Embed Size (px)
Citation preview

h
81l
Early-Stage Hodgkin Disease in a24-Year-Old Woman
Christopher Peters, Eli Glatstein, Julie Vose, Lisa C. Thomas, and Gloria J. Morris
dtaceaulcpon
dtlfa
nnttwp(gcr
Gcart3
seue
At times we encounter clinical prob-lems for which there are no directly ap-plicable evidence-based solutions, butwe are compelled by circumstances toact. When doing so we rely on relatedevidence, general principles of bestmedical practice, and our experience.Each “Current Clinical Practice” featurearticle in Seminars in Oncology de-scribes such a challenging presenta-tion and offers treatment approachesfrom selected specialists. We invitereaders’ comments and questions,which, with your approval, will be pub-lished in subsequent issues of the Jour-nal. It is hoped that sharing our viewsand experiences will better inform ourmanagement decisions when we nextencounter similar challenging patients.Please send your comments on thearticles, your challenging cases, andyour treatment successes to me [email protected]. I lookforward to a lively discussion.
Gloria J. Morris, MD, PhDCurrent Clinical Practice Feature Editor
Hodgkin lymphoma is consid-ered relatively uncommonby the National Compre-
ensive Cancer Network (NCCN)1
and the American Cancer Society(ACS),2 with 2010 statistics showing,490 new cases diagnosed and,320 deaths attributable. Epidemio-
ogic statistics show that Hodgkin
Address correspondence to Gloria J. Morris,MD, PhD, Editor, Current Clinical Practice,Hematology and Oncology Associates ofNortheastern PA, PC, 1100 Meade St, Dun-more, PA 18512. E-mail: [email protected]
0270-9295/ - see front matter© 2011 Published by Elsevier Inc.
doi:10.1053/j.seminoncol.2011.06.003Seminars in Oncology, Vol 38, No 6, Decem
isease (HD) incidence peaks be-ween 15 and 30 years of age, andgain after age 55. HD is classified aslassical, characterized by the pres-nce of the Reed-Sternberg (RS) cell,nd includes subcategories of nod-lar sclerosis, mixed cellularity,
ymphocyte-depleted, and lympho-yte-rich, all accounting for ap-roximately 95% of cases, and 5%f cases are lymphocyte-predomi-ant.1,3
Staging is according to the AnnArbor Staging System, and takes intoaccount the affected lymph nodegroups on either side of the muscu-lar diaphragm, and presence in thebone marrow; favorable status also
epends on whether systemic fac-ors, such as unexplained weightoss (�10% of total body weight),evers, drenching night sweats, arebsent (A) or present (B).
Early stage favorable HD witho B symptoms or large mediasti-al lymphadenopathy is usuallyreated with combined modalityherapy, followed by restagingith positron emission tomogra-hy (PET)/computed tomographyCT). Additional chemotherapy isiven based on the obtaining of aomplete remission (CR) or partialemission (PR).
For stage IIA favorable HD, NCCNuidelines recommend continuedhemotherapy if the patient is in CR,nd chemotherapy or involved-filedadiation therapy (IFRT) for PR. Initialreatment has been compared with6 Gy and the Stanford V regimen.4,5
ABVD (doxorubicin, bleomycin, vin-blastine, and dacarbazine) has beendeemed an alternative to MOPP(meclhorethamine, vincristine, pred-
nisone, and procarbazine) with lowerber 2011, pp 705-713
risks of sterility and secondary leuke-mias.6 Other options include that pre-ented in the German Hodgkin Dis-ase Study Group-HD7 trial, whichsed two cycles of ABVD followed byxtended-filed radiation therapy.7 In
addition, a National Cancer Instituteof Canada Clinical Trials Group/East-ern Cooperation Oncology Groupstudy assessed chemotherapy alone8–10
as an option for early-stage HD. A Me-morial Sloan-Kettering Cancer CenterStudy showed equivalent duration ofcomplete response, time to progres-sion, and overall survival in patientstreated with ABVD plus radiation com-pared with those treated with ABVDalone.11
Tailoring these many options topatients and balancing both short-term and long-term risks requiressignificant consideration and discus-sion with the patient. In particular,issues specific to young women,such as impact on fertility, must beweighted.12,13
We present here a case of a 24-year-old woman, soon to be mar-ried, who was diagnosed withearly stage IIA HD, initially treatedwith ABVD, who had an excellentresponse on PET scan. We posethe following questions: (1) Giventhe patient’s excellent response tochemotherapy, would you offer ra-diation therapy, further chemo-therapy, or observation? (2) Howshould this be followed? (3) In theevent of recurrence, what furthertreatment course should the pa-tient embark upon? (4) What is herfuture risk for second malignan-cies? (5) What effects will the cur-rent treatment option have on the
patient’s future fertility?705

706 C. Peters et al
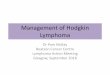
Figure 1. Excision of right supraclavicular lymph node showing classicial Hodgkin’s lymphoma, nodular sclerosis type. (A) 40xview highlighting Reed-Sternberg (RS) cell variants as well as lacunar cells (bottom left corner). (B) RS cell variants in acharacteristic background infiltrate composed of eosinophils, lymphocytes, plasma cells, and histiocytes. (C) 100x viewshowing the mixed cellular (eosinophils, lymphocytes, and histiocytes) background of classic Hodgkins’ lymphoma. (D)High-power view of lacunar cells characteristic for the nodular sclerosis type of Hodgkin lymphoma. (E) Membrane positivityin typical pattern of CD15 expression in RS cells of HD, and background expression in neutrophils. (F) Membrane positivity intypical pattern of both CD15 and CD30 expression in RS cells, with accentuation in the Golgi area of the cytoplasm. Figures
courtesy of Dr. Navid Ahmad, Department of Pathology, Pennant Laboratory Services, Wilkes-Barre, PA.
