Embed Size (px)
Citation preview
EDUCATING NURSING STUDENTS AND COMMUNITY ABOUT END
OF LIFE CONVERSATIONS
EDUCATION
Our Patients Depend on OUR Knowledge about End of Life Care
WE WILL NOT LIVE FOREVER

RELATIONSHIPS
EOL Nursing Competencies
1. Recognize dynamic changes in population demographics, health care economics, and service delivery that
necessitate improved professional preparation for end-of-life care.
(AACN, 2001)
.
2. Promote the provision of comfort care to the dying as an active, desirable, and important skill, and an integral component of nursing care.
3. Communicate effectively and compassionately with the patient, family, and health care team members about end-of-life issues.
4. Recognize one's own attitudes, feelings, values, and expectations about death, and the individual, cultural, and spiritual diversity existing in these beliefs and customs.
5. Demonstrate respect for the patient's views and wishes during end-of- life care.
6. Collaborate with interdisciplinary team members while implementing the nursing role in end-of-life care.

7. Use scientifically based standardized tools to assess symptoms (e.g., pain, dyspnea, gastrointestinal symptoms, anorexia/cachexia, asthenia, anxiety, delirium, depression, and communication barriers) experienced by patients at the end of life.

8. Use data from symptom assessment to plan and intervene in symptom management using state-of-the-art traditional and complementary approaches.
9. Evaluate the impact of traditional, complementary, and technological therapies on patient-centered outcomes.
10. Assess and treat multiple dimensions, including spiritual-psychosocial and physical needs to improve quality at the end of life.
11. Assist the patient, family, colleagues, and one's self to cope with suffering, grief, loss, and bereavement in end-of-life care.
12. Apply legal and ethical principles in the analysis of complex issues in end-of-life care, recognizing the influence of personal values, professional codes, and patient preferences.
13. Identify barriers and facilitators to patients' and caregivers' effective use of resources.
14. Demonstrate skill at implementing a plan for improved end-of-life care within a dynamic and complex health care delivery system.

