AFTER 20 MINUTES
For test strips:1. Bring all reagents and specimen to room temperature.2. Remove the test strip from the foil pouch and place on a clean dry surface.3. Identify the test strip for each specimen or control.4. Apply at least 80uL of specimen to the sample pad behind the (↓↓↓) mark at the bottom of the strip.5. Interpret test results at 15 minutes. . DO NOT INTERPRET RESULTS AFTER 20 MINUTES
CAUTION: use a clean pipette or tip for every sample to avoid cross-contamination
IINTERPRETATION OF RESULTS: The presence or absence of syphilis antibody provides useful information on the status of individuals with infection for syphilis.
1. NEGATIVE: only one purplish red test band appears in the control region2. POSITIVE: in addition to the control purplish red test band, a distinct purplish red band also
appears in the test region.3. INVALID: Neither test band nor control band appears. The specimen should be tested again using
a new test card.
Prepared by:
Faminialagao, KateMedical Technologist
Checked by:
Jon Paul Reyes RMTChief Medical Technologist
Noted by:
Rozani Odono Navarro MD FPSPPathologist
Code:Page:
DANIEL MERCADO MEDICAL CENTERSerology and Immunology
Standard Operating Procedure
Issue Date: Revision Date:Revision No. 0.0
DEFINITION AND DESCRIPTION OF THE RAPID ANTI-HIV (1&2) TEST
INTENDED USE:THE RAPID ANTI-HIV(1&2) TEST IS A COLLOIDAL GOLD ENHANCED, RAPID IMMUNOCHROMATOGRAPHIC ASSAY FOR THE QUALITATIVE DETECTION OF ANTIBODIES TO HUMAN IMMUNODEFFICIENCY VIRUS (HIV) IN HUMAN WHOLE BLOOD, SERUM OR PLASMA. THIS TEST IS A SCREENING TEST, AND ALL POSITIVES MUST BE CONFIRMED USING AN ALTERNATE TEST SUCH AS WESTERN BLOT. THE TEST IS INTENDED FOR HEALTHCARE PROFESSIONAL USE ONLY.
SUMMARYThe human immunodeficiency virus (HIV) is the causative agent of acquired immune deficiency syndrome (AIDS). The general method of detecting infection with HIV is to observe the presence of antibodies to the virus by an EIA method followed by confirmation with Western Blot. The Advanced Quality Rapid Anti-HIV(1&2) Test is a simple, visual qualitative test that detects antibodies in human whole blood serum or plasma. The test is based on immunochromatography and can give a result within 15 minutes.
PRINCIPLE OF THE PROCEDUREThe assay starts with a sample applied to the sample well. A recombinant HIV antigen conjugated to colloidal gold embedded in the sample pad reacts with the HIV antibody present in serum or plasma sample forming conjugate/HIV antibody complex. As the mixture is allowed to migrate along the test strip, the conjugate/HIV antibody complex is captured by recombinant HIV antigen immobilized on the forming a colored test band in the test region. A negative sample does not produce a test band due to the absence of colloidal gold conjugate/HIV antibody complex. The antigens used in the conjugate test are recombinant proteins that correspond to highly immunoreactive regions of HIV1 and HIV2. A colored control band in the control region appears at the end of test procedure regardless of test result. The control band indicates that the colloidal gold conjugate binding to the anti-HIV antibody immobilized on the membrane. The control band indicates that the colloidal gold conjugate is functional.
SAMPLE COLLECTION AND STORAGE:1. Collect serum or plasma specimens following regular clinical laboratory procedures2. Sample may be stored at 2-8◦C up to 3 days in case of delay of testing, for long-term storage, freeze the
specimen at -20◦C for 3 months.3. Repeated freezing and thawing of specimen should be avoided
ASSAY PROCEDURE:For test cards:
1. Bring all reagents and specimen to room temperature.2. Remove the test strip from the foil pouch and place on a clean dry surface.3. Identify the test strip for each specimen or control.4. Dispense 100uL (3 drops) of the specimen or control into the sample well on the card5. Interpret test results at 15 minutes. DO NOT INTERPRET RESULTS AFTER 20 MINUTES
For test strips:1. Bring all reagents and specimen to room temperature.2. Remove the test strip from the foil pouch and place on a clean dry surface.3. Identify the test strip for each specimen or control.4. Apply at least 80uL of specimen to the sample pad behind the (↓↓↓) mark at the bottom of the strip.5. Interpret test results at 15 minutes. . DO NOT INTERPRET RESULTS AFTER 20 MINUTES
CAUTION: use a clean pipette or tip for every sample to avoid cross-contamination It is recommended to run a known positive and negative control in each performance to ensue the assay procedure.