g3
saIC
Early-stage Hodgkin disease 707
THE PROBLEM
Case Report
A 24-year-old woman palpated anenlarged right cervical lymph nodeand presented to an urgent care fa-cility, where she was noted to havean elevated white blood cell (WBC)count, and was put on antibioticsfor presumed infection. She had aninitial partial response to the antibi-otics. She saw a surgeon, and a fine-needle aspirate of the cervical lymphnode was inconclusive. Three monthslater, she noticed an increase in thesize and number of enlarged lymphnodes in the neck and bilaterally inthe supraclavicular areas. She deniedany “B-type” symptoms, includingnight sweats, weight loss, anorexia,rash, or flulike symptoms. The lymphnodes were nontender. She under-
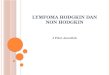
Figure 2. FDG-whole body PET scan imhowing hypermetabolic activity in cernd coronal sections (E and F), showingmages courtesy of Al Zelna, Dennis Saventer, Scranton, PA.
went an excisional biopsy of a
right supraclavicular lymph node,which showed Hodgkin lymphoma,with occasional multinucleated RSvariants and classical RS cells identi-fied, nodular sclerosis type, with im-munohistochemistry positive forCD15 and CD30, focally positive forBCL-2 and CD20, and negative forCD3, CD5, CD10, BCL-6, and PAX-5(Figure 1). Peripheral bloodworkshowed WBC count 10.9K/�L, hem-lobin 13.6 g/dL, platelet count75K/�L, normal blood chemistry,
and lactate dehydrogenase 168 U/L(reference range, 100–190). A chestx-ray showed no enlarged mediastinalmass or increase in thoracic ratio.
The patient underwent stagingstudies for HD including a CT scan ofthe chest, abdomen, and pelvis, aswell as a PET scan, which showedhypermetabolic right supraclavicular,
s with low-dose CT scan pretreatmentsupraclavicular, and mediastinal lymp
reased metabolic activity in cervical, supChristopher N. Hobbie, MD, and Jonat
paratracheal, and mediastinal lymph-
adenopathy only, with no otherlymph nodes seen below the dia-phragm. A bilateral bone marrow bi-opsy showed no evidence of RS cellsor lymphoma. Other pretreatmentstudies included a multi-gated acquisi-tion scan (MUGA) scan, whichshowed a normal left ventricular ejec-tion fraction at 69%, and pulmonaryfunction testing, which showed nor-mal spirometry, normal lung volumes,and normal diffusing capacity.
The patient was married 3 weeksafter the lymph node biopsy. Egg har-vesting was offered and declined.
She was given four cycles ofchemotherapy in the form ofABVD. A mid-treatment CT scanshowed a significant decrease inthe cervical, supraclavicular, andmediastinal lymph nodes (Figure1), and after four cycles a repeat
ial (A) and coronal sections (B and C),des; and post-treatment in in axial (D)avicular, and mediastinal lymph nodes.Sullum, MD, Northeastern PA Imaging
age in axvical, h nodec raclitski, hon
PET/CT showed no hypermeta-

ld
factc
708 C. Peters et al
bolic activity and mild persistenceof a small supraclavicular lymphnode only (Figure 2). She is nowevaluated for further treatment.