15. Apply knowledge gained from palliative care research to end-of-life education and care.

END OF LIFE REVIEW

1. Designate a surrogate decision maker
2. Stimulate end-of life discussions between patients, families and caregivers, 3. To document what outcome scenarios are
acceptable to the patient.
(Gordy& Klein, 2011)
Advance Directive
Living Will • A written document • Voluntarily executed by an individual.• Directing the withholding or withdrawal
of life-sustaining procedures • Usually when individual is in a terminal
condition, coma, or persistent vegetative state.
5 WISHES
WHO WILL MAKE DECISIONS WHEN I CAN’T
WHAT MEDICAL TREATMENT I WANT OR DON’T WANT
5 Wishes•How comfortable I want to be
•How I want people to treat me
•What I want my loved ones to know
• Introduced in 1997
• Distributed with support from a grant by The Robert Wood Johnson Foundation.
• Addresses Needs: Medical, personal, emotional, and spiritual.
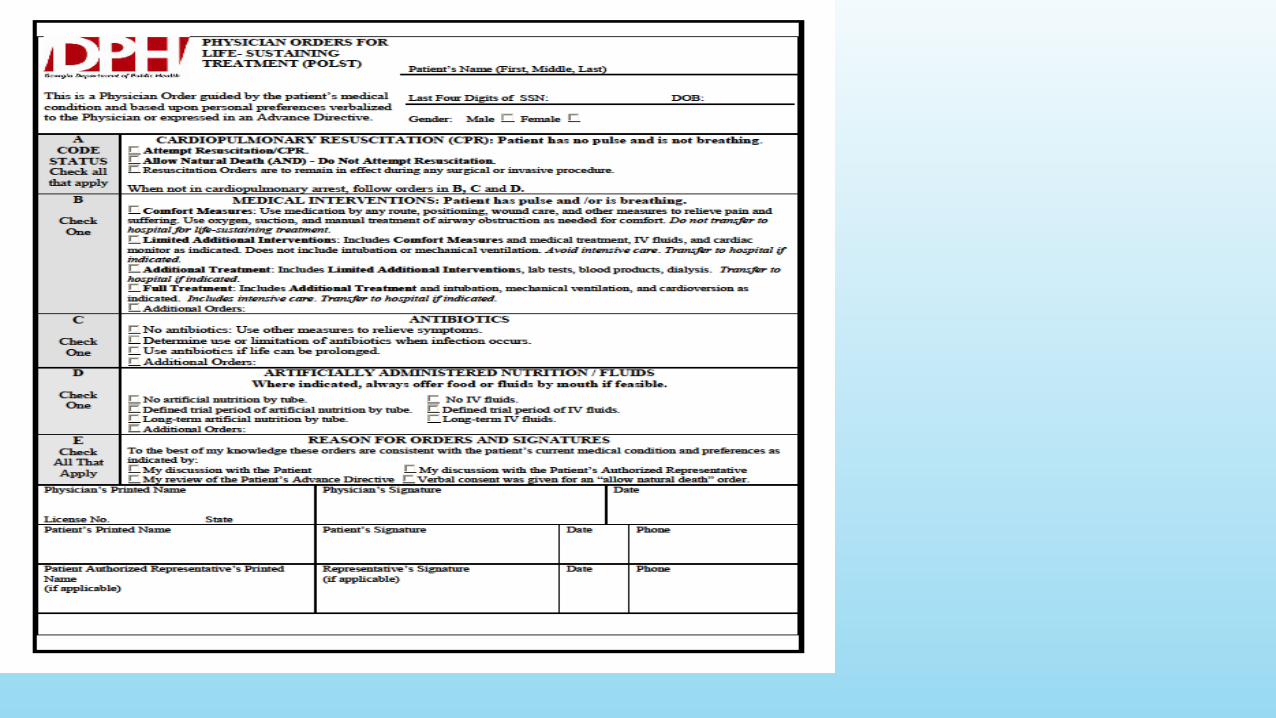
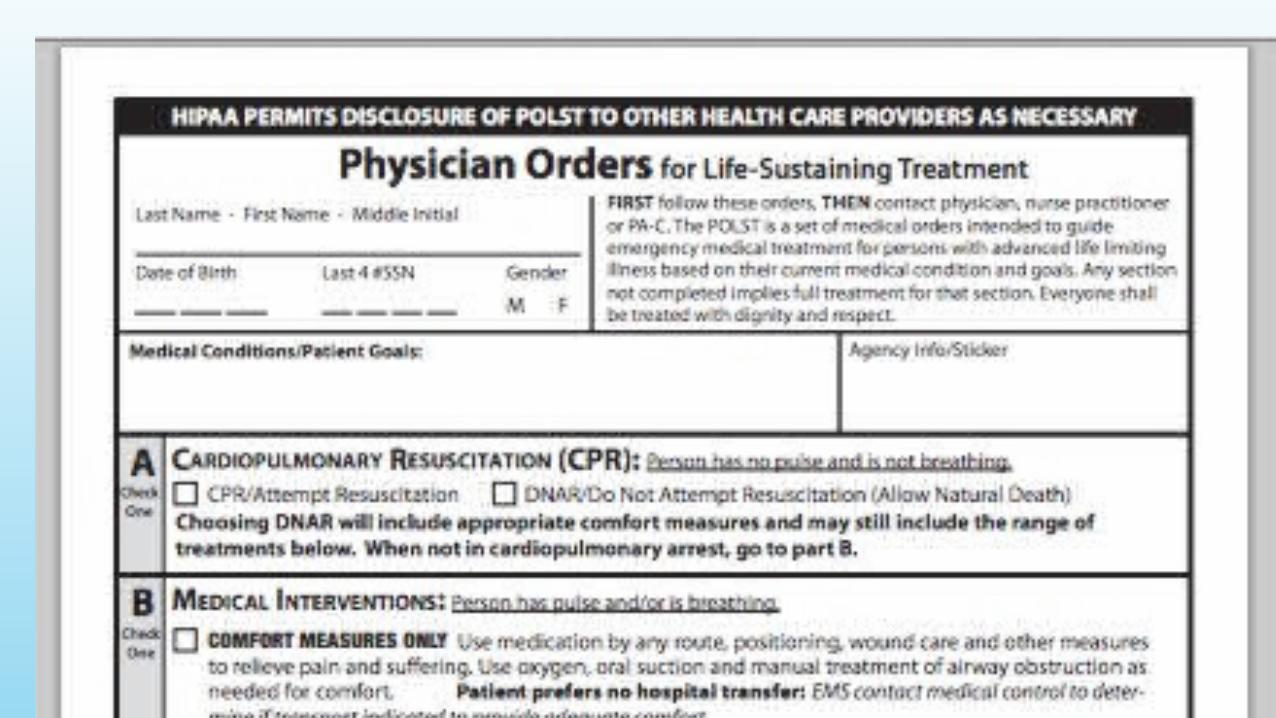
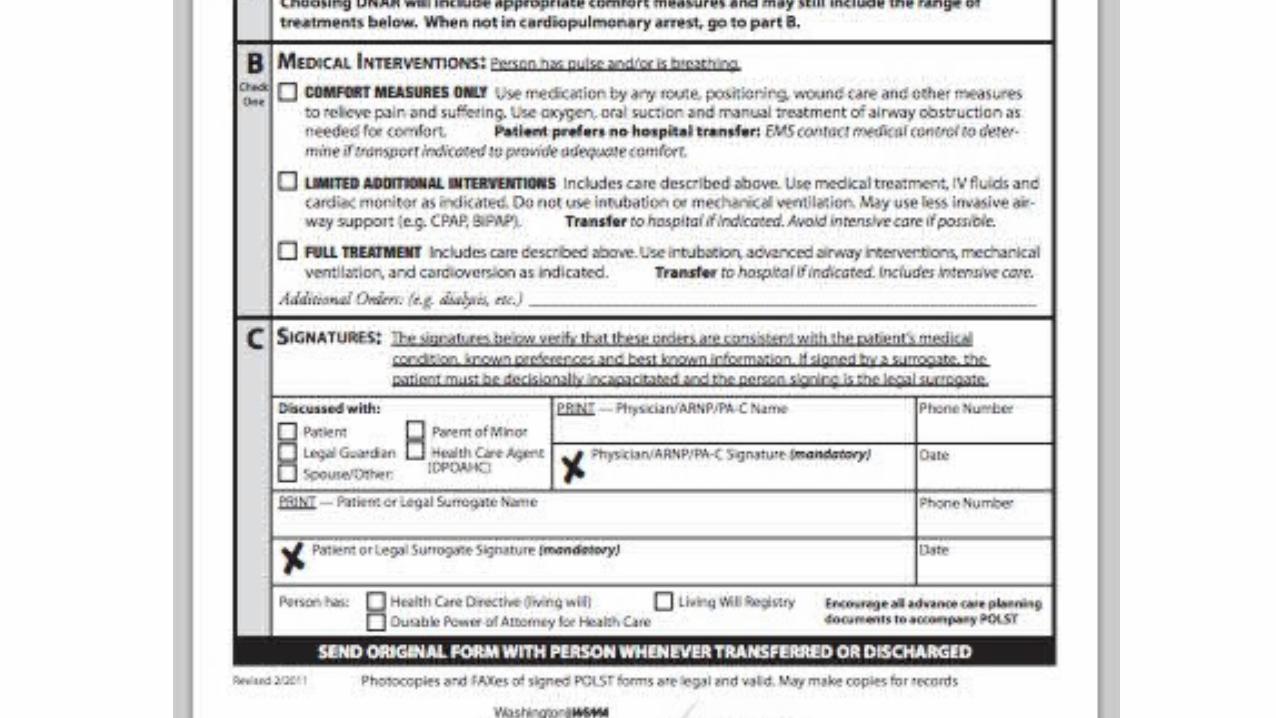
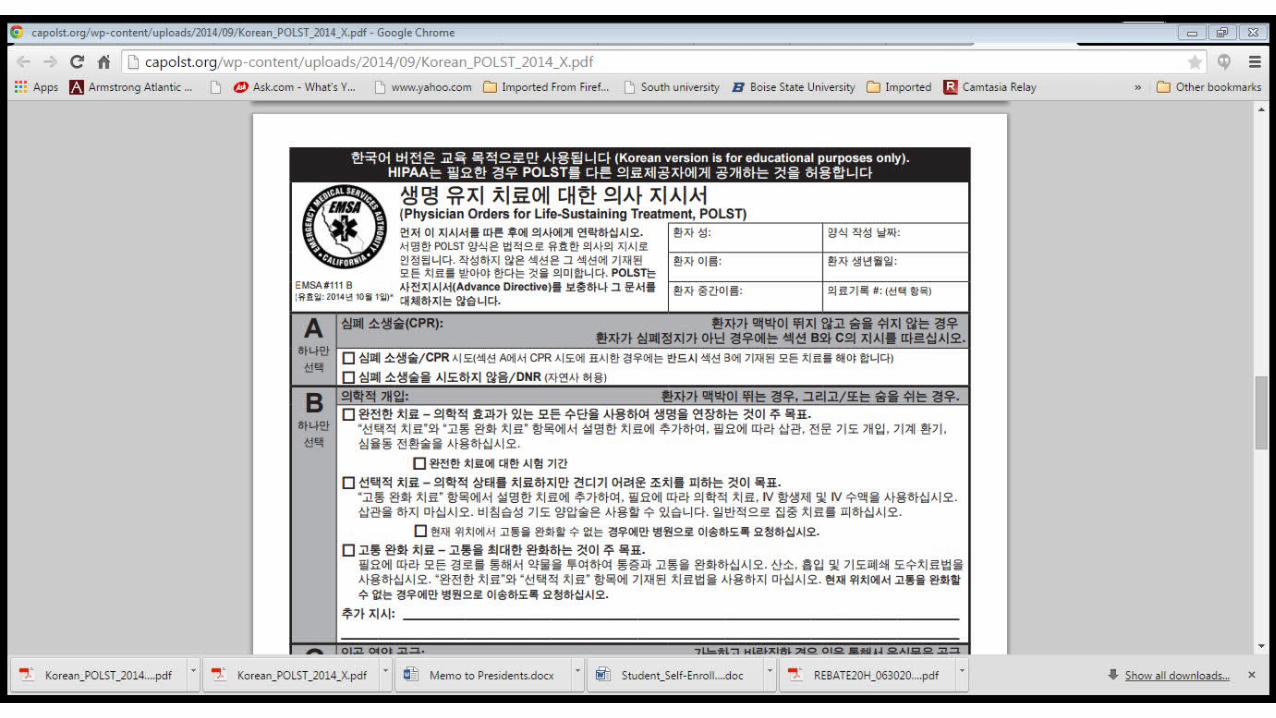
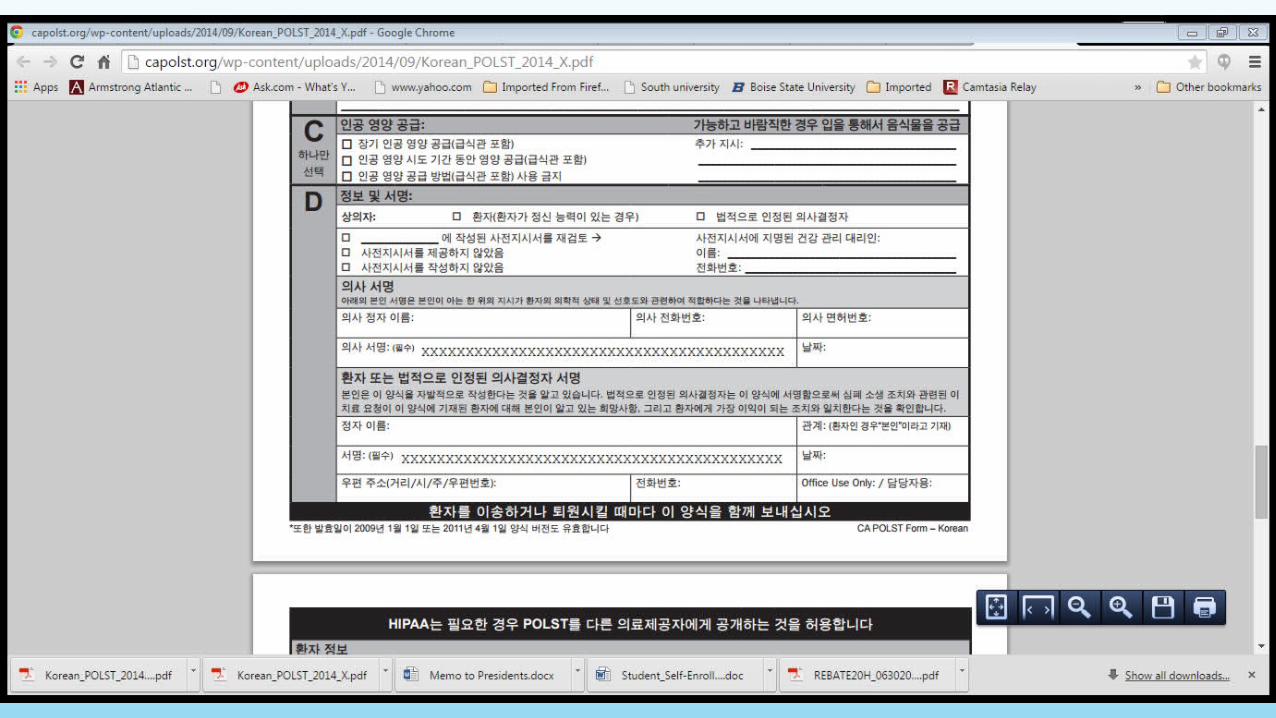
GEORGIA POLST FORMFive Sections•Cardiopulmonary Resuscitation•Medical Interventions•Antibiotics•Artificially Administered Nutrition•Reason For Orders And Signatures
POLST
• Medical order completed by a health care provider
• Mechanism to communicate patient preferences for end-of-life treatment
• Designed to travel with patient from one care setting to another
The Go Wish Game
• Developed by the Coda Alliance
• Values assessment tool
• Help people and their loved ones decide what is important to them at the end of life.
Why Does The Game Work?
• Educational- New Concepts/Ideas • Great for Visual, auditory and
Kinesthetic learners.
Flexible –Complete in many places
Simple not threatening
Open ended Wild card
Familiar comforting format