Prepared by:
Faminialagao, KateMedical Technologist
Checked by:
Jon Paul Reyes RMTChief Medical Technologist
Noted by:
Rozani Odono Navarro MD FPSPPathologist
Code:Page:
DANIEL MERCADO MEDICAL CENTERSerology and Immunology
Standard Operating Procedure
Issue Date: Revision Date:Revision No. 0.0
INTERPRETATION OF RESULTS:1. NEGATIVE: only one purplish red test band appears in the control region. The absence of the test
band indicates a negative result2. POSITIVE: both purplish red control band appears on the membrane. The lower the antibody
concentration the weaker the test band.3. INVALID: Neither test band nor control band appears. The specimen should be tested again using
a new test card.NOTE: it is normal to have a slightly lightened control band with very strong positive results as long as it is distinctly visible.
Prepared by:
Faminialagao, KateMedical Technologist
Checked by:
Jon Paul Reyes RMTChief Medical Technologist
Noted by:
Rozani Odono Navarro MD FPSPPathologist
Code:Page:
DANIEL MERCADO MEDICAL CENTERSerology and Immunology
Standard Operating Procedure
Issue Date: Revision Date:Revision No. 0.0
DEFINITION AND DESCRIPTION OF MALARIA (P.f./P.v.) TRI-LINE TEST
INTENDED USE:The malaria (P.f./P.v.) test is a two site sandwich immunoassay utilizing whole blood for the detection of
P. falciparum specific histidine rich protein 2 (Pf HRP-2) and P. vivax specific pLDH. The test can also be used for specific detection and differentiation of P. falciparum and P. vivax malaria.
PRINCIPLE OF TEST:A capture monoclonal antibody is immobilized on the nitrocellulose strip. The red blood cells are lysed
releasing Pf hrp-2 and P.vivax specific pLDH which binds selectively to this antibody as the blood is wicked up the strip. The signal reagent is coated with specific antibodies which bind with the antigen-antibody complex, producing a black line. The presence of an upper black line (the procedural control line) demonstrates the test has been performed correctly.
SAMPLE COLLECTION AND STORAGE:1. Collect whole blood specimens following regular clinical laboratory procedures2. Sample may be stored at 2-8◦C if not used the same day of collection.
BEFORE TESTING:1. Bring device, sample diluents and specimen to room temperature2. Remove test card/strip from the sealed pouch.
a) Select a finger for puncture, usually the side of the third or fourth finger. b) Clean with antiseptic and allow to airdry.c) Puncture the finger with a sterile lancet.d) Blood will well to the surface. Redo procedure on another finger if necessary.e) Collect blood using the plastic dropper provided.
ASSAY PROCEDURES:For test cards:
1. Bring all reagents and specimen to room temperature.2. Remove the test strip from the foil pouch and place on a clean dry surface.3. Dispense 1 drop (10uL) of whole blood to the “S” well of the test card using the plastic dropper provided.4. Dispense 100uL (3 drops) of sample diluents to the “D” well after the specimen is added5. Interpret test results at 15 minutes. DO NOT INTERPRET RESULTS AFTER 30 MINUTES
For test strips:1. Bring all reagents and specimen to room temperature.2. Remove the test strip from the foil pouch and place on a clean dry surface.3. Identify the test strip for each specimen or control.4. Apply at least 10uL of specimen to the sample pad behind the (↓↓↓) mark at the bottom of the strip.5. Add 3 drops of sample diluent at the same place.6. Interpret test results at 15 minutes. . DO NOT INTERPRET RESULTS AFTER 30 MINUTES
CAUTION: use a clean pipette or tip for every sample to avoid cross-contamination NOTES:
1. Applying sufficient amount of sample diluents is essential for a valid test result. If migration (the wetting of membrane) is not observed in the test window after 1 minutes, add one more drop of diluents to sample well.
2. The positive results could appear as soon as 1 minute for a sample with high levels of malaria.3. Do not interpret results after 30 minutes.
Prepared by:
Faminialagao, KateMedical Technologist
Checked by:
Jon Paul Reyes RMTChief Medical Technologist
Noted by:
Rozani Odono Navarro MD FPSPPathologist
Code:Page:
DANIEL MERCADO MEDICAL CENTERSerology and Immunology
Standard Operating Procedure
Issue Date: Revision Date:Revision No. 0.0
IINTERPRETATION OF RESULTS:1. NEGATIVE: only the black control band appears on the membrane. The absence of a test band
indicates a negative result2. POSITIVE: control line and at least one test line appear on the membrane. The appearing of T1
test line indicates a Pf. HRP-2 positive result, the appearing of T2 test line indicates a P. vivax specific pLDH positive result, the appearing of both T1 and T2 test lines indicates both Pf. HRP-2 and P. vivax specific pLDH positive result. The lower the antigen concentration is, the weaker the test line is.