RADIATIONONCOLOGIST’S OPINION
Radiation therapy has a rich his-tory in the efficacious treatment ofHodgkin lymphoma. Its current use,like any therapeutic intervention,must be placed in the context of itsefficacy versus its side effects.Shortly after the discovery of thex-ray by Roentgen in 1896, radio-therapy started to be used with suc-cess in the palliation of HD adenop-athy. There were many limitationsof radiotherapy in the early 1900s,mostly due to the relatively primi-tive electrical circuitry of the time.Radiotherapy was the first curativetherapy for HD; with initial reportsof cure documented in 1950. Priorto this, HD was a universally fataldisease, and a substantial majority ofpatients suffered significant morbid-ity prior to death. In her classic pa-per published in 1950, Peters re-ported on the Princess MargaretHospital experience using large ra-diation fields treating known diseaseand adjacent uninvolved nodal re-gions, leading to the cure of the ma-jority of their patients.14 Radiationoncology as a field and in the treat-ment of HD was significantly ad-vanced by Henry Kaplan and othersat Stanford University in the 1960s,leading to the cure of the majority ofpatients with early-stage HD with ra-diotherapy alone.15,16 These pio-neers discovered that lymphomawas a systemic disease with a pro-clivity for local failure, and that inorder to achieve high cure rates,nodal regions not clinically involvedneeded to be treated, at that timewith radiotherapy alone.
Chemotherapy for HD started inthe 1940s with limited success. Theearliest regimens were based mainlyon the nitrogen mustards. Althougheffective initially, almost all patientsrelapsed after chemotherapy. This
changed drastically in the late1960s, when Devita and others re-ported on the four-drug MOPP com-bination, and demonstrated the abil-ity to cure more than half of HDpatients with stage �III disease.17
Soon after, combined modality man-agement strategies were introduced,based on the differing toxicity ofchemotherapy and radiotherapy, aswell as the spatial coordination oftherapy. In the United States, ABVDreplaced MOPP as the front-line che-motherapy when it was shown to beequally efficacious and less toxic interms of secondary leukemias andsterility.18
The combined strategy of full-dose chemotherapy with extended-field radiation therapy was effectivein achieving cure; however, the un-foreseen costs were observed de-cades later with late treatment-re-lated morbidity and mortality.
In particular, long-term follow-upof HD survivors who had been treatedwith large-field/high-dose radiother-apy showed a disparate number ofsecondary lung and breast cancerscompared with age-matched controls.Excess leukemias were seen in pa-tients receiving MOPP chemotherapy.The risk of developing a second can-cer is clearly related to the irradiatedvolume and radiation dose.19,20 It isimperative to note that the radiother-apy techniques used in the 1950s–1980s are no longer applied. Due totechnological advancements, as wellas a better understanding of the prob-lems associated with large-field radio-therapy, radiation oncologists nowemploy limited-field techniques suchas involved-field or involved-nodetechniques, and can often treat thepost-chemotherapy volume. This re-duction in radiation dose and volumehas translated to a significantly de-creased secondary malignancy ratescompared to extended-field tech-niques.21
More recently, efforts have fo-cused on reducing the toxicity oftreatment for early HD, eitherthrough reduced-dose combinedmodality treatments (ie, smaller ra-diation volumes, limiting radio-
therapy fields to involved fields, treducing the number of cycles ofchemotherapy), or eliminating ra-diation therapy all together.
Trials addressing the question ofcombined modality therapy versuschemotherapy alone for early, favor-able HD are nicely summarized in arecent review article from Yahalom atMemorial Sloan-Kettering CancerCenter.22 In short, combined modalitytherapy maximizes disease control(typically measured by event-free sur-vival or freedom from progression),but the effect on overall survival isless clear when looking at the individ-ual trials. These trials may be under-powered to adequately study overallsurvival. However, a recent meta-anal-ysis of all published randomized pro-spective trials comparing combinedradiation/chemotherapy approachesversus chemotherapy alone revealedimproved tumor control and overallsurvival in those patients who re-ceived combined modality treat-ments. The hazard ratio was 0.41 fortumor control (95% confidence inter-val [CI], 0.25–0.66) and 0.40 for over-all survival (95% CI, 0.27–0.61).23
For most patients with stage I–IIHD, I would recommend combinedmodality approaches based on thedata discussed here. This approachis supported by the NCCN Guide-lines. Recent interest in dose de-in-tensification exploits the “best” thatboth chemotherapy and radiother-apy have to offer, and minimizes the“worst” they bring to the table. Forexample, in the recently publishedGerman HD10 trial, favorable early-stage HD patients had similar dis-ease control with 20 Gy of involved-field radiation therapy and twocycles of ABVD compared to 30 Gyinvolved-field radiation therapy andfour cycles of ABVD, with less acutetoxicity.24 One would postulate thatate toxicity would be less in theose de-intensified arms.