Easy to read
Basic format
Young to Old is appropriate
Introspection

NATIONAL INITIATIVE
Conversation Ready National Health Care Community
February 13, 2014

OPPORTUNITIES FOR HAVING THE CONVERSATION
Senior CentersNursing AD, BSN, APN ClassesCommunity Outreach Events
Church/Temple/Synagogue gathering and services
END OF-LIFE PRINCIPLES
End-Of-Life Care Is About:
•Compassion at the bedside
•Providing comfort
•Honoring patients’ preferences
GOLD STANDARD
Discussing and following a patient’s preferences for end-of-life care is as routine as asking about and responding to a patient’s allergies to medicines

HEALTH CARE AGENT
Responsibilities:•To follow the patient’s known preferences•To honor the patient’s Advance Directive and POLST•To act in the best interest of the patient

Responsibilities:•To follow the patient’s known preferences•To honor the patient’s Advance Directive and POLST without regard to personal views•If unable to honor preferences, facilitate the transfer of patient’s careWhen necessary, Clinical Ethics Departments can be utilized as a resource in the hospital systems.
Healthcare Team
• Honor all patients wishes• Encourage all patients to
have an Advance Care Plan• Utilize POLST when patient
condition applies• Apply reasonable medical
judgment
Getting It Right
When, in the judgment of the physician, one of “three conditions” are met:•Patient is in a Terminal Condition•Patient is in a permanent state of unconsciousness•Medical judgment that CPR would be futile
Honoring End of Life Documents
ADVANCE CARE PLANNINGDiscus
sion
Decision
Documentatio
n
•Engage with our patients and families to understand what matters most to them at the end of life
•Steward this information as reliably as we do allergy information

NURSING CURRICULUM EOL
Health Assessment
Pharmacology
Psychiatric-Mental Health
Nursing Management Courses
Interprofessional Collaboration for EOL Care
Ethical Legal
Cultural Issues Content
Nursing Research
Hospital, Nursing Home/Home Care/Assisted Living
EOL COSTS OF CARE: WHERE IS THE MONEY GOING
•Health Care Costs Highest in the World
• Outcomes No Better
( Goodman, Skinner, Bronner, Fisher,2009)
Barriers to Effective Palliative End of Life Care
• Minority Populations
• Rural settings
• Patients with FFS insurance
Langton et.al., 2014)
Regardless of the Outcome
Resource utilization increased sharplyAs death approached
Particularly in the last 3 months of life.
(Langton, et al, 2014)
In nearly half of the patients that die in US hospitals,
the last three days of their life is spent in an ICU.

More than 25% of health care cost is spent
in the last year of life.
(Curtis, Engelberg, Bensink & Ramsey, 2012)

Australian Trial
Hospitalized patients over 80 years old
100% May Opt Out of ICU Care
(Detering, Hancock, Reade, Silvester, 2010)
Patients Die in the ICU
• 60–80% do so after life-sustaining therapy is held.
(Abrahm, 2011)
Education of Nursing Students Involves
Interprofessional Effort of Engagement in Many Ethical Opportunities.
LET’S TAKE OUR EOL TEACHING RESPONSIBILITY SERIOUSLY

References
Abrahm JL. Advances in Palliative Care Medicine and End-of-Life Care. Annu Rev Med. 2011;62:187–9.
AACN: Peaceful Death: Recommended Competencies and Curricular Guidelines forEnd-of-Life Nursing Care:
Amercian Association of Colleges of Nursing Publications, Washington, D.C.: 2001: p, 1-5, Retrieved
from: http://www.aacn.nche.edu
Curtis, J. R., Engelberg, R. A., Bensink, M. R., Ramsey, S. D. (2012) End-of-Life care in the intensive care unit:
Can we simultaneously increase quality and reduce costs? American Journal of Respiratory and
Critical Care Medicine, 186, 587-592
Langton, Blanch, Drew, Haas, Ingham & Pearson (2014) Retrospective studies of end-of-life
resource utilization and cost in cancer care using health administration data: A systematic
review. Palliative Medicine, 28, 1167-1196.O’Mahony, S., Mchenry, J., Blank, A. E, Snow, D., Eti Karakas, D., Santoro, G.,…Kvetan, V. (2010). Preliminary report of the integration of a palliative care team into an intensive care unit.
Palliative Med 24, 143-165.
Neuberg, G. W. (2009). The cost of end of life care. A new efficiency measure falls sort of AHA/ACC
standards, Circulation: Cardiovascular Quality Outcomes, 2, 127-133.