3. INVALID: there should always be a black control band in the control region regardless of test result. If control band is not seen, the test is considered invalid. Repeat the test using a new test device.
NOTE: it is normal to have a slightly lightened control band with very strong positive results as long as it is distinctly visible.
Prepared by:
Faminialagao, KateMedical Technologist
Checked by:
Jon Paul Reyes RMTChief Medical Technologist
Noted by:
Rozani Odono Navarro MD FPSPPathologist
Code:Page:
DANIEL MERCADO MEDICAL CENTERSerology and Immunology
Standard Operating Procedure
Issue Date: Revision Date:Revision No. 0.0
DEFINITION AND DESCRIPTION OF ANTI-HCV RAPID TEST KIT
INTENDED USE
THE RAPID ANTI-HCV TEST IS A COLLOIDAL GOLD ENHANCED, RAPID IMMUNOCHROMATOGRAPHIC ASSAY FOR THE QUALITATIVE DETECTION OF ANTIBODIES TO HEPATITIS C VIRUS (HCV) IN HUMAN WHOLE BLOOD, SERUM OR PLASMA. THIS TEST IS A SCREENING TEST AND ALL POSITIVES MUST BE CONFIRMED USING AN ALTERNATE TEST SUCH AS WESTERN BLOT. THE TEST IS INTENDED FOR HEALTHCARE PROFESSIONAL USE ONLY.
SUMMARY
The general method of detecting infection with HCV is to observe the presence of antibodies to the virus by an EIA method followed by confirmation with Western Blot. The Advanced Quality Rapid Anti-HCV Test is a simple, visual qualitative test that detects antibodies in human whole blood, serum or plasma. The test is based on immunochromatography and can give a result within 15 minutes.
PRINCIPLE OF THE PROCEDURE
The assay starts with a sample applied to the sample well and add provided sample diluent immediately. The HCV antigen-colloidal gold conjugate embedded in the sample pad reacts with the HCV antibody present in blood, serum or plasma sample forming conjugate/HCV antibody complex. As the mixture is allowed to migrate along the test strip, the conjugate/HCV antibody complex is captured by a antibody-binding protein A immobilized on a membrane forming a colored test band in the test region. A negative sample does not produce a test line due to the absence of colloidal gold conjugate/HCV antibody complex. The antigens used in the test are recombinant proteins corresponding to highly immunoreactive regions of HCV. A colored control band in the control region appears at the end of test procedure regardless of test result. This control band is the result of colloidal gold conjugate binding to a anti-HCV antibody immobilized on the membrane. The control line indicates that the colloidal gold conjugate is functional. The absence of the control band indicates that the test is invalid.
SAMPLE COLLECTION AND STORAGE:1. Collect serum or plasma specimens following regular clinical laboratory procedures2. Sample may be stored at 2-8◦C if not used the same day of collection.
ASSAY PROCEDURE
1. Dispense 1 drop (10μl) of whole blood, serum or plasma specimen to the “S” well of the test card using the plastic dropper provided according to the figure.
2. Add two drops of Sample Diluent to the “D” well after the specimen is added. 3. Interpret test results at 15 minutes.
NOTES:1. Applying sufficient amount of sample diluent is essential for a valid test result. If migration (the wetting of
membrane) is not observed in the test window after one minute, add one more drop of diluent to sample well.
2. The positive results could appear as soon as 1 minute for a sample with high levels of HCV antibodies. 3. Do not interpret result after 20 minutes.
READING THE TEST RESULTS
1. Positive: Both purplish red test band and purplish red control band appear on the membrane. The lower the antibody concentration, the weaker the test band.
2. Negative: Only the purplish red control band appears on the membrane. The absence of a test band indicates a negative result.
3. Invalid: There should always be a purplish red control band in the control region regardless of test result. If control band is not seen, the test is considered invalid. Repeat the test using a new test device.
Note: It is normal to have a slightly lightened control band with very strong positive samples as long as it is distinctly visible.
Prepared by:
Faminialagao, KateMedical Technologist
Checked by:
Jon Paul Reyes RMTChief Medical Technologist
Noted by:
Rozani Odono Navarro MD FPSPPathologist