Because the efficacy of treatmentor early, favorable HD is so high,nd the toxicity of radiotherapy andhemotherapy can be significant,reatment approaches need to beustomized to the individual pa-
ient. We are concerned about the
Early-stage Hodgkin disease 709
potential risks of a secondary breastcancer whenever the axilla orbreasts are in the radiation field, es-pecially in young women. If thechest or axilla is not in the radiationfield, such as in a patient presentingwith disease confined to the neck,the risk of second malignancy fromradiation therapy is of much lessconcern.
In terms of the clinical scenarioprovided, the patient plays an inte-gral part in the decision-making pro-cess. Patients should be seen byboth medical and radiation oncolo-gists before treatment, and the casediscussed in multidisciplinary set-ting with radiology and pathologystaff. If she is concerned more aboutsecondary malignancies than failurefrom her HD, then chemotherapyalone would be acceptable. The ca-veat to this is that we do not havelong-term follow-up data for patientstreated with six cycles of ABVD, andthere are similar theoretical con-cerns about cardiotoxicity and pul-monary toxicity that may manifest20 to 30 years later. If the patientwants to maximize her chance ofcure, then I would offer combinedmodality treatment as in the GermanHD10 trial. Her axilla would not beirradiated, and I would not treat theuninvolved high cervical necknodes. Doses of 20 to 30 Gy wouldbe used after two to four cycles ofABVD.
Follow-up would include a regu-lar history and physical examina-tion, and annual blood work includ-ing thyroid-stimulating hormone(TSH) determination. Due to the me-diastinal disease, I would recom-mend CT chest with contrast for thefirst 3 years, then switching to an-nual chest x-rays, with CT and/orPET/CT based on abnormal history,physical signs, or chest x-ray find-ings. If she had mediastinal radiationtherapy, I would recommend breastscreening beginning 10 years aftertreatment has been completed. Inwomen who received chest radia-tion therapy prior to age 30, mag-netic resonance imaging (MRI) is
recommended in addition to mam-mography. Her risk of infertility islow with either ABVD alone orABVD and involved-field radiation tothe mediastinum and low-neck.
Moving forward, an exciting areaof active research involves the useof interim PET scanning and tailor-ing the subsequent therapies forearly HD. Three ongoing phase IIItrials in Europe will evaluate omis-sion of radiotherapy in PET-negativepatients after two to three cycles ofABVD. Until we have the results ofthese trials, combined modality careremains the standard for most pa-tients with localized Hodgkin lym-phoma.
Christopher A. Peters, MDRadiation Oncologist and Clinical
Research DirectorNortheast Radiation Oncology
Center (NROC)Clinical Assistant Professor of
MedicineThe Commonwealth Medical
College, Scranton, PA
RADIATIONONCOLOGIST’S OPINION
This patient is a young womanwith enlarged cervical and supracla-vicular nodes bilaterally. Lymphnodes have size (three dimensions),mobility, location, texture, and aresometimes painful. None of thosefactual characteristics are describedbut it is noted that she had a fine-needle aspiration of the cervicalneck node initially that was incon-clusive. This is not unusual in lym-phoma, particularly HD, and is reallywhy one needs a nodal biopsy ini-tially for the diagnosis of HD or non-Hodgkin lymphoma. (Aspirates arereasonable to confirm relapse butare suboptimal for initial diagnosis,both because of difficulties in iden-tifying RS cells and also inability todescribe internal nodal architectureitself.)
In HD it is necessary to see a RScell for a diagnosis. If the biopsy isdescribed as “consistent with” HDbut no RS cell is observed, then the
physician does not have a diagnosisof HD. In my experience, this situa-tion is most frequently seen in themediastinum and treatment is typi-cally urgently administered. If thatpatient relapses after treatment, it isoften then called diffuse large B-celllymphoma on biopsy at relapse.One other point to make is that HDis a good name for this illness. Thereis no animal model for it because itrepresents an admixture of both tu-mor cells and inflammation. As far asone can tell the tumor cells are gen-erally less than 10% of the total cel-lular population and the inflam-matory component itself is not ma-lignant and presumably evolvesfrom secretions of lymphokines andcytokines from the RS cells. This isprobably a major reason why HD iseasier to cure than the non-Hodgkinlymphomas.
Once the diagnosis was estab-lished in this case, the patient wasstaged as supradiaphragmatic stageIIA, having disease in the right neckand the paratracheal and mediasti-nal area but in no other lymphnodes below the diaphragm. I can-not tell from this report if they areseparating the hilar nodes into a dif-ferent category from the mediasti-num as the staging classification ac-tually does. Bone marrow biopsywas negative. After four cycles ofABVD she is said to be in a completeremission, at least by PET scanning.They describe a mild persistence ofsupraclavicular adenopathy but theydo not furnish any standardized up-take value (SUV).
The question is what to do now:radiation therapy, further chemo-therapy, or observation? Apparently,her mediastinal disease was on PETscan only and that seems to havecleared; the other factors are rela-tively favorable in terms of histologyand blood chemistries. There wasno enlarged mediastinal mass onchest x-ray, although the paratra-cheal/mediastinal nodes were ap-parently abnormal on PET/CT; theresults of the CT scan of the chestare unclear from the description.
The three listed options for treat-
ment should be the basis for a very
mertewt
710 C. Peters et al
good prospective study that couldeasily be done by the cooperativestudy groups, using the PET/CT scanas the definitive tool for calling“complete remission.” I would haveno trouble randomizing on such astudy; moreover, at the moment, itis probably the last major questionin the treatment of HD.
It is not entirely clear what thefalse negative rate is among PET/CTscans, but it is probably over 10%.Every time a patient is deemed to bein CR and then subsequently re-lapses, that is a false negative. None-theless, PET/CT scans are clearly amajor improvement in the manage-ment of these patients and weshould use them routinely despitetheir excessive cost.
The recommendation for thetreatment in this particular patientdepends on the patient herself. Ifshe is anxious and wants everythingpossible done, I would recommendadditional radiation treatment, butbecause she has favorable character-istics and has had what was appar-ently a complete response on PET, Ido not feel compelled to recom-mend radiation treatment under allcircumstances. I would have notrouble following such a patient norwould I object to an additional twocycles of chemotherapy. But asnoted, if the patient and family de-sire every possible step being taken,then I would offer radiation treat-ment.
Why combined modality? Thereare two fundamental reasons. First,if the patient were to relapse aftermulti-agent chemotherapy alone, itis very likely that she would relapseat initial sites of involvement,whereas if she were to relapse afterradiation treatment alone, it is likelyit would occur outside radiationportals. Thus, these two treatment
odalities complement each otherxceptionally well. The secondeason for combined modalityreatment is that, because of theffectiveness of both treatments,hen put together each can be
runcated to a degree that mini-
mizes the morbidities classicallyassociated with each modality.
Those who argue against com-bined modality treatment in HDhave a high degree of faith in theability of bone marrow transplantsto salvage such patients. It is cer-tainly reasonable to go that route forrelapse. On the other hand, bonemarrow transplants do not salvageall patients. Not only do they notsalvage everybody, but many re-lapsed patients never get that far. Inorder to undergo a transplant, thepatient needs to have a completeresponse or a near complete re-sponse to second-line chemother-apy. While that is often the case, it isnot always the case. In addition, onerarely transplants a patient who iselderly and certainly not one whoremains sick from disease or has ma-jor comorbid illnesses. Thus, it isimportant to do what one can toavoid transplants, which I considerto be a “last ditch” maneuver. I saythat largely because following atransplant, most patients cannotsubsequently receive aggressive fur-ther treatment, either radiation orchemotherapy, without major he-matologic risks. Their blood countsmay be good following the trans-plant, but the real issue is how wellthose counts will hold up to stress-ful treatment interventions.
In radiation therapy most of ourcomplications are dose-related. Thestudies from the 1960s, 1970s, and1980s that are often quoted as refer-ences really reflect an era of radia-tion therapy in which the radiationoncologist pushed the dose to themaximum. In today’s world we do itmuch differently. The volumes aremuch smaller typically and thedoses have been reduced by roughly25% to as much as 50%. If I were totreat such a patient as described, Iwould not treat the axillae. This ma-neuver virtually eliminates breastcancer secondary to radiation treat-ment in female HD patients be-cause, in my experience, virtually allwomen who have suffered thatproblem have had upper outer
quadrant lesions related to the axil-lary exposure where the dose is fall-ing off at the edge of the field. It is aparadox in mammals that radio-on-cogenesis in the area where the tu-mor begins is usually not in the high-est dose region but typically wherethe dose is falling off at the edge ofthe field. When a patient is treatedto a field that is as large as a mantle,there is a range of doses that thepatient sees depending on whichlymph node group we are talkingabout. The axillary dose tends to bethe lowest. Also by omitting the ax-illa, pulmonary doses and morbidi-ties are markedly reduced becausethere is an enormous reduction inthe scattered dose under mantlelung blocks that classically consti-tutes most (roughly 80%) of the pul-monary dose.
When I treat such a patient today,I start a modified mantle (we virtu-ally never treat a full mantle any-more) at the level just below thevocal cords. There is no particularreason to make the patient hoarse,even transiently, nor to cause rou-tine hair loss after effective chemo-therapy. If there is upper neck dis-ease (defined as something abovethe level of the thyroid notch), thenI do a more classic field that goesall the way up to the inferior surfaceof the mandible and mastoid tipwith the neck maximally extended,but that is very uncommon today.For about a year and a half I tried toreduce the volumes in treating suchpatients and to treat only involvednodes plus margin. During thattime, four patients relapsed in car-diophrenic nodes that were not ini-tially involved, sitting on the dia-phragm in proximity to the heart.Again, I consider those to be falsenegatives on the PET/CT scan. Fol-lowing the fourth case I went backto treating the full mediastinal sil-houette including the entire heartinitially to cover those cardio-phrenic nodes. Since then, I havenot seen a cardiophrenic relapse.The entire heart and the cardio-phrenic areas receive 15 Gy at rateof 150 cGy/d because the entire car-
diac silhouette as well as a lot of
Early-stage Hodgkin disease 711
lung behind the heart are directlyexposed. At 15 Gy I shrink the fieldby raising the inferior collimator toapproximately 5 cm below thecarina, and bringing the left-sidedcollimator in toward the hilum (un-less there is bulky axillary diseasethat has to be treated on the left).Then I boost the nodes that sur-round the airway for another 18 Gy,at 180 cGy/d. Thus, such patientstoday receive a total dose of 33 Gyover 4 weeks. Here at the Universityof Pennsylvania, it has been exceed-ingly safe. There have been no car-diac problems and only one pneu-monitis in a patient who continuedto smoke despite pleas to stop.
I would add one other comment:there are many who want us to re-duce the dose of radiation further. Iunderstand their concerns, but re-ducing the dose cannot possiblymake the results of treatment anybetter unless one is having majormorbidities. That has not been ourexperience following the treatmentoutlined here. It is unclear what theoptimal prophylactic dose of radia-tion is because many patients do nothave any residual microscopic tu-mor; we simply do not know whichones. It is for this reason that I adaptmy recommendations to what I be-lieve are the risks associated witheach individual patient: I want thepunishment to fit the crime. Thosewho have had favorable characteris-tics, standard chemotherapy withappropriate doses and schedule, andno drug substitutions do not needadditional radiation if they haveachieved a CR.
With respect to follow-up, I rec-ommend routine CT scans about ev-ery 3 months and PET/CT abouttwice a year for the first 3 years,before spacing them out further.With respect to relapse, certainlymost are treated today with bonemarrow transplant. There is a minor-ity of relapses that occur in onenodal group that I believe are appro-priate for involved-field radiationtreatment plus second-line chemo-therapy but that opinion is not
shared by all patients.The issue of second malignanciesis still evolving. Most analyses lookat an actuarial risk, but I am not at allconvinced that is the best way tostudy the problem.
As for fertility, the treatment ofABVD and modified mantle radio-therapy has minimal risks of infertil-ity. There must be some but thequantified risk as a function of age attreatment has not been well studied.
Eli Glatstein, MDVice Chairman
Department of Radiation OncologyUniversity of Pennsylvania
Philadelphia, PA
MEDICALONCOLOGIST’S OPINION
Given the patient’s response andthe fact that she is a young female, Iwould say that she would not needradiation at this point and could beobserved with no further therapy.We would just follow her with rou-tine examiantions, blood work, andchest x-rays and not necessarily anyroutine scans unless somethingshowed up. In the event of recur-rence, she would need salvage che-motherapy followed by high-dosechemotherapy and autologous pe-ripheral blood stem cell transplant.Future risk for secondary malignan-cies with ABVD alone is quite low(�1%–2%). ABVD in a youngwoman does not usually cause infer-tility and she should be able to havechildren in the future.
Julie M. Vose, MDNeumann M. and Mildred E. Harris
Professor Chief, Division ofHematology/OncologyProfessor of Medicine
Nebraska Medical CenterOmaha, NE
MEDICALONCOLOGIST’S OPINION
This patient has favorable stage IIAdisease. The HD-6 trial randomizedbetween the standard arm, whichwas radiation therapy versus two cy-
cles of ABVD in arm 2. If the patientachieved CR after these two cycles,two additional cycles (four in total)were completed. If the patient had aPR, four more cycles (six in total)were completed. The chemotherapy-only arm allowed 90% of patients toavoid radiation therapy and preservedequivalent survival. Four cycles areadequate in this patient.
PET scans can be used for follow-up. Although the trials in HD (HD15/Intergroup) were in advanced-stage patients, the data can be extrap-olated to favorable-stage patients aswell. I would obtain PET scans at3-month intervals for the first year, 4months for the second year, every 6months for year 3, and then yearlyuntil year 5. I would follow the pa-tient clinically on the same scheduleas the PET scan and obtain completeblood cell counts, lactate dehudroge-nase, blood chemistry, and liver func-tion tests at each visit.
With Stanford V4,5 and BEACOPP(bleomycin, etoposide, doxorubi-cin, cyclophosphamide, vincristine,procarbazine, prednisone) there arefertility issues. ABVD should pre-serve fertility.
MOPP and its variants have beenstudied extensively for adjuvant ther-apy of patients with early-stage dis-ease but are associated with the devel-opment of secondary malignancies,including acute leukemia and solid tu-mors. ABVD has been compared withMOPP in combination with radiationtherapy for patients with stages IIBand IIIB, and ABVD is not associatedwith a high risk of acute leukemia;however, cardiac and pulmonary tox-icities have been reported, and theremay be long-term complications fol-lowing ABVD in combined modalityprograms (combination bleomycinuse � lung radiation can cause severeradiation pneumonitis). Interestingly,granulocyte-colony-stimulating factorin combination with ABVD may makethe lung toxicity associated withABVD worse.
In the event of recurrence, pa-tients can be salvaged with radiationtherapy for localized recurrence,and conventional-dose chemother-
apy regimens such as ICE (ifosf-
1
1
1
1
1
1
1
1
1
712 C. Peters et al
amide, carboplatin, etoposide),DHAP (cisplatin, cytarabine, dexa-methasone), ESHAP (etoposide,methylprednisolone, cisplatin, cyt-arabine), and mini-BEAMHD (BCNU,etoposide, high-dose cytarabine,melphalan), and autologous stemcell transplant, as well as investiga-tional agents.
Lisa C. Thomas, MDAttending Physician and Director,Hematology/Oncology Fellowship
ProgramHematology & Oncology Associates
of NE PA, PCClinical Assistant Professor of
MedicineThe Commonwealth Medical College
Scranton, PA
SUMMARY AND ASSESSMENT
We present a case of early-stage(IIA) HD in a young woman whosedisease has responded to initial che-motherapy, leaving a clinical conun-drum as to how to proceed with fur-ther suppressive therapy prior toembarking on observation and follow-up. While the NCCN Guidelines sug-gest that either completion of a totalof six cycles of ABVD or involved-fieldradiation therapy is appropriate forPR, the choice of either of thesemodalities must be weighted verycarefully and the possible long-termeffects uniquely and specifically con-sidered for a 24-year-old woman. Asdiscussed above, the immediateshort-term effects of chemother-apy, including risks of infection,cardiomyopathy, pulmonary toxic-ity, bone marrow suppression anddisorders, and of infertility, mustbe weighed against the risks of ra-diation, which may include an in-creased breast cancer risk in ayoung woman. While this is notabsolute, additional breast cancerscreening such as MRI surveillance(ACS) may be useful in the futurefor this patient at the time she be-gins routine mammograms if shedoes undergo radiation therapy to
the chest.I thank the authors for theirthoughtful contributions.24
Gloria J. Morris, MD, PhDHematology & Oncology Associates
of NE PA, PCDunmore, PA
The Commonwealth Medical CollegeScranton, PA
REFERENCES1. NCCN Hodgkin Lymphoma. Practice
guidelines in oncology, v.2.2010.http://www.nccn.org/professionals/physician_gls/PDF/hodgkins.pdf.
2. ACS American Cancer Society. Can-cer facts & figures 2010. Atlanta:American Cancer Society; 2010.
3. Swerdlow SH, Campo E, Harris NL,et al (eds). WHO classifciation oftumours of haematopoietic andlymphoid tissues (ed 4). Lyon,France: IARC; 2008.
4. Horning SJ, Hoppe RT, Breslin S, etal. Stanford V and radiotherapy forlocally extensive and advancedHodgkin’s disease: mature results ofa prospective clinical trial. J ClinOncol. 2002;20:630–7.
5. Advani RH, Hoppe RT, Baer DM, etal. Efficacy of abbreviated StanfordV chemotherapy and involved fieldradiotherapy in early stage Hodg-kin’s disease: mature results of theG4 trial. ASH Annual Meeting As-tracts. Blood. 2009;114:1670.
6. Santoro A, Bonadonna G, ValagussaP, et al. Long-term results of com-bined chemotherapy-radiotherapyapproach in Hodgkin’s disease: su-periority of ABVD plus radiother-apy versus MOPP plus radiother-apy. J Clin Oncol. 1987;5:27–37.
7. Engert A, Franklin J, Eich HT, et al.Two cycles of doxorubicin, bleo-mycin, vinblastine, and dacarbazineplus extended0field radiotherapy issuperior to radiotherapy alone inearly favorable Hodgkin’s lympho-ma: final results of the GHSG HD7trial. J Clin Oncol. 2007;25:3495–502.
8. Longo D, Glatstein E, Duffey P, etal. Radiation therapy versus combi-nation chemotherapy in the treat-ment of early-stage Hodgkin’s dis-ease: seven-year results of aprospective randomized trial. J ClinOncol. 1991;9:906–17.
9. Meyer RM, Gospodarowicz MK, Con-
nors JM, et al. Randomized comparisonof ABVD chemoterhapy with s strategythat includes radiation therapy inpatients with limited-stage Hodgkin’slymphoma: National Cancer Instituteof Canada Clinical Trials Group andthe Eastern Cooperative OncologyGroup. J Clin Oncol. 2005;23:4634–42.
0. Rueda Dominguez A, Marquez A,Guma J, et al. Treatment of stage Iand II Hodgkin’s lymphoma withABVD chemotherapy: results after7 years of a prospective study.Ann Oncol. 2004;15:1798 – 804.
1. Straus DJ, Portlock CS, Qin J, et al.Results of a prospective random-ized clinical trial of doxorubicin,bleomycin, vinblastine, and dacar-bazine (ABVD) followed by radia-tion therapy (RT) versus ABVDalone for stage I, II, and IIIA non-bulky Hodgkin disease. Blood.2004;104:3483–9.
2. Hodgson DC, Pintilie M, GittermanL, et al. Fertility among femaleHodgkin lymphoma survivors at-tempting pregnancy followingABVD chemoterhapy. Hematol On-col. 2007;25:11–5.
3. Anselmo AP, Cartoni C, Bellan-tuono P, et al. Risk of infertility inpatients with Hodgkin’s diseasetreated with ABVD vs MOPPvs ABVD/MOPP. Haematologica.1990;75:155– 8.
4. Peters MV, Middlemiss KC. Astudy of Hodgkin’s disease treatedby irradiation. Am J RoentgenolRadium Ther Nucl Med. 1958;79:114 –21.
5. Kaplan HS. The radical radiother-apy of regionally localized Hodg-kin’s disease. Radiology. 1962;78:553–61.
6. Kaplan HS. Clinical evaluation andradiotherapeutic management ofHodgkin’s disease and the malig-nant lymphomas. N Engl J Med.1968;278:892–9.
7. Devita VT Jr, Serpick AA, CarbonePP. Combination chemotherapy inthe treatment of advanced Hodg-kin’s disease. Ann Intern Med.1970;73:881–95.
8. Santoro A, Bonadonna G, Vala-gussa P, et al. Long-term results ofcombined chemotherapy-radio-therapy approach in Hodgkin’sdisease: superiority of ABVD plusradiotherapy versus MOPP plus ra-diotherapy. J Clin Oncol. 1987;5:
27–37.
2
2
2
2
Early-stage Hodgkin disease 713
19. Travis LB, Hill DA, Dores GM, et al.Breast cancer following radiother-apy and chemotherapy amongyoung women with Hodgkin dis-ease. JAMA. 2003;290:465–75.
20. Travis LB, Gospodarowicz M, CurtisRE, et al. Lung cancer followingchemotherapy and radiotherapy forHodgkin’s disease. J Natl Cancer
Inst. 2002;94:182–92.1. De Bruin ML, Sparidans J, van’tVeer MB, et al. Breast cancer risk infemale survivors of Hodgkin’s lym-phoma: lower risk after smaller ra-diation volumes. J Clin Oncol.2009;27:4239–46.
2. Yahalom J. Does radiotherapy stillhave a place in Hodgkin lym-phoma? Curr Hematol Malig Rep.
2009;4:117–24.3. Herbst C, Rehan FA, Skoetz N, etal. Chemotherapy alone versuschemotherapy plus radiotherapyfor early stage Hodgkin lym-phoma. Cochrane Database SystRev. 2011;16;2:CD007110
4. Engert A, Plütschow A, Eich HT, et al.Reduced treatment intensity in patie-nts with early-stage Hodgkin’s lymph-
oma. N Engl J Med. 2010;363:640–52.